Fracture management
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms

Fracture
Complete/incomplete break of bone continuity
Causes of bone fractures
Traumatic, Avulsed, Pathological, Stress and Compression
Traumatic fracture
Direct - blow/injury results in fracture at site of trauma
Indirect - impact/contact made away from fracture site i.e. twisting injury
Avulsed fracture
Bone damaged by violent contraction of attached muscles
Pathological fracture
Spontaneous bone fracture already weakened due to pathological process i.e. neoplasia
Stress fracture
Fatigued bone fractures due to prolonged, repetitive stress
Compression fracture
Cancellous bone fracture after compression, causing collapse in on itself, typically skull or vertebrae
Clinical signs of broken bones
Swelling, heat, bruising, pain, deformity, crepitus (crunching sound bone rubs), function loss, unnatural mobility
Classification of fractures
Open versus closed, anatomical location, number of fragments
Open versus Closed
Open - broken bone visible through skin. Potentially due to overlying wound exposing bone, or bone fragments poke through skin. Without skin barrier to protect bone, risk of infection greater
Closed - broken bone remains covered by skin. Reduces likelihood of infection, injury less obvious, therefore damage overlooked/underestimated
Anatomical location
Articular - fracture associated with joint, implications for movement & healing. Avulsed fractures can occur when attachment of muscles (tendons) ‘rip’ away bone section, leaving fragment free-floating on radiographs
Diaphyseal - most common, main shaft of bone (diaphysis) broken, due to trauma/pathological
Physeal - in epiphyseal (growth) plate in immature animal. Significant implications for growing and categories of injury can help determine risk factors
Epiphyseal - involves ends of bone - epiphyses
Condylar - involves condyles of long bone
Number of fragments
Simple - one fracture line, two bone fragments (bone above and below fracture). Heal quickly, without complications
Comminuted (image) - multiple fracture lines, more than two fragments
Wedge - multiple fracture lines, some contact between main fragments create patch/wedge pattern damage
Segmental - one or multiple complete fragments/sections of bone, each segment having intact shaft of bone (360 cortical bone)
Irregular - multiple fragments, no complete shaft, other than sections above and below injury. Little fragments like shattered glass
Multiple - multiple fracture lines, across different bones e.g. across digits or involving more than one rib
Salter-Harris (growth plate) fractures
Epiphyseal plate fractures interrupt normal growth processes involved with growth plate, can impact development of limb architecture and have lifelong impact on animals mobility
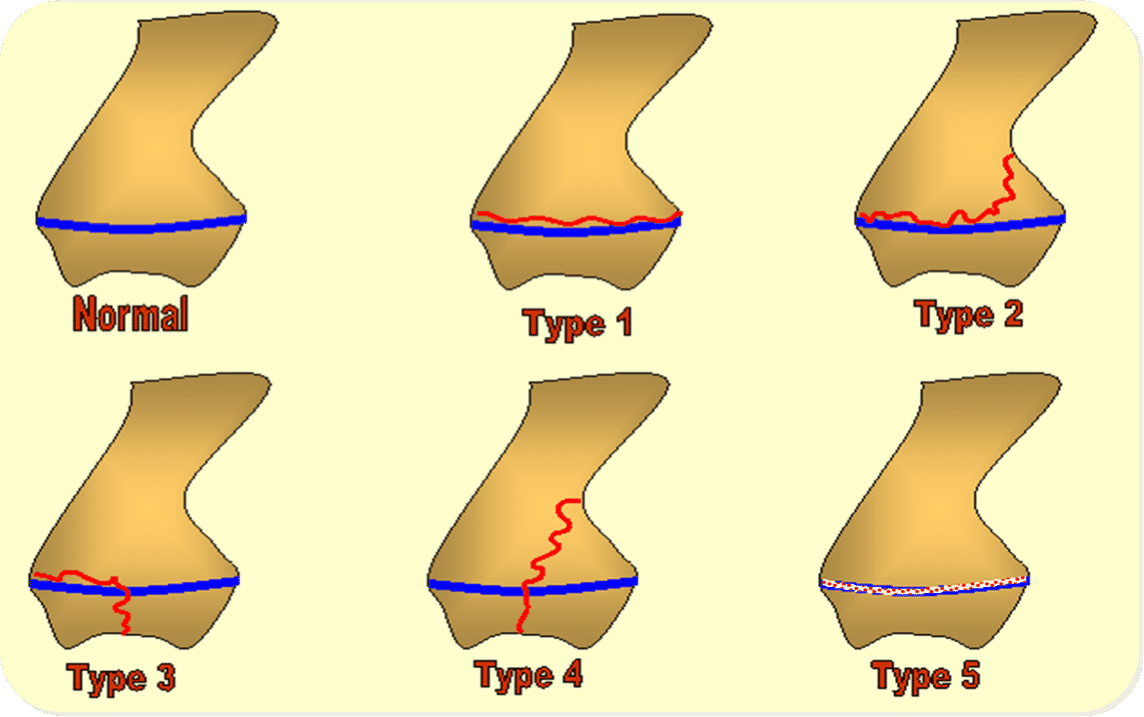
Fracture grades
Type 1: Fracture across growth plate, without bone. Best prognosis for repair and normal function
Type 2: Fracture beyond growth plate, include bone within metaphysis (area above growth plate). Most common Salter-Harris fracture
Type 3: Fracture beyond growth plate, into epiphysis (end of long bone). Reflects complications associated with joint involvement
Type 4: Involves metaphysis, growth plate and epiphysis, significant effect on joint development and mobility
Type 5: Crush injury to growth plate, may unnoticed until animal develops, result angular abnormalities in affected limb
Types of displacement
Greenstick, fissure, depressed, compressed, oblique, spiral and longitudinal

Greenstick
Incomplete fracture of bone in immature animal (not involve growth plate)
Fissure
Fine crack may displace during surgery/stress
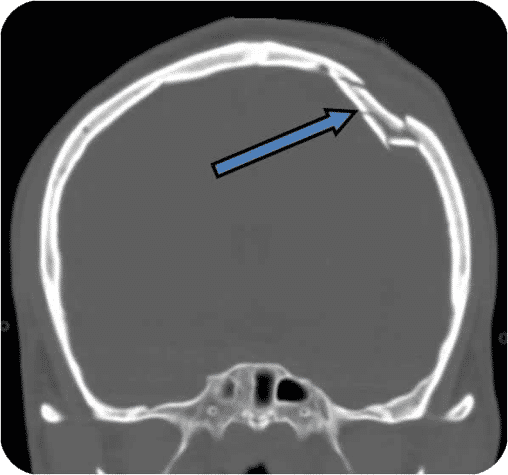
Depressed
Flat bones pushed into underlying cavity e.g. skull fractures
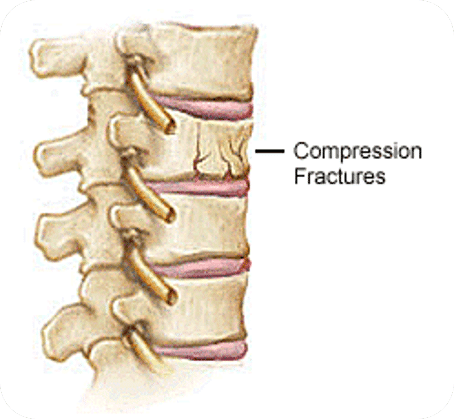
Compressed
Compressive force crushes bones into each other, shortening effect on bone(s) e.g. vertebral fracture

Oblique
Fracture line angle of at least 30

Spiral
Fracture line curves around bone, typically twisting injury

Longitudinal
Fracture on longitudinal axis of bone
Dislocation
Clinical signs - deformity, function loss, pain, limb shortening
Does not involve break in bone continuity, but displacement of joint

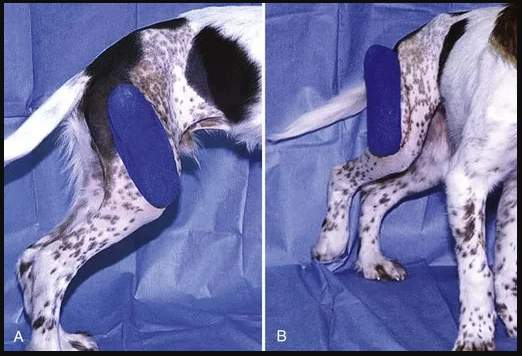
Sub-luxation
Left hip not snug within acetabulum, some connection between the two.
Articular surfaces reduced contact

Luxation
Left hip sits above acetabulum, no connection between two
Articular surfaces no longer in contact
Congenital dislocation
Anatomical abnormalities at birth, may be inherited
Most common congenital luxation involves patella (dislocated kneecap) small breed e.g. jack russell
Acquired
Trauma e.g. RTA
Ligaments keeping joint in normal position are damaged and joint is forced out of alignment, typically involving hip and elbow
Dislocation correction
Before correction animal movement restricted to reduce trauma to soft tissues surrounding joint
Closed reduction
Manipulation of joint, maintaining structural integrity of skin, thereby reducing infection risk
Technique can be used for full/partial luxations
Bones either side of dislocation manipulated into position while under anaesthetic
Strict rest, evaluated frequently to check joint in correct position
Specialised flexion bandaging technique sometimes used to help keep joint in place: Ehmer sling (image) for hind limb, Velpeau sling forelimb

Surgical correction
Surgical intervention to ensure prolonged stabilization of joint
Increased support of joint - tightening joint capsule/providing prosthetic joints, e.g. total hip replacement
Surgery can re-contour joint anatomy to reduce risk of redislocation.
Post-reduction care
Vital to avoid complications exercise restricted 3-4weeks
Applying bandaging/immobilisation to fractures
Manipulation of site increase risk of traumaising soft tissues, e.g. ligaments, nerves and blood vessels, movement painfuk
Better to restrict movement, allow to assume comfortable postion, await veterinary assessment
Diagnosis
Radiographs, CT/MRI warranted with spinal or skull fractures
Anaesthesia recommended due to manipulation and associated pain
Two views ensure abnormailites identified and degree of displacement determined
Non-affected limb for comparison
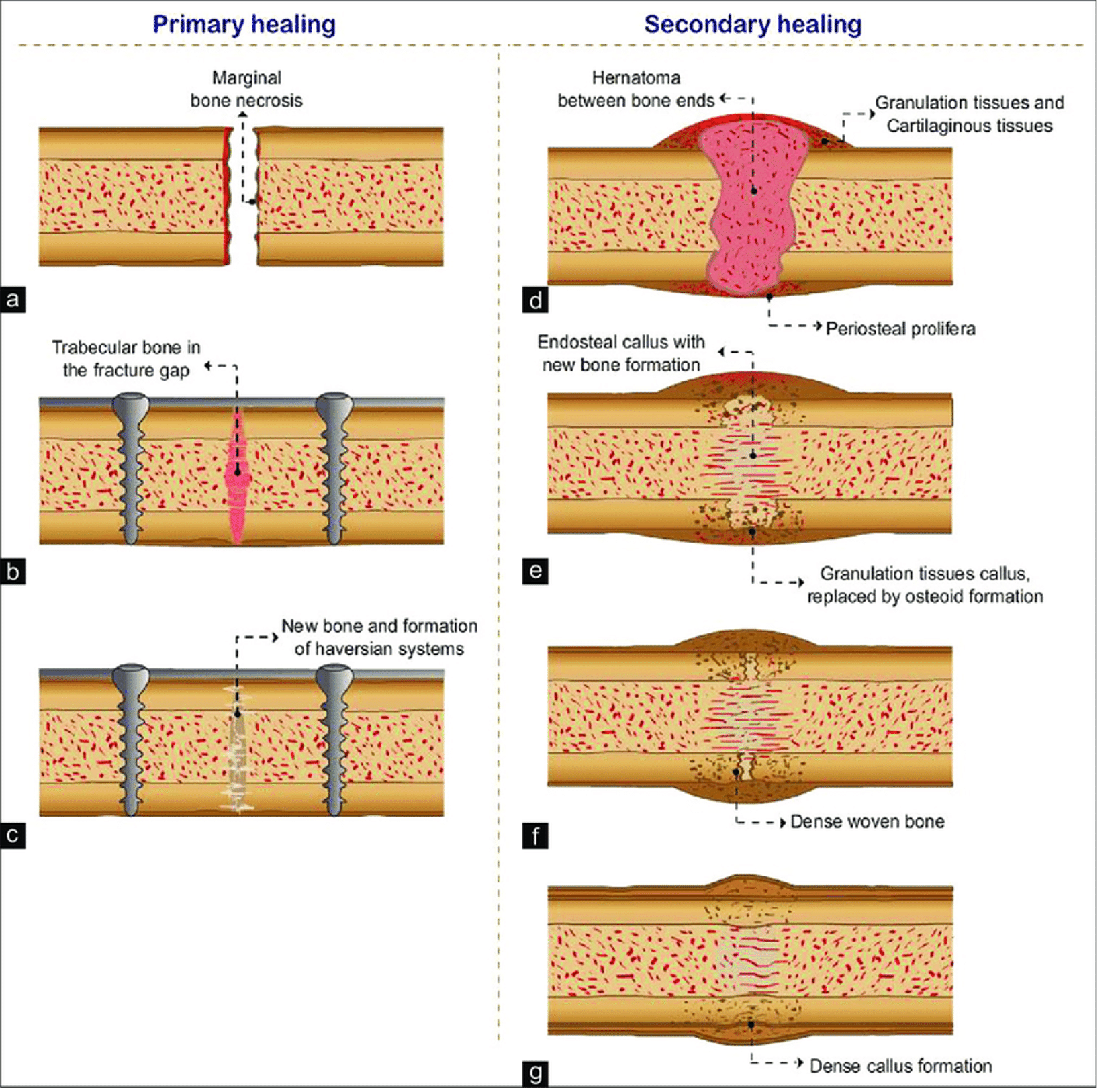
Primary fracture healing
When bone ends closely aligned, simple fracture/surgically repaired, direct healing can occur.
Bone cells (osteoblasts) within Haversian canals able to bridge gap between bone fragments, negating stablising fibrous framework (callus)
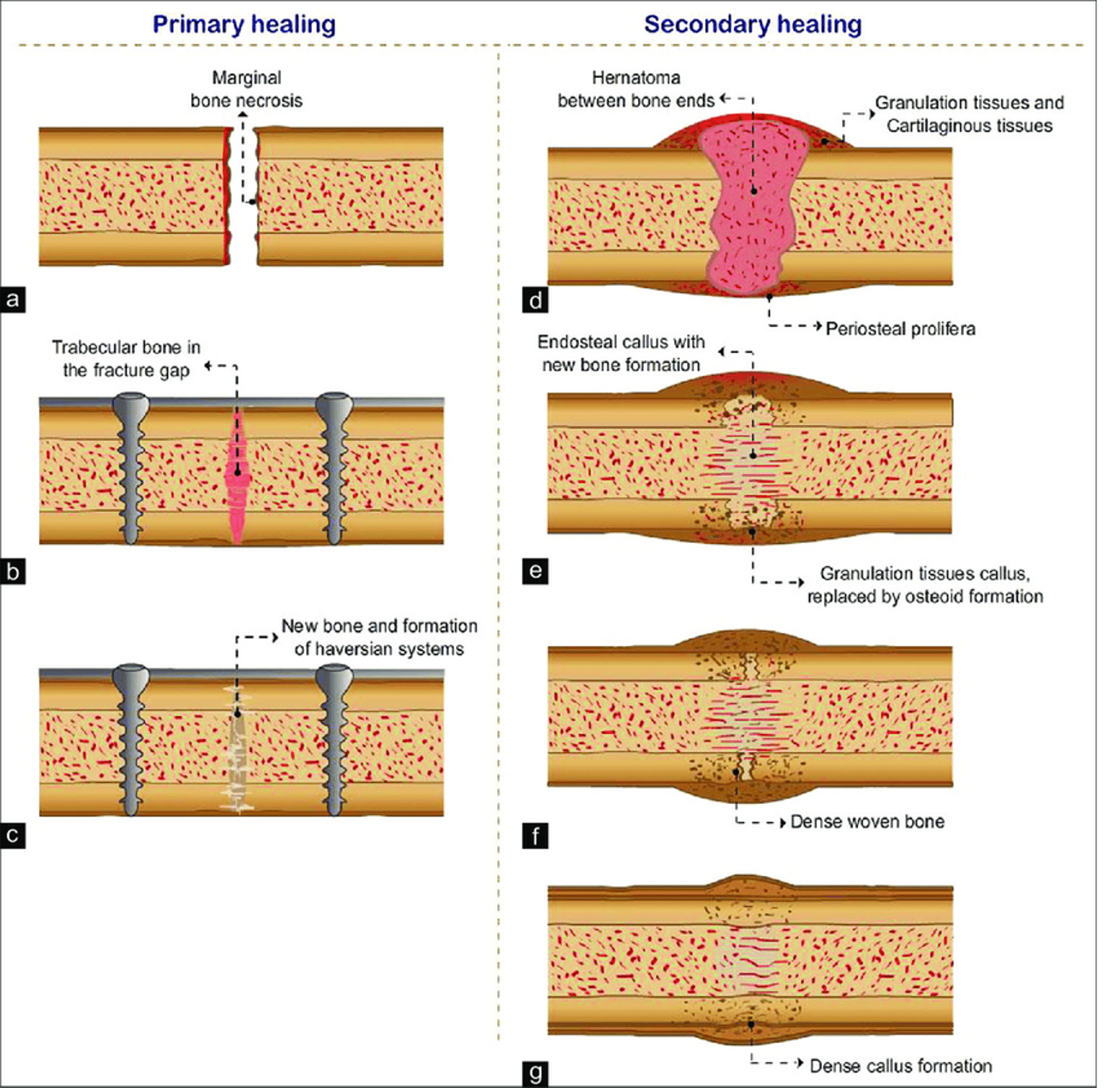
Secondary Fracture healing
Unstable fracutres/multiple fragments
Increased trauma to soft tissues and medullary cavity results in formation of haematoma - subsequent infiltration of fibrous material to create callus. Haversian remodelling restores normal architecture of bone, unless increased movement of bone fragments occurs during healing, prolonged callus (thickening) or malunion can occur
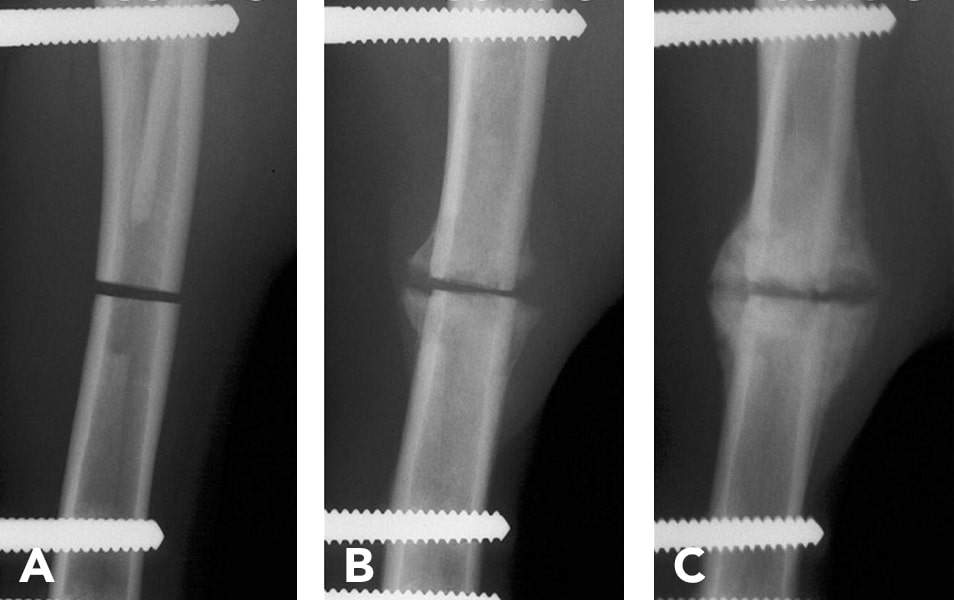
Rate of healing
Clinical (weight bearing) union averaging 12-16 weeks. Remodelling can continue for months after clinical union.
Assessed by CE and radiographs to determine development, remodelling of callus
Rate of healing points
Immature heal quicker, geriatric/debilitated longer
Fractures within cancellous bone often heal quick than cortical bone, as good blood supply promote healing
Osteomyelitis (bone inflammation) delay healing, reversal with appropriate antibiotic therapy
Oblique fracture quick heal than transverse, larger contact area promoting tissue re-growth
Poor reduction (space between fragments/movement connecting edges) slow healing
Non-union
Complete failure of fracture ends to unite
Delayed union
Slowed fracture healing, clinical union not achieved within expected time
Mal-union
Fracture heals in abnormal position
Shortened limb
Inadequate reduction of overriding fracture fragments causing shortening of limb, function severley compromised
Sequestrum
Necrotic bone piece incorporated successfully into fracture repair
Osteomyelitis
Inflammation of bone, bacterial osteomyelitis due to inadequate asepsis during surgery, damaged to local blood supply
Implant failure
Stress applied to surgical implant due to inappropriate selection of implant, due overactive patient, suddent deteroration, instability and pain
Reduction fracture repair
Reduction - fragments brought together in correct anatomical alignment either:
Closed - traction applied to bone fragments through skin, manipulated into place
Open - skin and overlying tissues surgically retracted to visualise fracture, then manipulated into place
Fixation fracture repair
Bone fragments immobilised in correct alignment until clinical union occurs, either directly over fracture or distally (intact bone above and below site). Fragments may also be compressed together to narrow fracture gap, promoting primary healing and speedier recoveries
Principles of fracture fixation
Ensure correct alignment of interrupted bone architecture, restoration of normal function
Immobilising fracture sites
Restore functional anatomy
Restore continuity of bone
Restore bone length
Restore functional shape
Maintain soft tissue function
Prevent pain by fragment movement
Prevent displacement of bone fragments
Prevent movement within fracture site, may delay healing or cause non-union
Methods of fracture fixation
External coaption (splints/casts)
Internal fixation (pins, plates, screws and wire)
External-internal fixation (external skeletal fixators)
External fixation/Coaption
Non-invasive, simple, cheap
For minimally displaced fractures, well tolerated
Careful application of splint/cast due to pressure/rubbing sores
Gross limb immobility - muscle atrophy (wastage)
Casts
Moulded to individual contours of limb
Stable fracture site for method to success, at least 50% fracture in contact with adjoining bone. use limited to lower limb (below elbow/stifle) to ensure adequate immobilisation while preventing slippage
Plaster of Paris (POP) can be time-consuming and messy. Resultant cast heavy for smaller patients, increasing slipping, non-use (muscle atrophy) and fragment displacement
Synthetic casts - quickly mould/harden. Lightweight though may not provide sufficient support for heavier patients

Splints
Bandaging techniques e.g. Robert Jones used for simple fractures
Expensive, time consuming, potential for slipping
Splints on own support or into bandages e.g. wooden splints, Zimmer splints, gutter splints
Resin/plastic splints, inflatable splints
Limited to limbs, straightforward fractures, minimal involvement of other structures e.g. muscles/nerves/blood vessels
Internal fixation
Surgical exposure of fracture site
Invasive, expensive, complex, risks of surgery, anaesthetic, infection, implant reaction, soft tissue injury
Accurate reduction and provides rigid fixation.
Repair encourages return to full function, optimal fracture healing, reduced long-term complications e.g. prolonged callus formation
(Implant, intermedullary pins, cerclage wire and plates/screws)

Implants
Join bone fragments together, restoring normal bone architecture. Provide support while bone heal
Remain in situ for life or removed once site healed
e.g. Tension-band wires and Association for osteosynthesis (AO)/Association for study of internal fixation (ASIF) techniques

Intermedullary pins
Placement of metal rod through medullary cavity to join two ends of bone
Cheap, quick, minimal surgical exposure. Pin easy remove once bone healed to avoid implant reactions
Not ideal for all fractures, less stability than other forms, slower heal
Arthrodesis or Kirschner wire used as intermedullary pin in small animals/bones, used in addition to larger intermedullary pin to increase stabilisation or incorporate additional fragments
image - central intermedullary pin, Kirschner wires each side extending into condyles

Cerclage wire
Stabilise fracutres and compress bone fragments, ensuring close connection, optimal healing
Can be used instead of intermedullary pins/Kirschner wire and bone plates. Wire placed around bone fragments, tightened, compressing fragments and increasing support of fracture site
Helpful with multiple fracture fragments i.e. communited fractures
Cerclage wire useful on small non-weight bearing bones e.g. jaw
Plates and Screws
Metal plates held in position with screws, common method of stabilising fracture sites, some capable being bent to closely fit contours of bone
Useful for fragmented bones, multiple screws holding small bone fragments in place while healing
Plates durable and strong, in situ for animal life, providing support for large animals. Can provide accurate reconstruction of bone architecture, enable longevity of support for slow healing fractures
Venebles, sherman and dynamic compression plates most used
External Fixators
Pins driven into bone, proximally and distally to fracture, to stabilise fracture site during healing.
Pins connected on outside of body to one/more connecting bars, allowing compression of site to encourage close contact of fragments and optimal healing
Useful for open/infected fractures, reduced surgical involvement when compared to plate/screw methods, delayed/non-union fractures following intermedullary pin placement.
Useful for highly contoured bones e.g. mandibular fractures

Kirschner-Ehmer system
One/more straight pins to stabilise/compress fracture site

Llizarov system
Circular frame to stabilise/compress fracture site
External fixation concerns
Prolonged exposure of bone to external environment (internal-external pins). Bone infection serious complication if not managed aseptically
Loose pins, increased movement if clamps not tight. Increase instability within fracture site, delay healing
Soft tissue irritation, swelling quickly impinging on metalwork surrounding site. Pain, risk of infection and exudates
Managing external fixation
Rubber tips/silicon coating/bandaging