Looks like no one added any tags here yet for you.
what are the two main classifications for gram + bacilli
endospore formers and non endospore formers( which can further be divided into regular and irregular shape and staining)
what are the two types of endospore forming gram positive bacilli
bacillus which is aerobic and clostridium wich is anaerobic
eg:
bacillus anrthicos/ anthrax
bacillus cereus/ food poisoning in rice and ice
clostridium perfringens/ gas gangrene often in battelfield
clostridium tetani/ tetanus
clostridium botulinum/ botulism, botox causes paralysis
clostridium difficile/ AAD
what are the types of non endospore forming bacilli
can be first classified as either being of regular or irregular shape and staining
regular shape and staining:
listeria
erysipelothrix
irregular shape and staining
non- acid fast
corynebacterium
propionibacterium
acid fast
mycobacterium
filamentous
actinomyces
nocardia
listeria monocytogenes/ listerosis
• Severe disseminated infection in immune compromised people and in pregnancy – transmitted to foetus).
• Usually acquired from contaminated foods (esp. cold meats, soft cheeses)
erysipelothrix
It is a zoonotic bacterium primarily found in animals, especially pigs, fish, and birds. Humans typically acquire it through occupational exposure (e.g., veterinarians, butchers, fish handlers) via skin abrasions or wounds.
While it is not a common human commensal, it can cause erysipeloid, a localized skin infection, and in rare cases, systemic infections like endocarditis or septicemia in immunocompromised individuals.
corynebacterium
non acid fast, irregularly shaped, non endospore forming bacteria
Normal flora of the skin – rare infections, except Corynebacterium diphtheriae – recent resurgence of diphtheria
Corynebacterium diphtheriae is a Gram-positive, non-motile, non-spore-forming, pleomorphic bacillus that is the causative agent of diphtheria. It belongs to the Corynebacterium genus,
Diphtheria Disease:
C. diphtheriae causes diphtheria, a serious upper respiratory tract illness that can lead to:
Pharyngeal/tonsillar diphtheria – Formation of a thick, gray pseudomembrane in the throat, causing difficulty swallowing, breathing issues, and potential airway obstruction.
Toxin-mediated complications – Systemic absorption of the diphtheria toxin can result in myocarditis, neuritis, and kidney damage
is vaccine preventable
mycobacterium
acid fast, irregularly shaped, non endo spore forming, gram positive bacilli
causes tuberculosis
Actinomyces
Gram-positive, filamentous bacteria
Characteristics
Gram-positive, filamentous, branching rods
Anaerobic or facultative anaerobic
Non-acid-fast
Part of the normal flora of the oral cavity, gastrointestinal tract, and female reproductive tract
Disease: Actinomycosis
Chronic suppurative infection forming abscesses and draining sinuses with characteristic sulfur granules (yellow granules in pus).
Common forms:
Cervicofacial actinomycosis ("lumpy jaw") – often due to dental infections or trauma
Thoracic actinomycosis – can mimic TB
Pelvic actinomycosis – associated with IUD use
Treatment: Penicillin G (long-term), sometimes surgical drainage
no cardia
Characteristics
Gram-positive, filamentous, branching rods
Aerobic
Partially acid-fast (due to mycolic acid in the cell wall)
Found in soil (not part of normal human flora)
Disease: Nocardiosis
Pulmonary nocardiosis – pneumonia-like symptoms, often in immunocompromised patients (e.g., HIV, transplant, corticosteroid use)
Cutaneous nocardiosis – from trauma, causing skin infections
Disseminated nocardiosis – can spread to the brain, leading to brain abscesses
Treatment: Trimethoprim-sulfamethoxazole (TMP-SMX) (first-line), sometimes combined with other antibiotics
bacillus anthracis
gram positive bacilli, endospore fromer
anthrax
spores inhaled or ingested or contaminate a wound
is rapidly progressive, causes skin sores, vomiting and shock
is a bioterrorism agent
is common in areas where animal carcases arent disposed properly
clostridioides /clostridium/ difficile
is present infaeces of most neonates and up to 30% of hospital patients
its spores are widespread in the environment
Gram-positive, rod-shaped
Spore-forming – allows survival in harsh conditions
Obligate anaerobe – cannot grow in oxygen-rich environments
Toxin-producing strains – Toxin A (enterotoxin) and Toxin B (cytotoxin
c.difficile pathogenesis
Normally found in low numbers in the gut microbiota.
Disruption of normal gut flora (due to broad-spectrum antibiotic use, especially clindamycin, fluoroquinolones, cephalosporins) allows C. difficile to overgrow.
Produces Toxin A (causes fluid secretion and inflammation) and Toxin B (cytotoxic, causing cell death).
clinical manifestation of c. difficile
Mild to moderate diarrhea
Pseudomembranous colitis – inflammation of the colon with formation of yellowish plaques (pseudomembranes)
Toxic megacolon – life-threatening dilation of the colon
Sepsis and perforation (in severe cases
Toxin-producing strains cause antibiotic associated diarrhoea -
during or after antibiotic treatment
- mild to severe, intractable diarrhoea
- most severe: pseudomembranous colitis
• Disease is a consequence of disruption of the gut microbiome
c.difficile risk factors
Risk Factors
Recent antibiotic use
Hospitalization, hospital caare facilities
Proton pump inhibitor (PPI) use
Immunosuppression
food contaminated with c difficile
pH increasing agents
treatment for c.difficile
Antibiotics (metronidazole, vancomycin)
If refractory or severe(recurrent infections or unresponsive to antibiotics), consider faecal transplant
microbiome
microbial cimmunity that occupies a well defined habitat- includes viruses, bacteria and parasites
dysbiosis
an imbalance in the microbial community associated with disease
what are the causes for dysbiosis
overgrowth of members of the commensal microbiotae e.g., Enterobacteriaceae, in inflammatory bowel disease
loss of commensals (eg antibiotic therapy)- often accompanied by pathogen overgowth eg clostridioides difficile associated with colitis
loss of diversity- associated with inflammatory bowel disease, HIV, type I diabetes ,mellitus, overgrowth of a few species
pathobiont
a potentially pathogenic organism which under normal circumstances lives as a symbiont
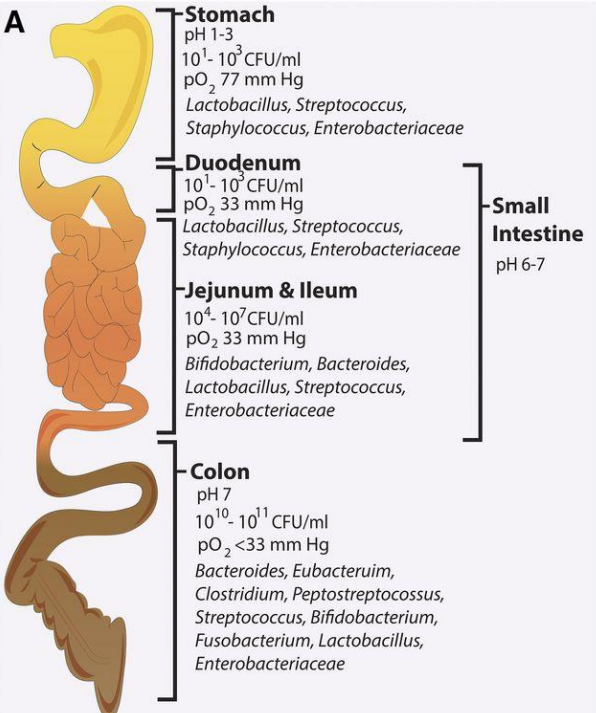
what are the factors determining microbial community composition
environmental parameters
eg oxygen tension(difference between upper respirartory tract and lower GIT),pH, temperatture,energy sources,
interactions between microbes
competition and collaboration between microbes
positive: cross feeding to help others grow is seen when two species of bacteria co exist
negative; bacteria produce antibiotics/ bacteriocins/ that inhibit the growth of competing bacteria
rapid evolution
stochastic/ unpredictable forces
eg dispersal
how to measure the microbiota and its function
through sequencing its genetic composition
there is new technology called next generation sequencing
sequencing many genes in parallel
this removes the need to sequence bacteria individually
composition of the gut microbiome
varies due to environmental changes eg what you eat
what are some factors influencing the gut microbiome
geographical location
host genetics
exercise
stress
antibiotics
age
gastric motility
antimicrobial peptides and igA
gastric secretion
diet
mode of delivery: c section vs natural
obesity and the gut microbiota
there are two main bcteria to consider: firmicutes and bacteroidetes
in obese individuals, there is a higher firmicutes to bacteroidetes ratio
while in lean individual then is higher bacteroidetes to firmicutes
lean vs obese micorbiota transplant experiment
two test subjects where taken, one lean one obese
there microbiota was implanted in recipient mice, and both mouse groups had a low fat high fibre diet
it was observed that the mouse that received the obese twins microbiota displayed increased adiposity while the other mouse became more lean
how does a diet consisting of high plant fibre and low animal fat and protein impact metabolic health
these plant fibres are indigestable to humans but gut bacteria can ferment them
it is linked to increased metabolic health as well as daily defacation
how does a high animal fat and protein diet and low in fibre influence metabolic health
aberrant microbiota related to metabolic diseases
what are some microbiome- directed interventions
exercises
individualised nutrition
faecal mucrobiota transplantation
prebiotics- nutrients that are degraded by and may change composition of the gut microbiota
probiotics- live microorganisms that confer a healthbenefit when consumed in adequete amounts
synobiotics
postbiotics- functional bioactive compounds, generated during fermentation which may be used to promote health
Mycobacterium tuberculosis
causes tuberculosis
needs an acid fast cell wall to be seen as its a gram intermediate
is the leading cause of death- 1.4 million deaths p.a
around 30% of the population is infected but latent TB infection is pathogenic
poverty and crowding increases the risk of TB
Key Characteristics of Mycobacterium tuberculosis
Acid-fast (Ziehl-Neelsen stain positive) due to mycolic acid in the cell wall
Obligate aerobe – prefers high-oxygen areas (lungs)
Slow-growing – takes 2-6 weeks to grow in culture
Resistant to drying & disinfectants due to its waxy cell wall
Can remain latent in the body for year
how is Mycobacterium tuberculosis transmitted
airborne aerosol droplets from infected individuals, coughing sneezing talking
no animal or environmental reservoir
direct human to human transmission
very low infectious dose 1-10 bacteria
how does TB enter body
small droplet nuclei enter terminal airspaces
phagocytosed by alveolar macrophages
spread throughout body
survive within macrophages- by evading killing
primary TB infection
Usually asymptomatic or mild flu-like symptoms
Bacteria multiply in alveolar macrophages
Forms Ghon complex (infected lung area + nearby lymph nodes)
Outcomes:
Latent TB (most cases): Bacteria remain dormant in granulomas
Progressive primary TB (immunocompromised patients): Leads to active disease
latent TB /dormant phase
No symptoms, not contagious
Bacteria are "walled off" inside caseating granulomas
Can reactivate later (especially with immunosuppression)
secondary/ reactivation of TB
Occurs when immune defenses weaken (e.g., HIV, diabetes, malnutrition)
Commonly affects upper lung lobes (more oxygen)
Symptoms:
Chronic cough, hemoptysis (bloody sputum)
Night sweats, weight loss, fever ("consumption"\
pathogenicity largely due to host inflammatory reaction to the bacterium which causes tissue destruction- no classic toxins produced
TB treatment
multi drug therapy to prevent emergnece of resistant strains
minimum treatment duration is 4-6 months for drug sensitiveTB
usually INH (1 in 10^6 is resistant)and rifam (1 in 10^8 is resistant)
MDR (multidrug resistant 1 in 10^14)
how does multi drug therapy work
antibiotic resistance arises in TB as a consequence of chance spontaneous mutations in the chromosome
antibiotics dont cause mutation, but they select for pre-existing resistant mutants
by combining two or more drugs, chance of a particular strain being resistant is 10^14 which is extrememly rare thus the infection will be cleared
what happens if inappropriate treatment is administered
firstly antibiotic resistance of first antibiotic occurs
then this causes the resistant strain to be spread