J Psych CM
1/253
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
254 Terms
T/F: by consensus a formal diagnosis of a “Personality Disorder” can NOT be made before the age of 18
T
1st line tx for paranoid personality
psychotherapy
differences b/w PPD and schizophrenia
PPD: suspicious, NO active delusions (false, fixed ideas) or auditory hallucinations. NO impaired reality testing
People with PPD may experience brief, mini-psychotic like episodes when under significant stress though
difference between schizoid (SPD) and schizotypal (STPD) personality disorder
SPD: avoid social interactions/lack interest. do NOT have cognitive distortion/eccentricities. emotional flatness.
STPD: desire relationships but struggle w/ anxiety, bizarre/idiosyncratic thinking, beliefs, behaviors. DO have cognitive distortions and eccentricities (magical thinking). have anxiety, paranoia, possible intimidation or aggression to others
how to distinguish between Borderline Personality Disorder and Histrionic Personality Disorder?
Borderline patients are generally more depressed and suicidal
Histrionic patients are generally more functional and want praise
how to distinguish between Dependent Personality disorder (PD) and Avoidant PD?
Avoidant PD patients are slow to get into relationships
Dependent PD patients aggressively seek relationships out
OCPD vs. OCD
OCPD: NO obsessions.compulsions. unaware of or don’t care they have “Problems”. MAY respond to SSRIs.
OCD: HAVE recurrent obsessions/compulsions. aware and distressed by problems. OFTEN respond to SSRIs
avoidant PD affects men and women _
equally
overt parental deprecation OR overprotection; phobias in parents
distinguish between Social Anxiety Disorder and Avoidant PD
Avoidant PD is fear of rejection and affects more areas of life
Social Anxiety Disorder is fear of embarrassment in a particular setting (such as giving a public presentation)
when was prolonged grief disorder was placed in the “Trauma & Stressor Related Disorders” category?
2023
what is useful in tx of OCD and social anxiety?
SSRIs/SNRIs
benzo role, when are they used, when not and why?
enhance, augment GABA type A receptors
→ only used if severe/acute life threatening emergency otherwise NOT 1st line d/t potential for addiction
what should you do when an individual has anxiety and separate unrelated medical condition?
ALWAYS r/o possible organic etiologies
You can begin treatment for a severe anxiety disorder while still working up other causative or contributory medical factors
1st line tx for specific phobias
Exposure / desensitization therapy is first-line treatment here
tx for social anxiety disorder and its SE
Tricyclic antidepressants (TCAs)
antichol, can be fatal in overdose, not as effective as SSRIs
PTSD sx manifestations
within a week of the traumatic event,
OR years after the event, being triggered by a similar event, sound, sight, etc.
What is the difference between Acute Stress Disorder and Adjustment Disorder?
Acute Stress Disorder: exposure to actual death, injury, violence. has at least 9 sx of PTSD. lasts few days to less than a month
Adjustment Disorder": identifiable nonthreatening stressors (job loss, divorce) within 3 months of stressor → distress but max 6 mos
risk factors for suicide and _ of depressed patients will ultimately die by suicide
discharge from psych inpatient
15+% of depressed patients will ultimately commit suicide (closest # to 15% would be accurate)
tx for atypical depression (first line and other)
TOC: MAOIs (monoamine oxidase inhibitor) 1st line
SSRIS (not FDA approved for this preferred because they are safer)
before starting antipsychotic medications, what do you do?
get a baseline:
EKG
Blood glucose
Lipids
BMI and waist circumference
Factitious Disorder, primary goal, another name?
mental illness is real
pain and suffering is manufactured by pt → gets taken care of (primary goal)
bona fide mental illness/somatic sx related disorder
illness anxiety disorder, when can you make this diagnosis?
SEVERE PREOCCUPATION with having a serious, undiagnosed medical illness
You can only make these diagnoses when ALL other testing has proven negative consistently
(feels pain)
FUNCTIONAL NEUROLOGIC SYMPTOM DISORDER, how to test?
NEUROLOGICAL symptoms that are found to be incompatible with neurologic pathophysiology
Testing by different methods, look for inconsistencies in PE
(feels pain)
factitious disorder - pain, psych, name, purpose of lying?
no pain, real psycho-pathology
bona fide mental illness
purpose of lying: to be treated/to be cared/pitied by medical staff
malingering - pain, mental disorder, purpose?
NO pain
deliberate manipulation
NOT a mental disorder
purpose of lying: to get something (money, comp, drugs)
does social (pragmatic) communication disorder have behavioral problems? what do they struggle with?
No behavioral problems (as we would see in Autistic Spectrum Disorder (ASD))
communication difficulties
ABC: The triad of clinical features associated with Autism:
A SOCIAL
B BEHAVIORALLY RESTRICTED
C OMMUNICATION IMPAIRED
Treatments for Autistic Spectrum Disorder, most effective
multidisciplinary support
most effective: behavioral tx (autism specialists, language path, audiologists)
remediation and psychotherapy
What is the difference between Autistic Spectrum Disorder (ASD) & Social [Pragmatic] Communication Disorder (SCD)?
ASD: struggle w social communication AND behavior
repeated/disruptive movements (flapping, rocking)
obsessive fixation on routine/rituals
putting things in order
primary sxs for ADHD (IHI)
Inattention
Hyperactivity
Impulsivity
T/F: neuroimaging is diagnostic for ADHD
F
ADHD dx
clinical
Tx for ADHD (non-pharm)
Psychotherapy: Early intervention works best; behavioral interventions should be tried first
Behavioral therapy
Social skills training
School-based interventions.
pharm tx for ADHD - when is it done, what is first line?
only when behavioral intervention insuff/cleared indicated
#1 line: CNS stimulates (ritalin, adderall, dextroamphetamine)
#2: SNRI (strattera - not a controlled substance), wellbutrin, or venlafaxine (SNRI)
advantage for strattera (ADHD)
not a controlled substance
venlafaxine MOA
increases 5HT & NE levels in the CNS
dextroamphetamine MOA
effect on DA => more DA availability
MOA of buproprion, risk?
NRDI
INC in dopamine
can lower seizure threshold
SE of CNS stimulants for ADHD
Appetite suppression,
insomnia,
dysphoria,
irritability,
VS & BP fluctuations
oppositional defiant disorder - can be defined by? what is it? how long?
Can be identified by age 3, (up to age 5)
A pattern of defiant, angry, negative behavior for >6 months
intermittent explosive behavior - identified by, definition, a “hallmark”?
Can be identified by age 6 (up to age 12)
Recurrent behavioral outbursts; a failure to control aggressive impulses.
Verbal aggressions: such as temper tantrums are followed by physical aggression toward property, animals, people
conduct disorder - definition, age, after 21?
Aggression and violation of the rights of others: bullying, threatening or intimidating others => sometimes a precursor to adult Antisocial Personality Disorder
Can be identified by age 13, (up to age 18
After 21, => antisocial personality disorder
A repetitive pattern of antisocial behavior, physical aggression, cruelty to animals, verbal abuse, violence, promiscuity, theft, deceit, lack of remorse or regret
most common cause of intellectual developmental disorders
down syndrome (Trisomy 21)
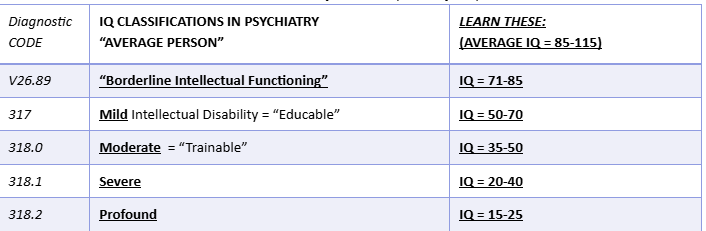
down syndrome classifications
causes of intellectual disabilities
Tay-Sach’s Disease
Phenylketonuria
Fragile X chromosome
Prader-Willi syndrome
Rett’s disorder
Lesch-Nyan syndrome
cause of tay sach’s disease (Phenylketonuria)
inborn errors of metabolism
cause of down syndrome
3 chromosome
genetic etiology of fragile X syndrome
mutation of X chromosome
genetic etiology for prader-willi syndrome?
Deletion fragment, chromosome 15
genetic etiology for rett’s disorder?
cerebroatrophic hyperammonemia
genetic etiology for lesch-nyan syndrome?
enzyme deficiency for purines
Strongest predictor of biological risk for health problems
Having a lower level of neighborhood “affluence” in childhood or adolescence
sleep wake disorder is assoc with a lack of
orexin
severity of a personality disorder depends on 3 things
Frequency (of the manifestations), intensity, and duration
Styles → Traits → Disorders
Cluster A (ODD & Eccentric): PSS (personality disorder)
Paranoid PD
Schizoid PD
Schizotypal PD
Cluster B (dramatic, emotional, unpredictable, erratic): BAHN (personality disorder)
Borderline PD
Antisocial PD
Histrionic PD
Narcissistic PD
Cluster C (anxious, scared, fearful): DOA *personality disorder cluster)
Dependent PD
Obsessive Compulsive PD
Avoidant PD
Paranoid Personality - SUSPECTS
S - suspicious of others
U - unforgiving and bears grudges
S - spousal fidelity questioned for cheating
P - perceives attackers
E - envious and jealous
C - cold affect; criticism disliked very much
T - trust in others is minimal, if any
S - self referential, “everything that’s going on is about me”
Schizoid Personality - DISTANT
D - detached from other with a flat affect
I - indifferent to praise or criticism, “don’t care,” nothing matters
S - sexual drive, libido very reduced
T - tasks done alone by choice
A - absence of close friends by choice
N - no emotional responsiveness
T - takes very little pleasure in doing anything
Schizotypal Personality - RECS
R - reduced capacity for love or close relationships
E - eccentric behavior marked; identifiable to anyone
C - cognitive and perceptual “magical” distortions, severe and prominent, occasional staring, threatening looks
S - strikingly odd appearance, face may appear threatening
Borderline Personality - AM SUICIDE
abandonment is extremely feared
M - mood instability
S - suicidal/parasuicidal behaviors, mostly attention seeking
U - unstable relationships
I - impulsivity
C - control of anger/emotions extremely poor
I - intensely ambivalent relationships
D - disturbed sense of self and personal identity
E - emptiness feeling that is chronic, and can never get fulfilled
Antisocial Personality - CORRUPT
C - callous
O - others are always to blame
R - reckless disregard for others
R - remorseless
U - underhanded
P - poor planning/impulsive
T - /tendency to violate the rights of others for personal gain
Histrionic Personality - PRAISE
P - provocative behaviors
R - real concern for physical attractiveness
A - attention seeking even during solemn events (i.e. wearing red to a funeral)
I - influenced easily
S - shallow, seductive and very inappropriate
E - exaggerated emotions, egocentric and vain
Malignant Narcissism
Narcissistic Personality Disorder + Antisocial Personality Disorder
Not a formal diagnosis but a term frequently used for an extreme blended personality disorders, more dramatic, even public, destructive for everyone
Dependent Personality - RELIANCE
R - reassurance required at all times
E - expressing disagreement is difficult
L - lack of any self confidence
I - initiating conversations or projects is difficult
A - abandonment is feared
N - needs others to assume responsibilities
C - constant companionship sought
E - exaggerated fears
Obsessive-Compulsive PD - LAW FIRMS
L - loses the point of an activity or relationship due to preoccupation with detail
A - ability to complete anything is compromised due to perfectionism
W - workaholic at the expense of others
F - fussy can’t see the big picture
I - inflexible
R - rigid, unyielding even when proven wrong
M - meticulous attention to detail to the point of not getting anything finished
S - stubborn
Avoidant Personality - CRIES
C - certainty/guarantee of being liked before becoming involved with anyone
R - restriction to lifestyle in order to maintain security
I - inadequacy felt
E - embarrassment potentially prevents involvement in new activities
S - social inhibition, slow to get into relationships, shy
Adjustment Disorders
excessive emotional or behavioral overreaction to a specific life stressor, like a breakup or job loss.
The symptoms must begin within 3 months of the stressor and completely resolve within 6 months after the stressor ends.
Generalized Anxiety Disorder, pertinent negatives
•It is NOT episodic (as seen in panic disorder)
•It is NOT situation-specific (as seen in specific phobias)
•It is NOT focalized to one place or time
•It is NOT due to an underlying medical illness
•It is NOT due to substance intoxication or withdrawal
Tx for GAD - benzos?
Benzodiazepines (BZDs), for very short-term or urgent adjunct use ONLY (so to avoid *habituation, tolerance and dependence).
BZDs are NOT considered to be a first-line choice. They are useful in emergency situations or until the SSRI becomes effective
GAD - WATCHERS
W = worry,
A = autonomic hyperactivity
T = tension in muscles/tremors
C = concentration difficulty/chronic aches
H = headaches/hyperventilation
E = energy loss
R = restlessness
S = startles easily/sleep disturbance
panic attack - how long does it last?
only one SYMPTOM of a “PANIC DISORDER”. It is NOT a DSM diagnosis by itself.
A panic attack is a rapid-onset episode of extremely intense anxiety that develops abruptly, usually PEAKS WITHIN 10 MINUTES and usually LASTS <60 MINUTES.
Panic Attack = Sympathetic Overdrive
panic attack symptoms
Dizziness; trembling; choking sensation; tingling in hands; sweating; shortness of breath; chest discomfort; chills or hot flashes; fear of losing control; fear of dying; palpitations; increased heart rate; nausea; abdominal distress; feeling detached from oneself (depersonalization) or feeling “unreal” (derealization)
greatest RF for panic disorder
FH
tx for panic disorder - first term and emergency?
SSRIs, first-line use and appropriate for long-term, maintenance use
Benzodiazepines for EMERGENCY USE ONLY: SHORT-TERM, ACUTE, URGENT (NOT first line)
OCD summary
anxiety disorder characterized by a combination of intrusive thoughts (obsessions) and intrusive behaviors (compulsions).
Equal in men and women
Recognize their thoughts as their own, recognize the absurdity, cannot stop themselves
if on a ceiling dose of a bzd (esp. xanax), what do you do?
move to hospital for a controlled detox and start med treatment over again
Screen for PTSD - TRAUMA
T= traumatic event (s)
R = re-experiencing the event
A = avoiding behaviors
U = unable to function, (emotional numbness)
M = more than 1 month of symptoms
A = increased arousal patterns (hypervigilance)
Acute stress disorder- symptoms occur _?
Symptoms occur within 1 month of the traumatic event and last only up to 30 days thereafter
prolonged grief disorder (PGD) tx
It should be noted that both Prolonged Grief Disorder and Major Depressive Disorder should be diagnosed if criteria for both are met.
MDD w/ tx and not getting better → check into the hx some more
Would tx MDD w/ SSRI and leave PGD to be tx with psychotherapy
ANHEDONIA
loss of interest in normally pleasurable activities. <<
One of the core symptoms of depression along with low mood (#1)
very high mood
mania
high mood
hypomania
normal mood
euthymia
low mood
dysthymia
very low mood
depression
MDD episode criteria
5 or more depressive sx for at least 2 weeks & representing a change from previous functioning.
This causes significant impairment in functioning.
One symptom must be depressed mood (NOT associated with normal bereavement)
The _ hormone influences many bodily processes, meaning that high levels can cause various symptoms that can also present in depression
T4
relationship between thyroid function and depression
Patients with thyroid disorders are more prone to develop depressive symptoms
- and –
depression may have subtle thyroid abnormalities.
High T4 (thyroxine) levels
Low T3
Blunted TSH response to TRH
risk of suicide with tx of MDD
If a patient's treatment is undertreated (not a high enough dose, wrong medication, or insufficient therapy), their risk of suicide is just as high as someone getting no help at all
suicide in women and women
Men COMMIT - suicide 3x more often than women
Women ATTEMPT - suicide 4x more often than men
suicide methods men vs. women
Men are more VIOLENT AND LETHAL; tend to use firearms, hanging
Women are more PASSIVE AND POSSIBLY LETHAL; tend to use overdose of (psychoactive) drugs, or wrist cutting (not along the course of the artery)
suicide age men vs. women
MEN: suicide rate peaks after 45
WOMEN: suicide rate peaks after 65
*Older persons attempt suicide less often, but if they do, they are more determined and successful.
spousal deaths and suicide relationship
Death of a spouse increases risk of suicide PROFOUNDLY
For women, having young children at home is protective against suicide; BUT this is not true for men
If someone shares this information with you then take the time to truly speak with them
MDD notes
66% of depressed patients have serious suicidal ideation
As energy improves with treatment, patients can become MORE suicidal.
An untreated depressed episode lasts ~10-11+ months
80% of patients have a 2nd episode within the first 6 months
Average number of major depressive episodes in a lifetime is 5
With each successive depression, the treatment becomes increasingly difficult.
in Twin studies for MDD, how many (%) is explained by genes?
50-70%
3 neurotransmitters lowered in MDD
norepinephrine
serotonin (5HT)
dopamine
noepinephrine in depression, tx
downregulated OR decreased sensitivity
low levels of MHPG (the principle metabolite of NE)
tx: effexor (venlafaxine) has an noradrenergic effect (inc functional NE)
serotonin deficiency in depression, tx
low levels of 5-HIAA (serotonin metabolite) is assoc with violence, suidicide
SSRIs inhibit the reuptake of serotonin, allowing more to be available at synaptic cleft
dopamine in depression, tx
DA reduced in depression (but INC in mania)
wellbutrin has a dopaminergic effect → INC DA