Assessment & Interviewing - MIDTERM
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What is the purpose of an MSE?
provides a brief overview of all the major symptoms (e.g., mental & emotional state, cognitive functioning) a patient may be experiencing
What domains are assessed within an MSE?
respondent appearance, behavior, mood, affect, thought processes, thought content, perceptual disturbances (psychosis), cognitive processes (memory, orientation), & insight/judgement
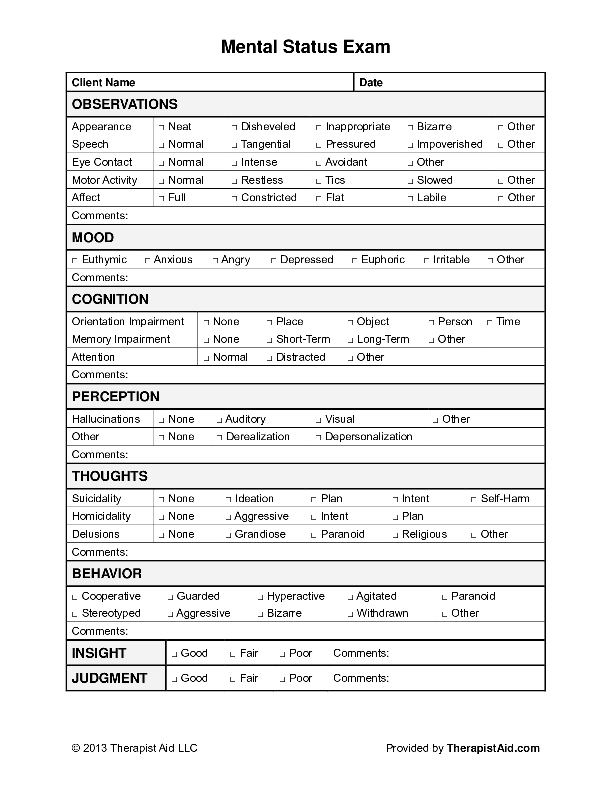
How is the information from an MSE obtained?
1) information is elicited from the respondent during the interview (responses to prompts/questions)
2) What the clinician observes about the respondent (body language, appearance)
Validity
Answers the question: Is this measure accurate?
exists on a continuum
central to validity = establishing a relevant criterion
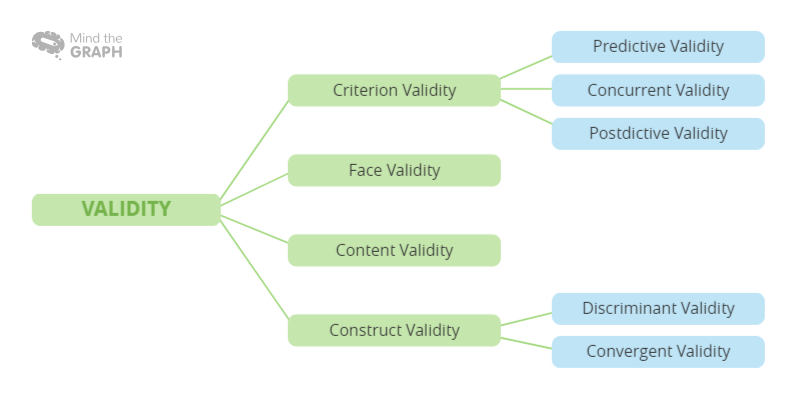
Different types of validity
Content Validity
Construct Validity
Convergent Validity
Discriminant Validity
Predictive Validity
Incremental Validity
Content Validity
the extent to which the content of an assessment tool adequately and comprehensively measures the construct or trait it is intended to assess. In other words, it assesses how well the items or questions within an assessment instrument represent the domain or content area of interest.
Construct Validity
supported via a combination of supportive qualitative evidence related to content validity and quantitative support of criterion validity
Theoretical validity - unifying form of validity regarded as a combination of content and criterion validity
Convergent Validity
addresses how well a scale correlates with other established scales measuring similar constructs at the same time. It is typically expressed using the coefficient r
Discriminant Validity
addresses the extent to which a scale does not correlate with a measure it should not correlate with
i.e., measures the “signal-to-noise” ratio of a measure
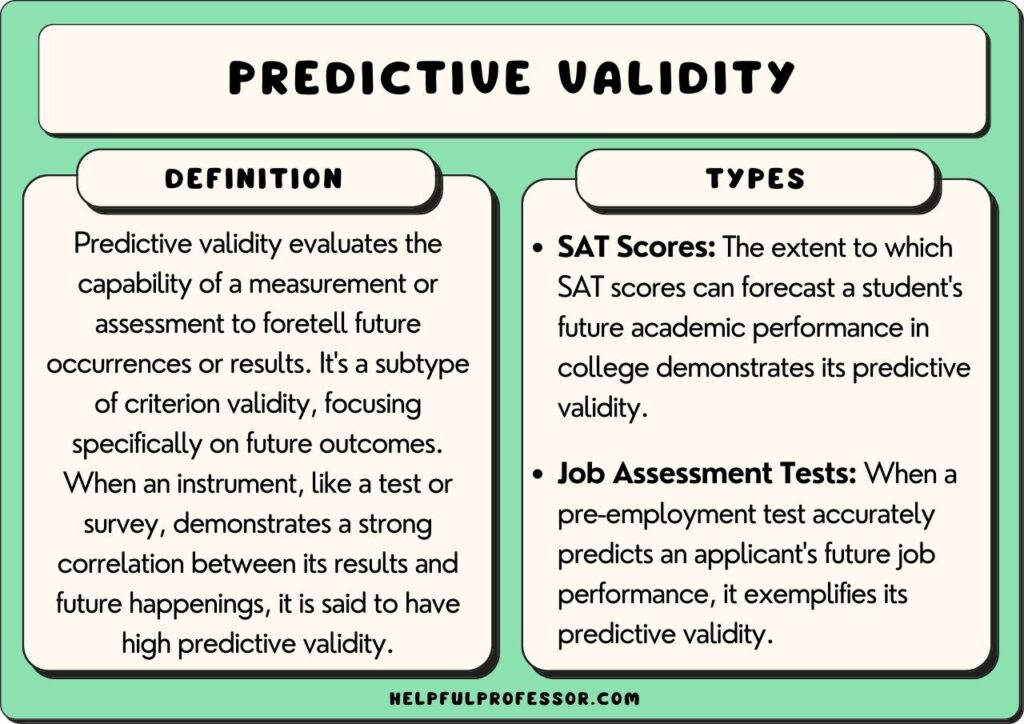
Predictive Validity
addresses how well a scale administered now correlates with some outcome in the future
measures the validity of a measure over time
criterion can be a behavioral outcome or a future measure
Incremental Validity
addresses the extent to which any additional scale contributes additional information beyond extant scales or indices to predict a relevant outcome
forces clinicians to ask: “Is this scale administering? Does it show/add something new to what is currently available?”
Reliability
consistency of results
Forms of reliability
Test-Retest Reliability
Inter-Rater Reliability
Internal Consistency
Test-Retest Reliability
the extent to which an examinee’s scores today are associated with their scores on the same test at some future time
Primarily relevant for characteristics that should be stable
High test-retest reliability over extended periods of time on symptom measures may be a red flag (e.g., depression levels should fluctuate over time, not remain stable)
Inter-Rater Reliability
the extent to which two separate raters agree on a score
Very relevant when a scale relies on some level of clinician judgment; less relevant for self-report inventories
Measured by kappa coefficient for categorical constructs and ICCs for constructs that exist on a continuum
Internal Consistency
the strength of the intercorrelation between the items in a scale
is measuring how well a measure defines a certain construct and whether or not this remains consistent throughout a measure
Low internal consistency tells you the scale isn’t tapping a single, homogenous construct
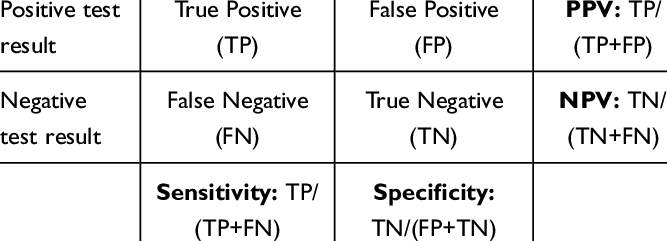
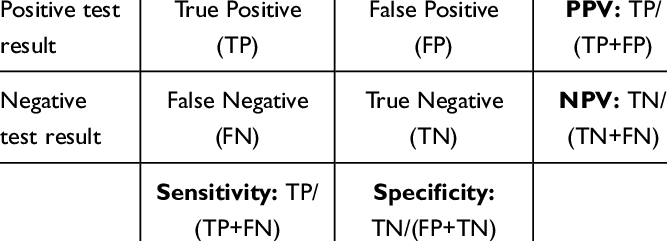
Sensitivity vs. Specificity
Sensitivity - proportion of all people who truly have a condition and are correctly identified as having it TP/(TP+FN)
Specificity - proportion of people who truly do not have a disease who are correctly identified as NOT having it TN/(FP+TN)
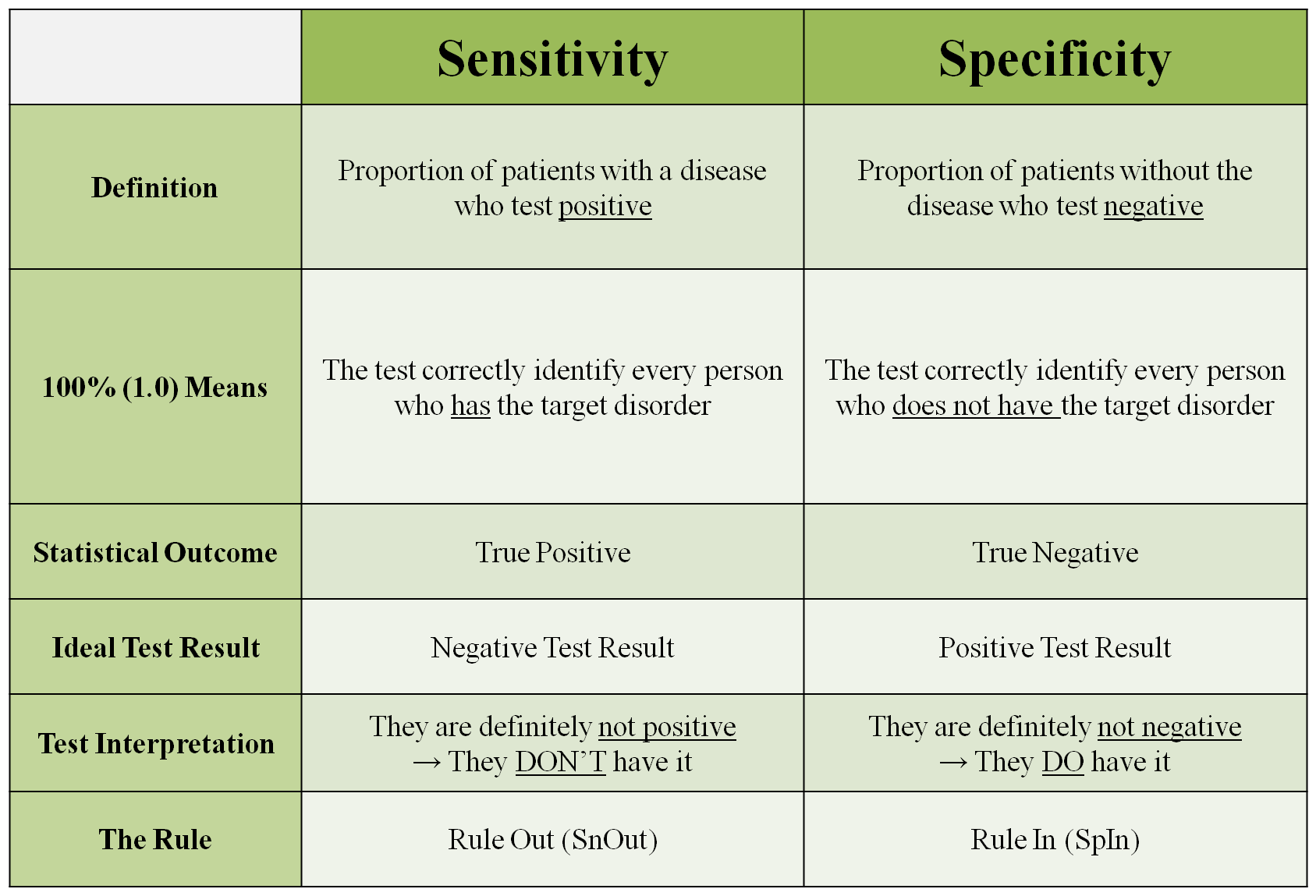
PPV vs. NPV
PPV = TP/(TP+FP)
NPV = TN/(TN+FN)
Norms
a set of standardized data that provide a basis for comparing an individual's performance on a psychological or educational assessment with the performance of a representative group of people
Norms, specific criterion-related cutoff scores, or both are needed to properly interpret a respondent’s results on a psychological assessment
Validity Generalization
the extent to which the validity evidence for a particular assessment tool or test can be applied to different populations or situations beyond the specific group for which the test was originally developed
Clinical Utility
practical value and usefulness of an assessment measure or instrument
test materials vs. test data
9.04 Test data refers to raw and scaled scores, client/patient responses to test questions or stimuli and psychologists’ notes and recordings concerning client/patient statements and behavior during an examination. Those portions of test materials that include patient/client responses are included in the definition of test data.
9.11 Test materials refers to manuals, instruments, protocols and test questions or stimuli and does not include test data
you are NOT ALLOWED to disclose test materials in court. However, with a release of information, you ARE allowed to disclose test data
MMPI basics
most widely used psychological test in the world
567 self-reported true or false items
developed in 1943 to assist in psychiatric diagnosis, with validity scales embedded into the measure
MMPI Norms
original normative sample for MMPI - gathered from data in 1943
typical person part of this sample - 35 years old, white, middle class, average of 8 years formal education
original sample also included people or friends visiting loved ones in the hospital
important considerations: lack of diversity within the sample, mental status of most individuals who were part of the sample (e.g., people visiting loved ones in the hospital are usually not in the best state of mind —> could skew results)
MMPI-2 Normative Sample
accumulated data by using the 1980 census for participant solicitation
There were 7 total testing sites across several states, resulting in a total of 2,600 participants
much broader range of ethno-racial identities, ages, education levels, marital status, income levels, and mental health statuses compared to original MMPI
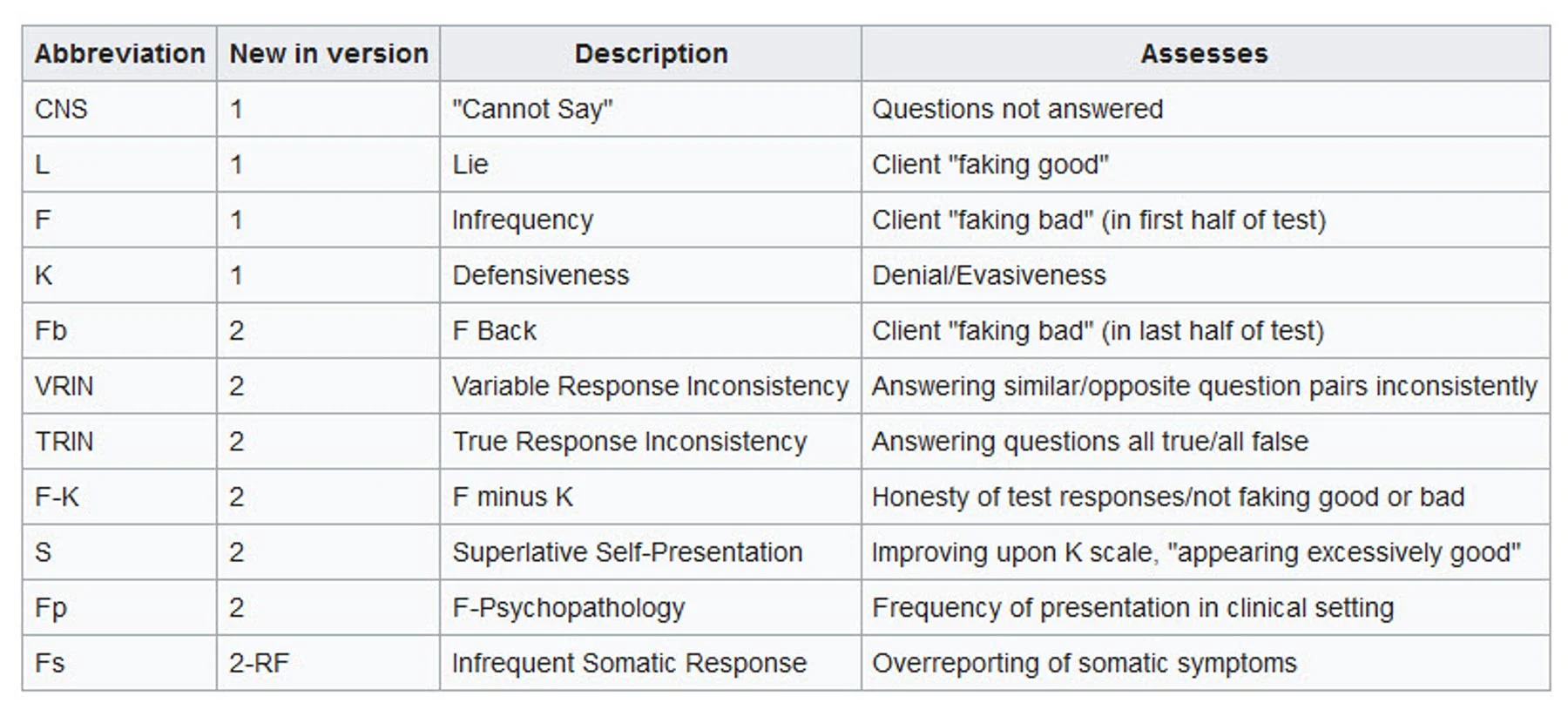
MMPI-2 Validity Scales
Cannot Say (CNS)
Variable Response Inconsistency (VRIN)
True Response Inconsistency (TRIN)
Infrequency (F)
Infrequency - Backside (Fb)
Infrequency - Psychopathology (Fp)
Fake Bad Scale (FBS)
Lie (L)
Correction (K)
Superlative (S)
MMPI-2 Cannot Say (CNS) Validity Scale
measures the number of items an individual fails to answer
high number of unanswered questions may indicate confusion, refusal to respond, or carelessness
MMPI-2 Variable Response Inconsistency (VRIN) Validity Scale
Evaluates inconsistent responding to pairs of items with similar content
can identify individuals who may be responding randomly or inconsistently
MMPI-2 True Response Inconsistency (TRIN) Validity Scale
Assesses inconsistencies in responding to pairs of items that are opposite in content but should be endorsed in the same direction (23 pairs of items that are semantically inconsistent)
can help detect individuals who answer inconsistency or indiscriminately
it reflects a tendency toward “yea-saying” (high scores) or “nay-saying” (low scores)
MMPI-2 Infrequency (F) Validity Scale
measures the frequency of rare or unusual symptoms or experiences
high scores on this scale suggest the possibility of exaggeration of psychological symptoms
MMPI-2 Infrequency - Backside (Fb) Validity Scale
Aimed at identifying individuals who might be exaggerating or providing an overly positive portrayal of themselves on the second half of the test
MMPI-2 Infrequency - Psychopathology (Fp) Validity Scale
Focuses on the frequency of psychological symptoms and atypical behaviors
Intends to detect individuals who may be exaggerating or endorsing symptoms that are infrequent and atypical, even for people with genuine psychological issues
MMPI-2 Fake Bad (FBS) Validity Scale

Used to assess whether an individual is exaggerating or feigning psychological symptoms or problems to appear more distressed or dysfunctional than they actually are
MMPI-2 Lie (L) Validity Scale
Measures the tendency to present oneself in a socially desirable manner
High scores may indicate attempts to minimize difficulties or present a favorable self-image
MMPI-2 Correction (K) Validity Scale
Assesses self-control and interpersonal relationships
high K score indicates that the person may be defensive or trying to present themselves in an overly favorable light
MMPI-2 Superlative (S) Validity Scale
Assesses an individual’s tendencies to present themselves in an unrealistically positive light
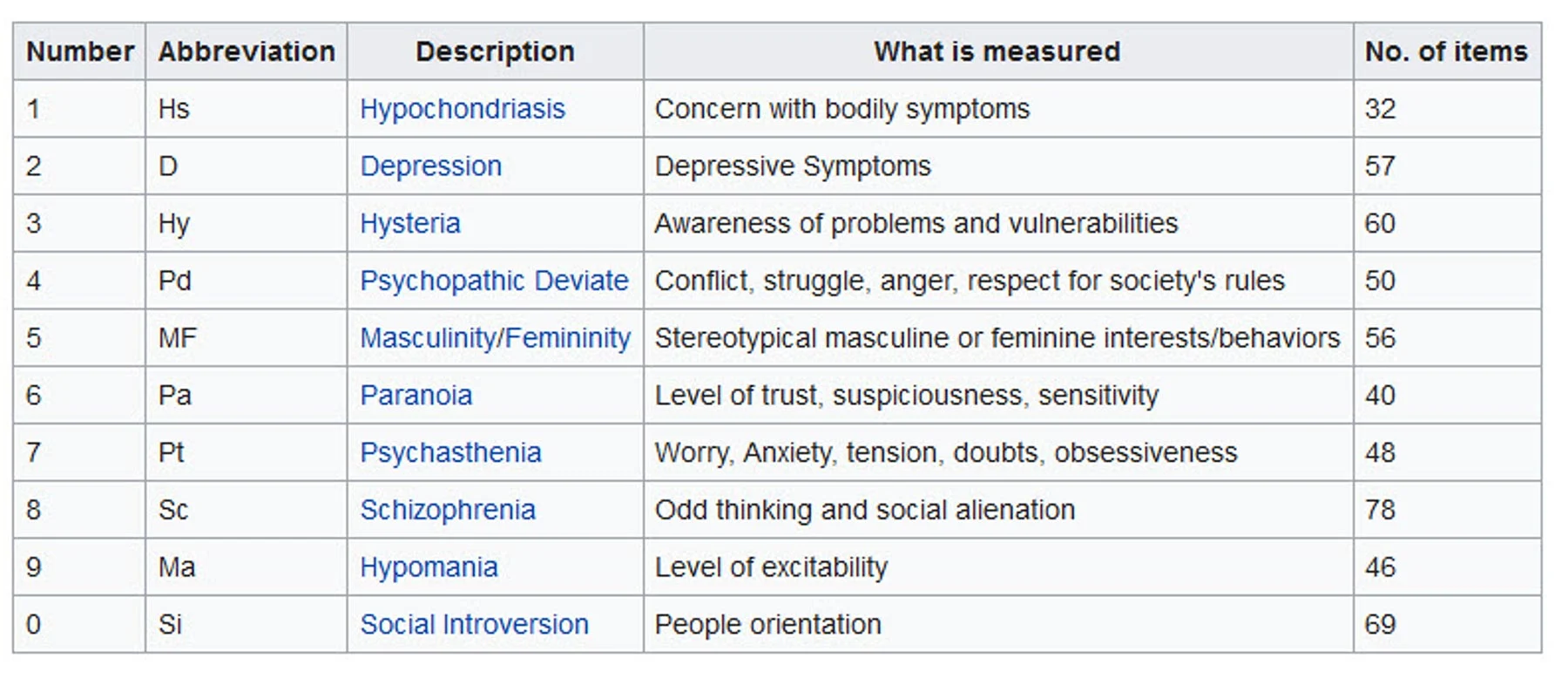
MMPI-2 Clinical Scales
Hypochondriasis (Hs)
Depression (D)
Hysteria (Hy)
Psychopathic deviate (Pd)
Masculinity-femininity (Mf)
Paranoia (Pa)
Psychasthesia (Pt)
Schizophrenia (Sc)
Hypomania (Ma)
Social introversion (Si)
MMPI-2 Clinical Scale 1: Hypochondriasis (Hs)
Measures concerns about physical health and the tendency to exaggerate or over report physical symptoms
MMPI-2 Clinical Scale 2: Depression (D)
Assesses depressive symptoms, including sadness, hopelessness, and loss of interest or pleasure in activities
MMPI-2 Clinical Scale 3: Hysteria (Hy)
Assesses emotional and psychosomatic symptoms, including anxiety, conversion symptoms, and other forms of emotional distress
commonly compared to/with scale 1 (Hs)
MMPI-2 Clinical Scale 4: Psychopathic Deviate
Assesses antisocial behaviors, aggression, and difficulties with impulse control and authority figures; measure of rebelliousness
associated with difficulty incorporating morals of society
MMPI-2 Clinical Scale 5: Masculinity-Femininity (Mf)
Measures stereotypical gender role behaviors and interests
assesses how well an individual’s self-presentation aligns with traditional gender expectations; largely not relevant today
elevated T score ≥ 65 for men = lack of stereotypical masculine interests
elevated T score ≥ 65 for women = may be rejecting traditional feminine role
MMPI-2 Clinical Scale 6: Paranoia (Pa)
Assesses suspiciousness, hostility, and mistrust of others
high T scores on scale 6, especially when it is the highest scale in the profile, indicates a potential for psychotic behavior
moderate elevations are less indicative of psychotic behavior, but more indicative of paranoid orientation
MMPI-2 Clinical Scale 7: Psychasthenia (Pt)
Measures obsessive-compulsive symptoms, such as doubts, compulsions, and excessive worrying
higher T score (≥ 70) = greater turmoil & discomfort
MMPI-2 Clinical Scale 8: Schizophrenia (Sc)
Assesses symptoms of thought disorder, social withdrawal, and perceptual disturbances
elevated T score of ≥ 75 suggest the possibility of a psychotic disorder
not all elevated scores indicate a psychotic disorder - may be in extreme emotional turmoil or endorsing deviant items as a cry for help
diagnosis of schizophrenia should not rely solely on elevated score on scale 8
MMPI-2 Clinical Scale 9: Hypomania (Ma)
Assesses symptoms related to bipolar or manic episodes, such as elevated mood, energy, and impulsivity (assesses both mania and hypomania)
moderate elevations are not likely to be associated with severe symptoms
extreme elevations = T > 80, may suggest a manic episode
MMPI-2 Clinical Scale 0: Social Introversion (Si)
Assesses introverted and socially withdrawn behavior and discomfort in social situations
low scorers tend to be sociable and extroverted
high scorers tend to worry, feel irritable, and be anxious
MMPI-2 Harris-Lingoes Scale
7 of the clinical scales are heterogeneous, meaning that there are several other factors that can elevate them
tell the clinician more about why a certain clinical scale is elevated; they should not be interpreted in isolation
general rule of thumb: if “parent” clinical scale is > 65, look to HL scales to see why it is elevated
NonContent-Based Scales within the MMPI-2
Cannot Say (CNS)
Variable Response Inconsistency (VRIN)
True Response Inconsistency (TRIN)
Positive Impression Management
Correction (K) and Lie (L) Scales
When an individual wants to appear more socially desirable, virtuous, moral, and socially responsible
Negative Impression Management
Infrequency (F), Infrequency - Backside (Fb) & Infrequency - Psychopathology (Fp) scales
When an individual wants to appear more psychologically distressed than they actually are
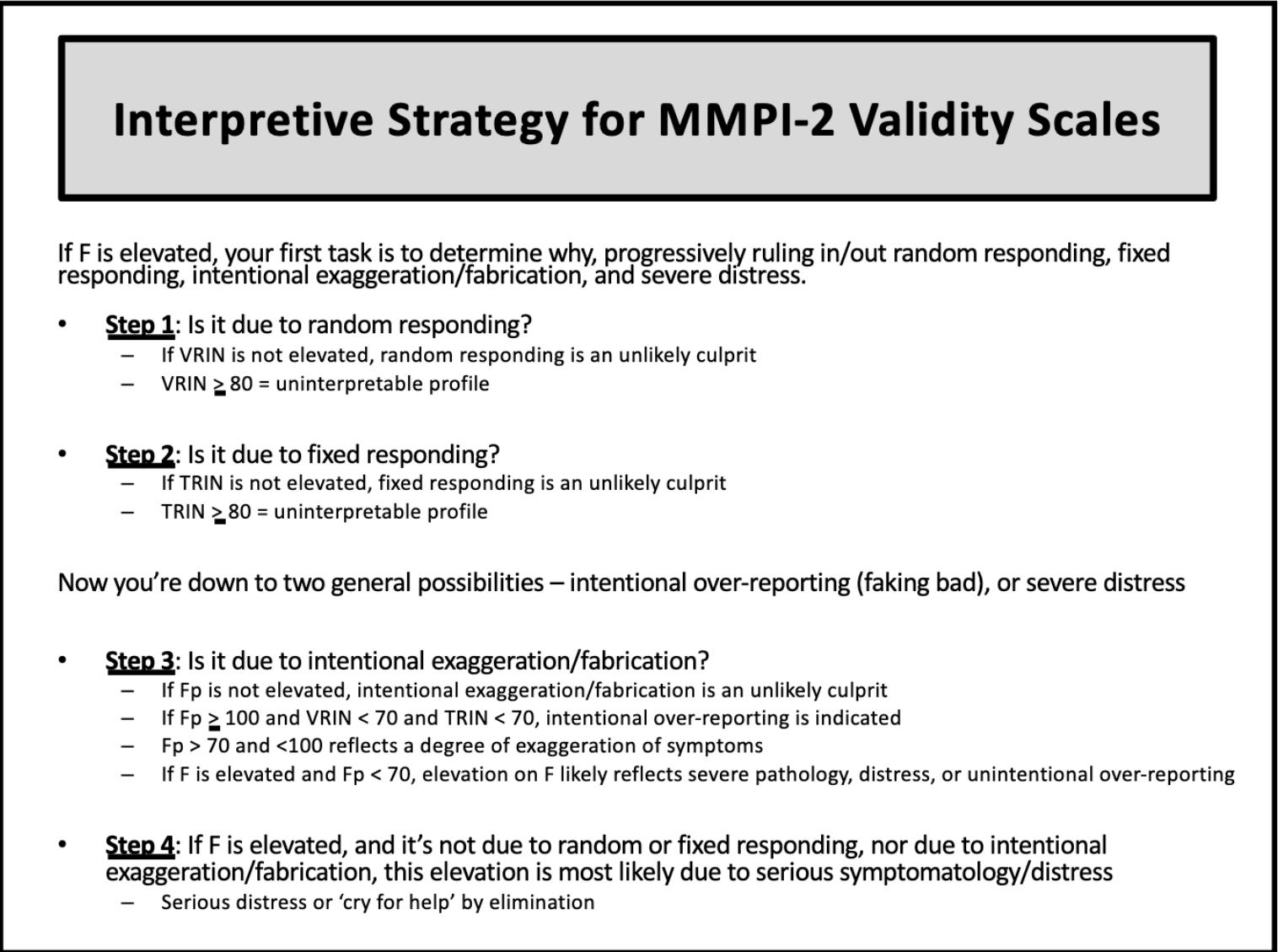
Why would an F scale be elevated on a particular profile?
If F scale is elevated → likely that an individual is exaggerating their psychological symptoms; indicates they were answering the scale in a way that does not appear to make any sense
if F is elevated → next step is to check VRIN (random responding), TRIN (fixed responding; yay or nay saying), & Fp (intentional overreporting)
F is invalid if T ≥ 120
1st step in MMPI-2 Interpretation
Check:
Lie (L)
Infrequency (F)
Defensiveness/Correction (K)
No interpretation should happen until we know how the individual approached the testing
Classical Test Theory
an individual’s “true score” is theoretical → we cannot truly know it
true score = average score after an infinite # of independent administrations
use observed score
Item Response Theory
how individual items within the test perform
avoids assumption that all items on a test will perform the same
probability that a person will endorse an item depends on:
their standing on characteristic measure
difficulty/severity of the item
Implicit vs. Explicit Referral Questions
implicit = involve unacknowledged motives for obtaining an evaluation
explicit = articulate specific motives + goals of the referral source
Test Accuracy Statistics
sensitivity
specificity
What is the average T-score for all scales within the MMPI-2?
T = 50
What is T-score indicates an elevation for all clinical scales within the MMPI?
T ≥ 65
Interpretive Strategy for MMPI-2 Validity Scales
Step 1: Check F, L, & K
Step 2: If F is elevated → is it due to random responding? → check VRIN
Step 3: If not VRIN → is it due to fixed responding? → check TRIN
Step 4: If not TRIN → is it due to intentional exaggeration/fabrication? → check Fp
Step 5: If none of the above → elevation is most likely due to serious symptomatology/distress