Week 4: Abdomen & Pelvis
1/240
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
241 Terms
Peritoneum
Serous membrane that lines the abdominal cavity
Visceral Peritoneum
The inner layer of the peritoneum that surrounds the organs of the abdominopelvic cavity
Parietal Peritoneum
The outer layer of the peritoneum that lines the interior of the abdominopelvic wall
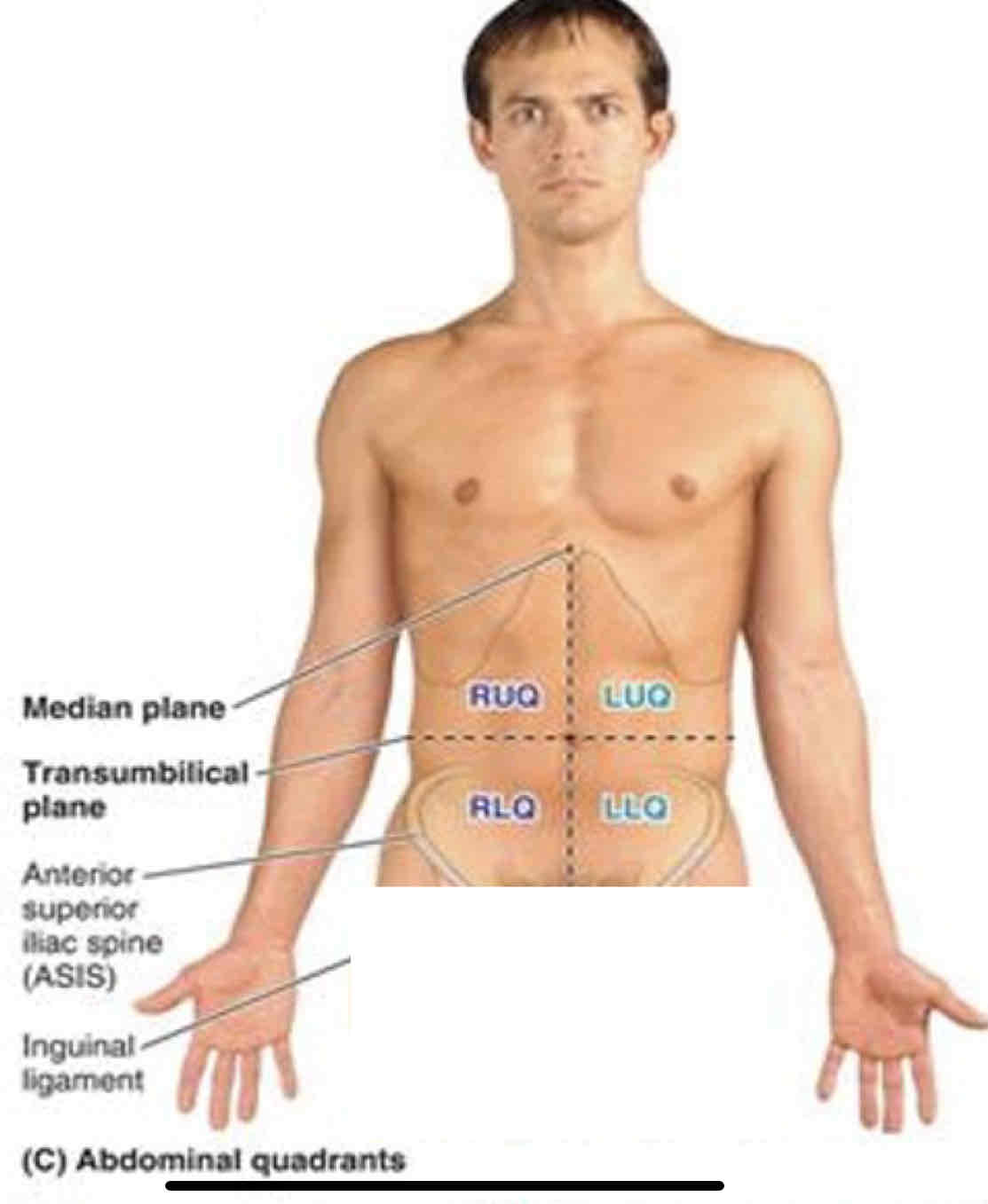
Transumbilical Plane (L3/4 disc)
Divides the abdomen into upper and lower halves
Peritoneal cavity
A potential space containing peritoneal fluid, between the parietal and visceral layers of the peritoneum. Within the abdominal cavity and continues inferiorly into the pelvic cavity
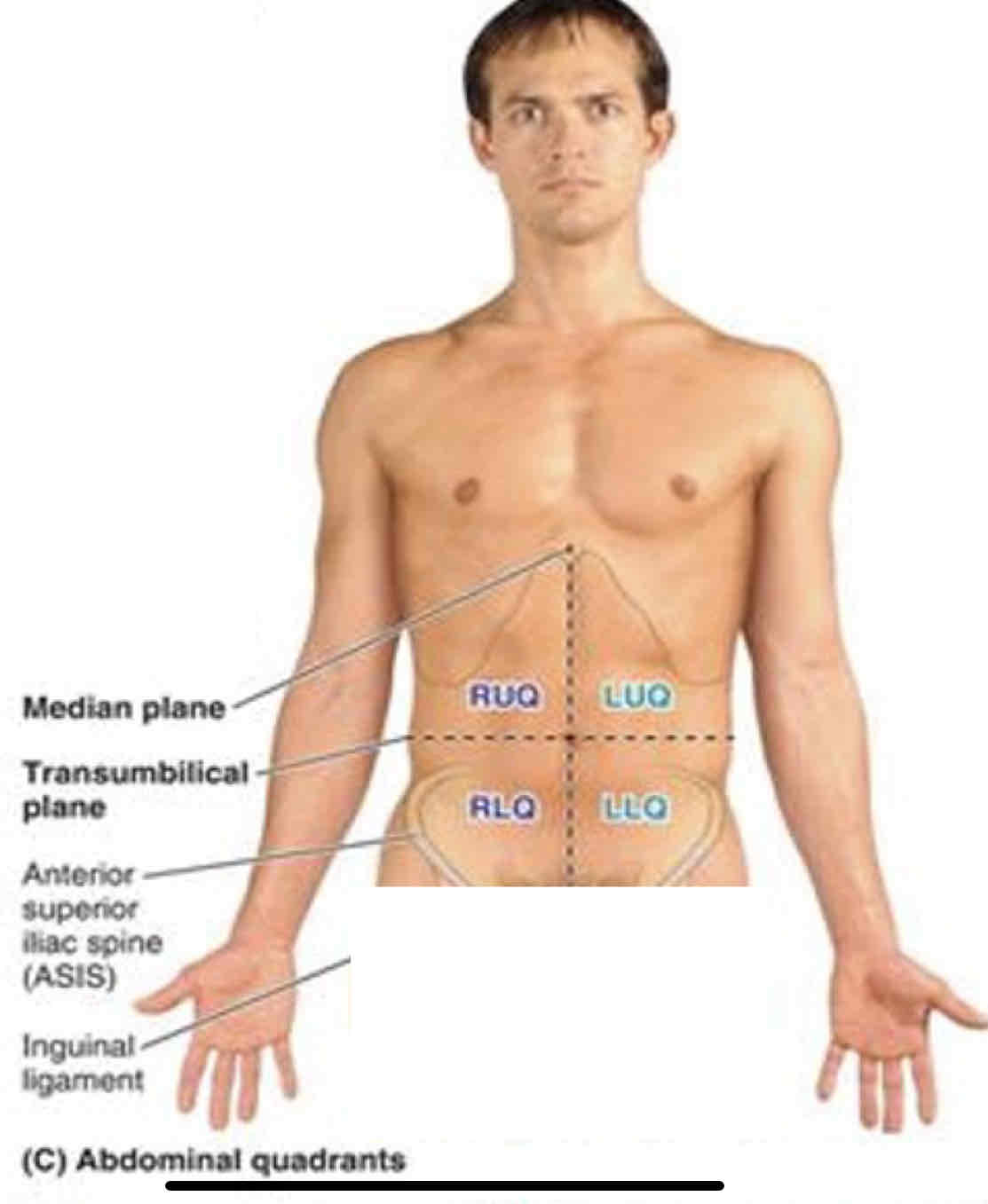
Abdominal Viscera in RUQ
Liver: Right Lobe
Gallbladder
Stomach: Pylorus
Duodenum: Parts 1-3
Pancreas: Head
Right suprarenal gland
Right Kidney
Right colic (hepatic) flexure
Ascending colon: superior part
Transverse colon: right half
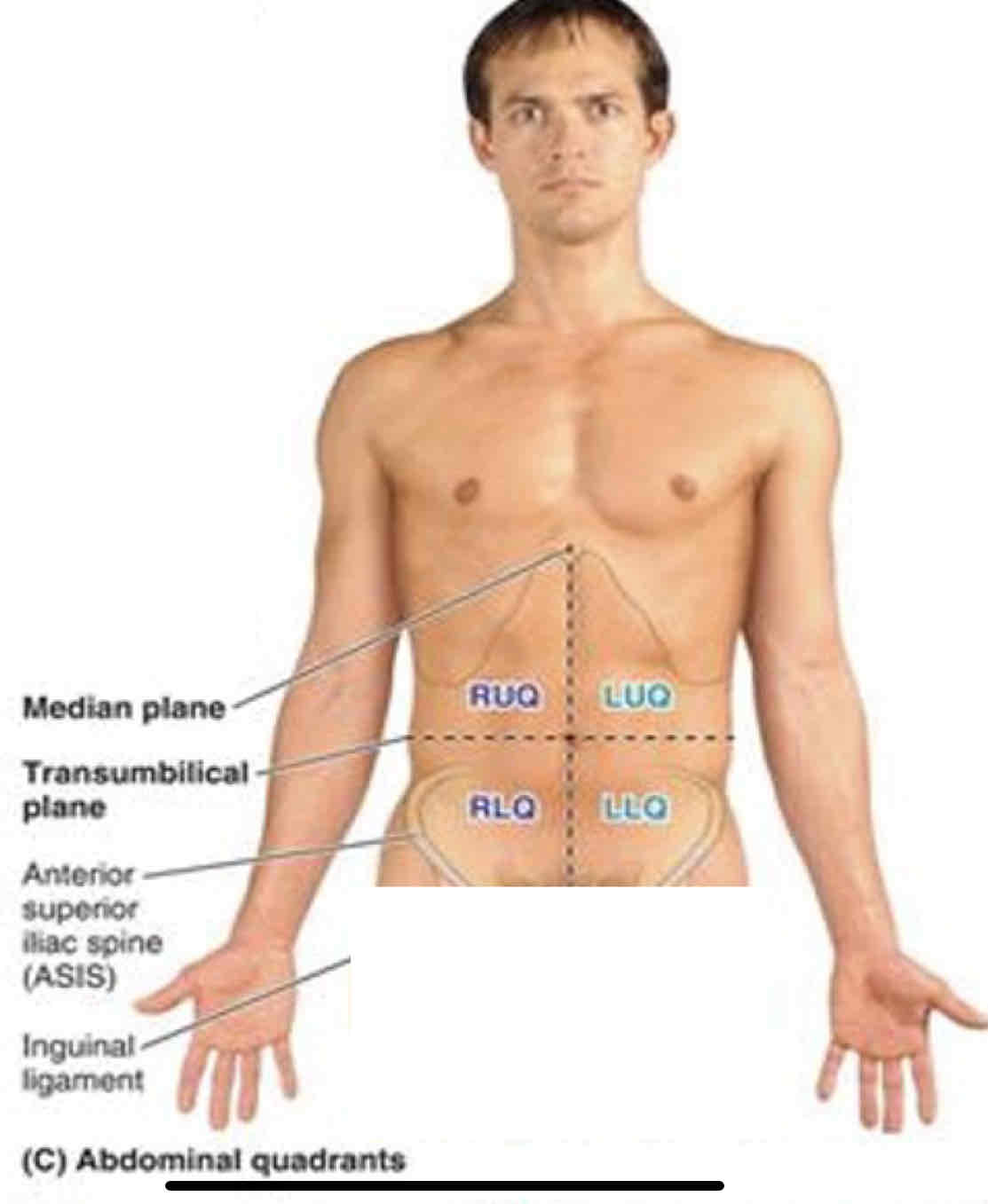
LUQ Viscera
Liver: Left Lobe
Spleen
Stomach
Jejunum and proximal ileum
Pancreas: body and tail
Left kidney
Left suprarenal gland
Left colic (hepatic) flexure
Transverse colon: left half
Descending colon: superior part
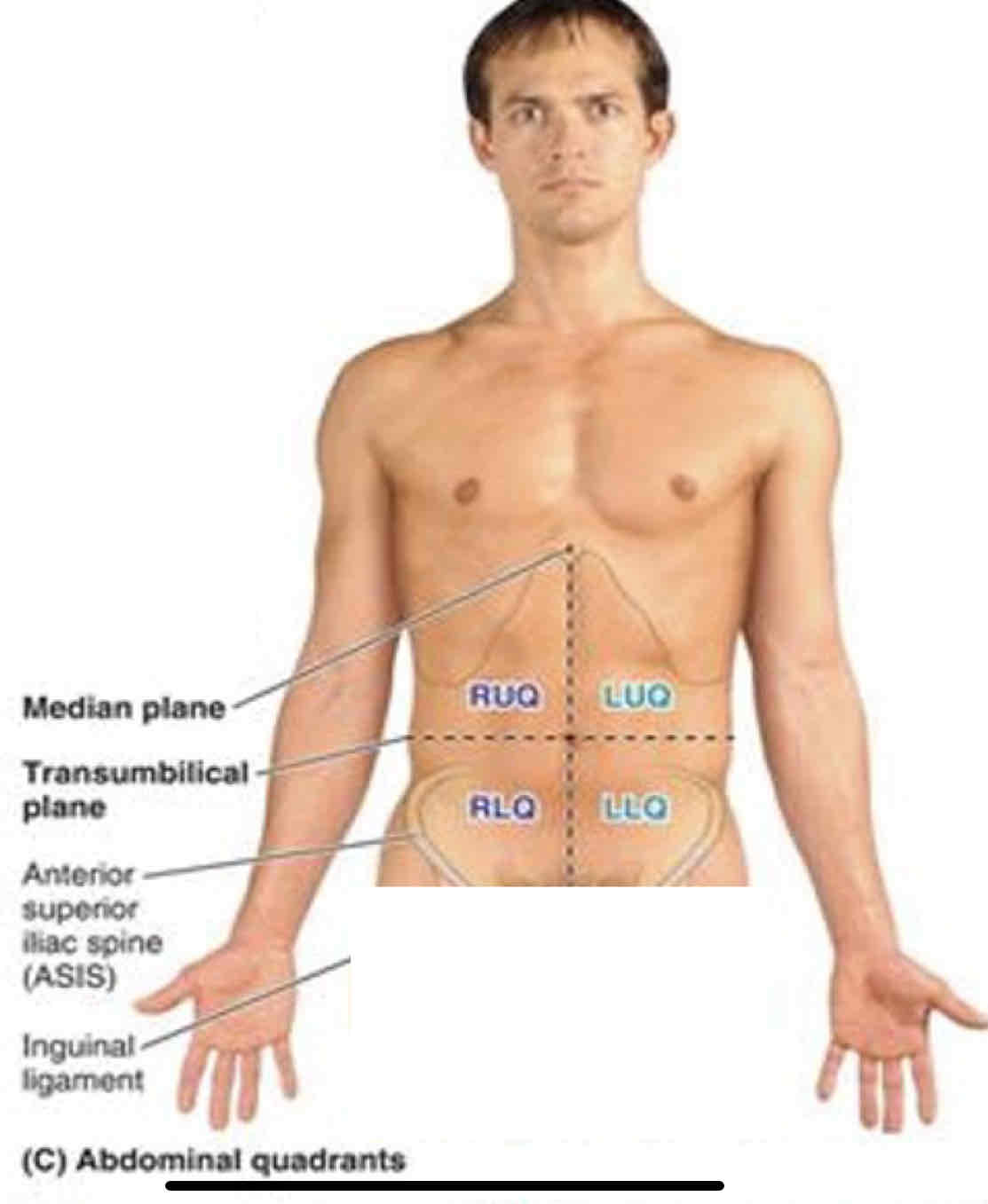
RLQ viscera
Cecum
Appendix
Most of ileum
Ascending colon: inferior part
Right ovary
Right uterine tube
Right Ureter: abdominal part
Right spermatic cord: abdominal part
uterus (if enlarged)
Urinary bladder (if very full)
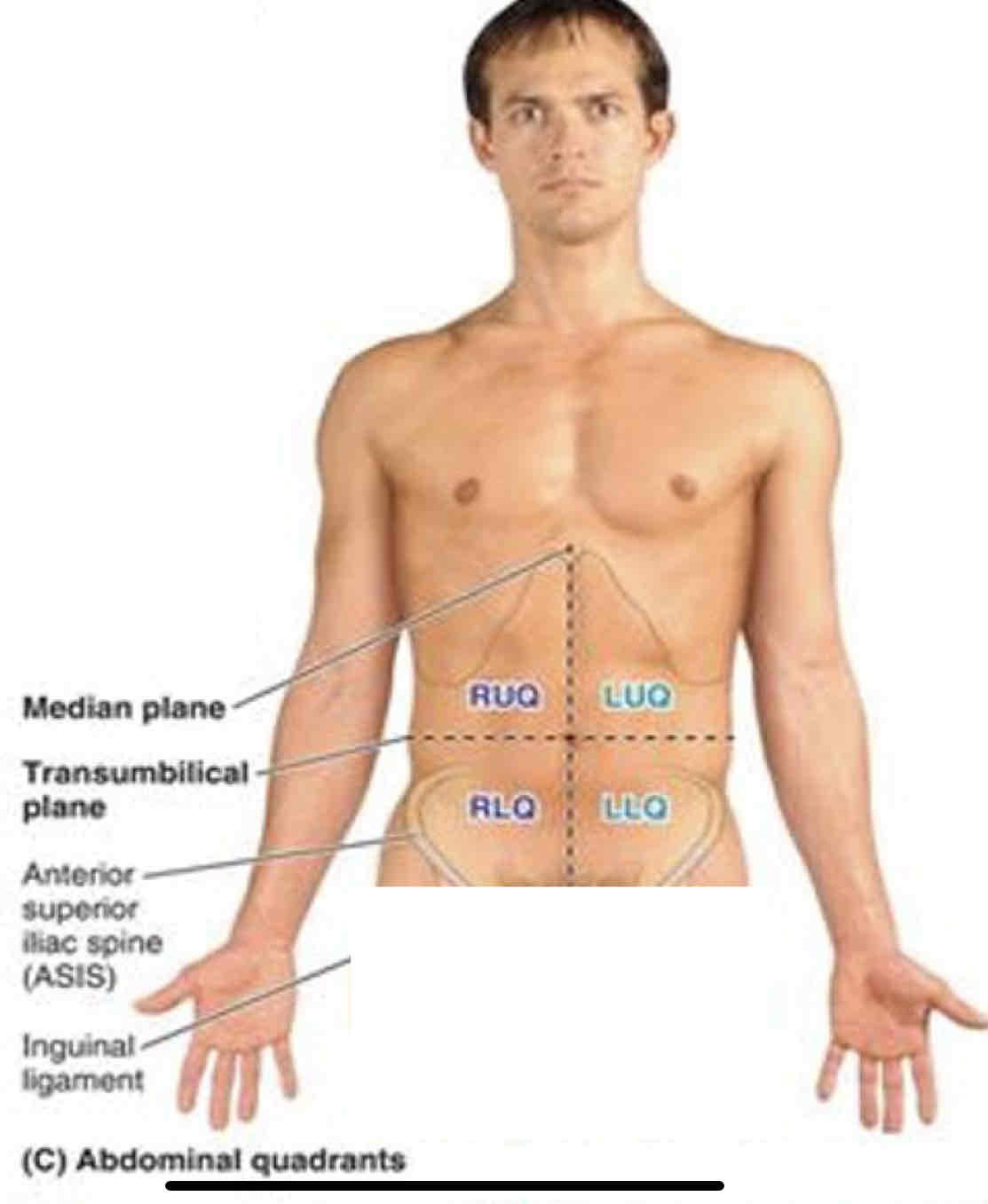
LLQ viscera
Sigmoid colon
Descending colon: inferior part
Left ovary
Left Uterine tube
Left Ureter: abdominal part
Left spermatic cord: abdominal part
Uterus (if enlarged)
Urinary bladder (if very full)
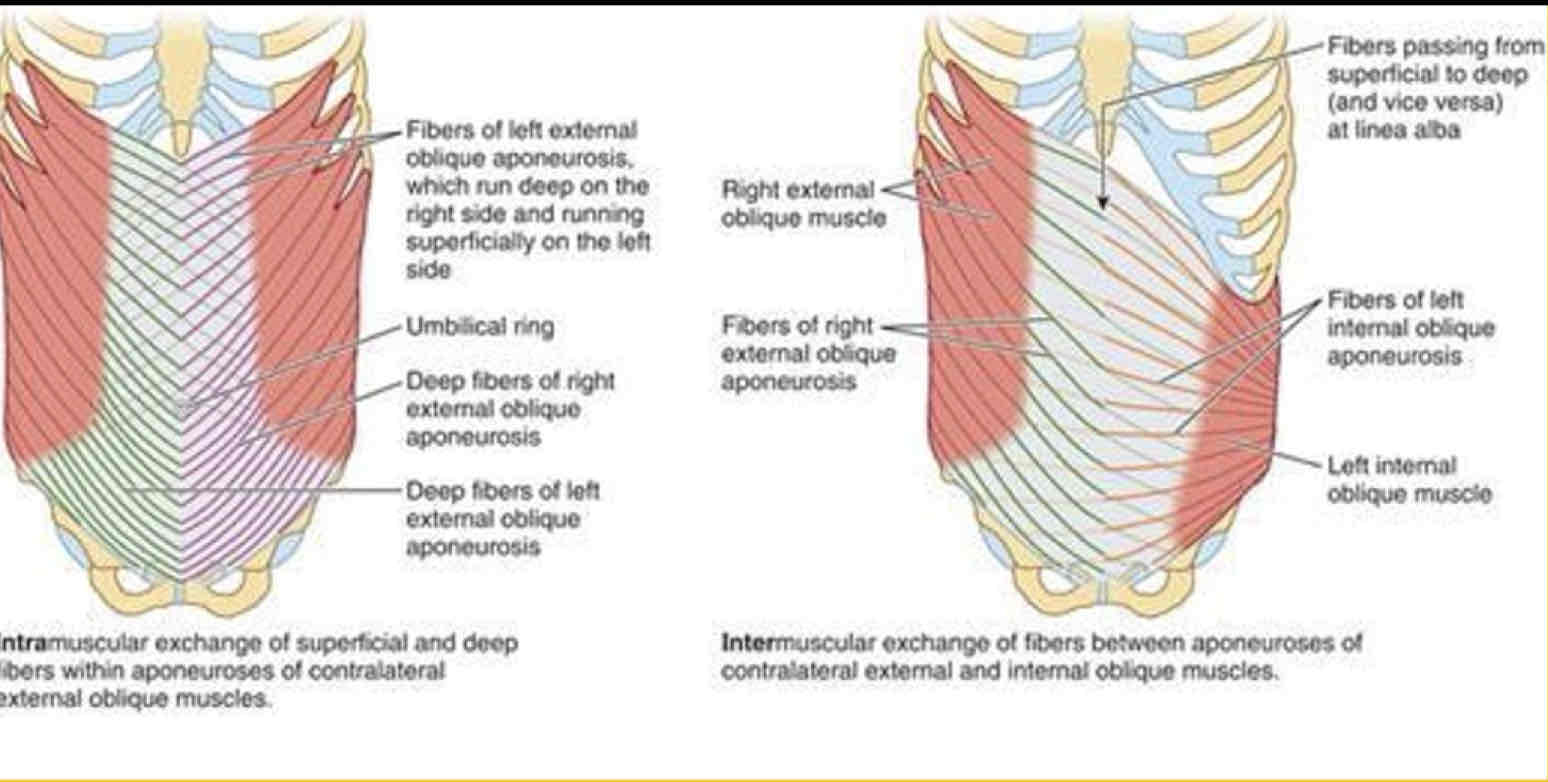
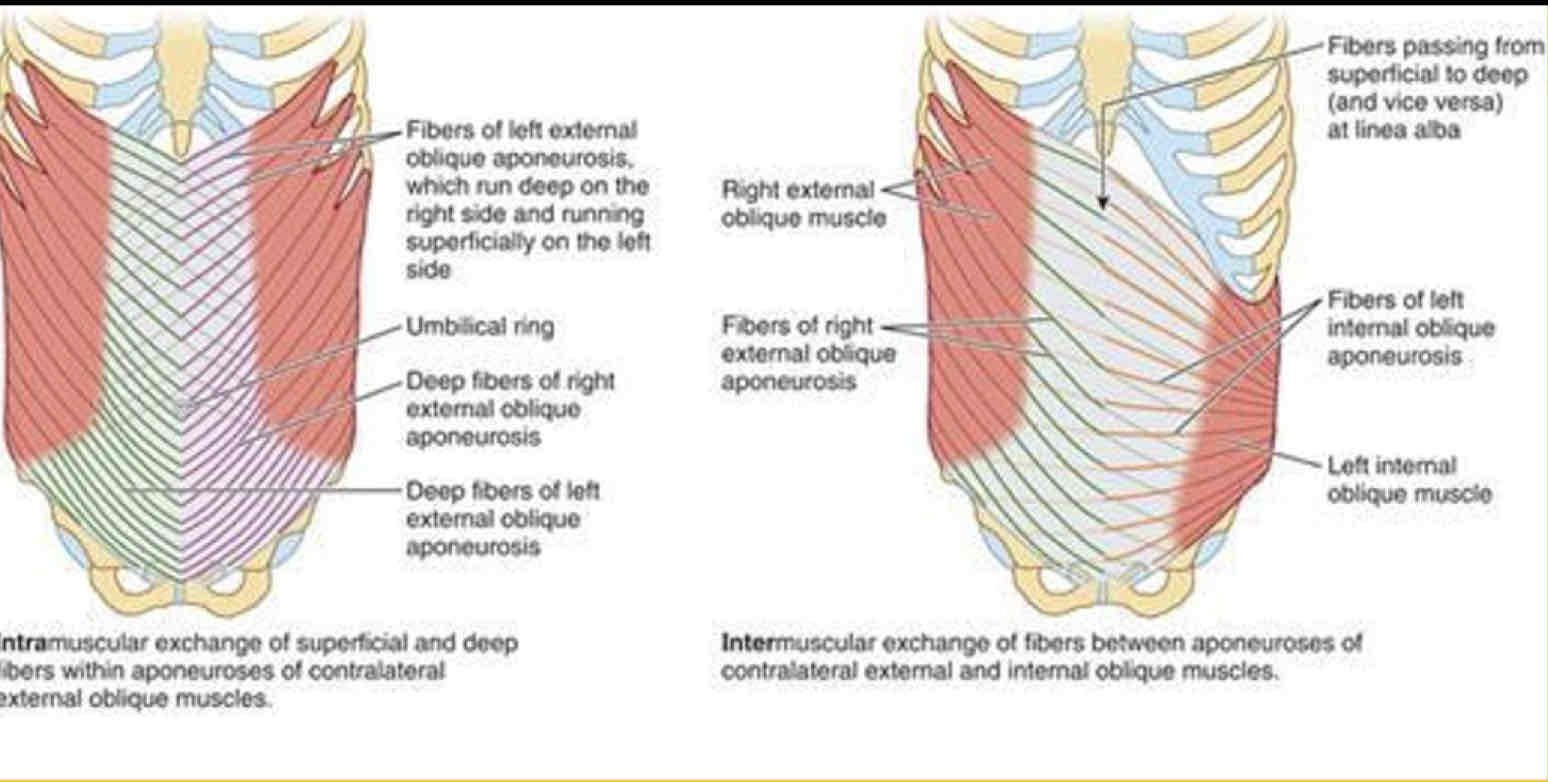
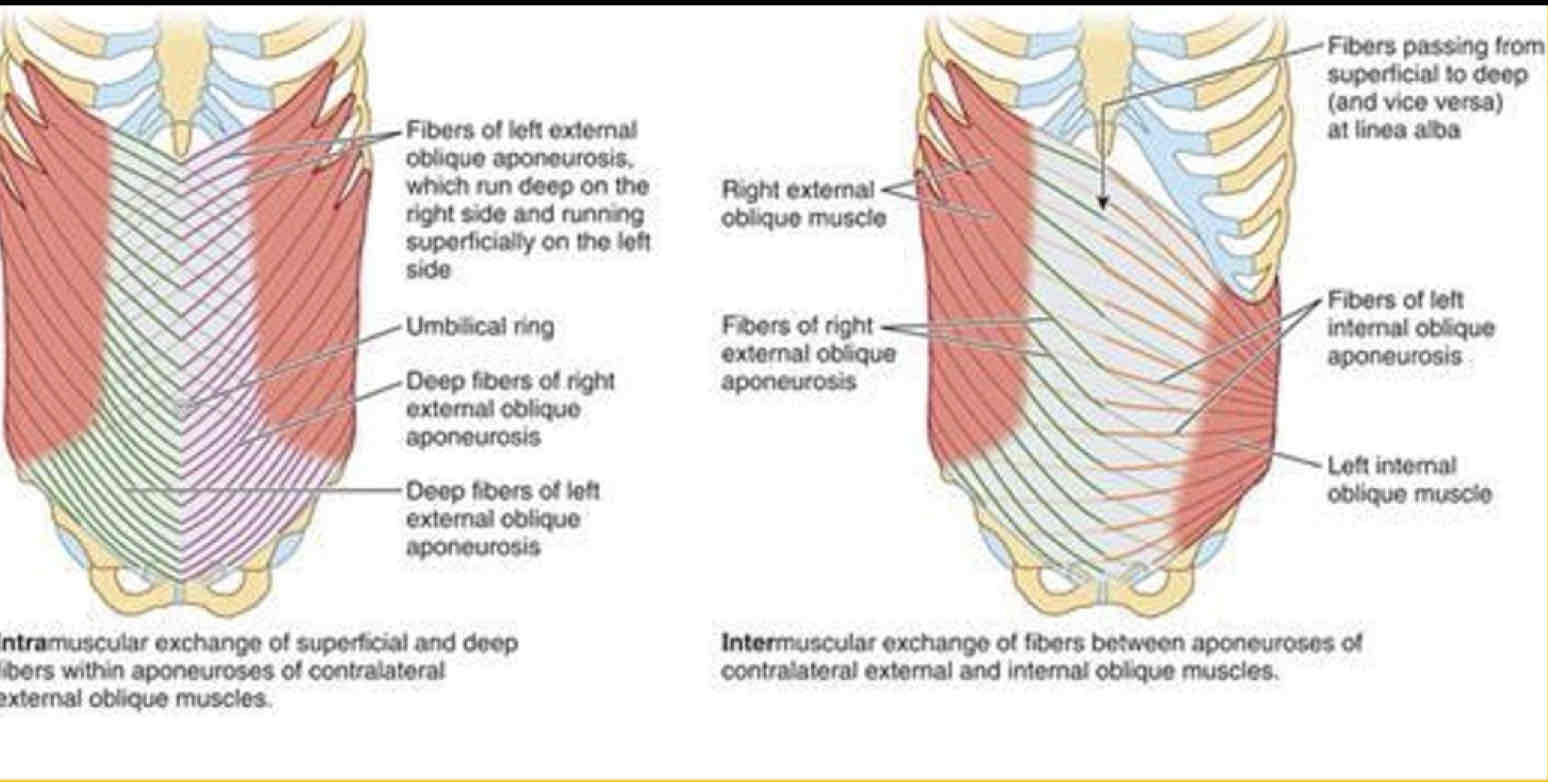
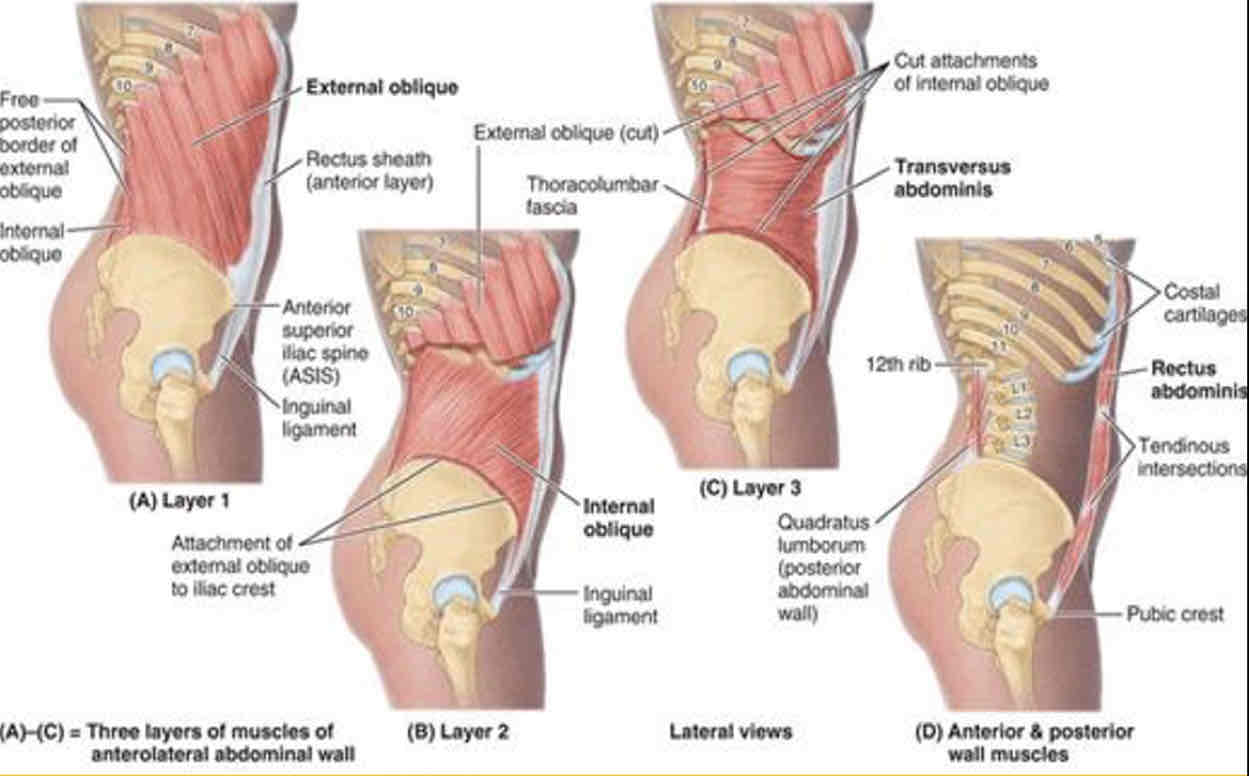
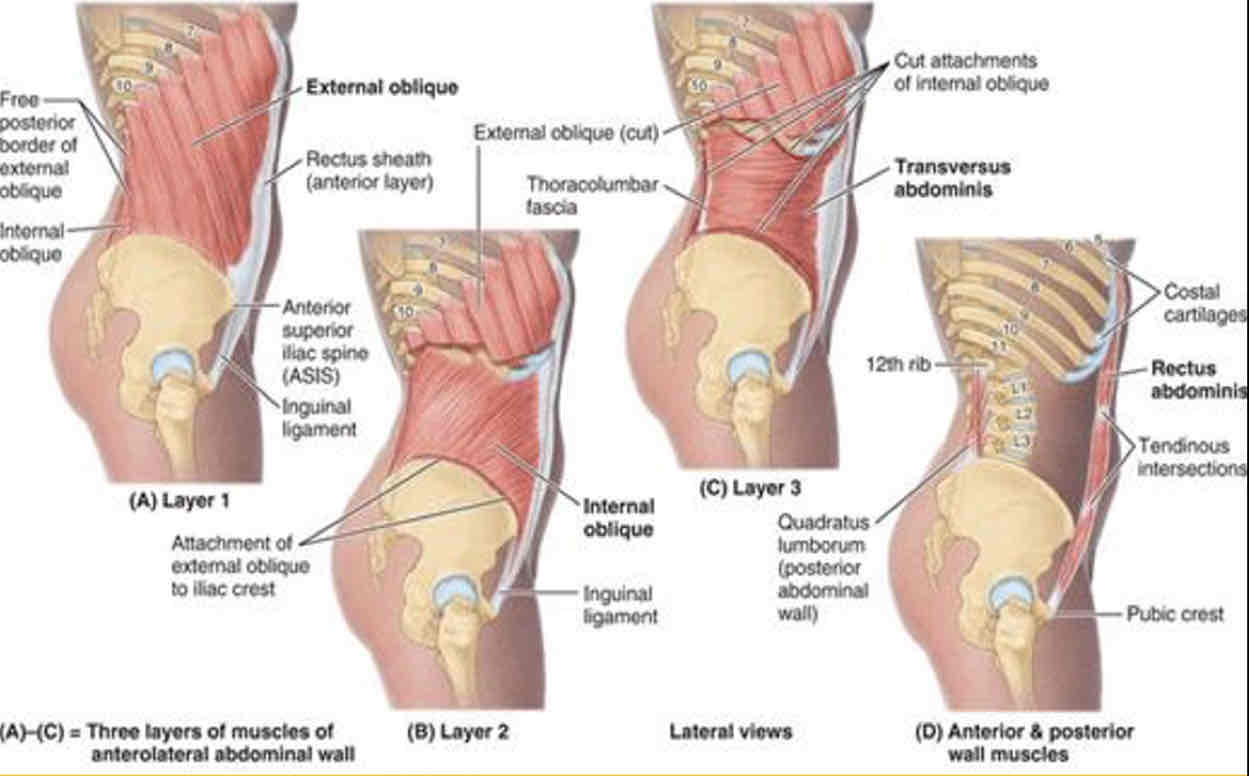
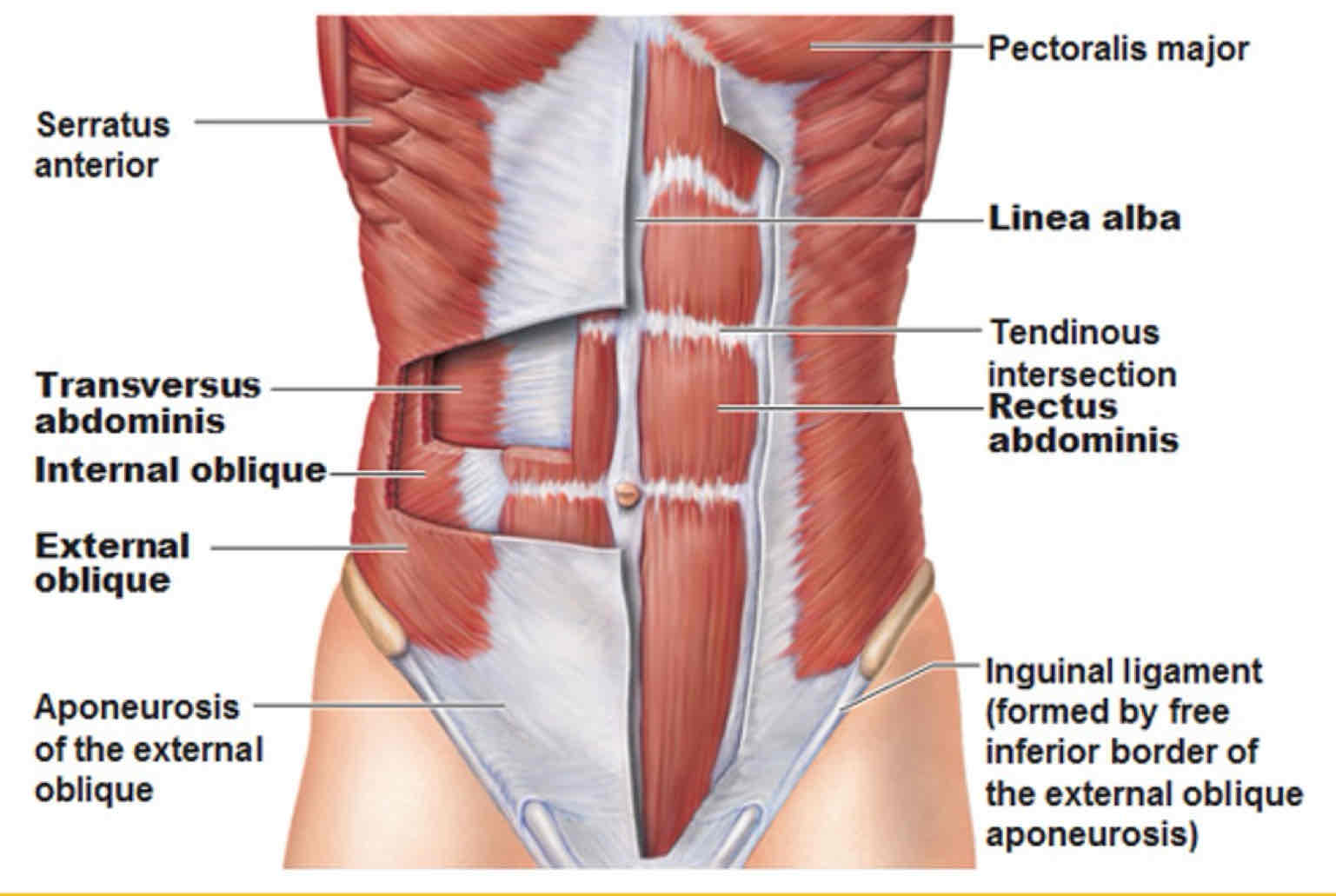
External Oblique Origin
External surfaces of 5th-12th ribs
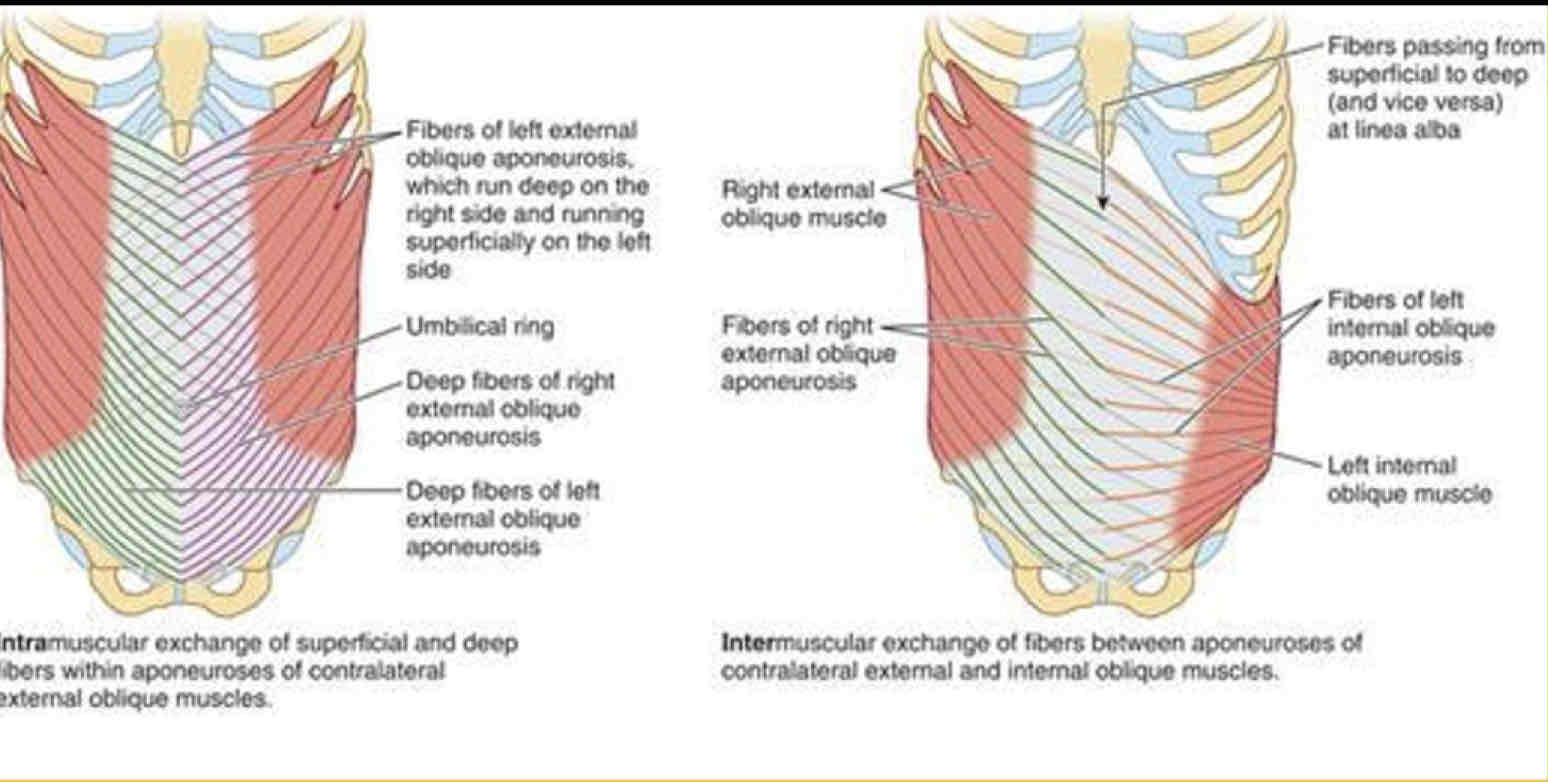
External Oblique Insertion
Linea alba, pubic tubercle, and anterior half of iliac crest
External Oblique innervation
Thoracoabdominal nerves (T7-T11 spinal nerves) and subcostal nerve
External Oblique Action
Unilateral: Trunk Contralateral Rotation
Bilateral: Trunk Flexion
Compress & Support Abdominal Viscera
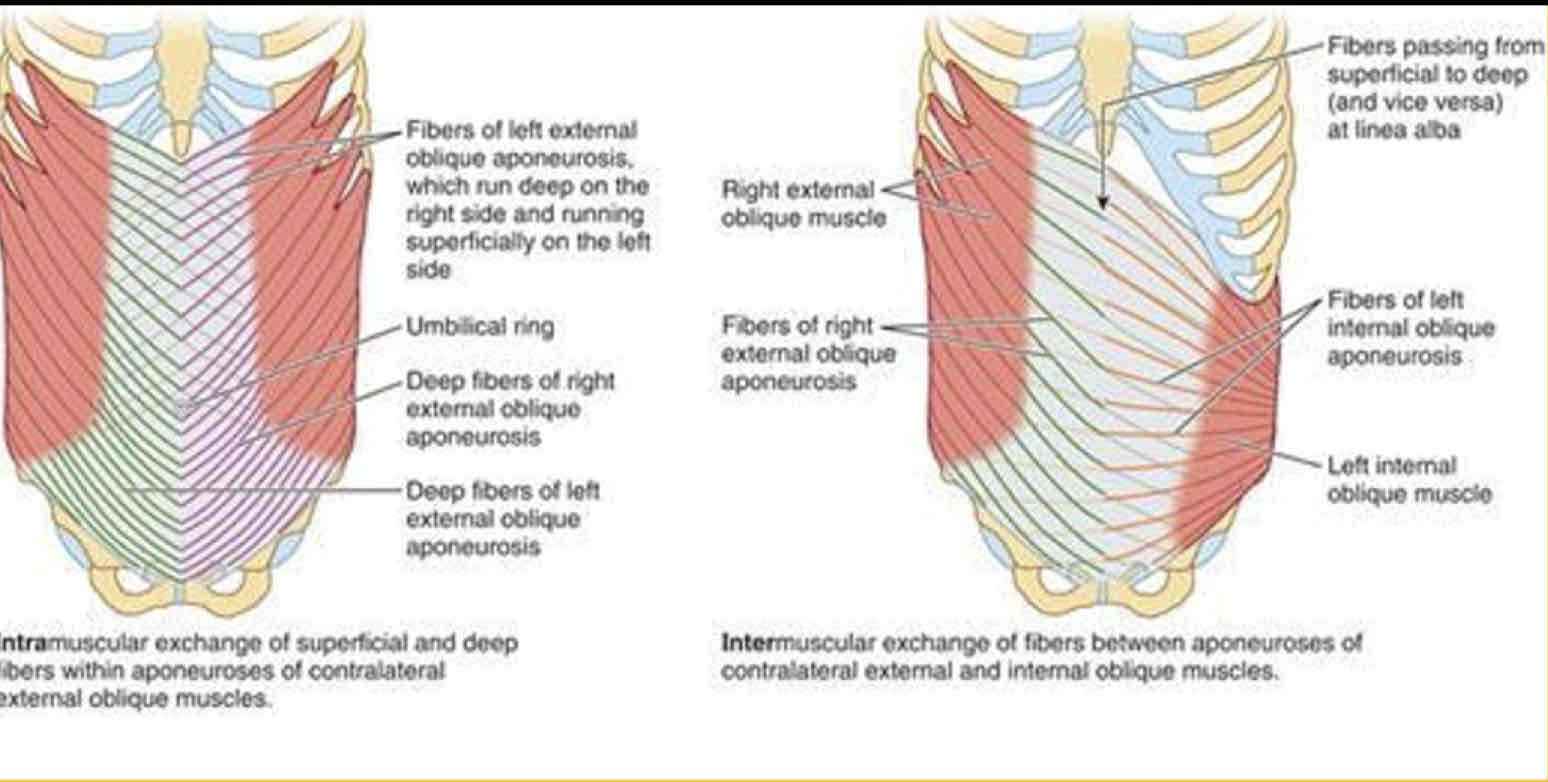
External oblique fiber orientation
Inferomedially
Internal Oblique Origin
Lower fibers: connective tissue deep to lateral third of inguinal ligament
Mid-upper fibers: Thoracolumbar fascia & anterior two thirds of iliac crest
Internal Oblique Insertion
Inferior borders of 10th-12th ribs, Linea alba, and Pecten pubis via conjoint tendon
Internal Oblique Innervation
Thoraco-abdominal nerves (anterior rami of T6-T12 spinal nerves) and first lumbar nerve
Internal Oblique Action
Unilateral: Trunk Ipsilateral Rotation
Bilateral: Trunk Flexion
Compress & Support Abdominal Viscera
Internal oblique fiber orientation
Superomedial
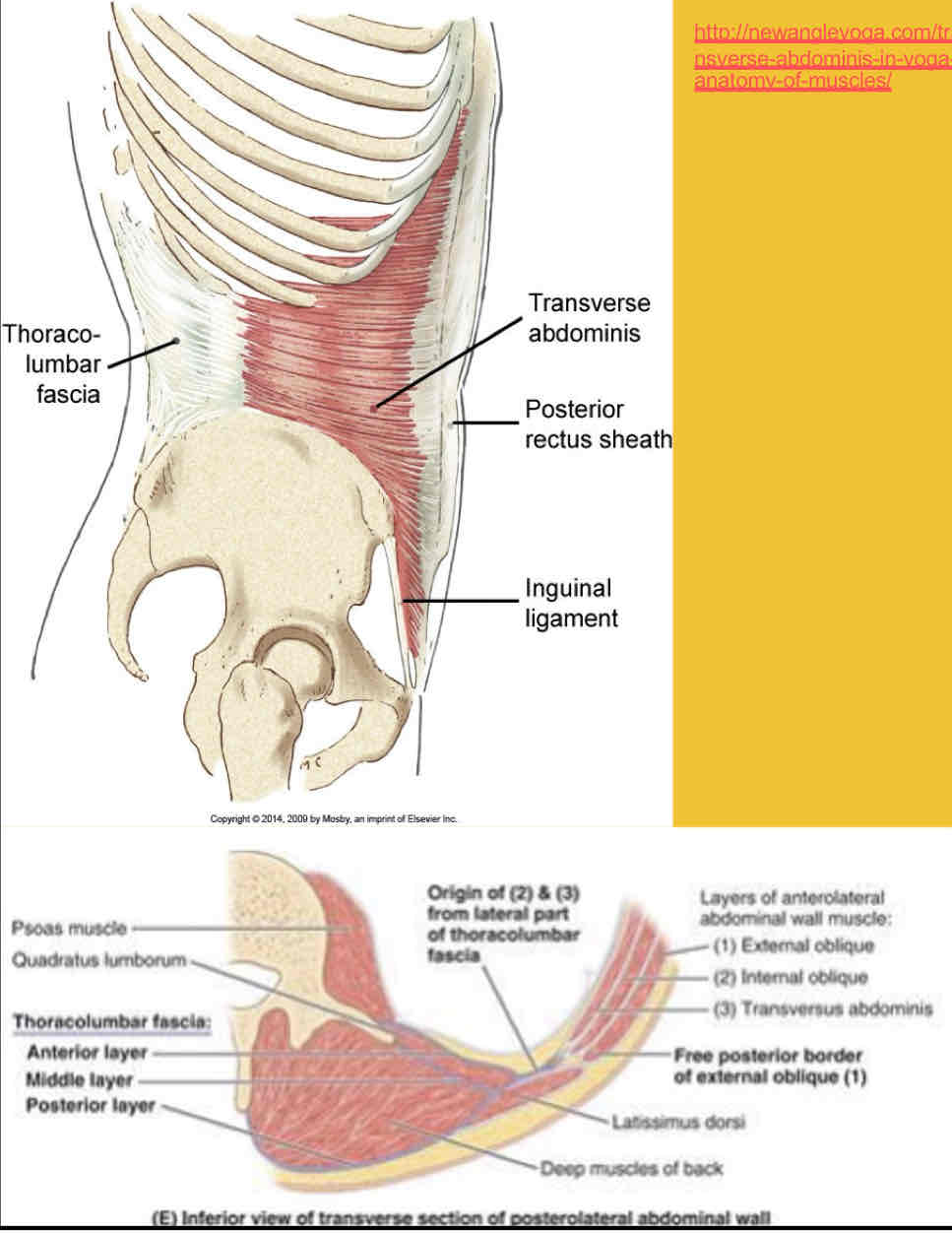
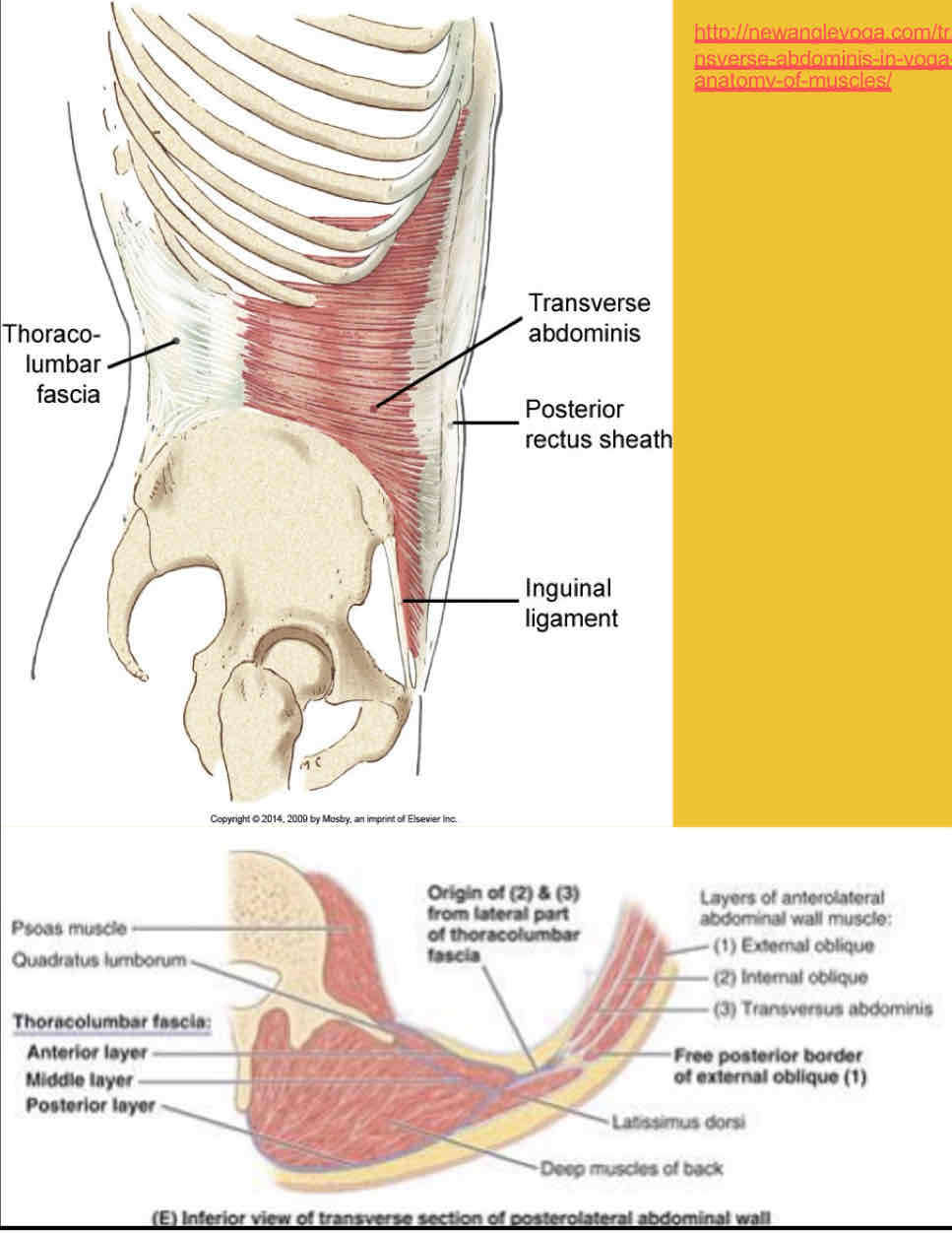
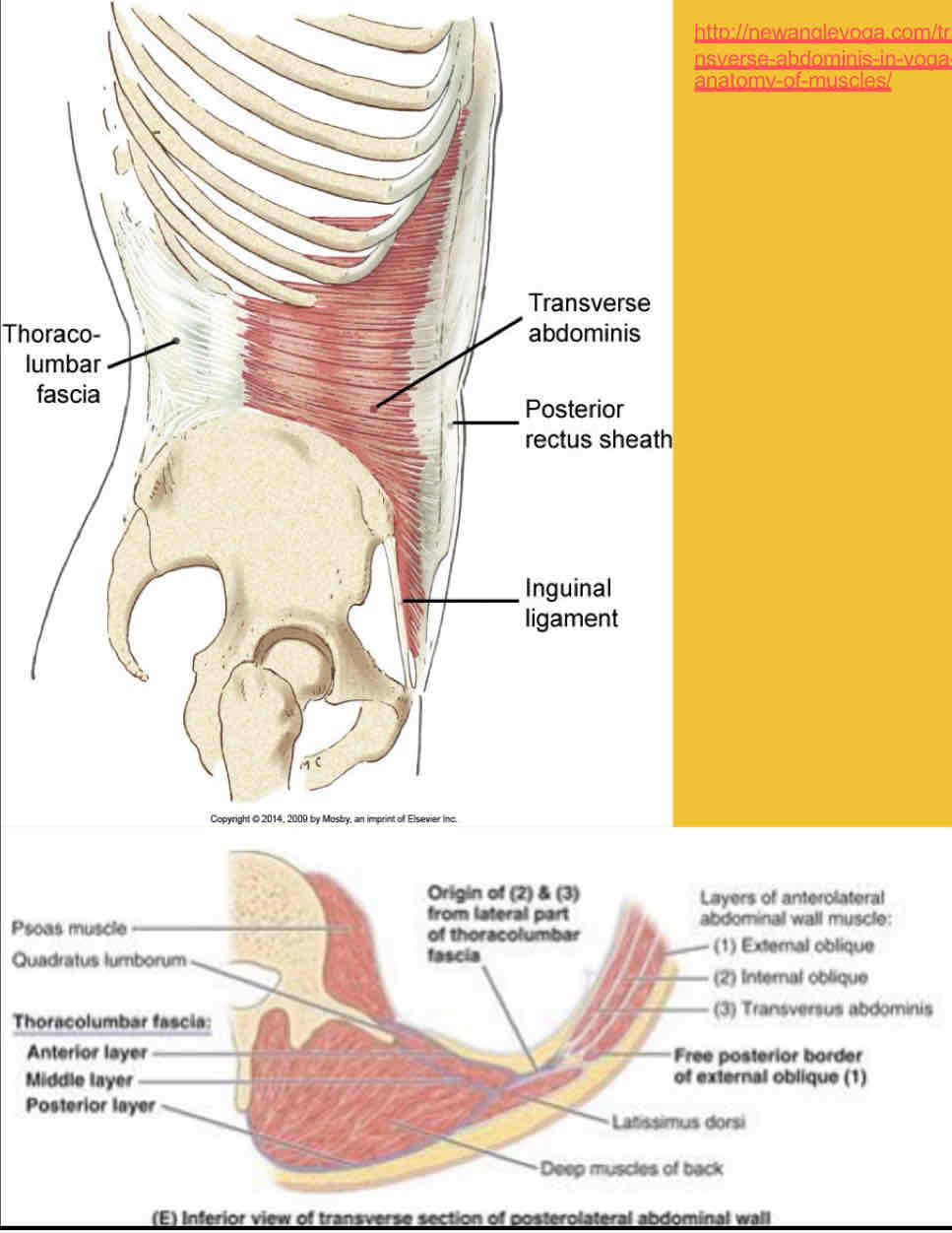
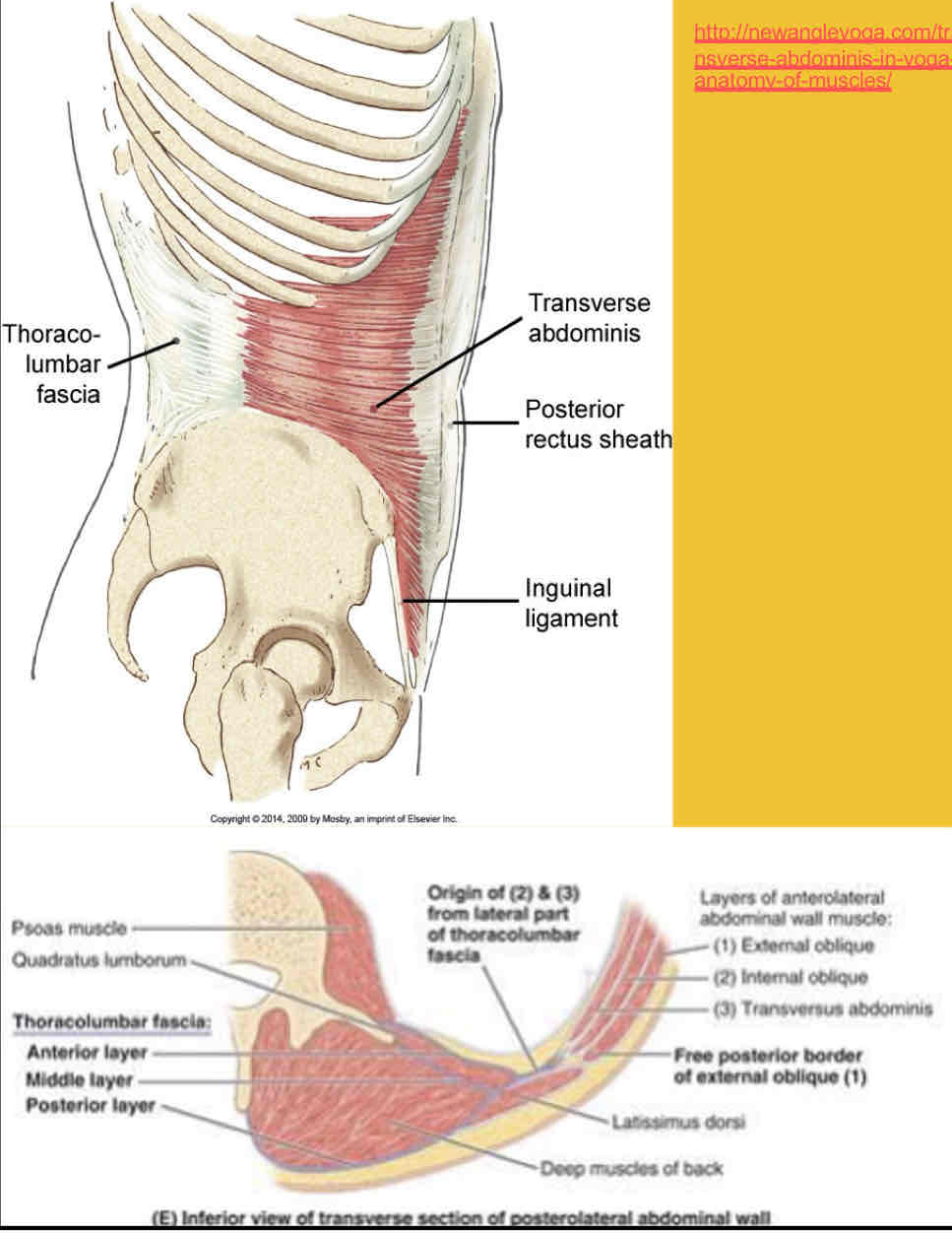
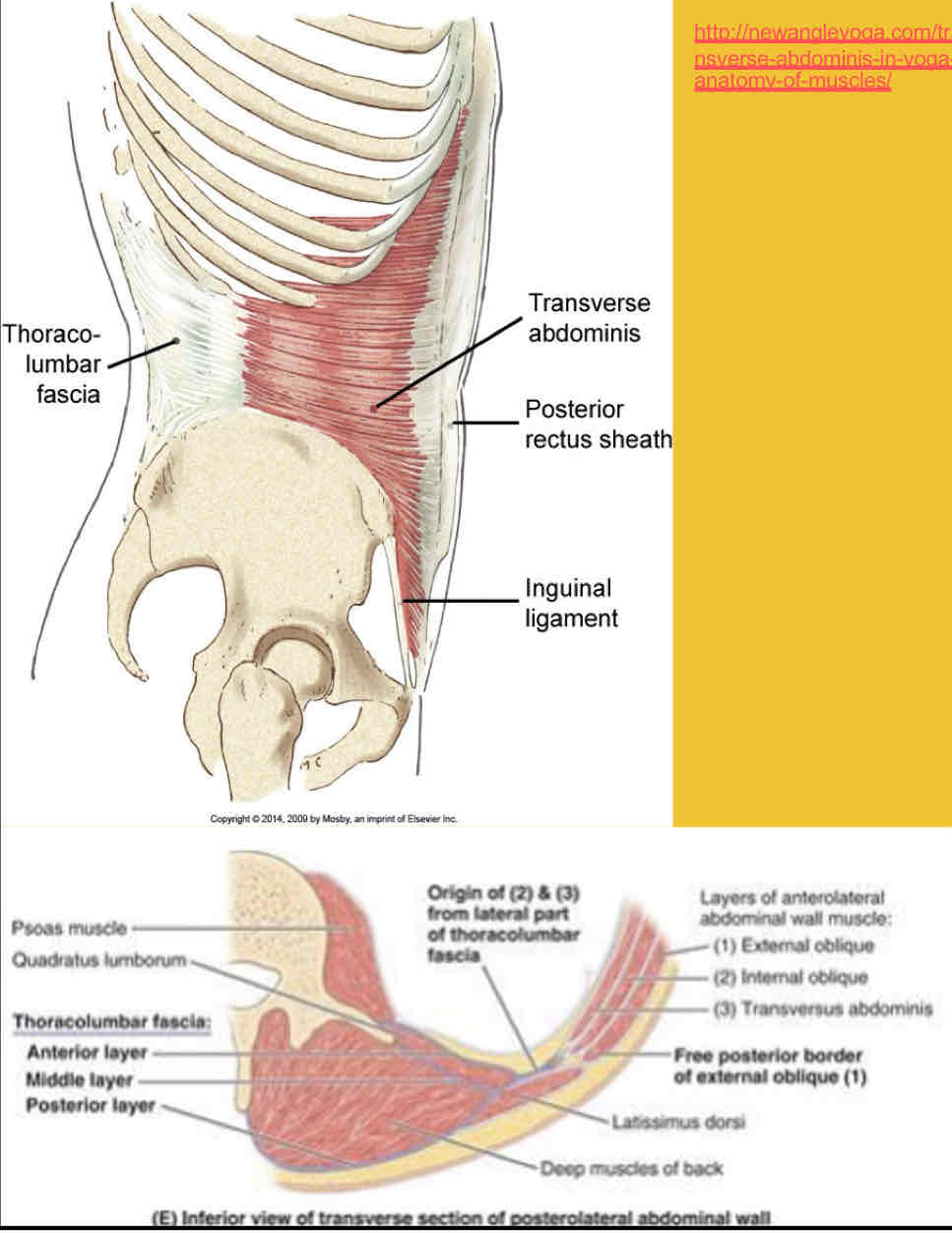
Transversus Abdominus Origin
Internal surfaces of 7th-12th costal cartilages
Thoracolumbar fascia
Iliac crest
Lateral third of the inguinal ligament
Transversus Abdominus insertion
Line alba with aponeurosis of internal oblique, pubic crest, and pecten pubis via conjoint tendon
Transversus Abdominus innervation
Thoracoabdominal nerves (ventral rami of T6-T12 spinal nerves) and first lumbar nerve
Transversus Abdominus Action
Compresses and supports abdominal viscera
Transverse Abdominis fiber orientation
Transverse
Rectus Abdominus Origin
Pubic crest and pubic symphysis
Rectus Abdominus insertion
Xiphoid process and costal cartilages of ribs 5-7
Rectus Abdominus innervation
Thoraco-abdominal nerves (anterior rami of T6–T12 spinal nerves)
Rectus Abdominus action
Flexes trunk (lumbar vertebrae) and compresses abdominal viscera
Stabilizes and controls tilt of pelvis (antilordosis)
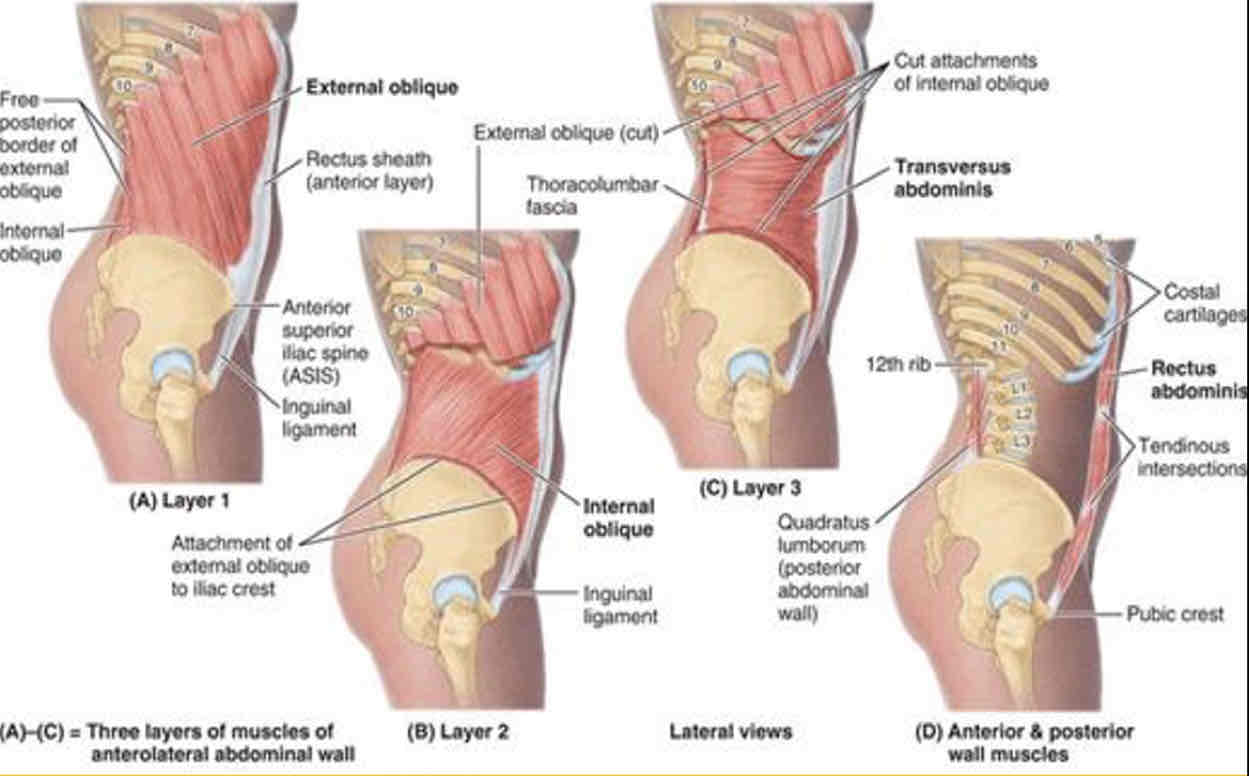
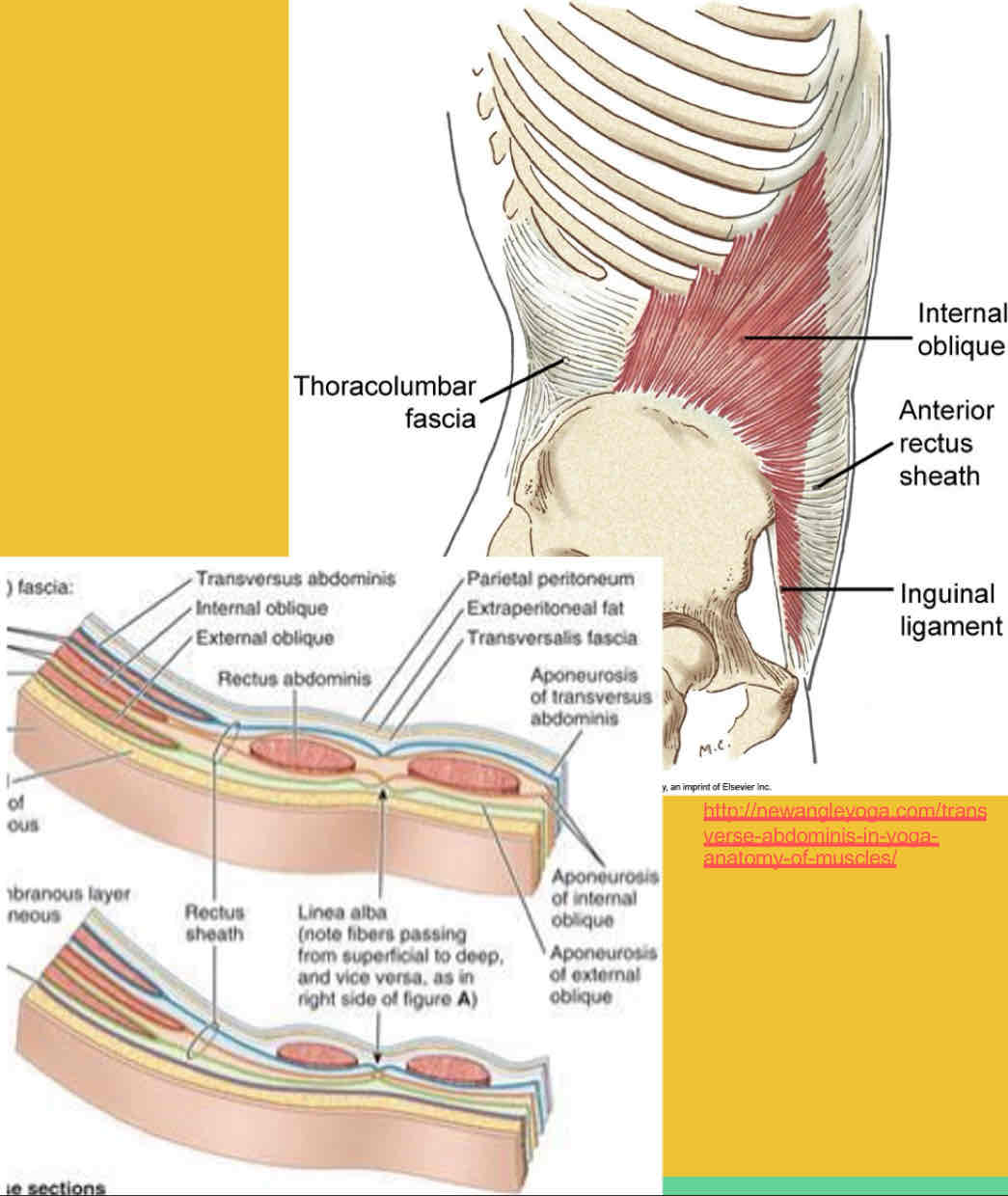
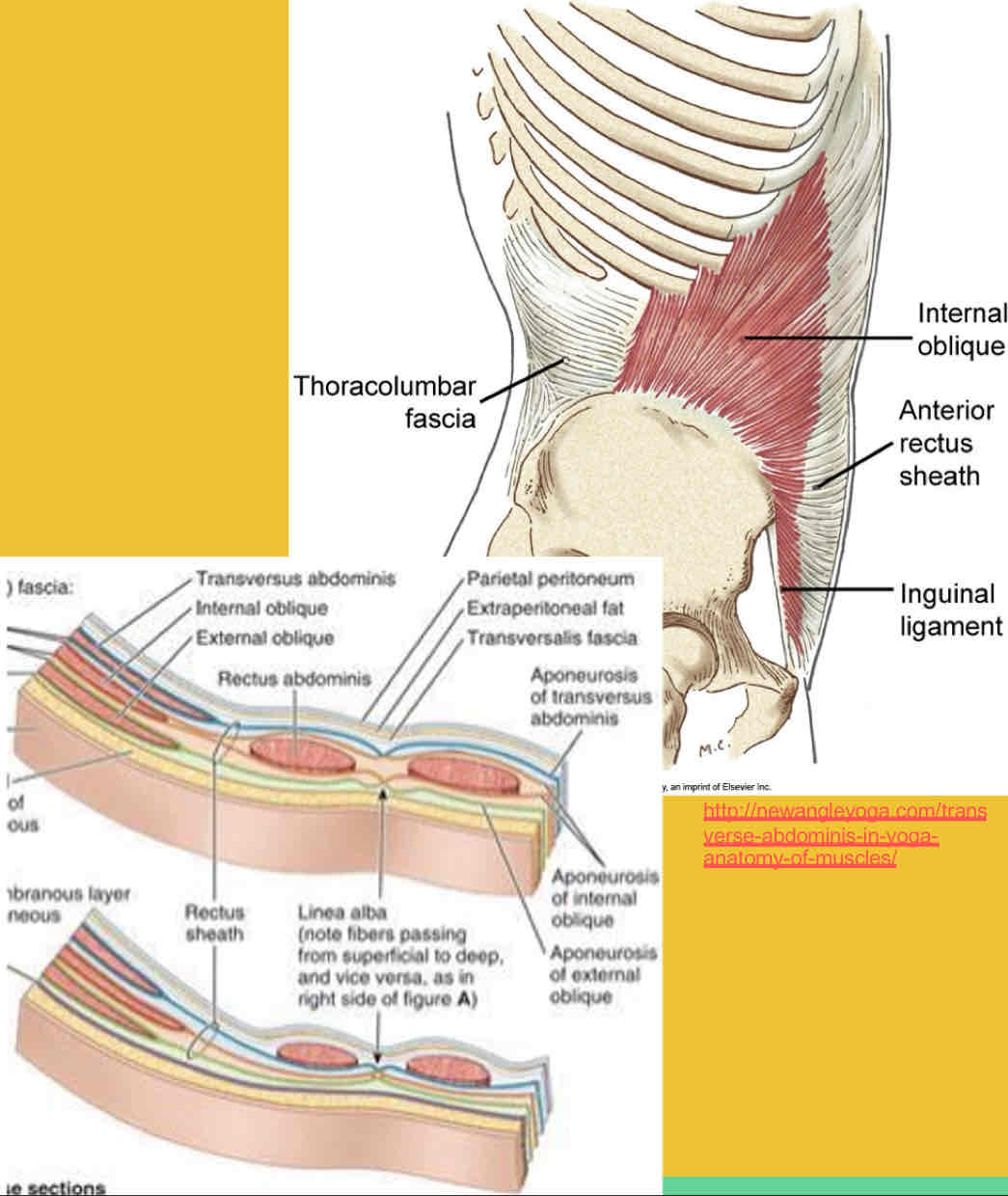
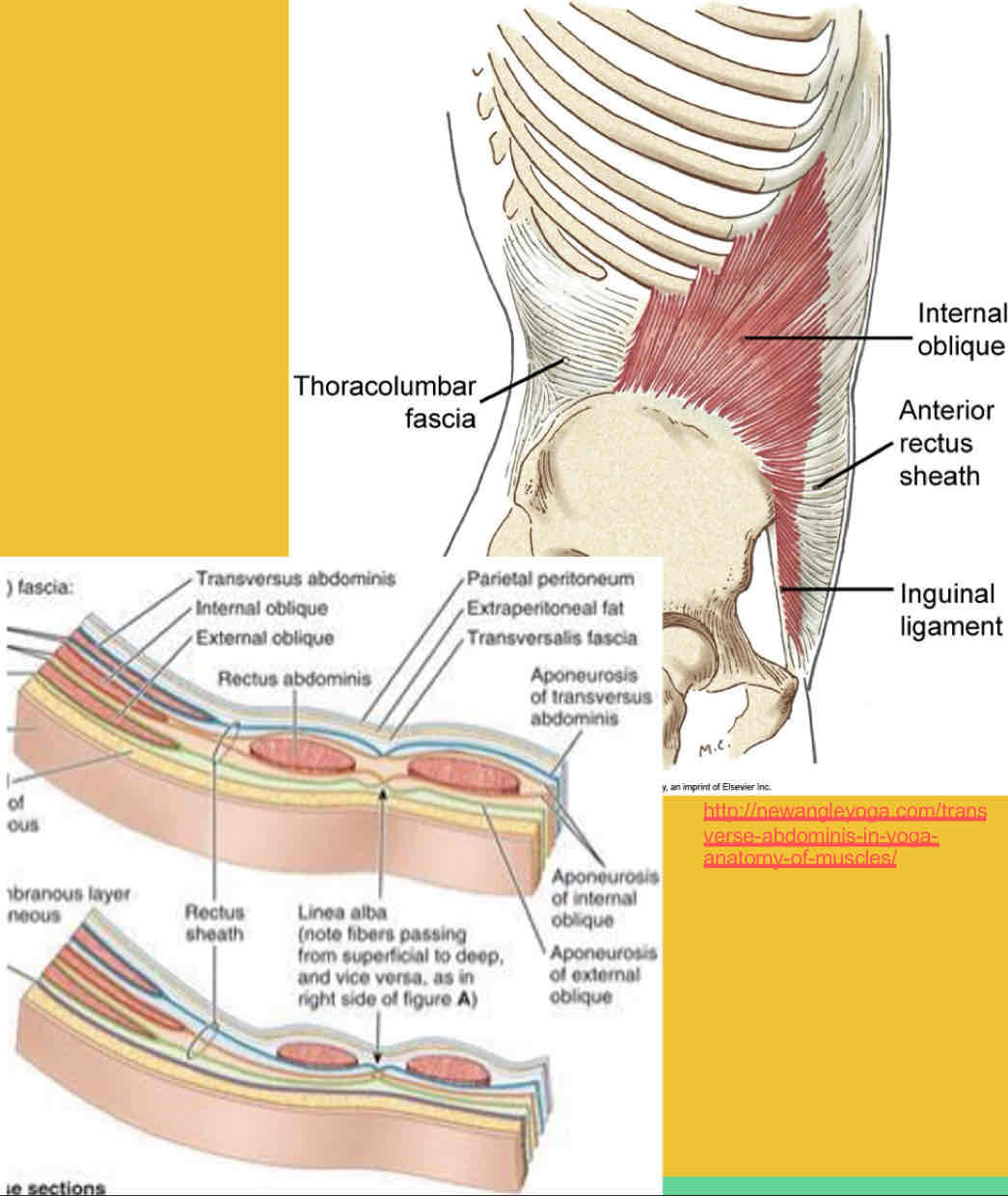
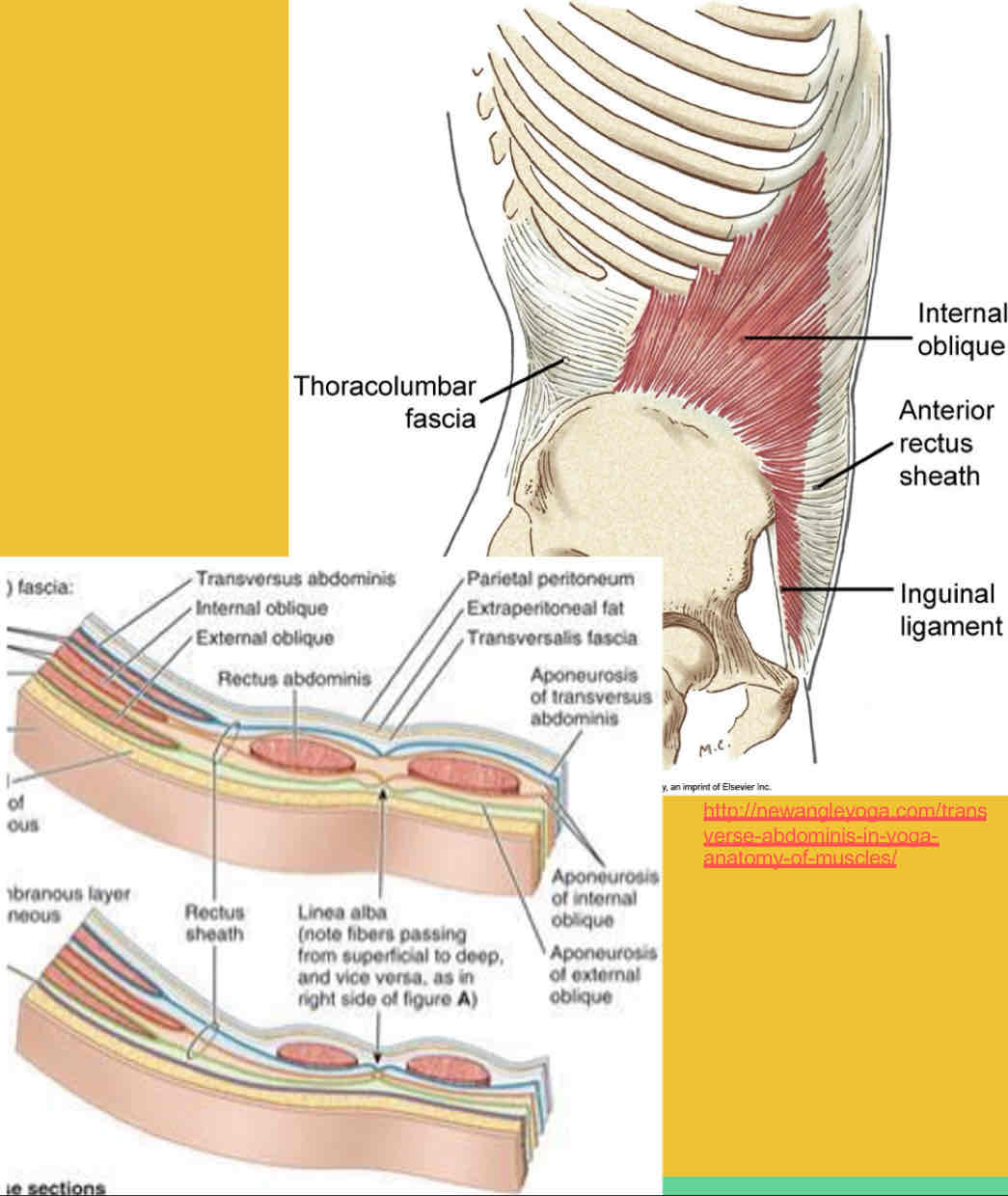
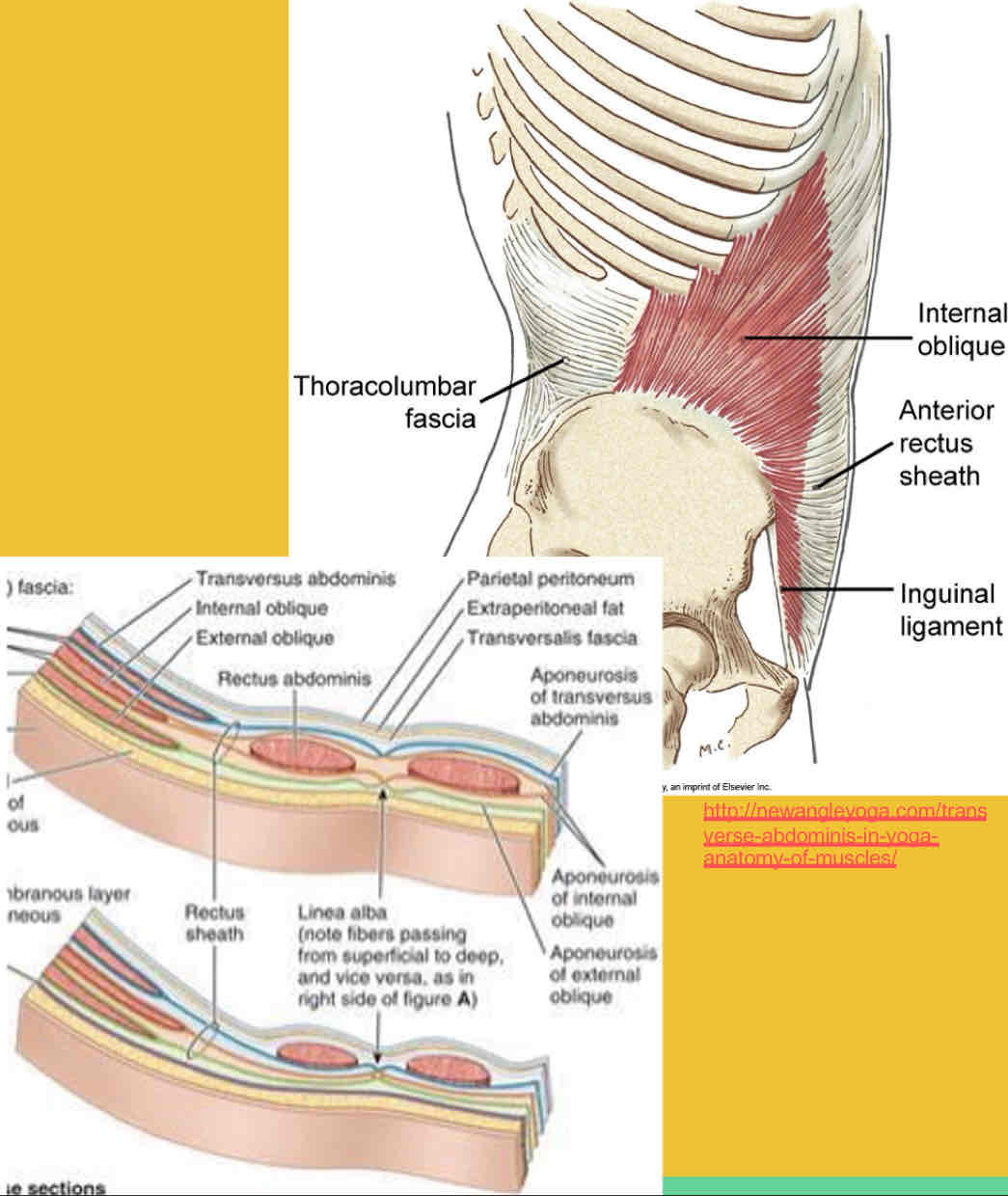
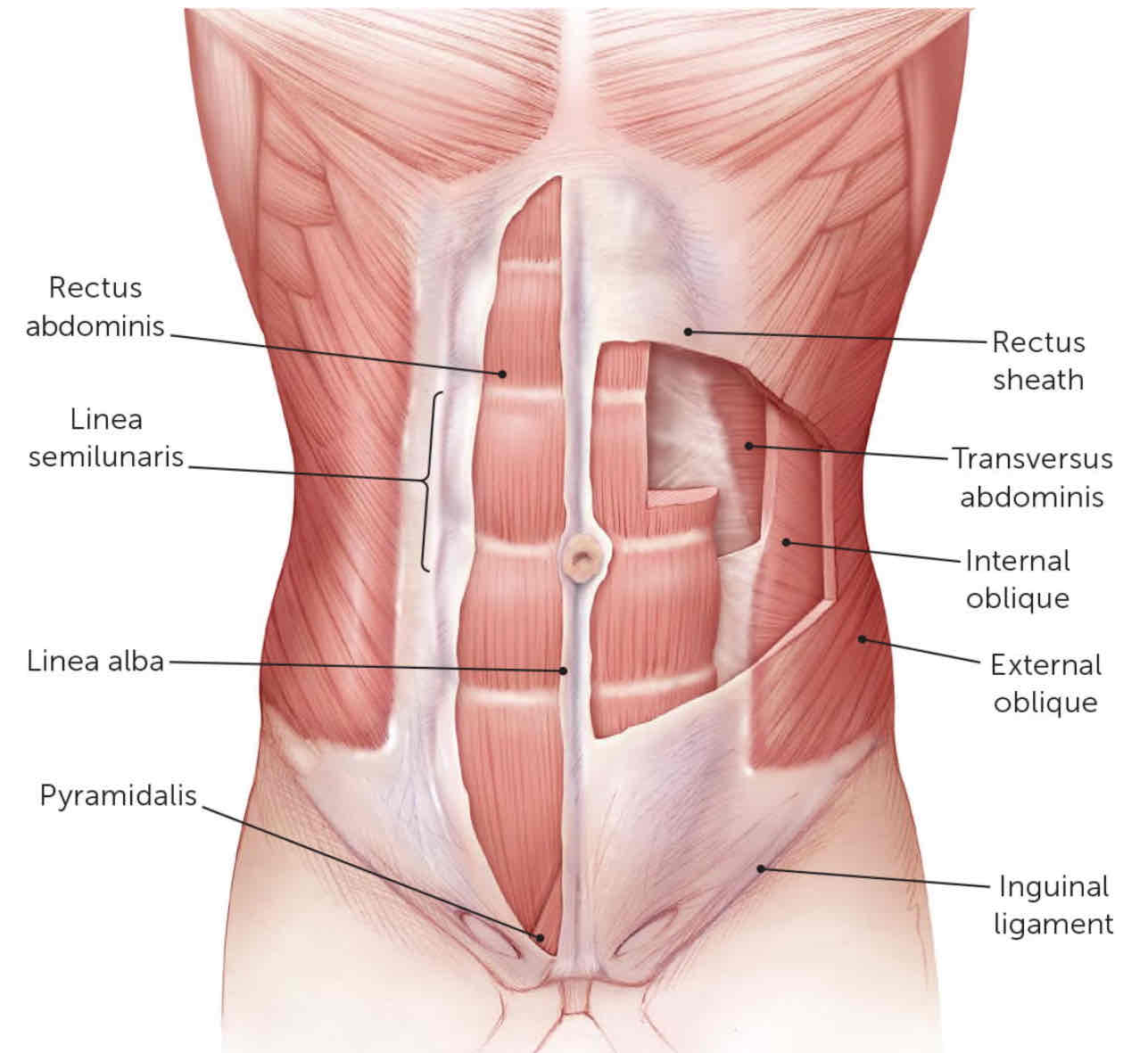
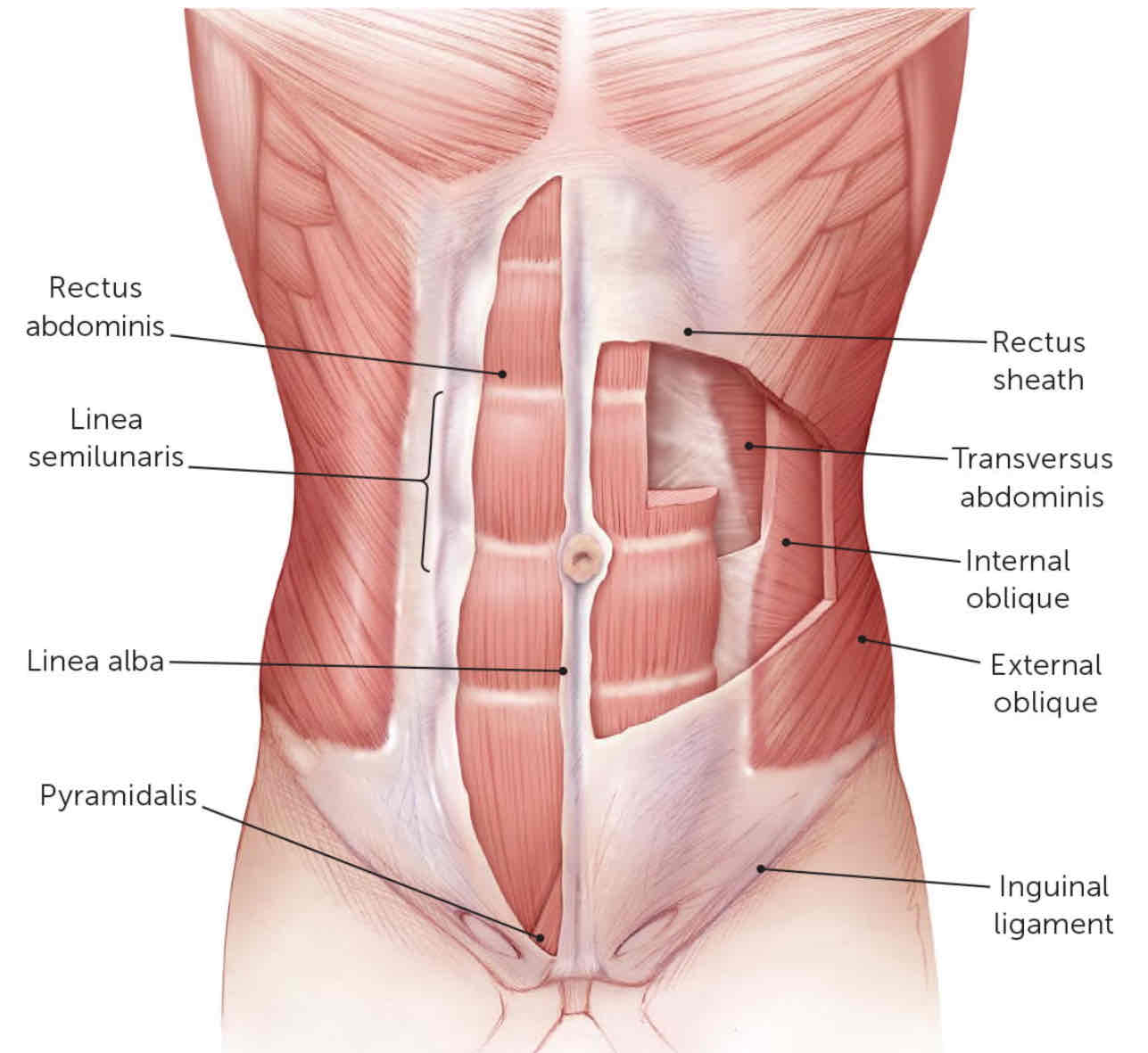
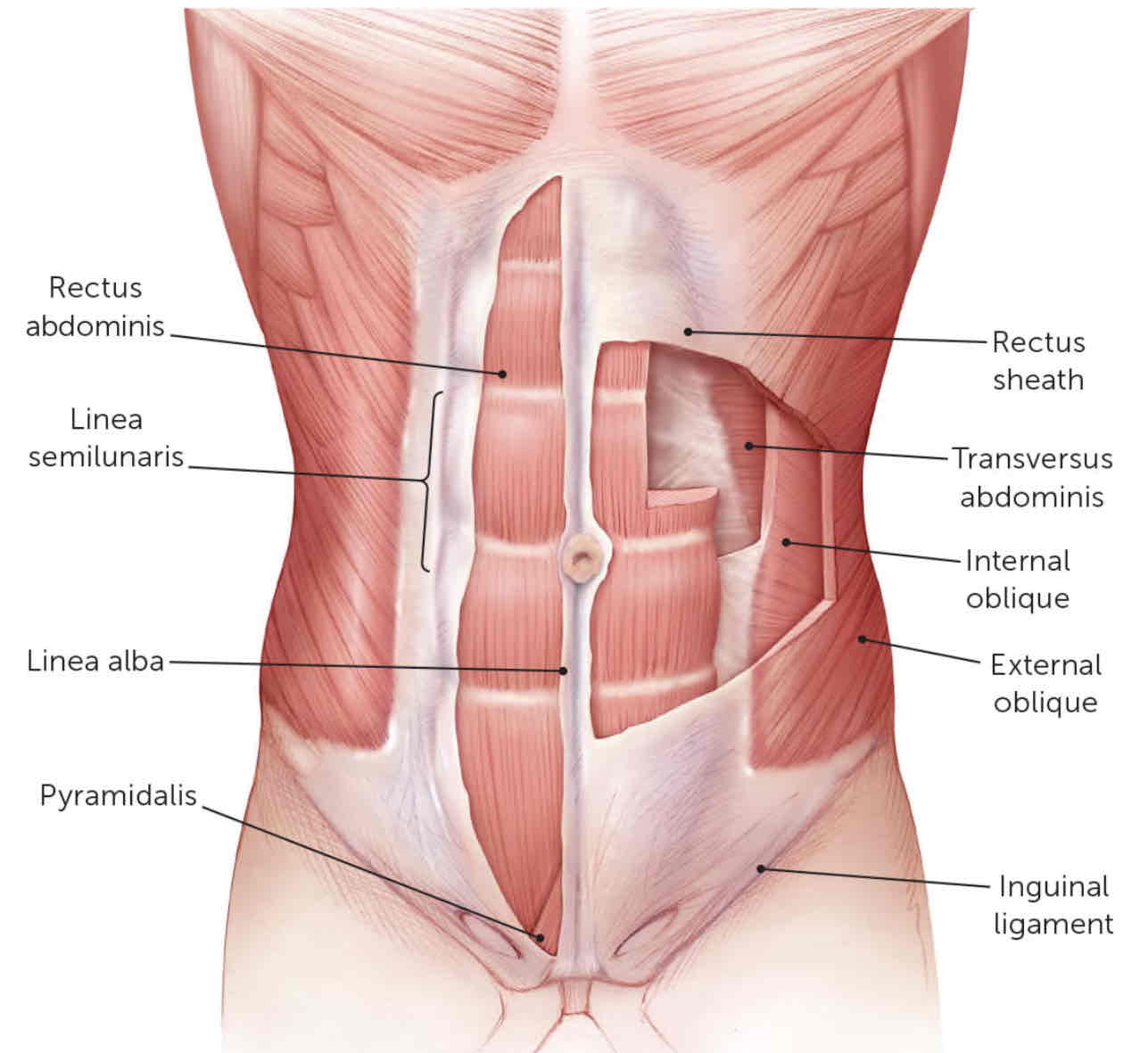
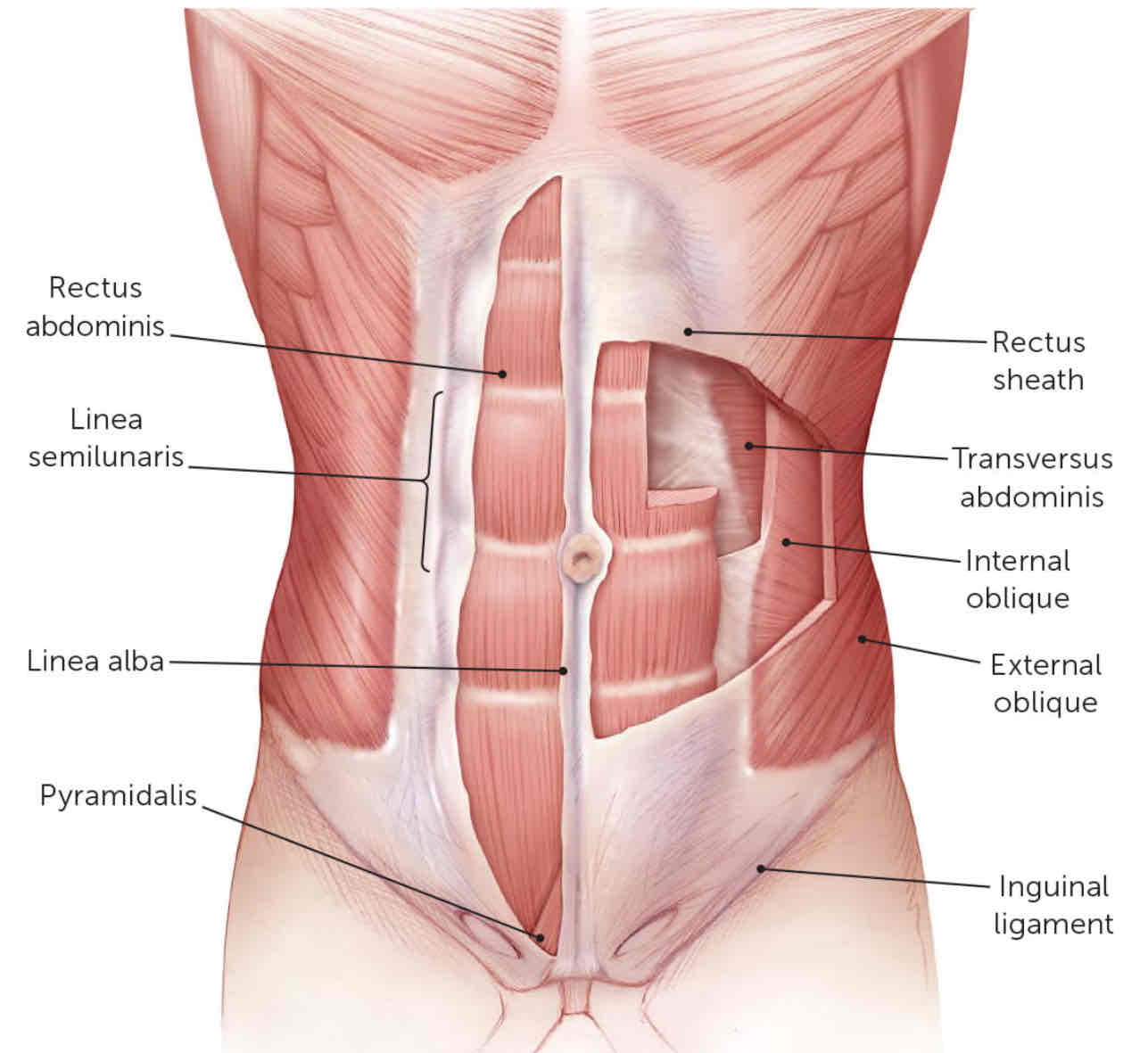
3 Flat muscles of the Anterolateral Abdominal wall
External oblique
Internal oblique
Transverse abdominis
These form Rectus Sheath & Linea Alba via aponeuroses
2 Vertical muscles of the Anterolateral Abdominal wall
Rectus abdominis
Pyramidalis
What is the significance, clinically, for the internal oblique and transversus abdominus muscles to attach to the thoracolumbar fascia?
Together, they form a muscular girdle that puts pressure on abdominal viscera which increases intra-abdominal pressure and elevates the relaxed diaphragm during forced expiration - cough, sneeze
What are other movements that the abdominal muscles can do individually or combined?
Increase Intra-abdominal pressure:
- Forced expiration
- Defecation
- Micturition (urination)
- Vomiting
- Childbirth
- Heavy lifting
Trunk movements & pelvis tilting
- Rectus abdominis flexes trunk (or posteriorly tilts pelvis)
- Obliques laterally flex & rotate trunk
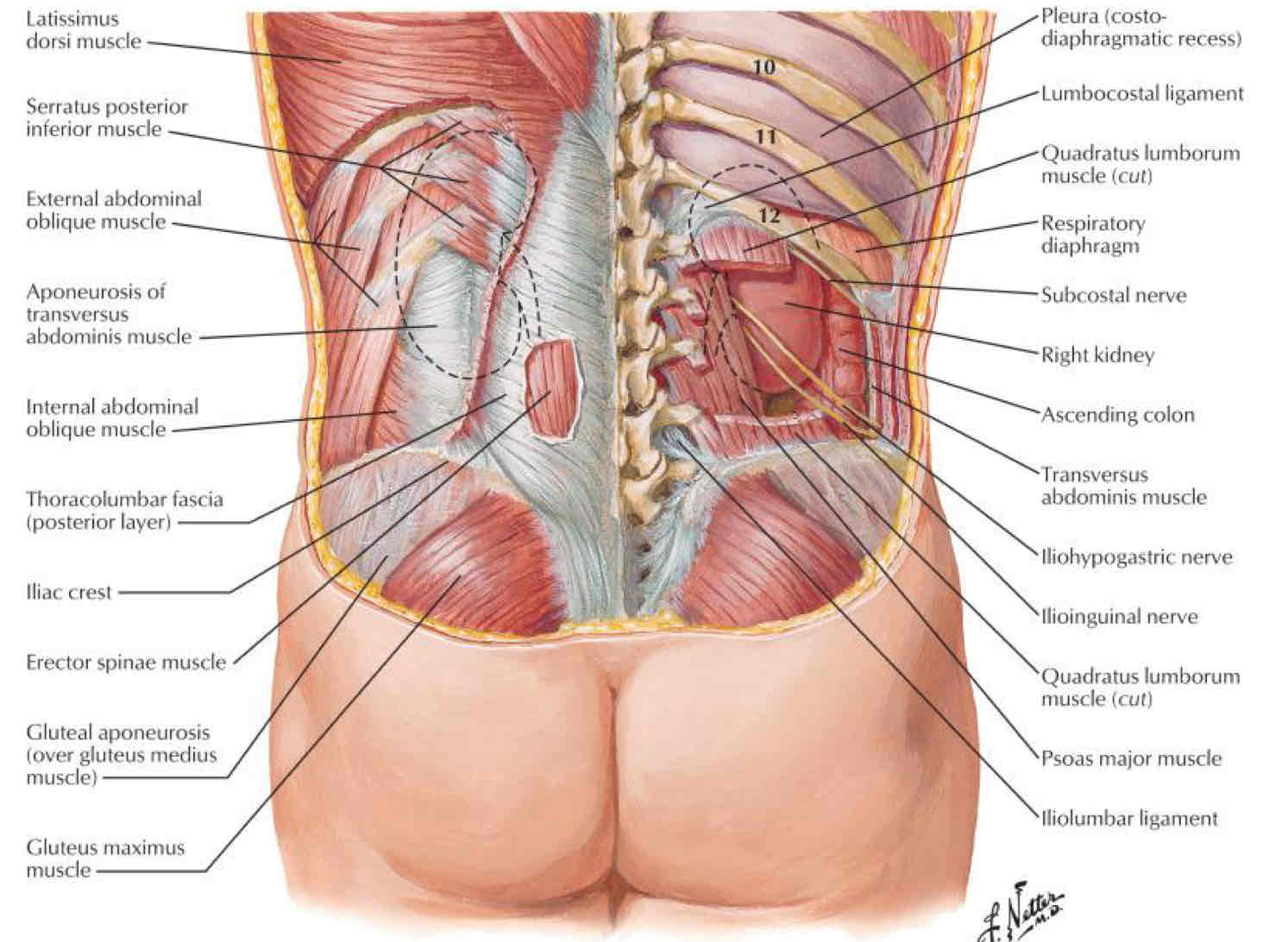
What layers would you have to cut through from posterior to anterior to reach the kidneys?
External Oblique —> Aponeurosis of Transversus abdominus —> Quad Lumborum
Parietal peritoneum characteristics
Lines internal wall
- Sensitive to pressure, pain, heat, cold, laceration
- Pain localized
Visceral peritoneum characteristics
Line organs
- Sensitive to stretching & chemical irritation
- Pain referred to dermatomes
Intraperitoneal
Completely surrounded by visceral peritoneum
Extraperitoneal
Outside the peritoneum
Retroperitoneal
Behind the peritoneum
Subperitoneal
Inferior to parietal peritoneum; superior surface of the organ is covered with parietal peritoneum
Intraperitoneal organs
Stomach
Jejunum and Ileum
Transverse and sigmoid colon
Appendix
Liver
Spleen
Extraperitoneal organs
Organs outside of the parietal peritoneum, but typically covered by parietal peritoneum on one side
Retroperitoneal organs
Located outside, or posterior to, the peritoneum
Includes most of pancreas, duodenum, and parts of large intestine
Subperitoneal organs
Bladder
Prostate
Rectum
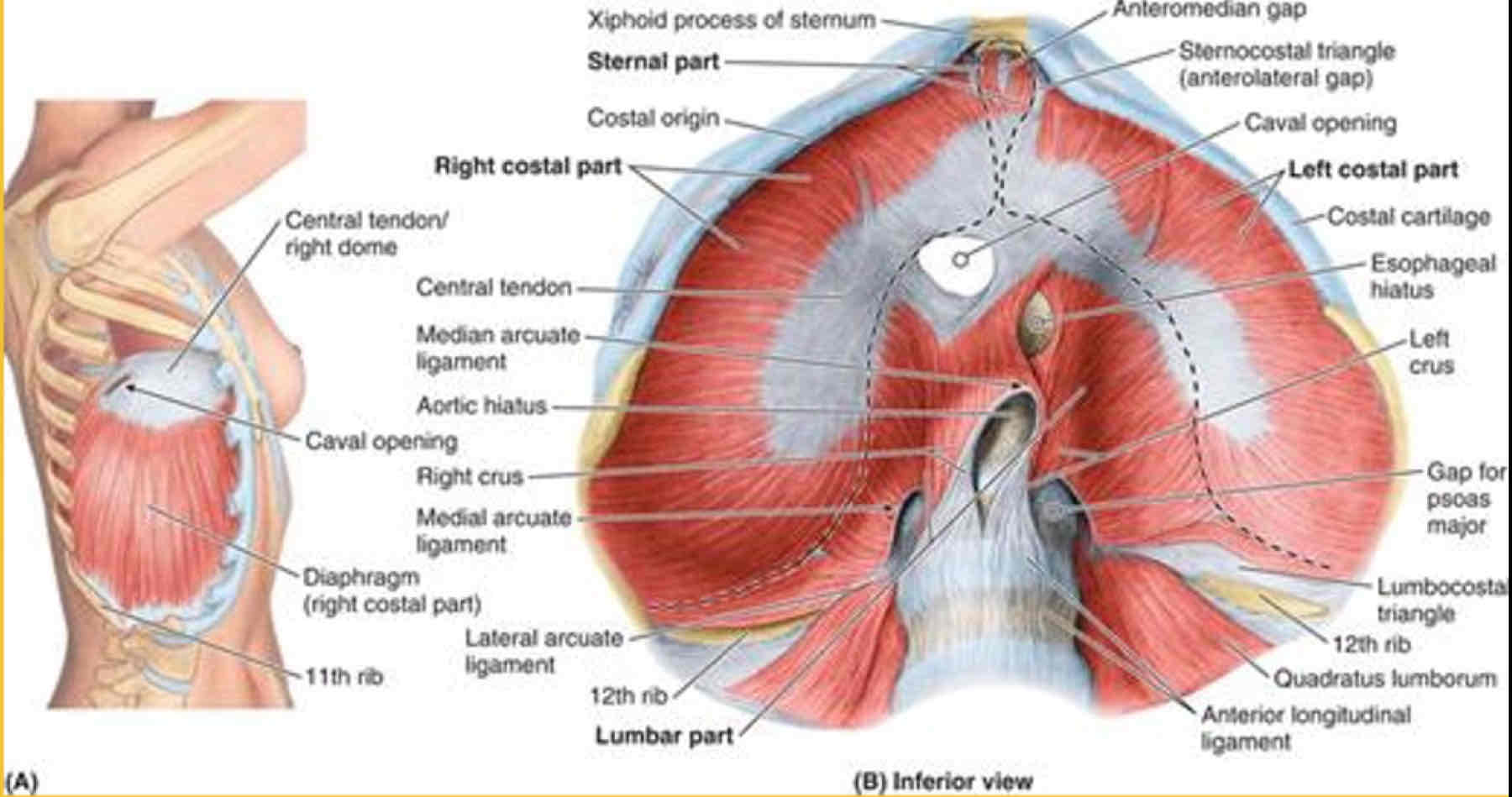
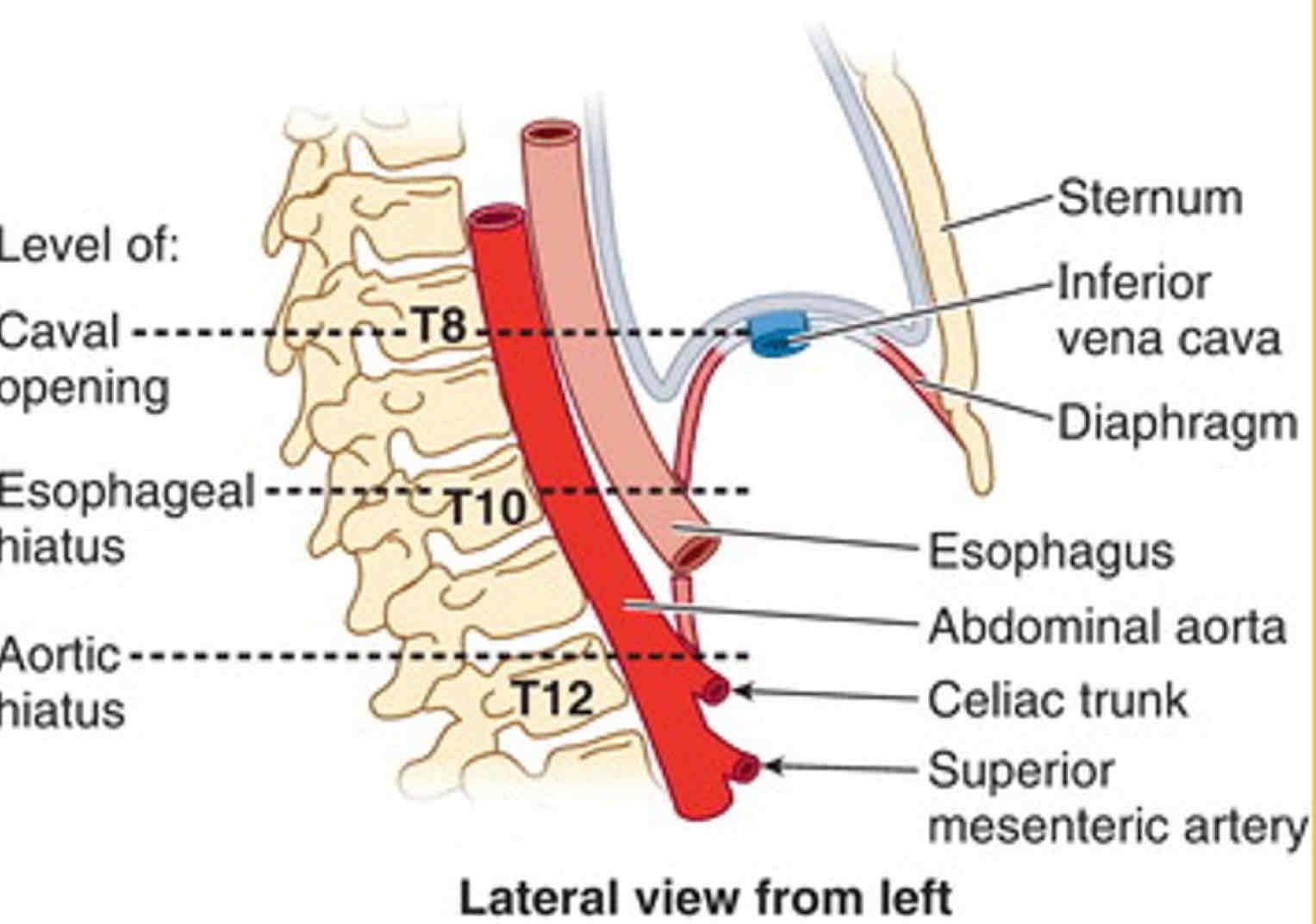
What passes through the Caval Opening
IVC
Right Phrenic Nerve
Lymphatic Vessels going to the liver
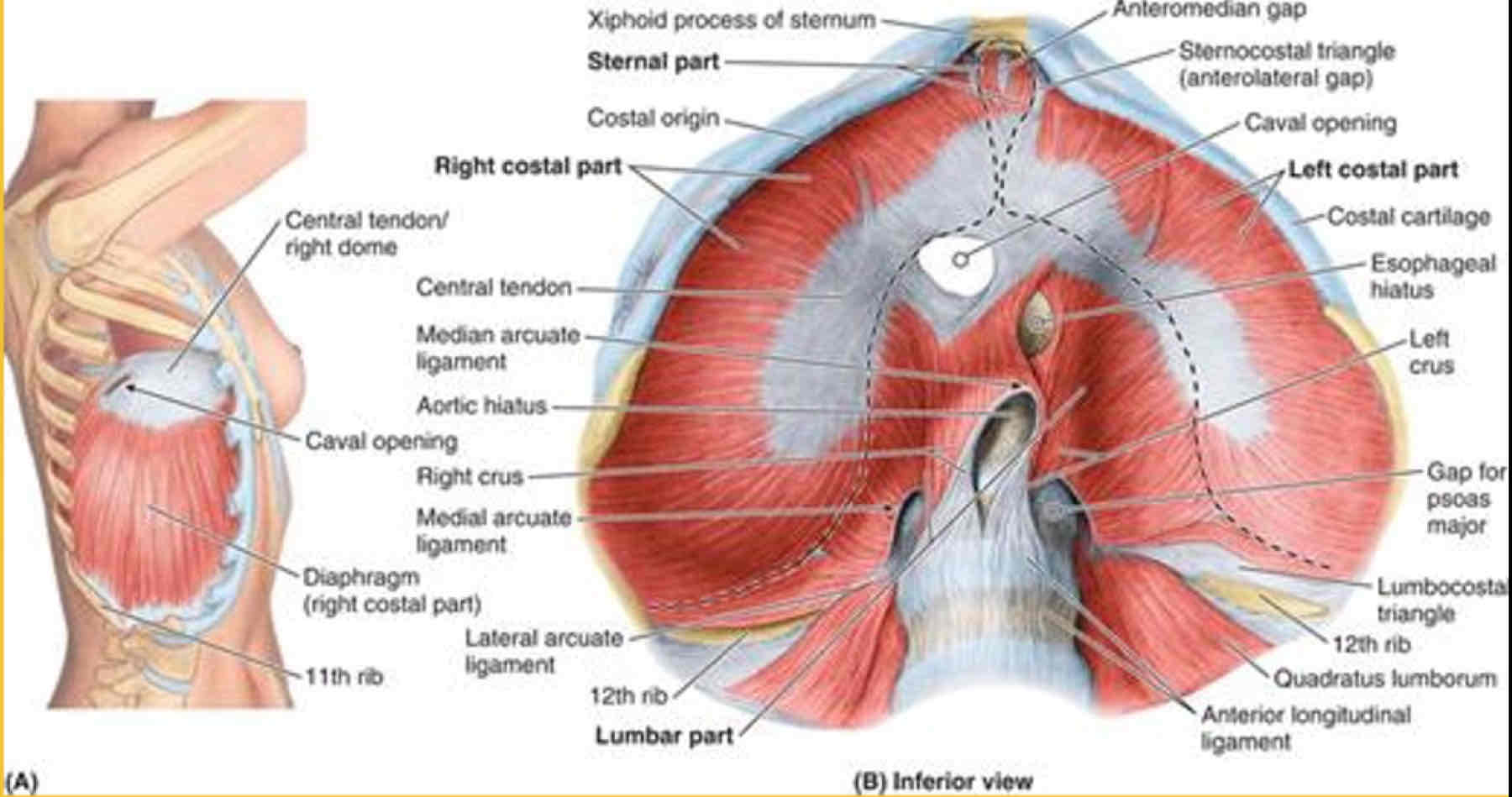
What passes through the Esophageal Hiatus
Esophagus
Vagal trunks
Gastric vessels
Lymphatic vessels
Right crus
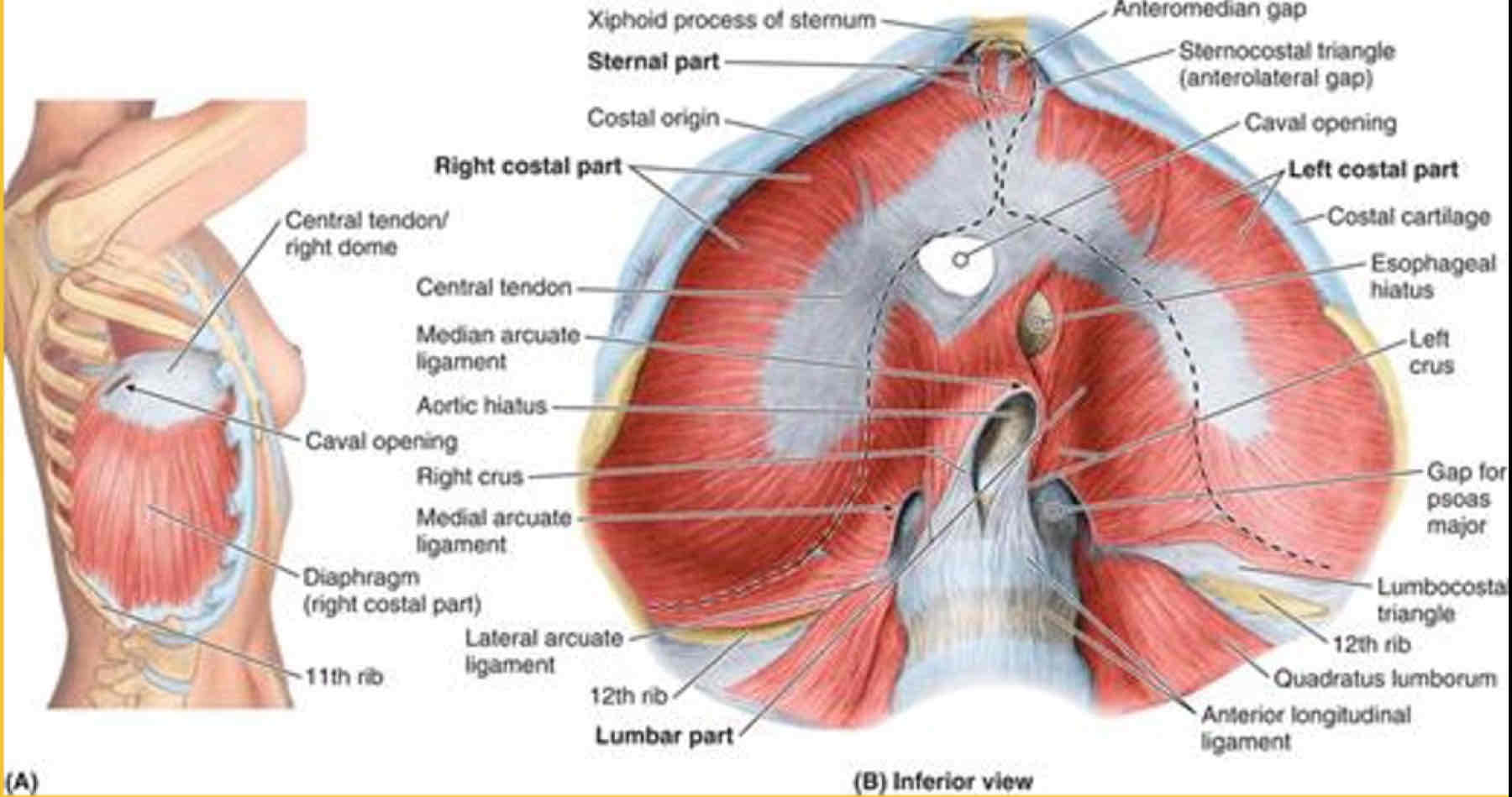
What passes through the Aortic Hiatus (Median Arcuate Ligament)
Descending aorta
Thoracic duct
Azygous vein
Hemi-azygous vein
Median Arcuate Ligament
Joins the R & L crura and forms the Aortic Hiatus
What Passes through Medial Arcuate Ligament
Psoas major
What passes through the Lateral Arcuate Ligament
Quadratus lumborum
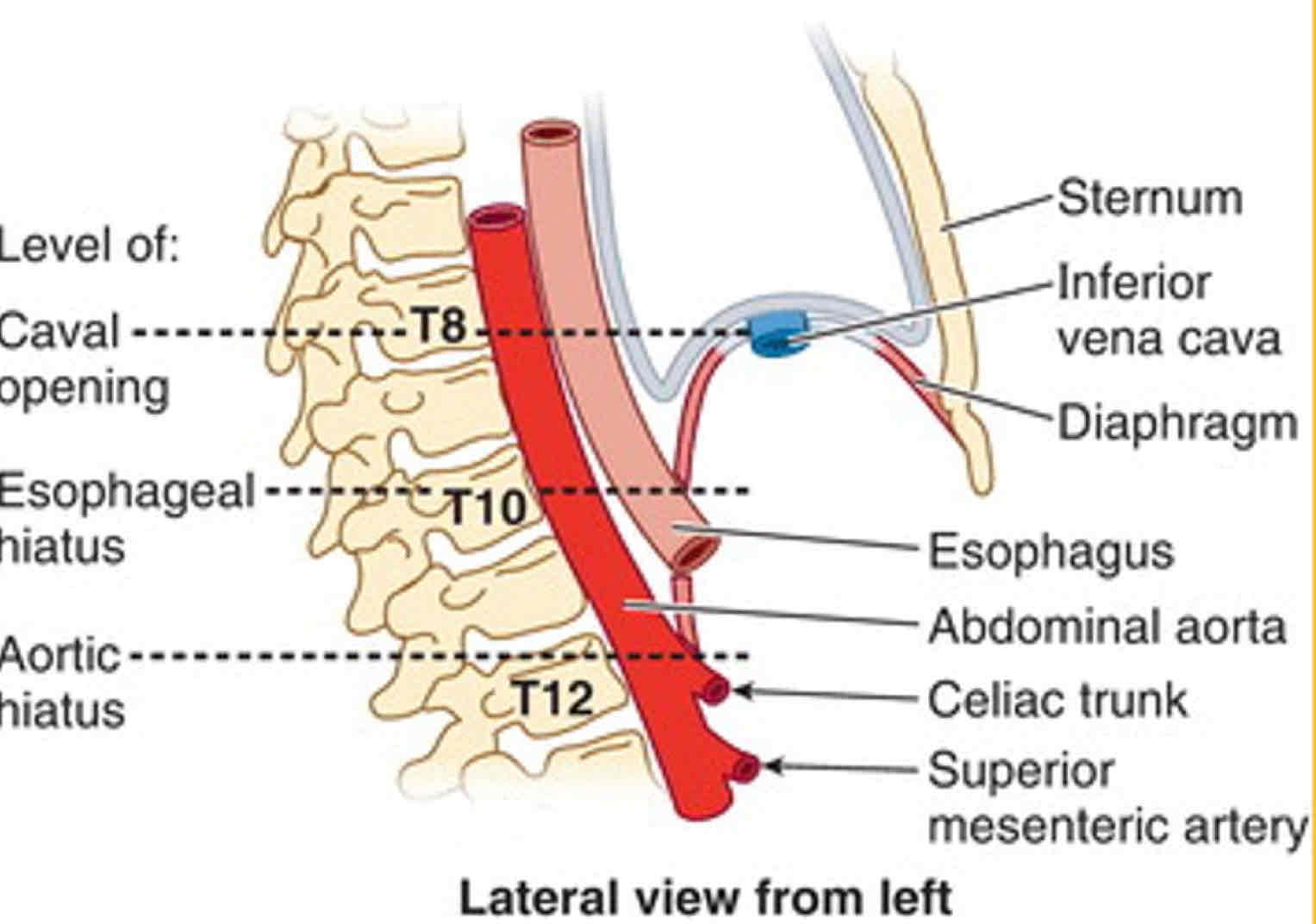
Level of Caval opening of the diaphragm
Level of T8-9
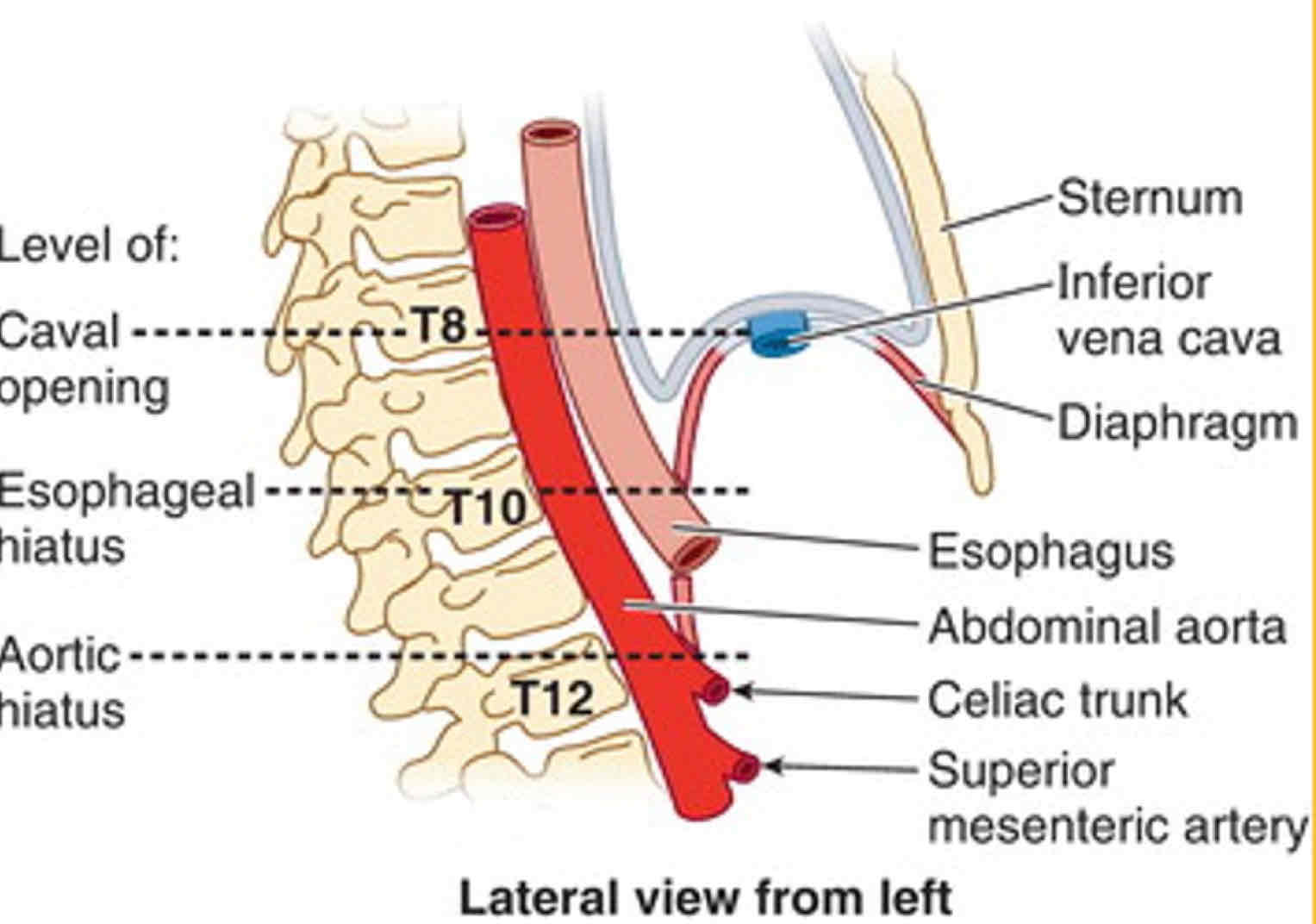
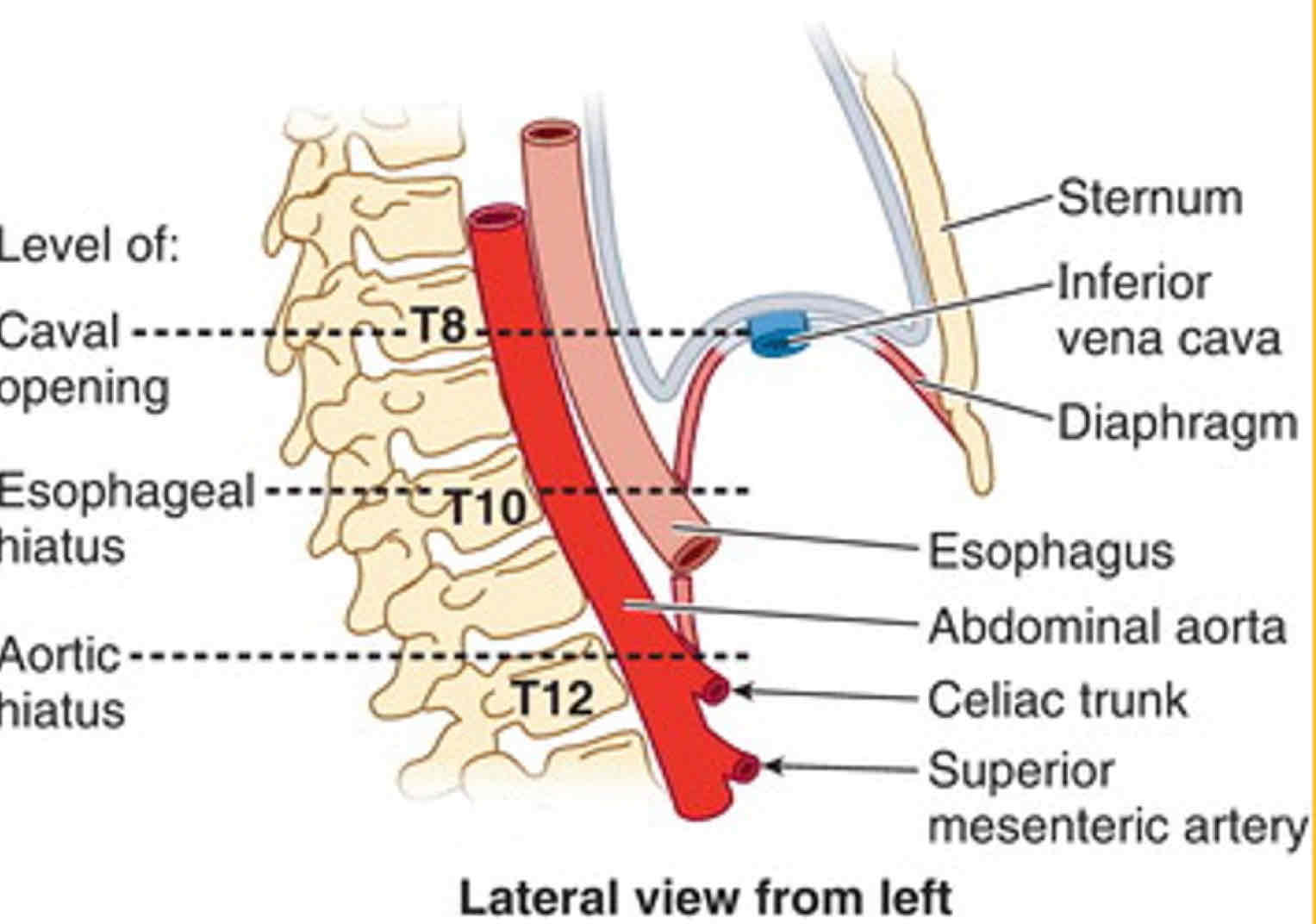
Level of Esophageal Hiatus of the diaphragm
Level of T10
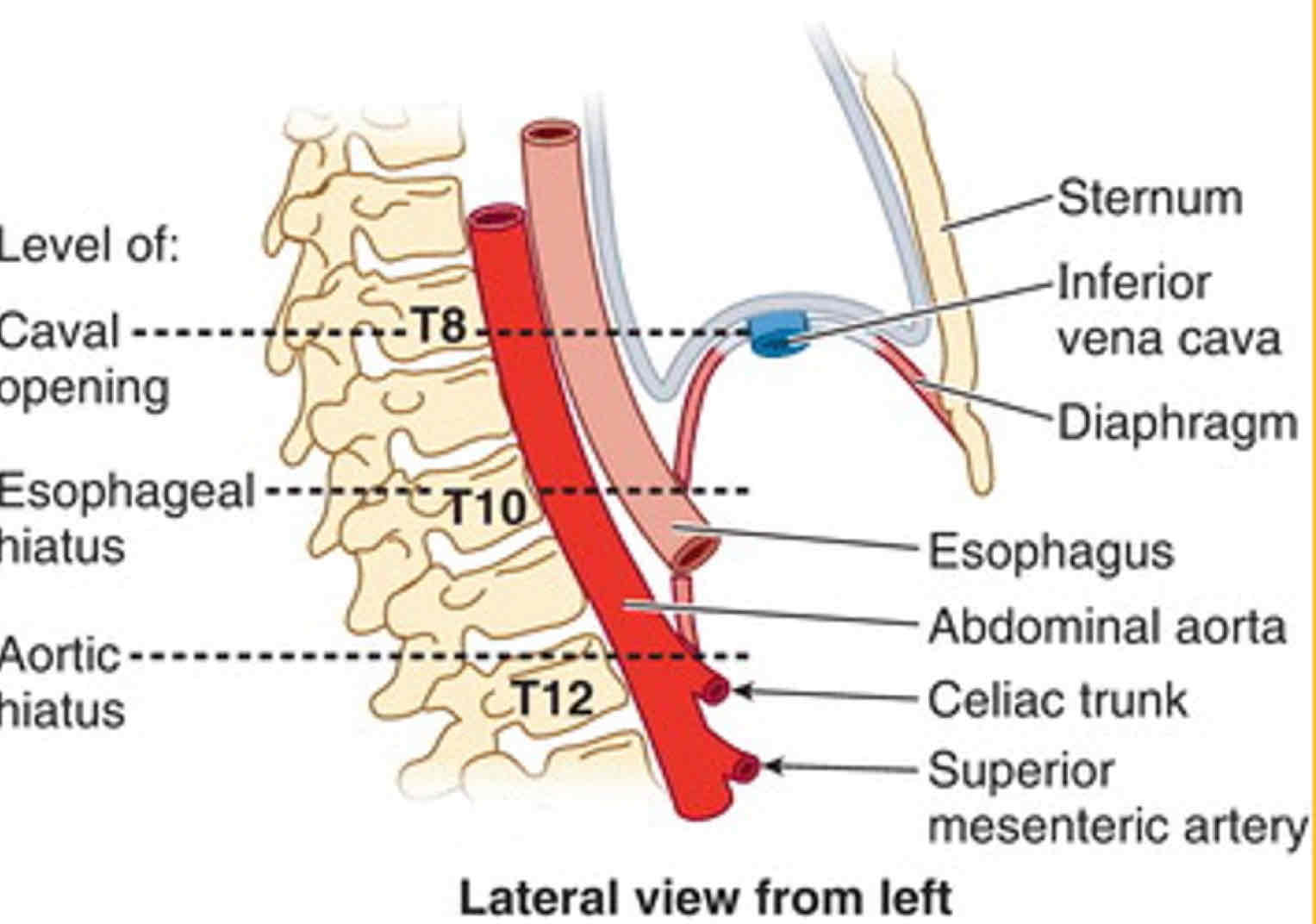
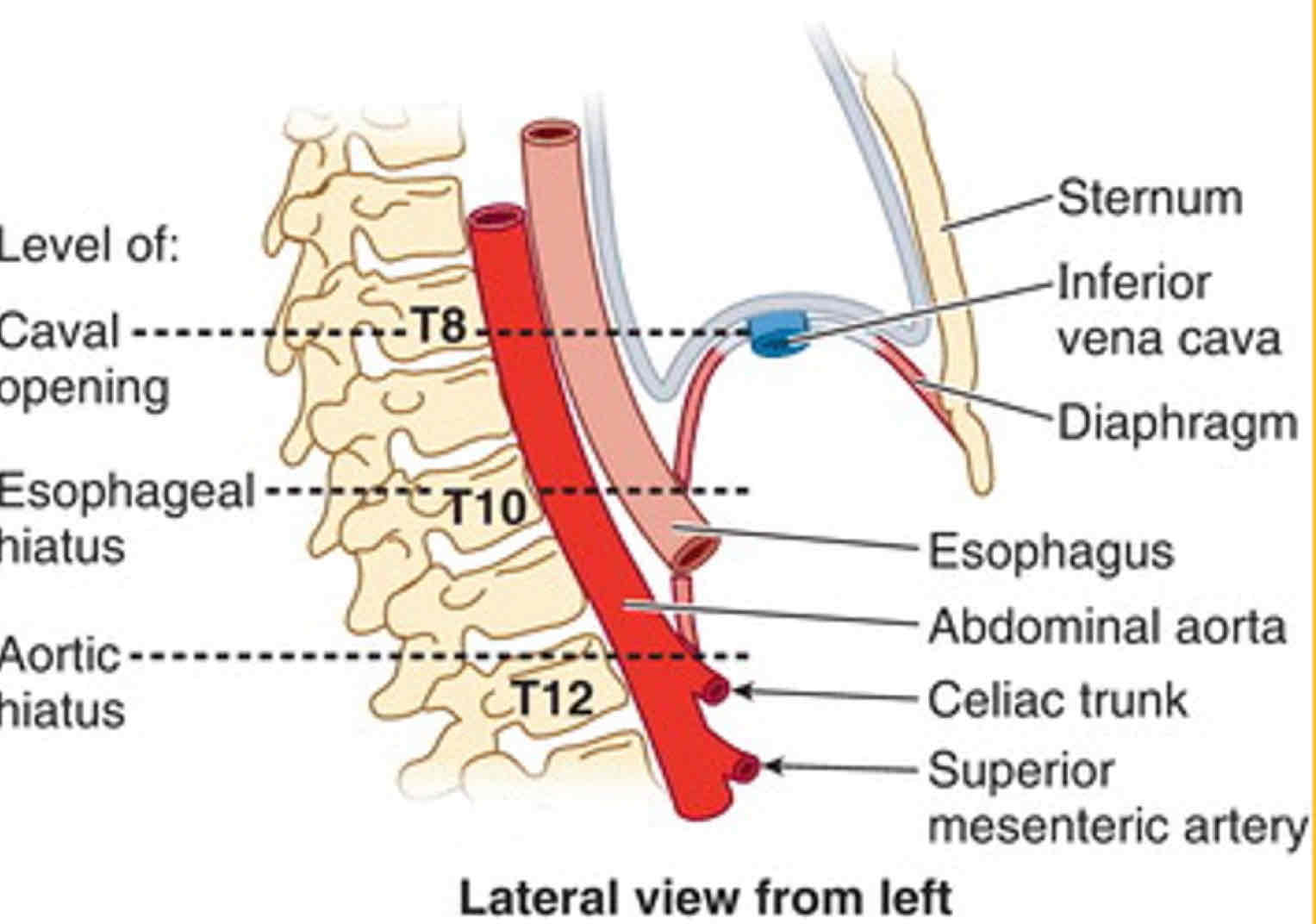
Level of Aortic Hiatus of the diaphragm
Level of T12
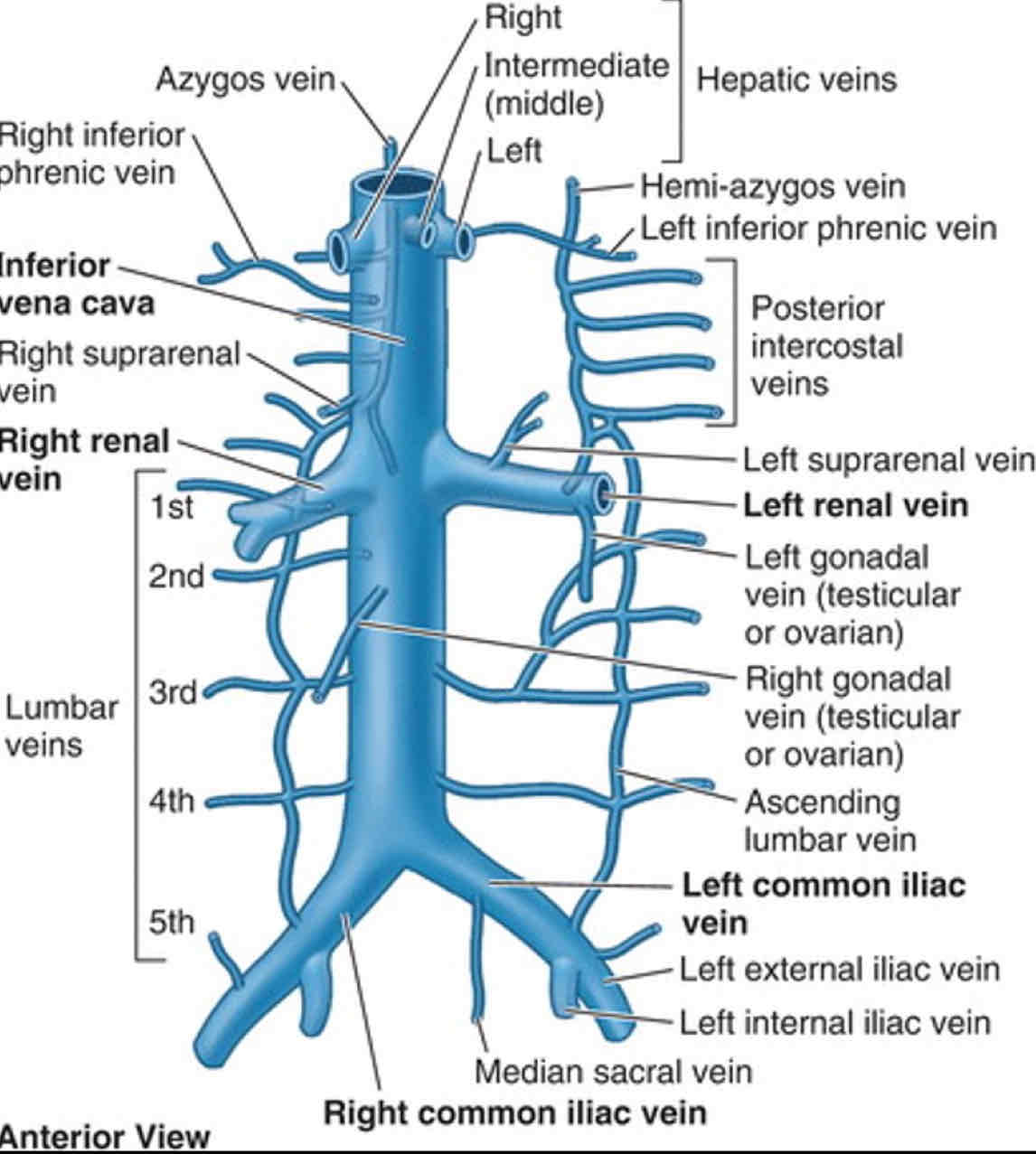
Veins from Abdominopelvic region to Inferior Vena Cava (IVC)
R&L Common Iliac Veins
Hepatic Portal Vein tributaries
Right Suprarenal Vein
R&L Renal Veins —> Inferior Vena Cava
Right Gonadal Vein
Inferior Phrenic Veins
L3 & L4 Lumbar veins
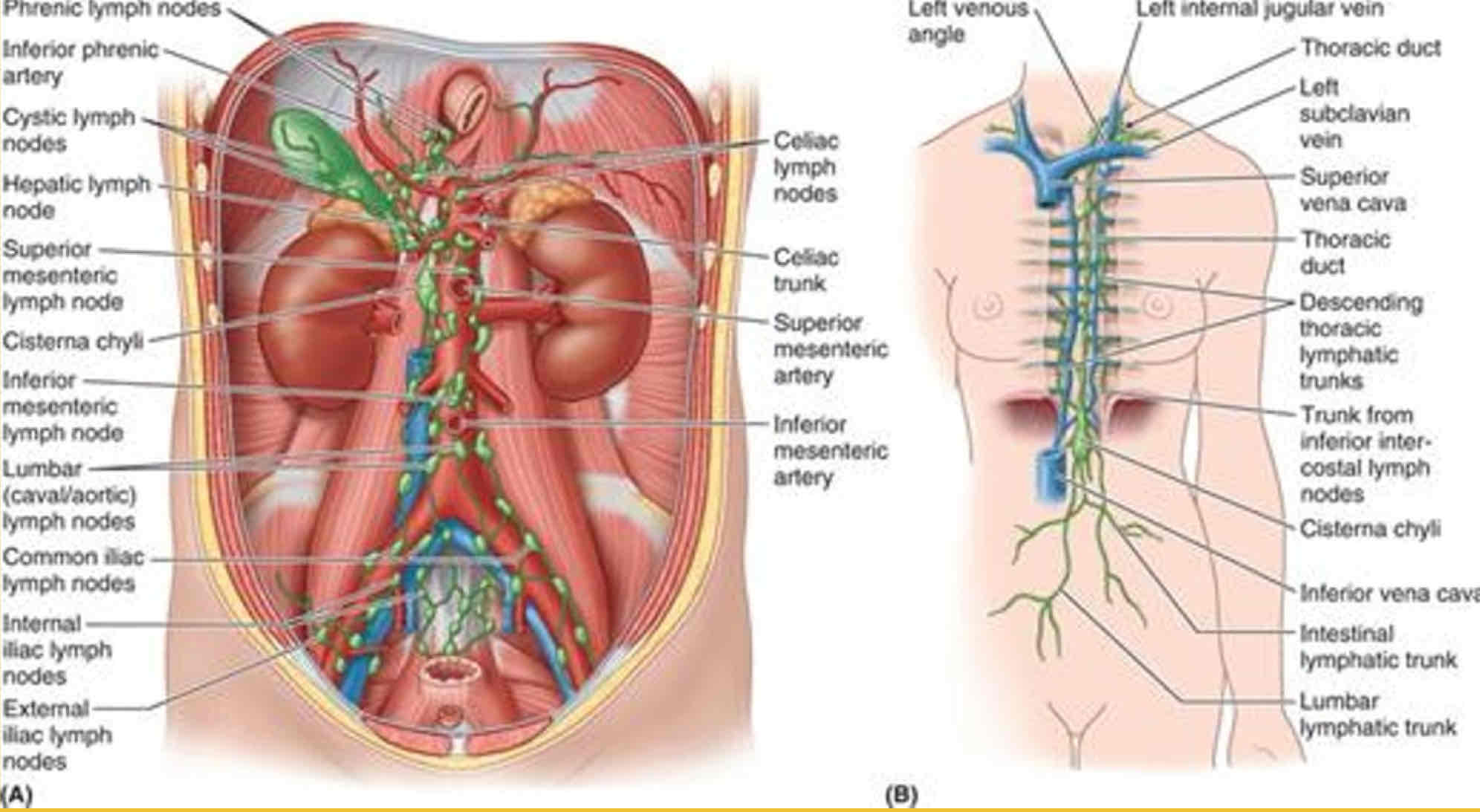
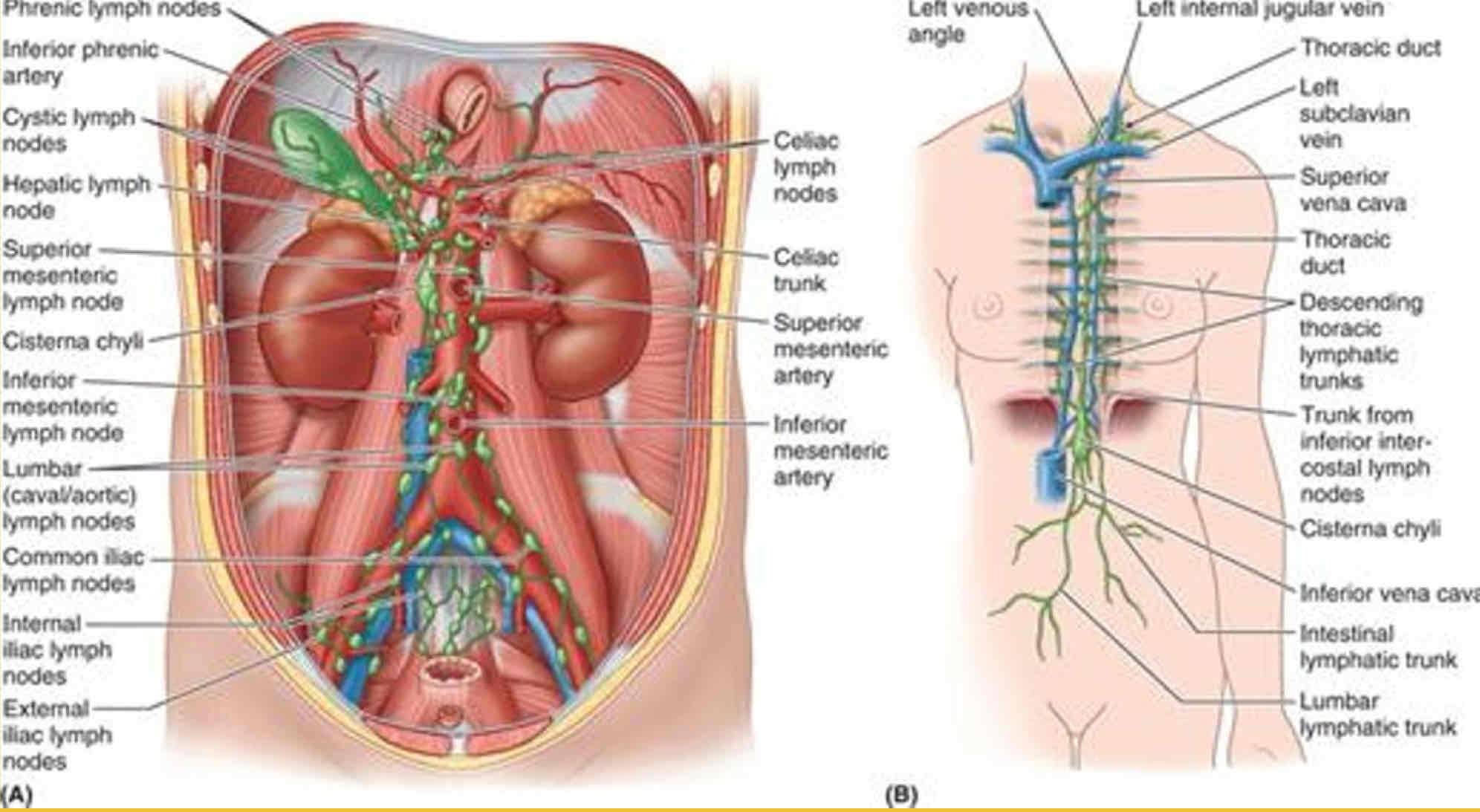
Basic flow of Lymph in Posterior Abdominal wall
Internal & External Iliac lymph nodes —> Common Iliac lymph nodes —> Lumbar lymph nodes —> Pre-Aortic lymph nodes —> Intestinal lymphatic trunks
Intestinal lymphatic trunks + Lumbar lymphatic trunks + Thoracic lymphatic trunks = Cisterna Chyli
Cisterna Chyli —> Thoracic duct —> Left Subclavian vein —> Internal jugular vein —> Left Venous Angle
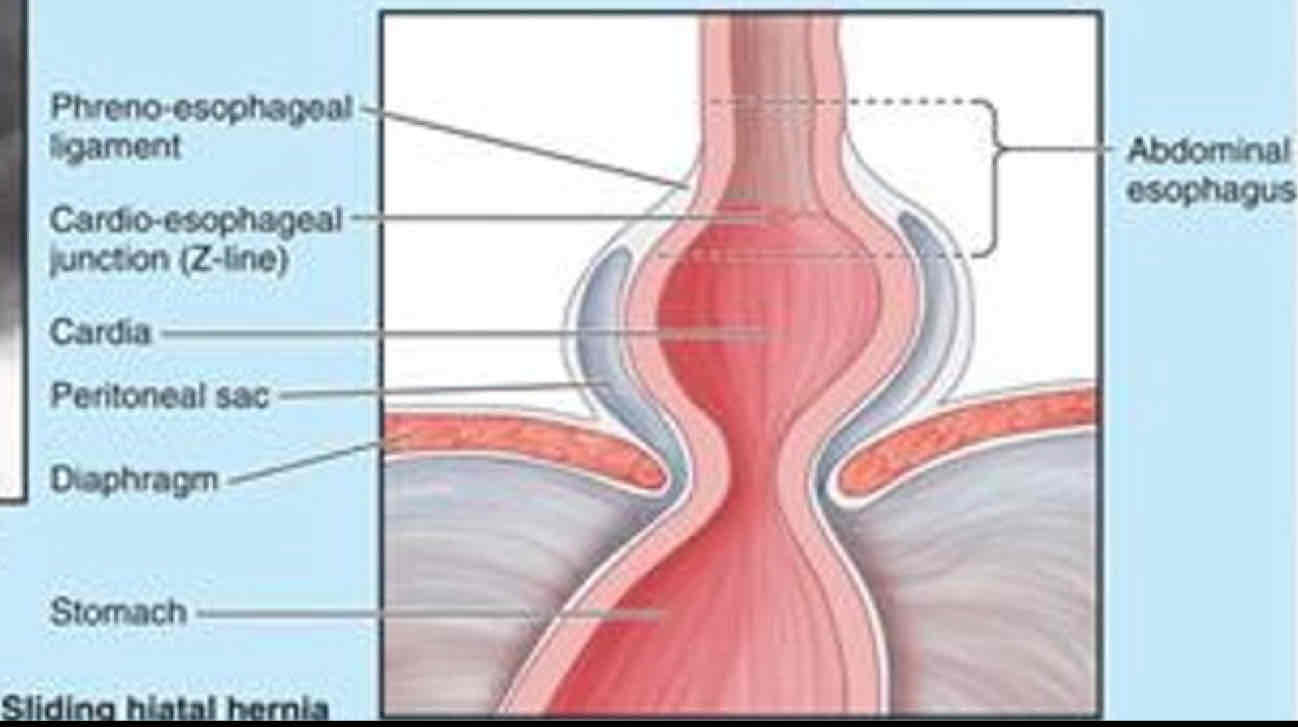
What are Hiatal Hernias?
When the stomach protrudes into the thorax through the Esophageal Hiatus of the diaphragm
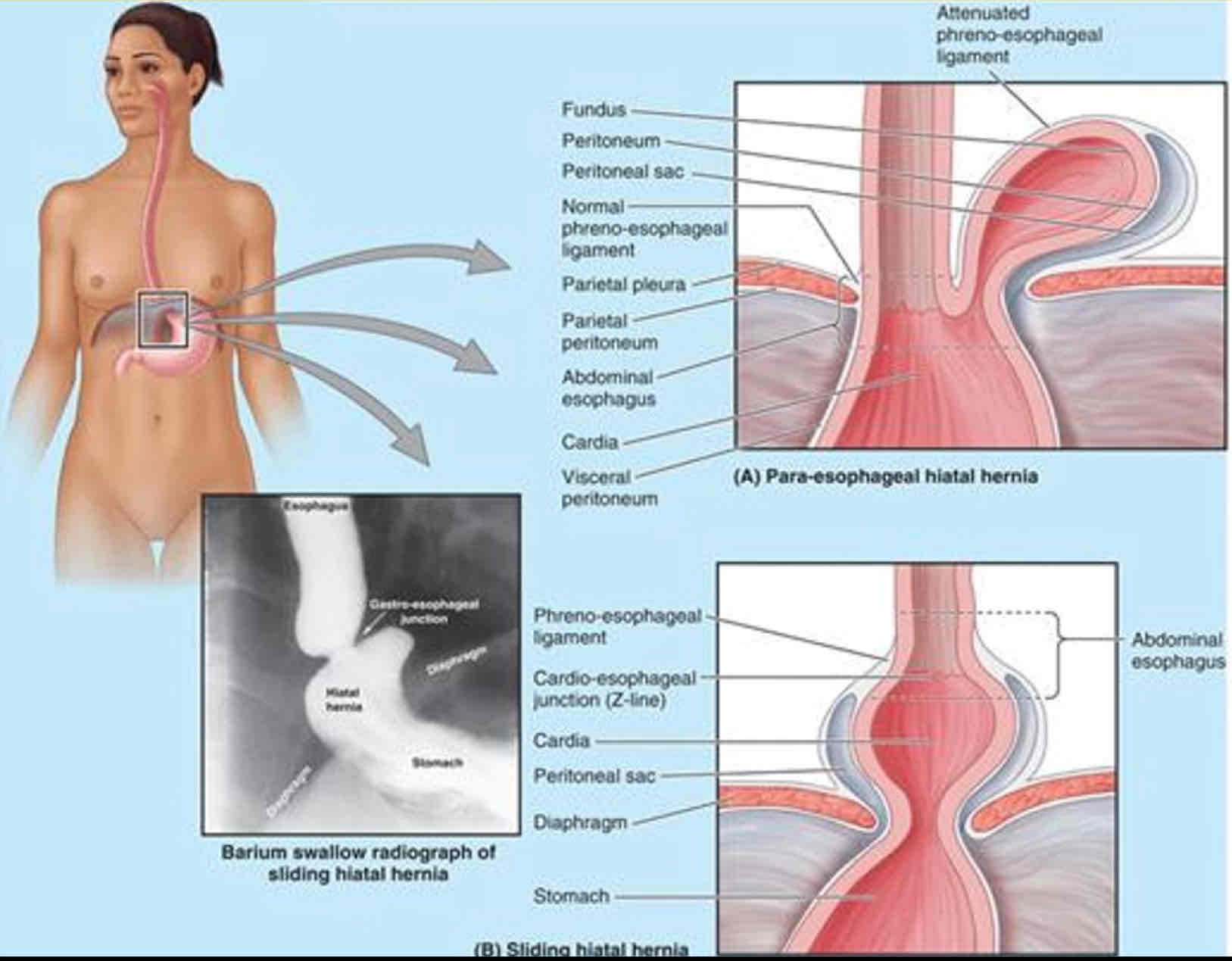
Type of Hiatial Hernias
Para-esophageal
Sliding
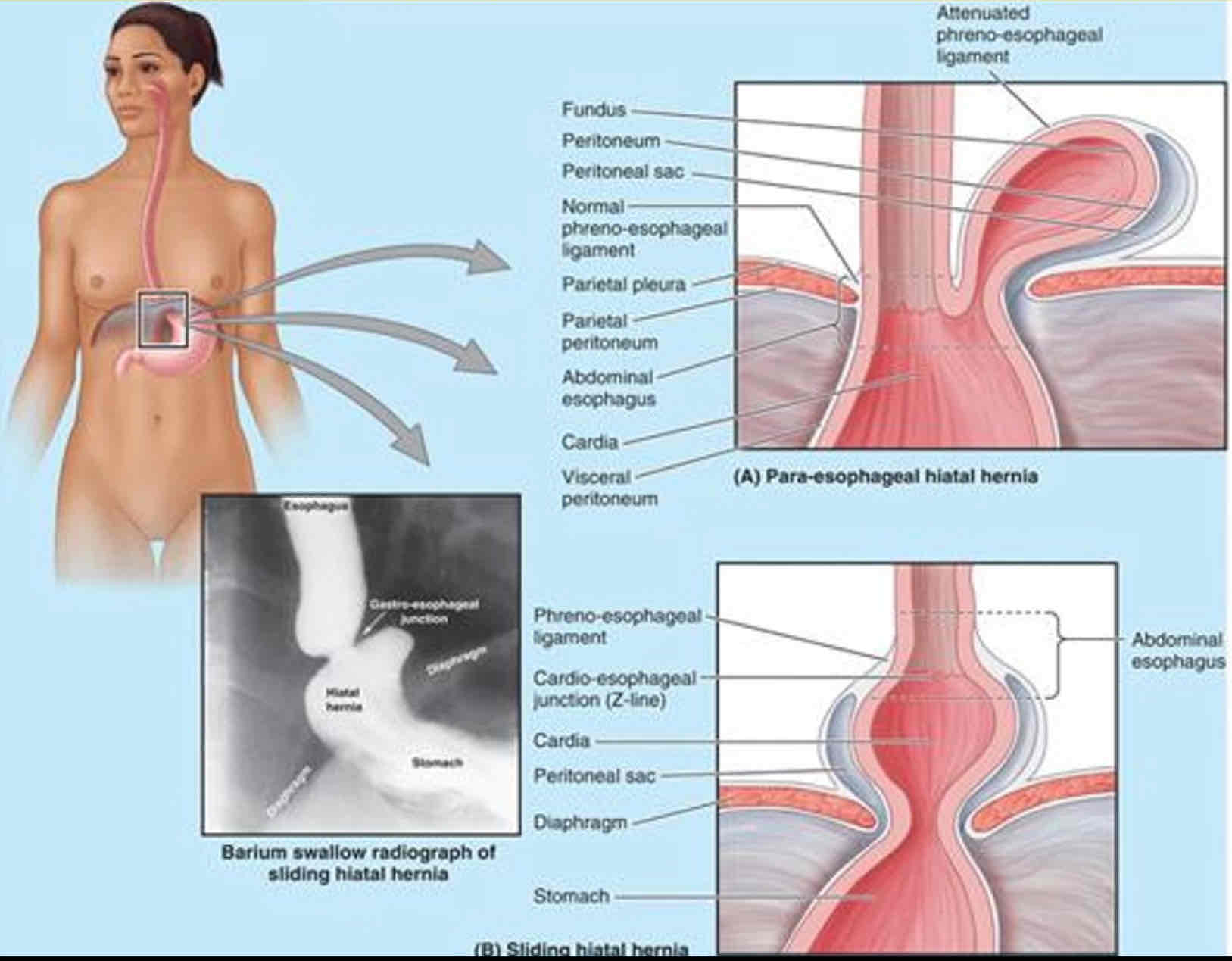
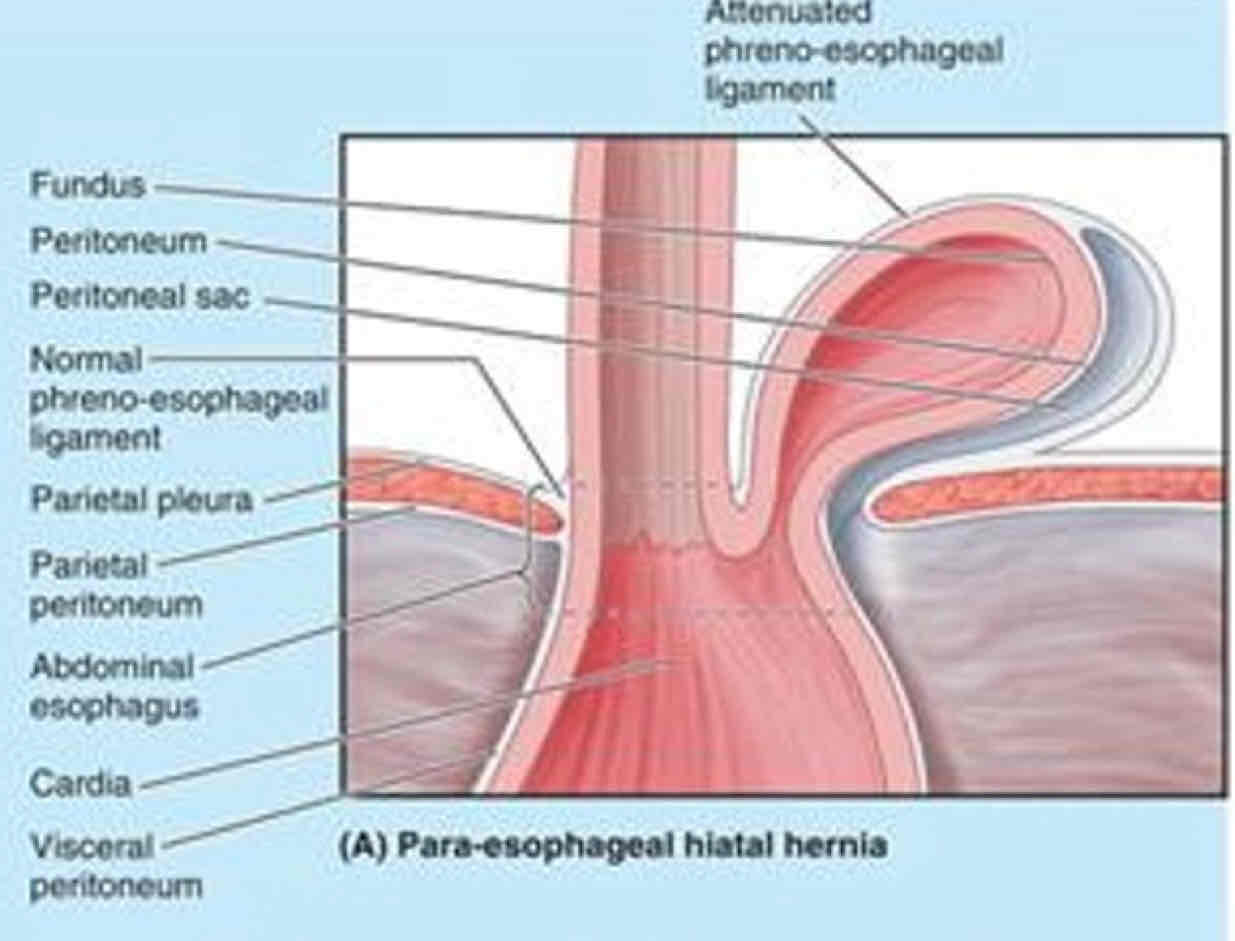
Para-esophageal Hernia
- Less common
- Fundus and pouch of peritoneum protrude
- No regurgitation because Cardia stays in place
Sliding Hernia is more or less common
More
Sliding Hernia
- Abdominal esophagus, cardia, and fundus move superiorly through hiatus when laying down or bending over
- Regurgitation possible due to weak right crus of diaphragm
What are Abdominal Hernias?
Occurs when a structure pierces the abdominal wall, creating a potential weakness
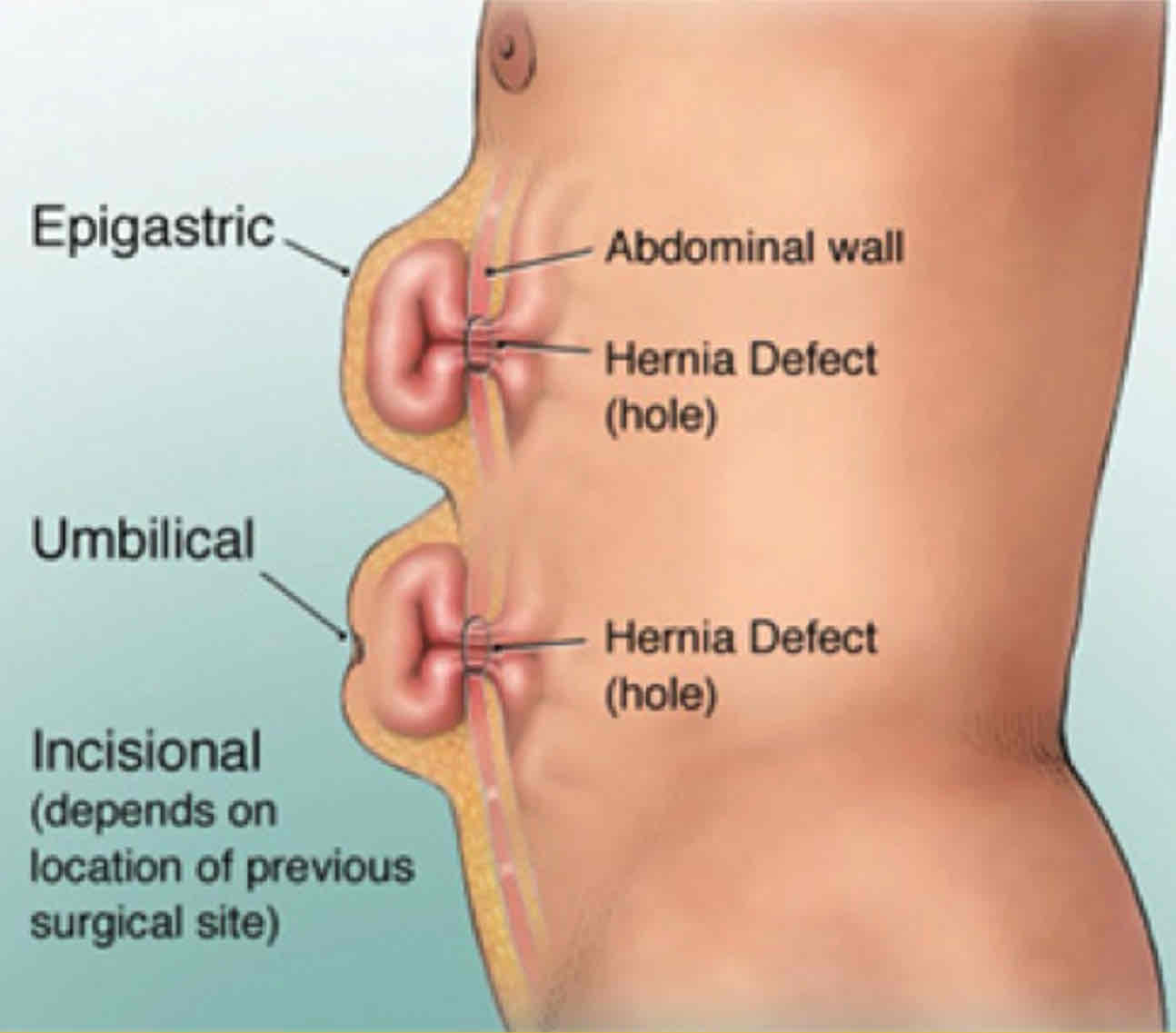
Type of Abdominal Hernias
Epigastric
Umbilical
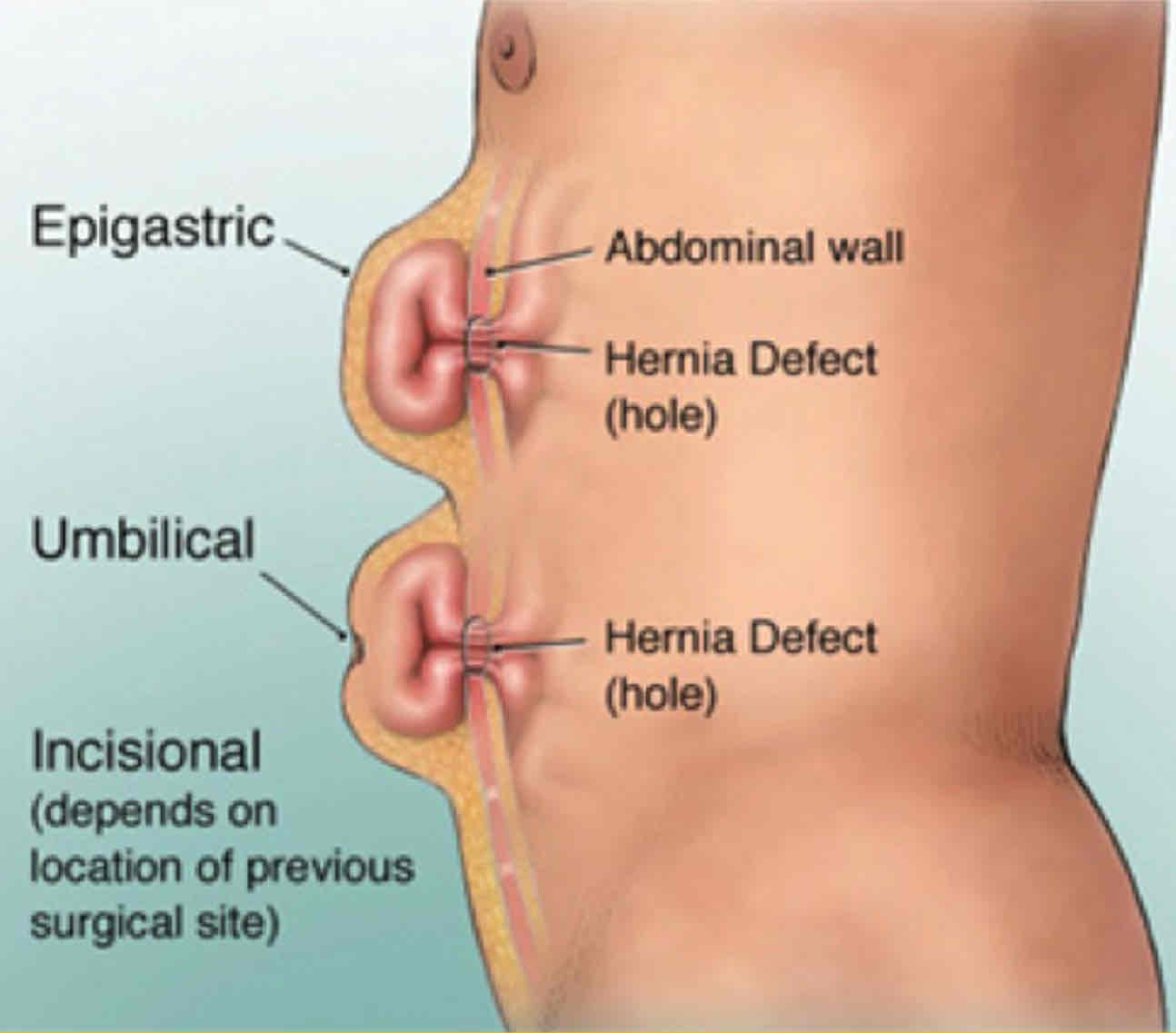
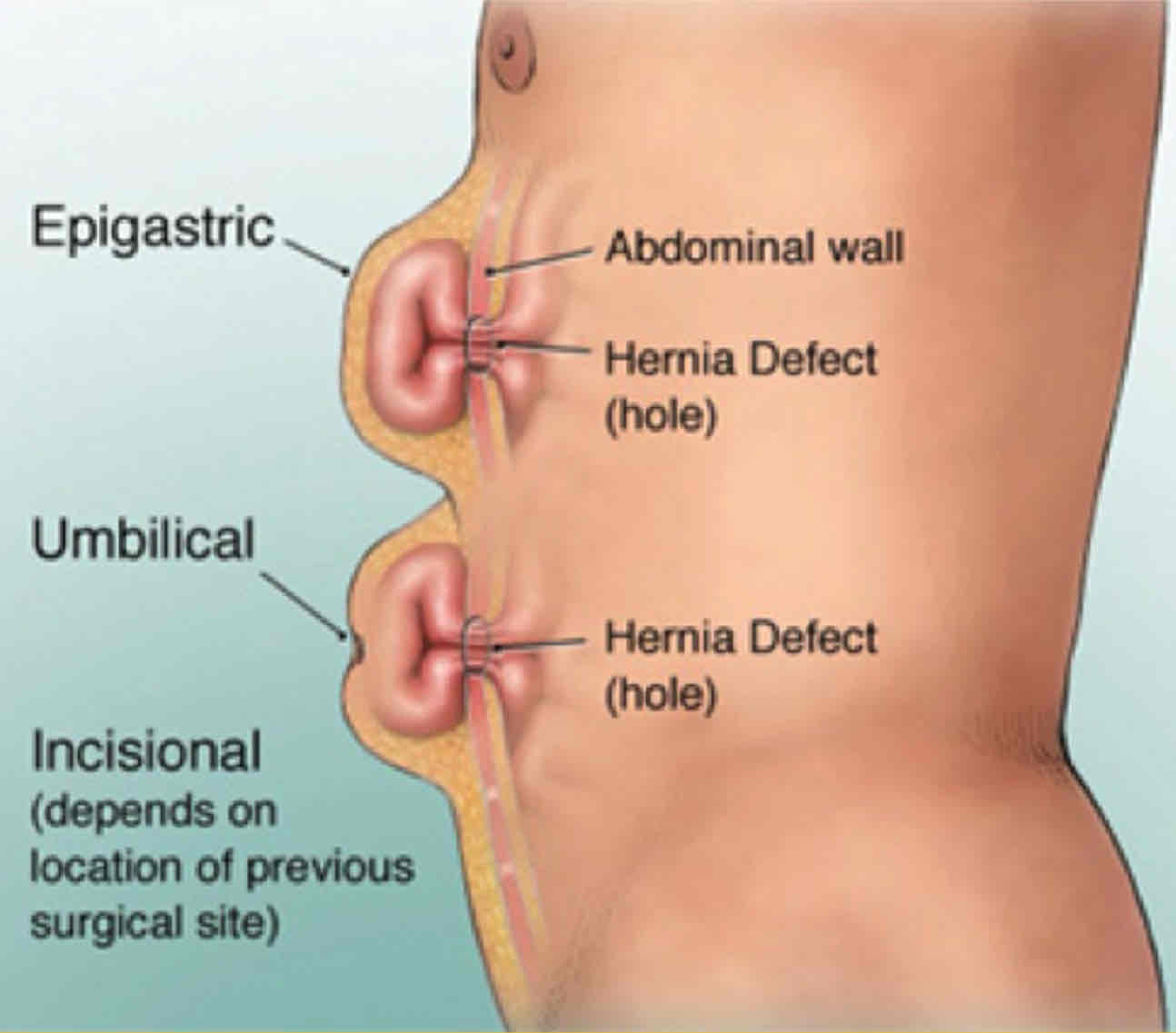
Epigastric Hernia
- Protrudes through Linea alba
- Usually fat lobules in the hernia
- Painful if nerves get compressed
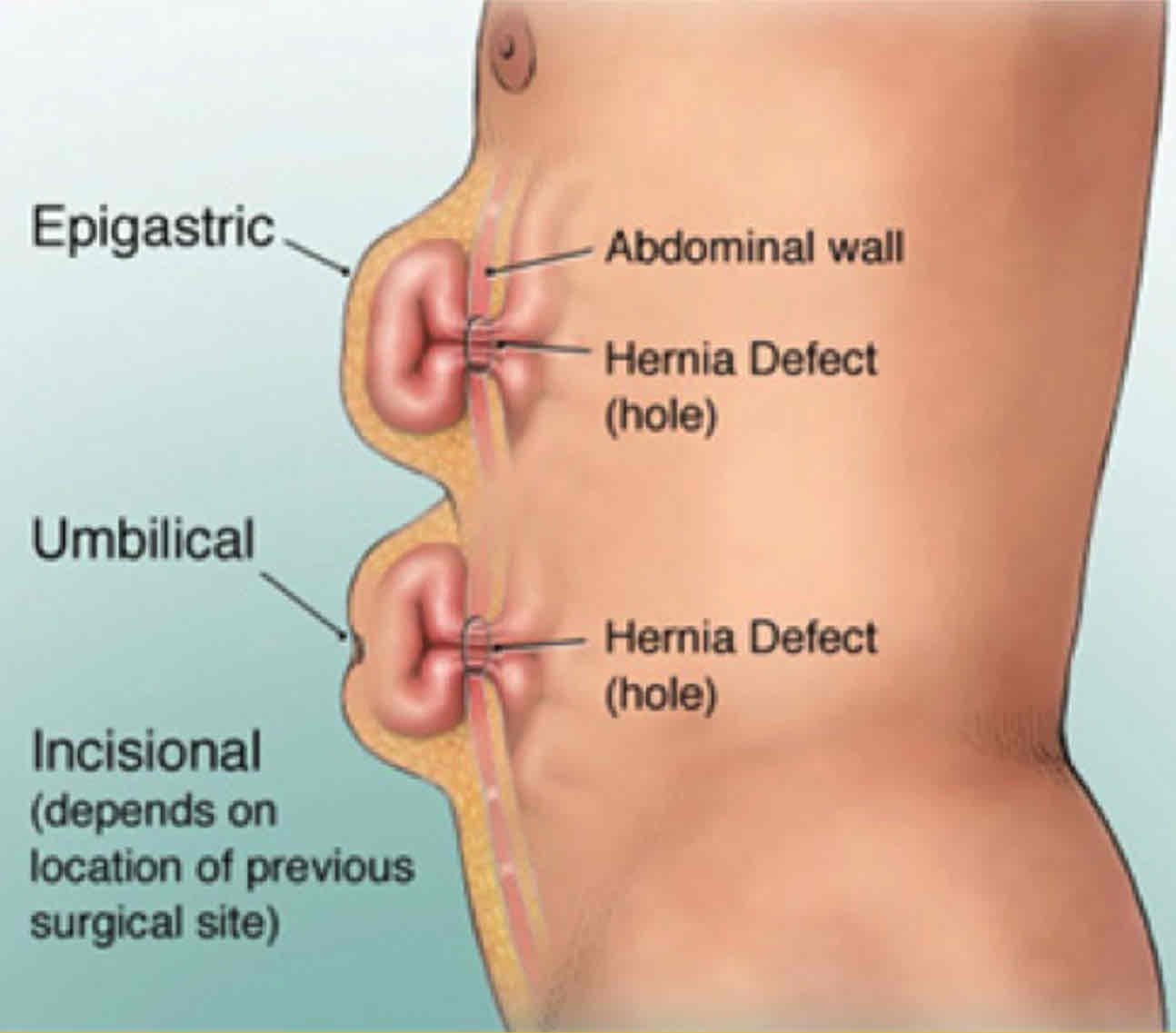
Umbilicial hernia
- Weakness from incomplete closure of umbilical ring
- Common in neonates
- Acquired in adults-most commonly women and obese individuals
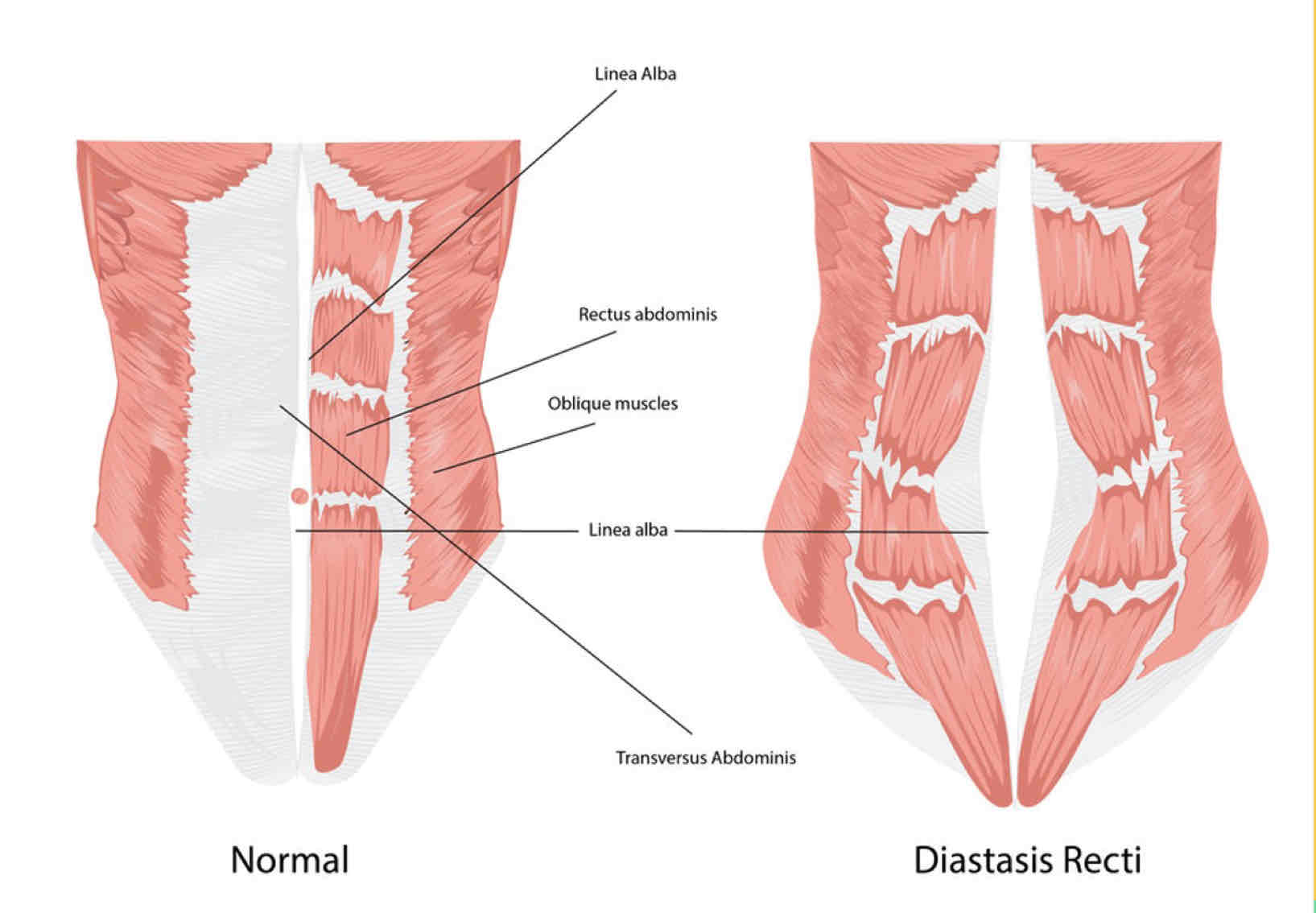
Diastasis Recti
- Linea Alba widens due to intra-abdominal pressure from pregnancy or obesity
- Rectus Abdominis columns separate creating area of weakness in anterior abdominal wall
- Structures can herniate in epigastric or umbilical regions
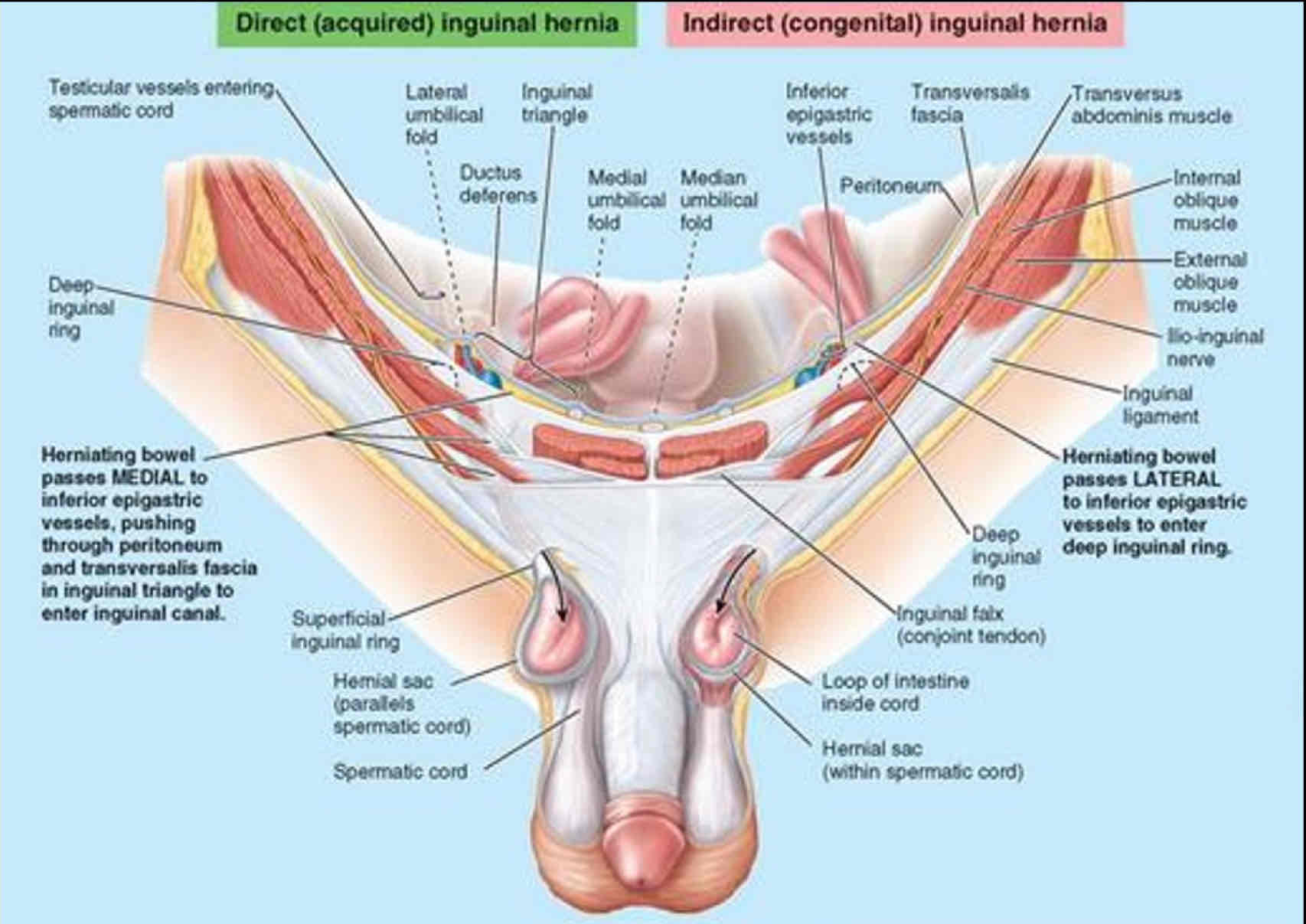
What are Inguinal Hernias?
Protrusions of parietal peritoneum and and viscera
- More common in males because of the passage of the spermatic cord through the inguinal canal
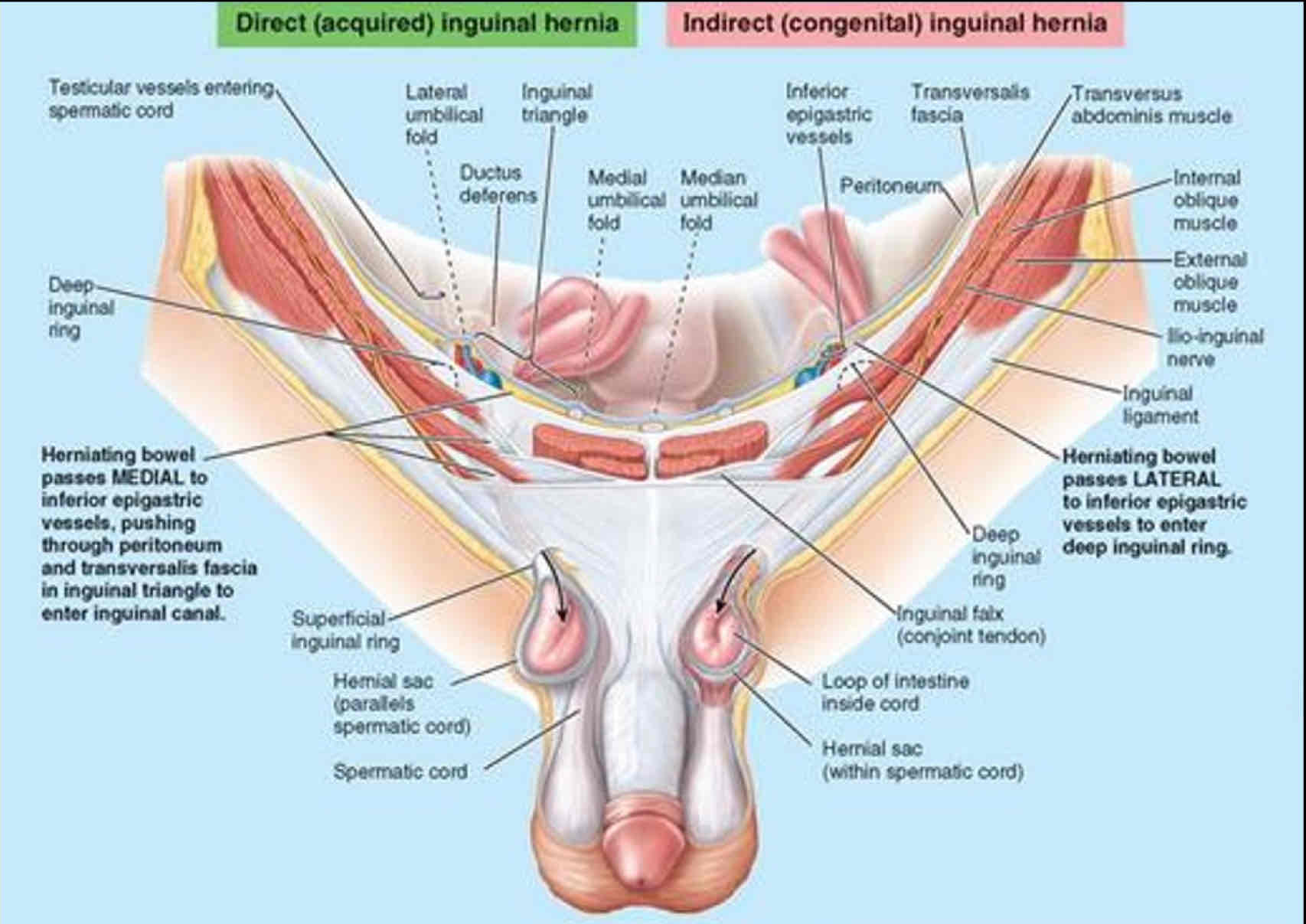
Types of Inguinal Hernias
Direct
Indirect
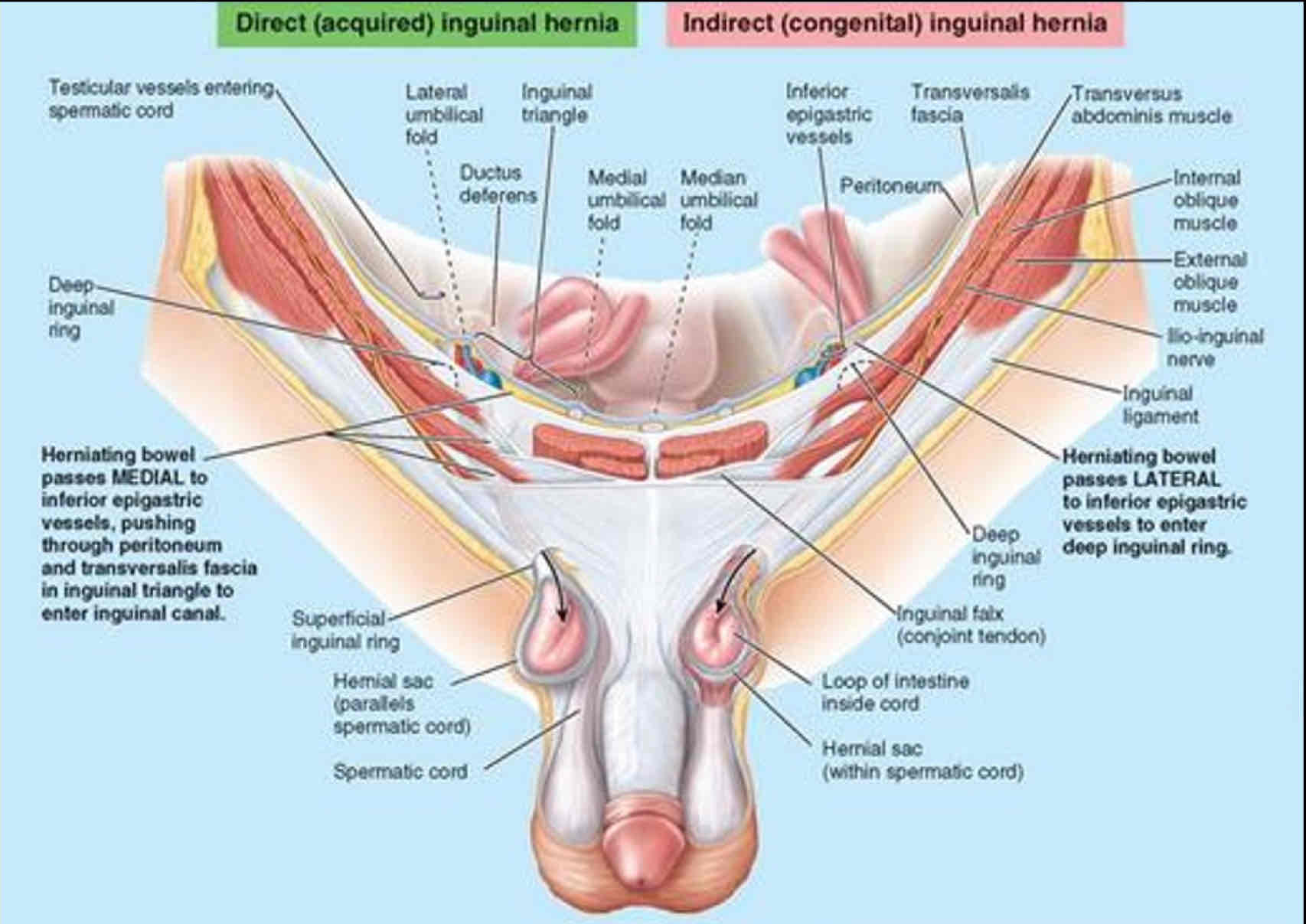
Direct Inguinal hernia
- Passes through or around inguinal canal
- Lateral to the spermatic cord
- Rarely enters the scrotum
- Palpable at superficial inguinal ring

Indirect inguinal hernia
- Most common type
- Inside spermatic cord
- The hernia passes down the inguinal canal and exits at the external inguinal ring into the scrotum.
- Palpable at superficial and deep inguinal rings
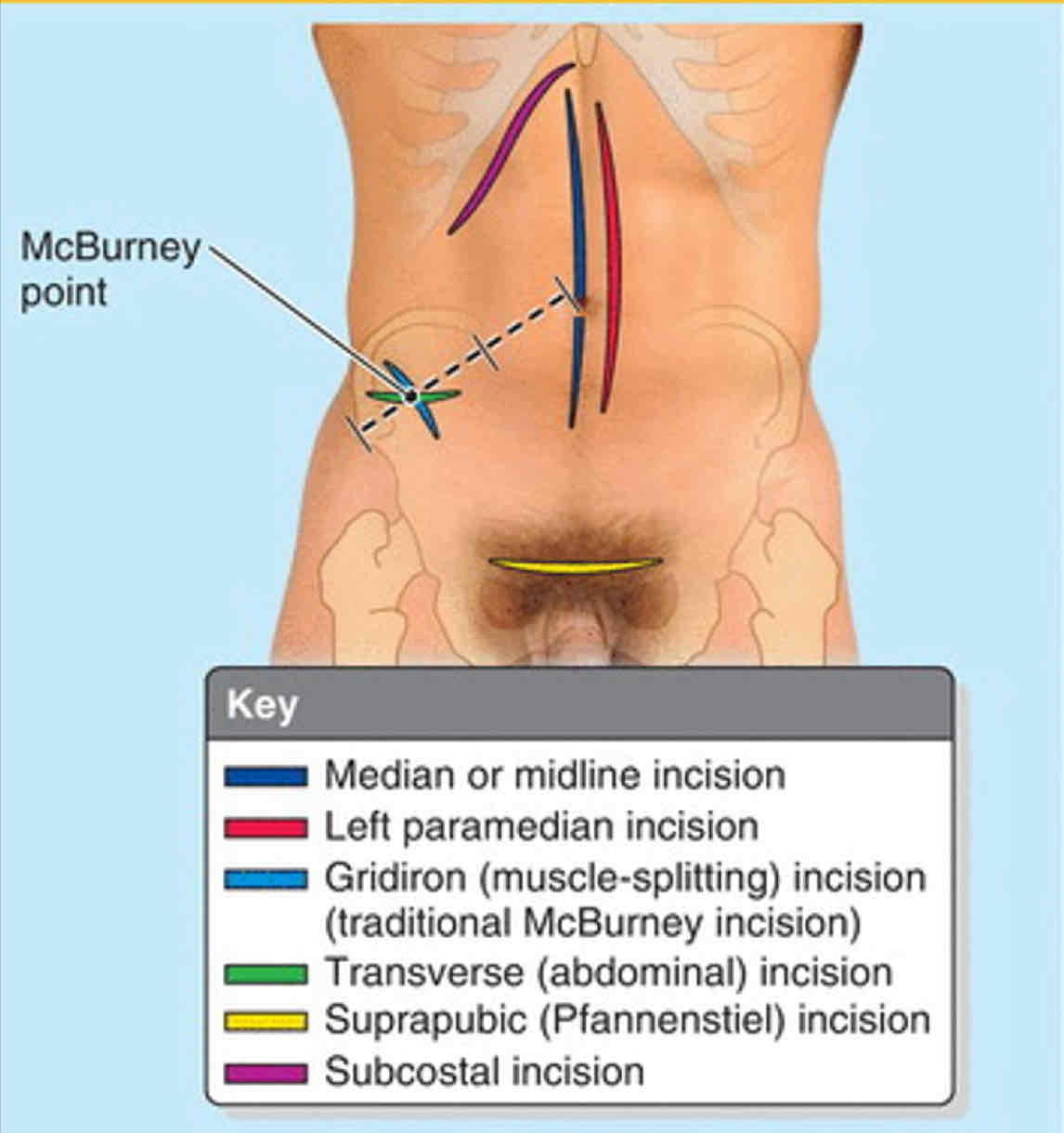
2 Gridiron incisions
McBurney
Suprapubic
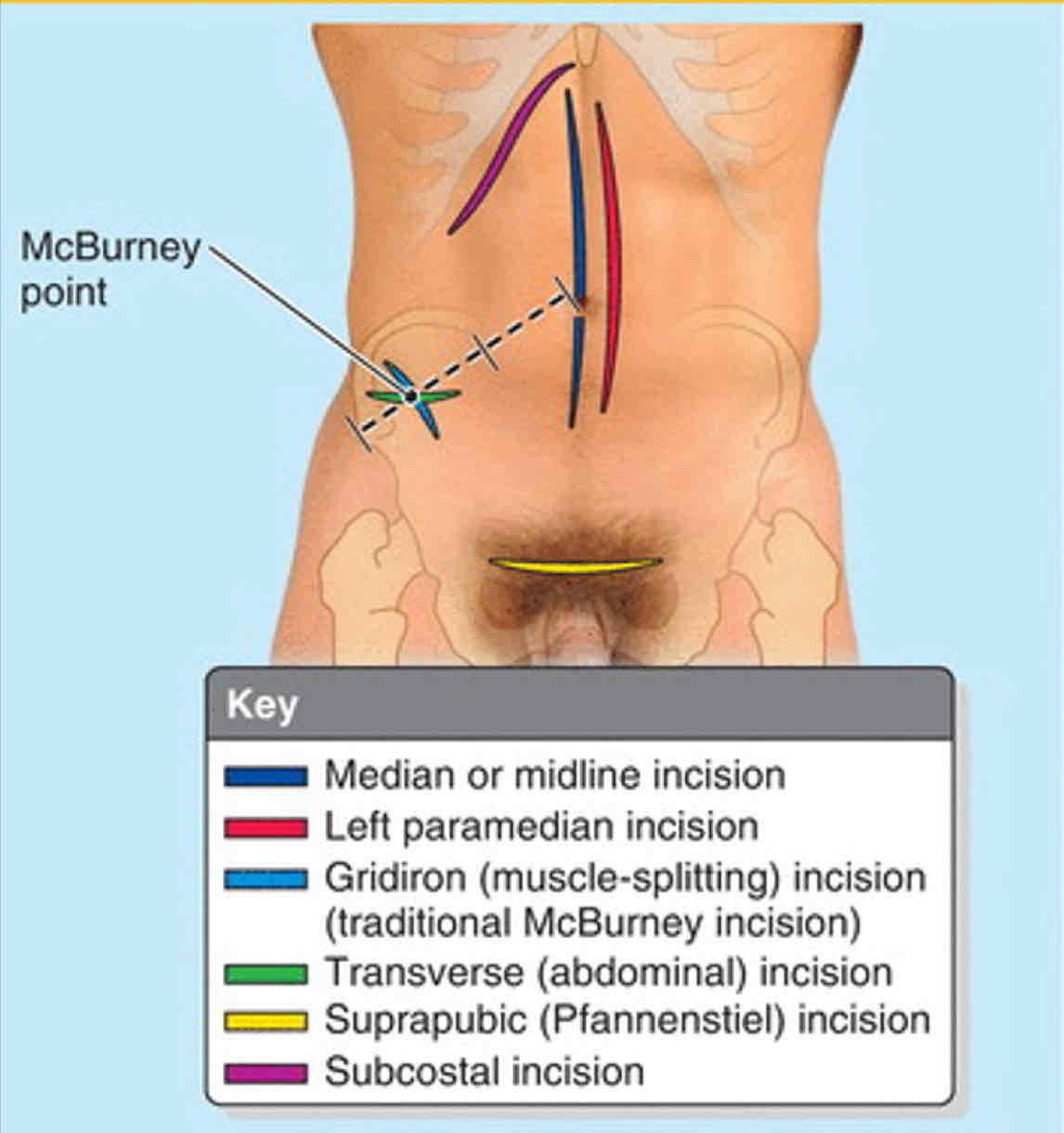
McBurney incision conditions
Appendectomy
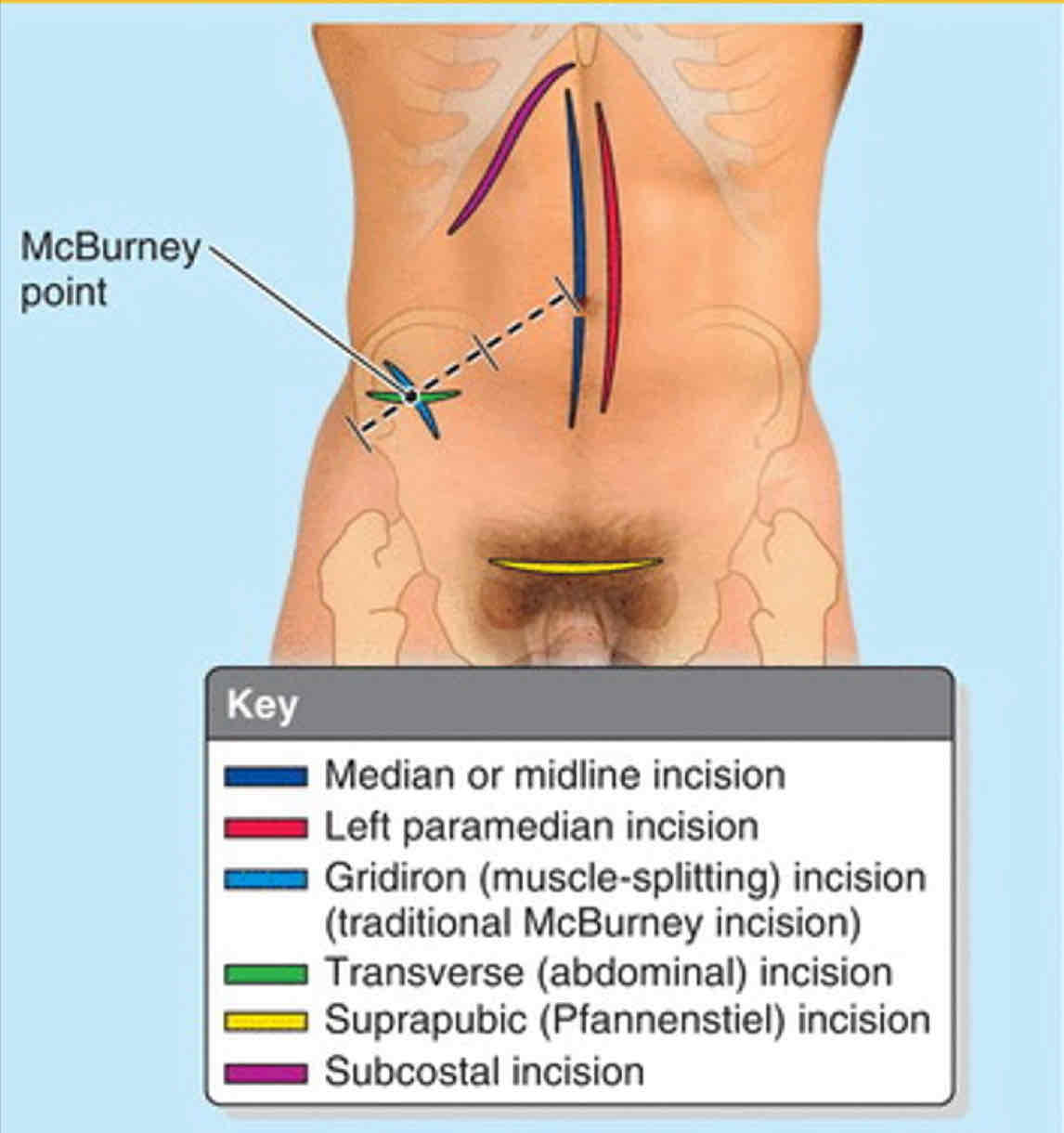
What gridiron incision spares muscle walls
McBurney
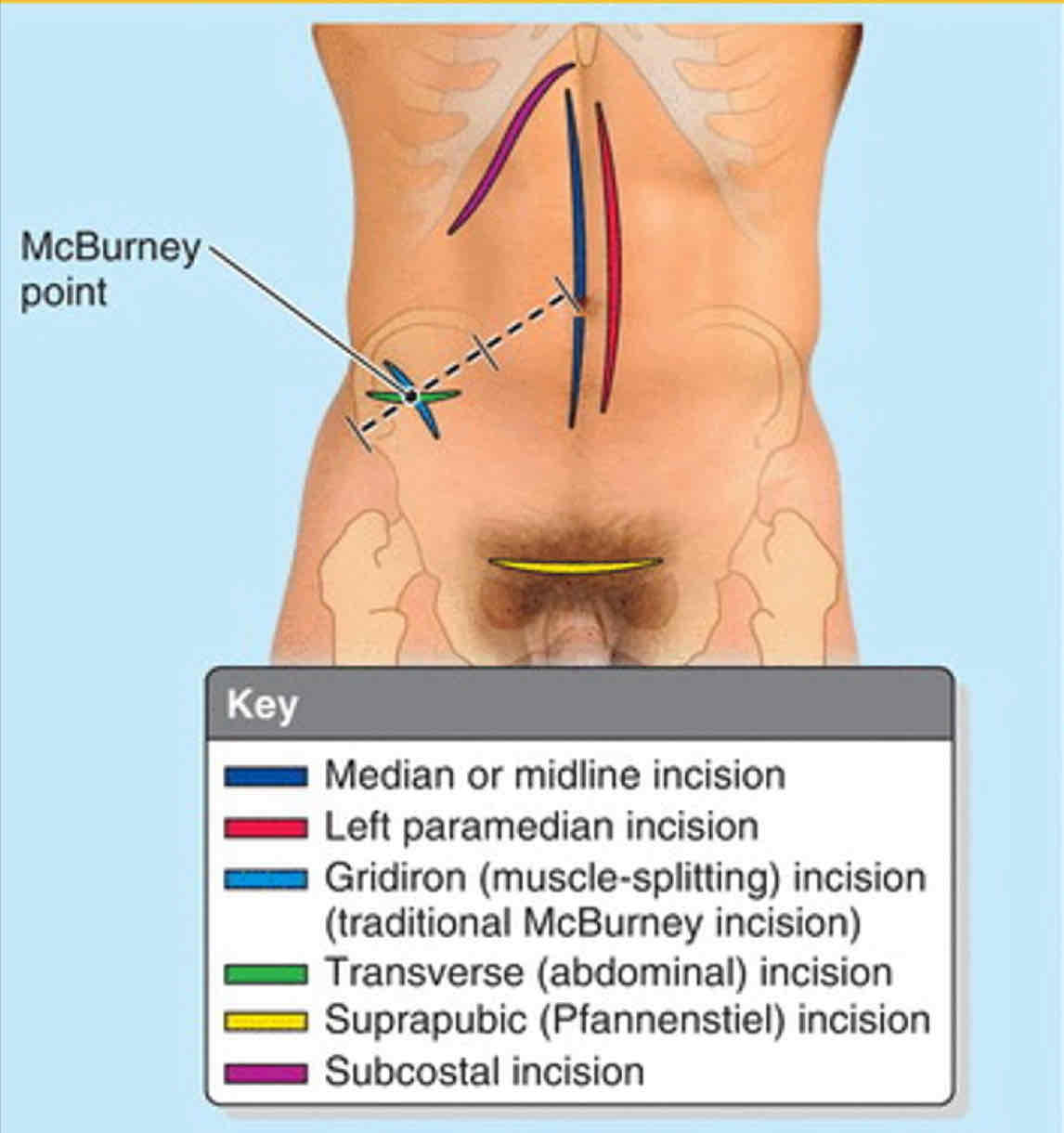
McBurney muscles
External Obliques
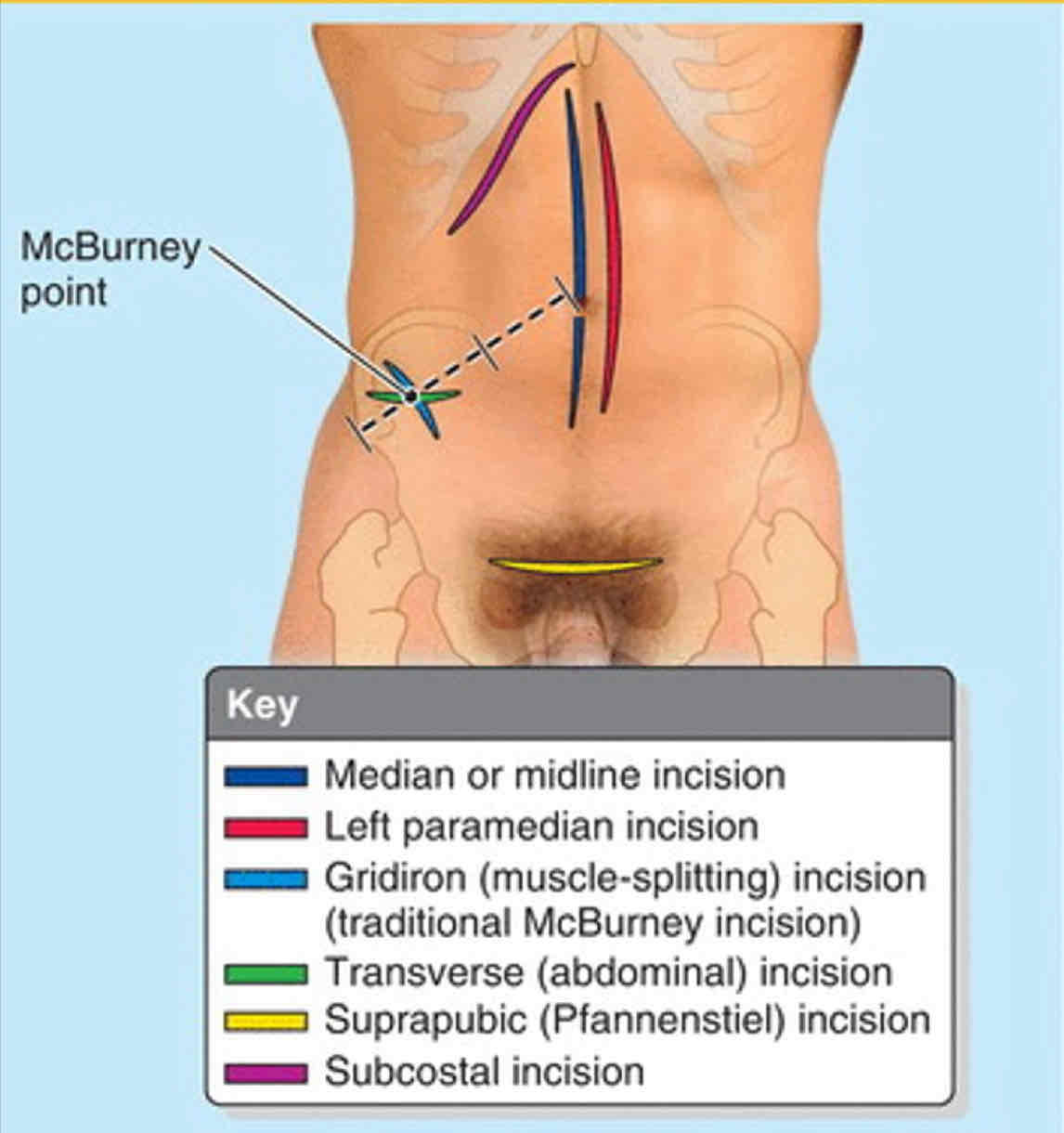
Suprapubic incision
“Bikini” Incision; A transverse incision just superior to the pubic hair line
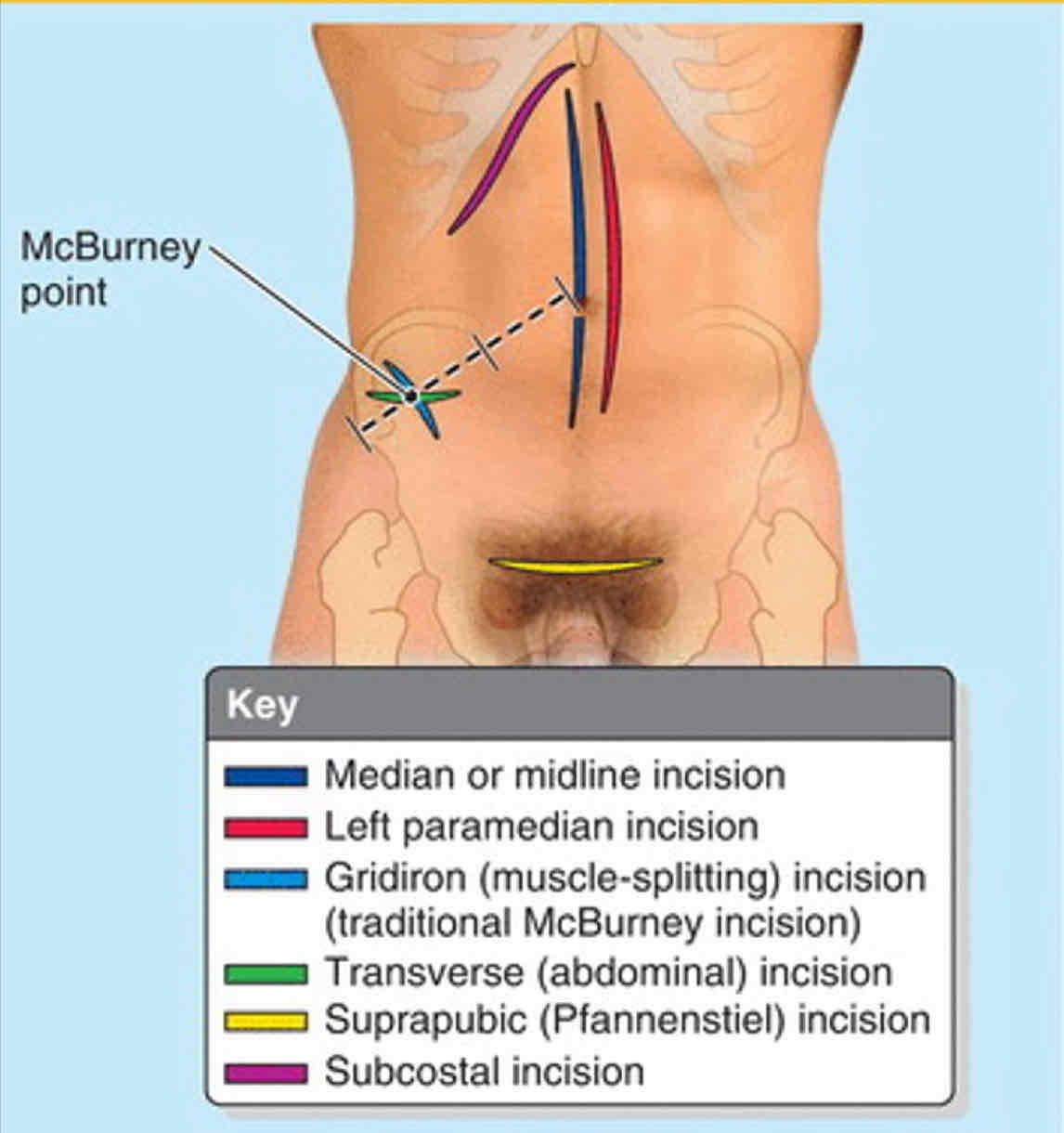
Suprapubic incision conditions
C-section
Peritonitis
Inflammation of the peritoneum, the serous membrane that surrounds the abdominal cavity and covers its organs
Peritonitis causes
Bacterial contamination from surgery
Traumatic penetration or rupture in gut
Peritonitis symptoms
Pain in overlying skin
Increased muscle tone
Tenderness, N/V, fever, constipation
Generalized Peritonitis
Widespread in peritoneal cavity
Dangerous & lethal because peritoneal surfaces rapidly absorb material
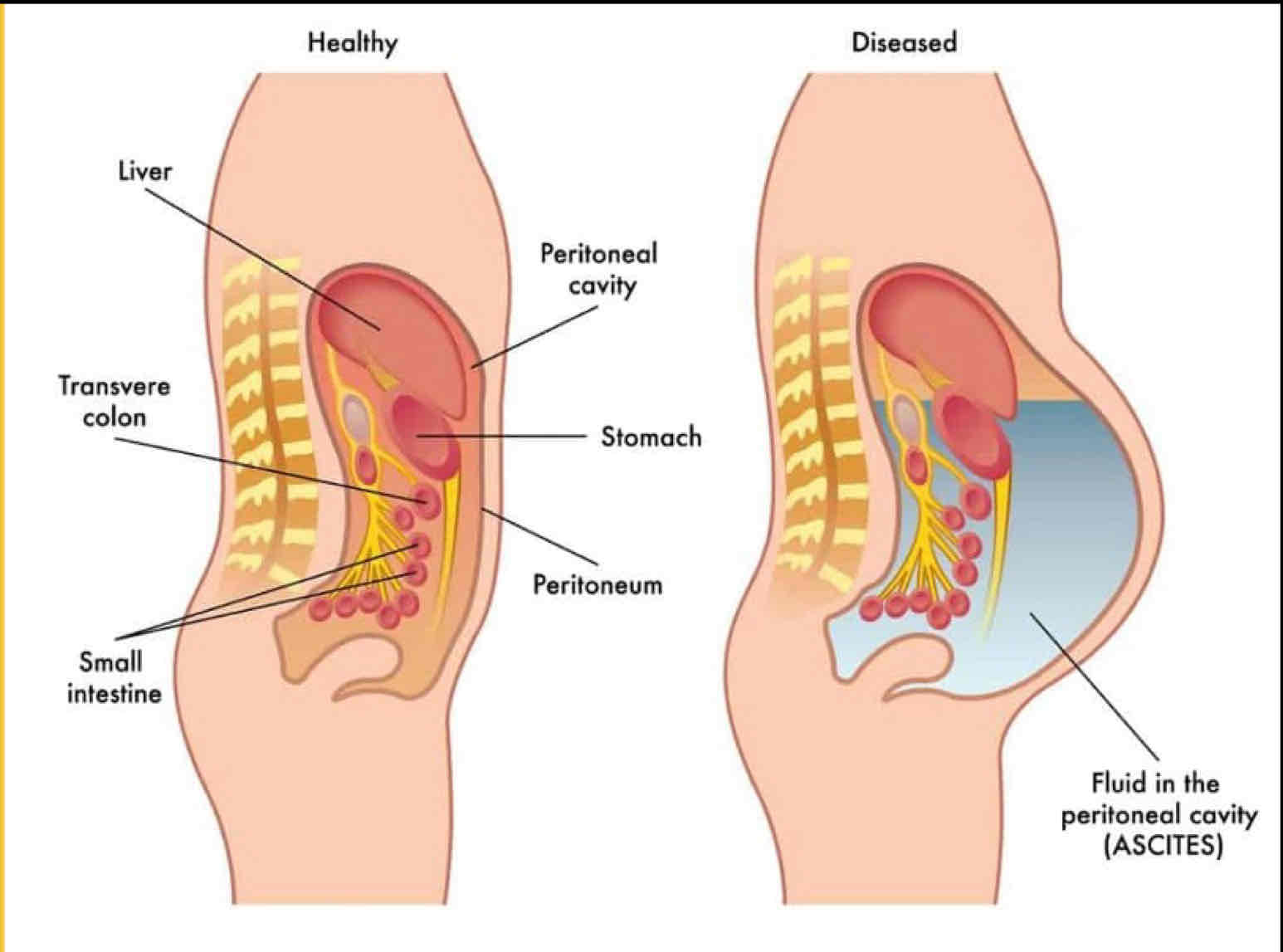
Acities
The accumulation of fluid within the peritoneal cavity
Distended abdomen
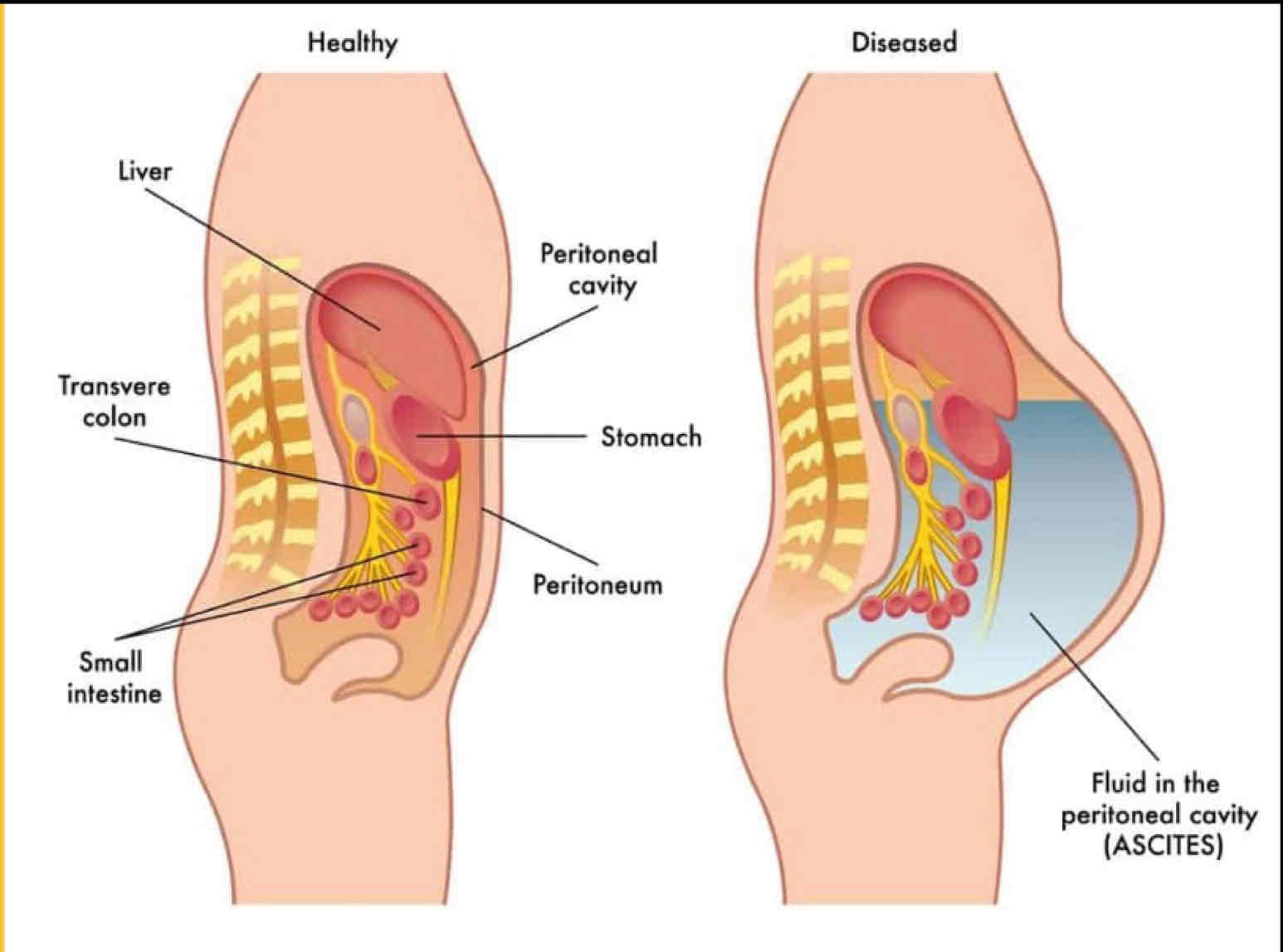
Ascites causes
Mechanical injury —> internal bleeding
Portal hypertension
Metastasis of CA cells
Starvation
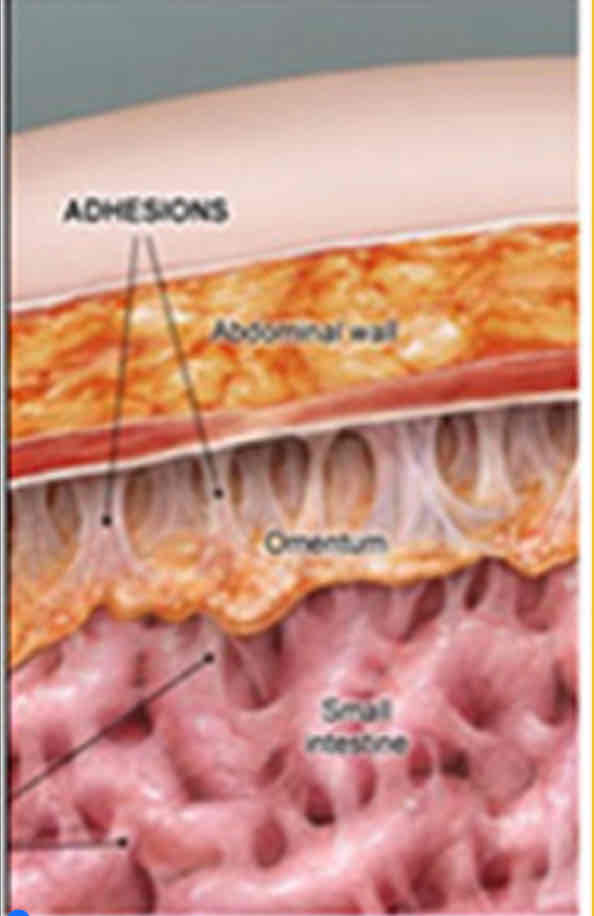
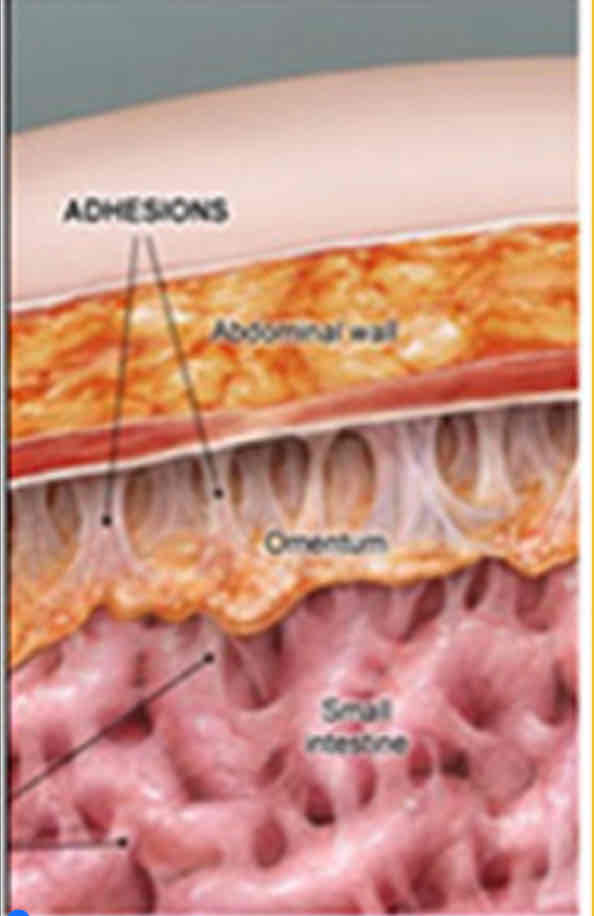
Peritoneal Adhesions
Adhesions = scar tissues
Peritoneum damage = inflamed surfaces = sticky from fibrin
Fibrin replaces with scar tissue during healing
Limits visceral movement, Causes chronic pain
Hiccups
Involuntary spasm of diaphragm
sudden inhalation
spasmodic closure of the glottis
Causes of hiccups
Irritation of afferent or efferent nerve endings, or medullary centers in brainstem
Indigestion
Diaphragm irritation
Alcoholism
Lesions disturbing phrenic nerves: cerebral, thoracic, abdominal
Diaphragmatic referred pain
Shoulders and Costal margins
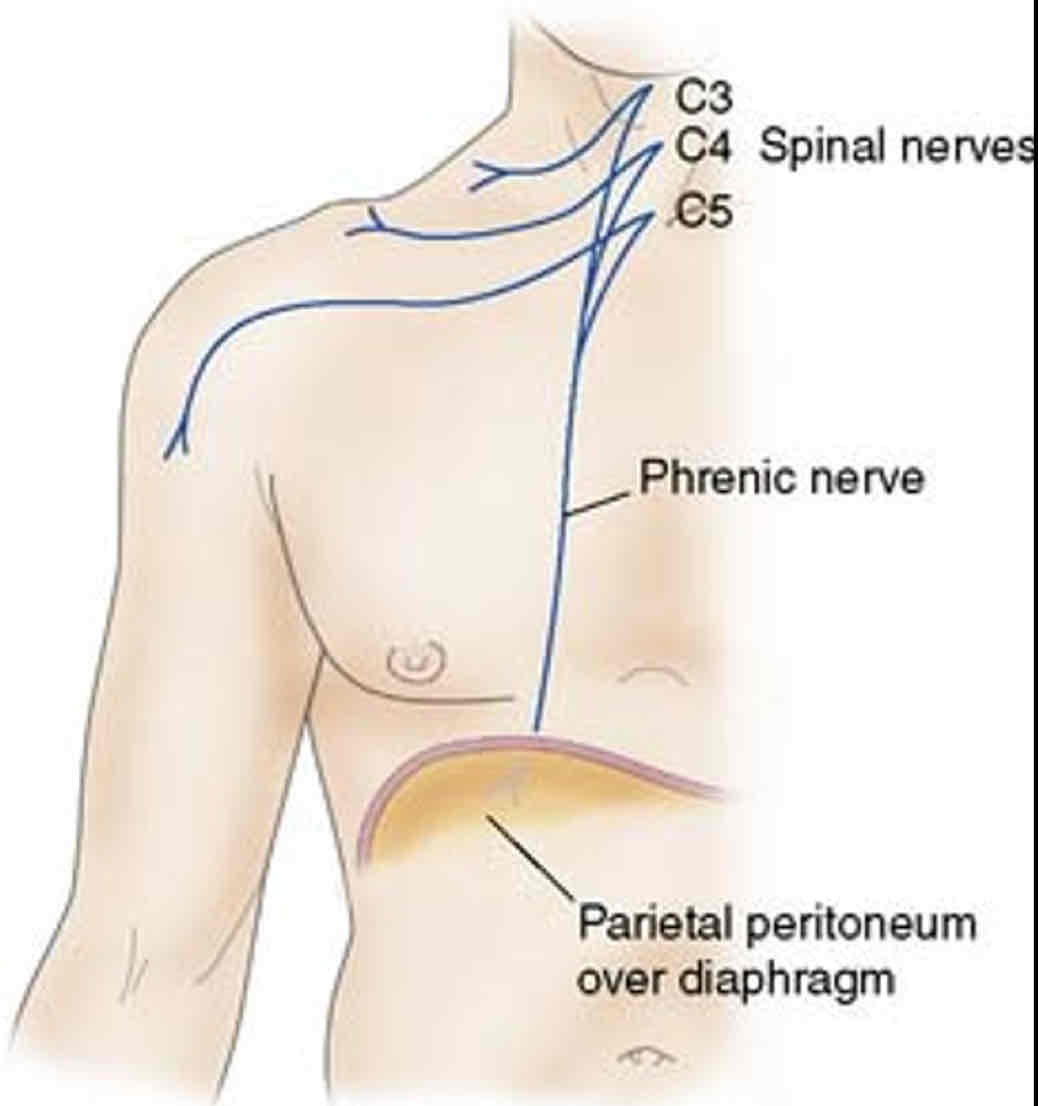
Phrenic diaphragmatic Pain
Shoulder
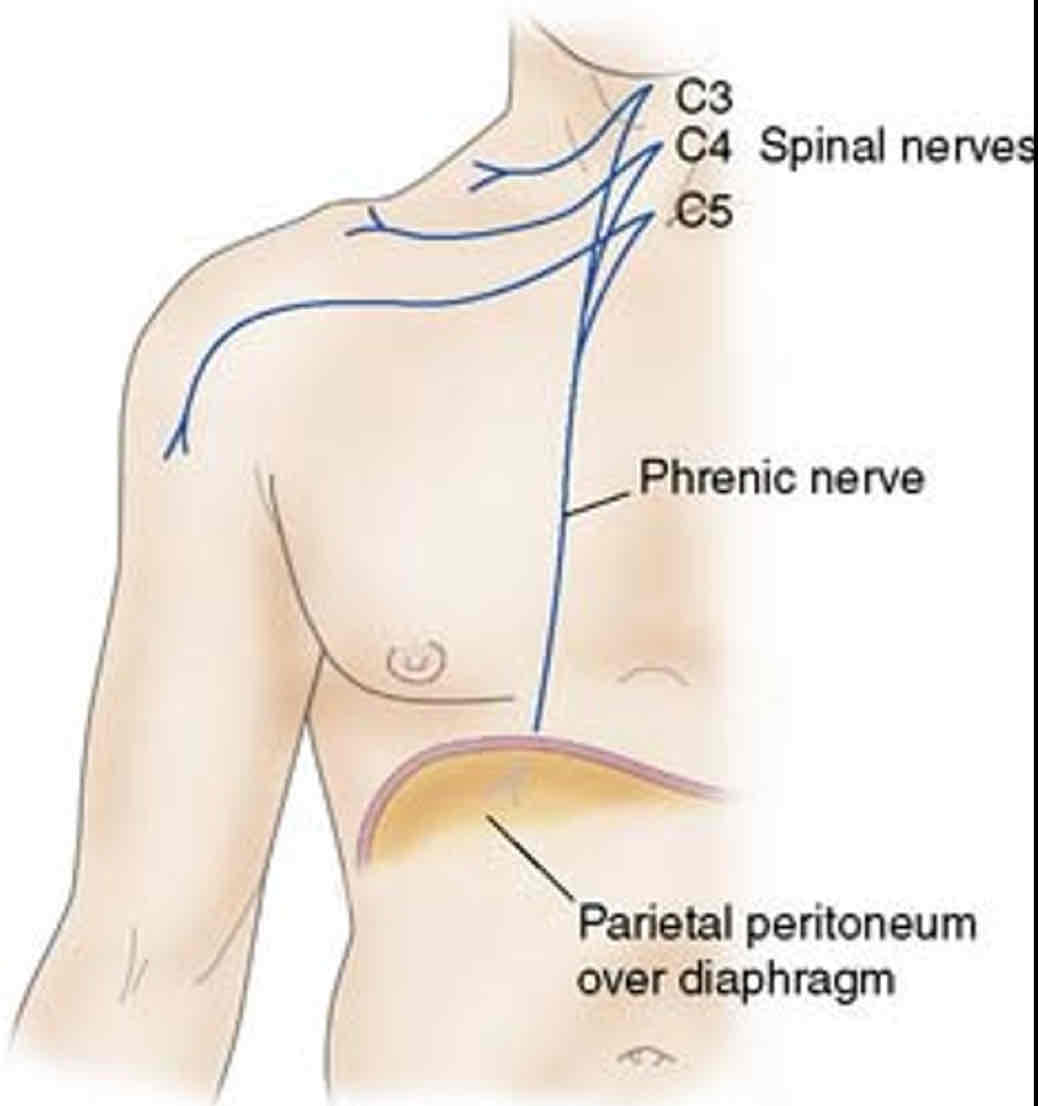
Inferior intercostal nerves diaphragmatic pain
Costal Margins
Abdominal Aortic Aneurysm (AAA)
Abnormal & excessive dilation or ballooning of abdominal aorta
Acute rupture = FATAL (90%)
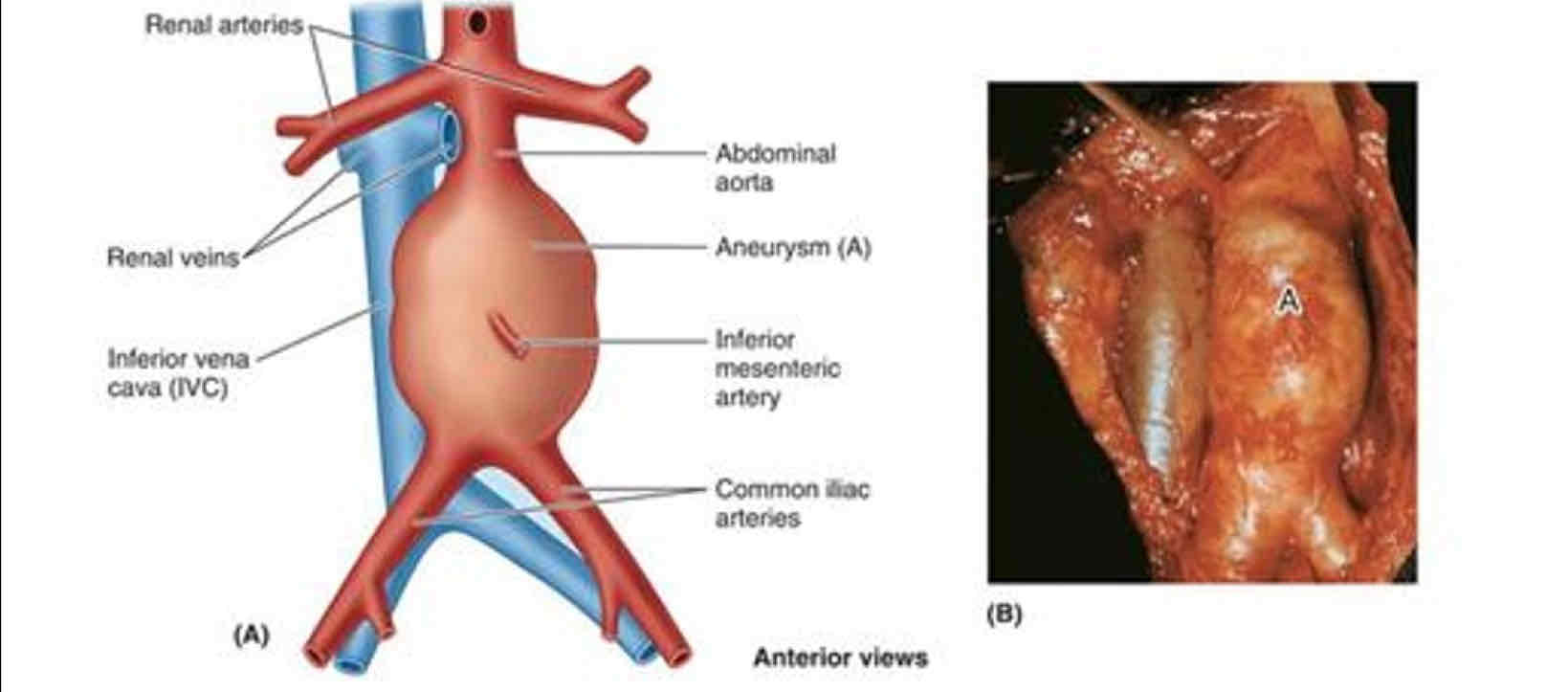
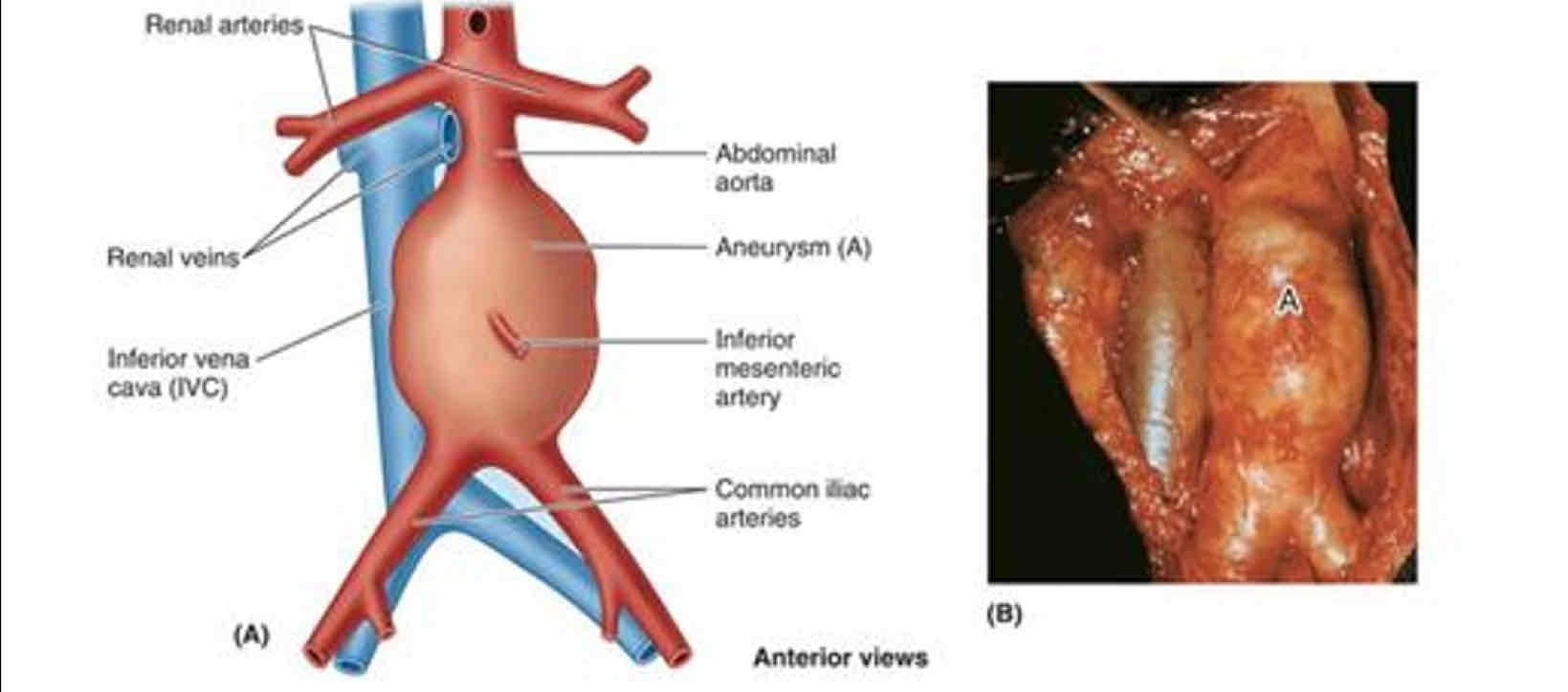
AAA causes
Congenital
Acquired weakness of arterial wall
Imaging confirms diagnosis
Distend
Expand; swell out
Ingest
To swallow for digestion
Digest
To break down food
Raphe
Seam of fibrous tissue
Navel
Umbilical
Decussate
Cross over
Rectus
Straight
Micturition
Urination
Defecation
Elimination of feces
Hernia
Protrusion of an organ or part through the tissues and muscles normally containing it
Spermatogenesis
Formation of sperm
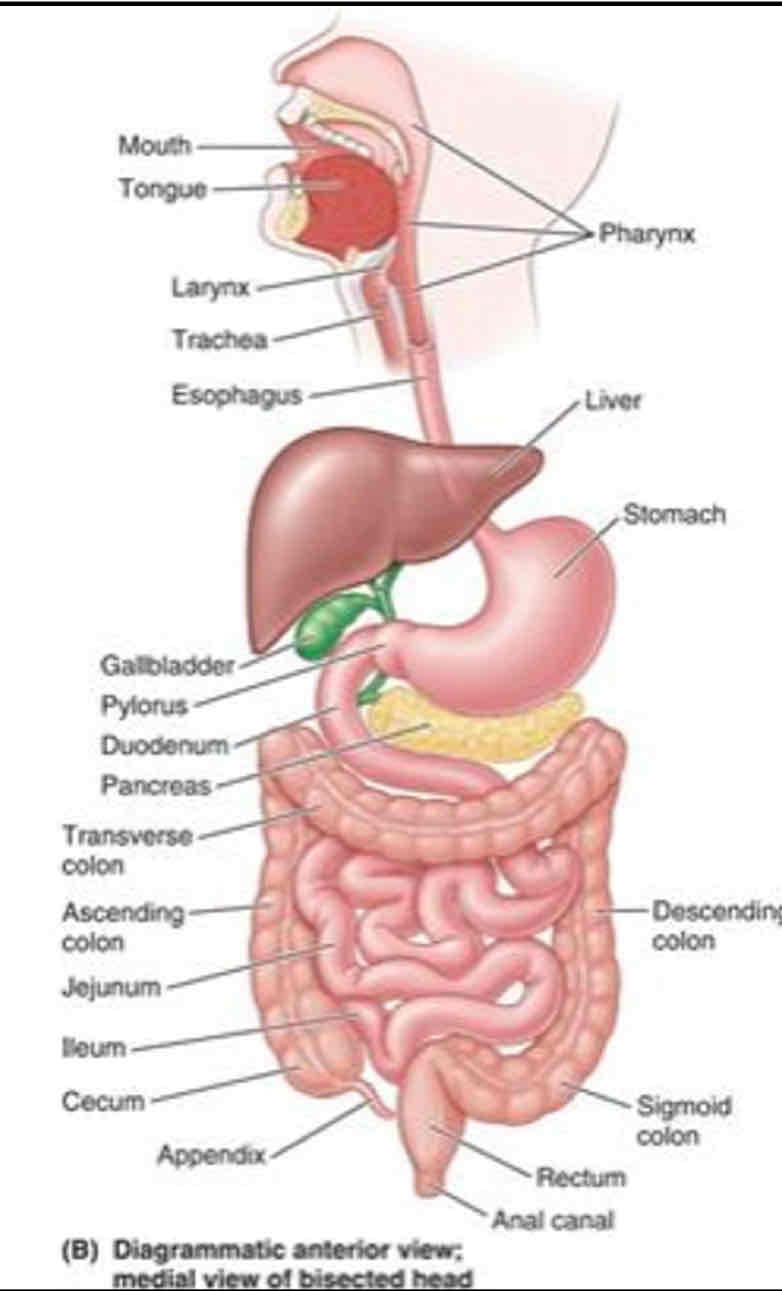
Path of food from entrance to exit
1. Mouth: teeth, tongue, salivary glands form bolus
2. Oropharynx: after being swallowed epiglottis closes over trachea
3. Esophagus
4. Stomach
5. Small intestine: Duodenum —> Jejunum —> Ileum
6. Large intestine: Cecum —> Ascending Colon —> Transverse Colon —> Descending Colon —> Sigmoid Colon
7. Rectum
8. Anal canal