GI: diarrhea and malaria
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Types of diarrhea
Acute watery diarrhoea: Diarrhoea that lasts less than 14 days.
• Dysentery: Diarrhea with visible blood in the faeces.
• Persistent diarrhea: Diarrhoea that begins acutely, but is of unusually long duration; lasting 14 days or more. It may begin as watery diarrhoea or as dysentery
Chronic diarrhoea, which is sometimes used interchangeably with persistent diarrhoea, actually refers to long-lasting (≥14 days) or recurrent diarrhoea that is not associated with an infectious cause.
Cholera: copious diarrhea and severe vomiting
Mechanisms of watery diarrhea
Secretion:It is characterized by abnormal secretion of fluid and electrolytes into the small bowel
Osmosis: When a poorly absorbed, osmotically active substance is ingested, water moves from the ECF into the bowel, thus increasing stool volume and causing dehydration.
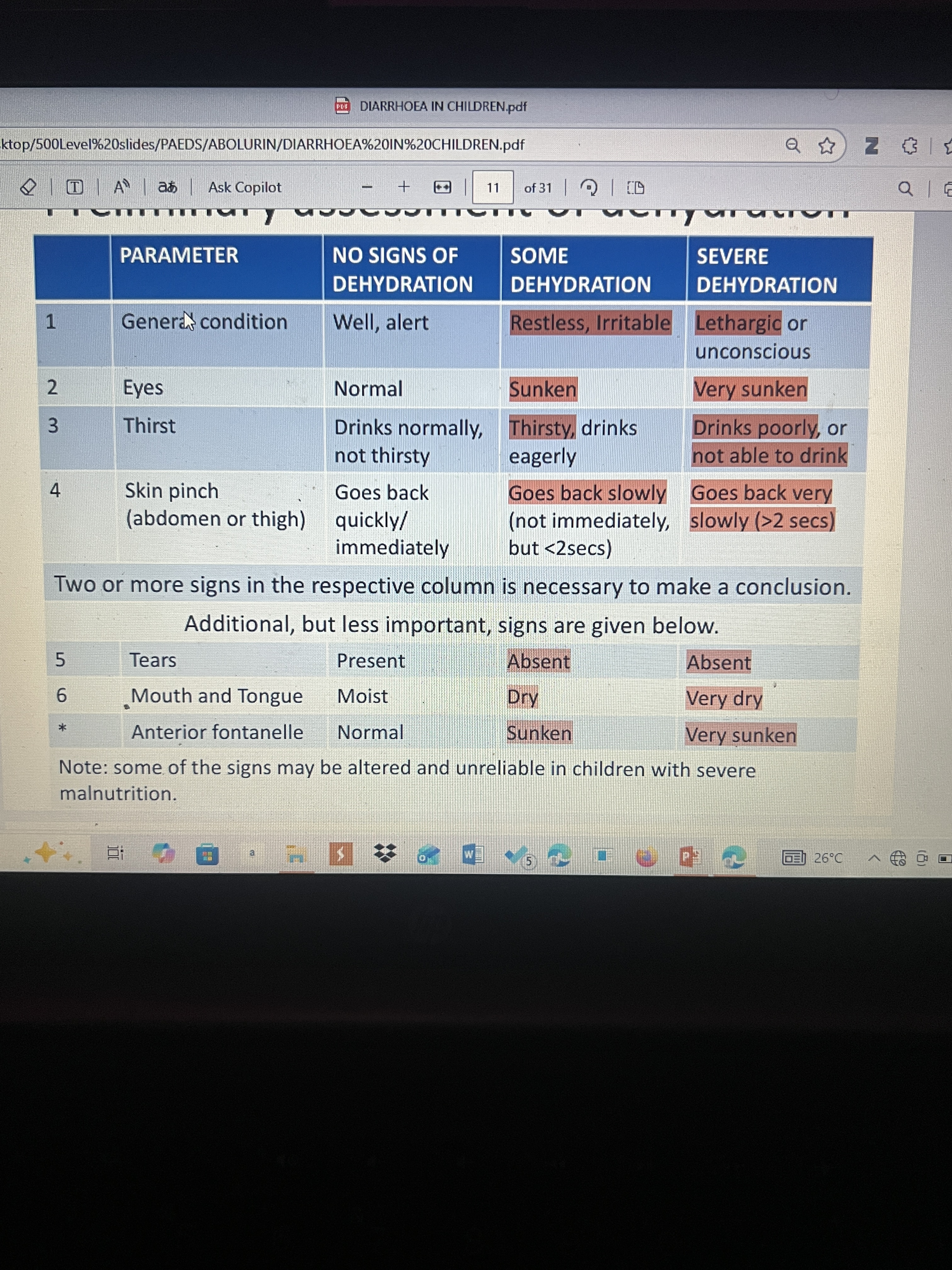
Assessment of dehydration
Mild: <5% infants <3% older children
Moderate: 5-10%, 3-6%
Severe: >10%, >6%
Problems associated with diarrhea
Malnutrition
• Fever
• Vomiting
• Excessive weakness • Rash
• Convulsion
• Sepsis
Treatment of no signs of dehydration
50-100 ml of ORS or SSS given after each loose stool if <2yrs, and 100-200mls if >2yrs.
Treatment of some Dehydration
Diarrhoea Treatment Unit’ (DTU) or ‘ORT corner’ of the health care facility. After being re-assessed to be improving, treatment can be continued at home.
75mls/kg of ORS over 4 hours.
Severe dehydration treatment
intravenous rehydration. 100mls/kg of IV fluid should be given over a total of 3 hours (for older children) or 6 hours (for infants).
30ml/kg over one hour, followed by 70ml/kg over the next 5 hours.
• For older children, 30ml/kg over 30 mins, followed by 70ml/kg over the next 2.5 hours
Preferred fluids
Maximum rate for ng tube and why?
When do you not give ors?
Ringers Lactate/Hartmann’s
Normal saline
Half strength Darrows
Note: dont give dextrose water only!
In exceptional cases where IV therapy is not possible, a nasogastric tube can be used to give ORS solution at about 20ml/kg/hour. This rate of NG tube infusion should not be exceeded so as to avoid abdominal distension and repeated vomiting.
W• ORS should not be given to patients who have paralytic ileus
Common electrolyte abnormalities
How are they treated?
Hypokalaemia: Serum K+ <3.5mmol/L
• Hyponatraemia: Serum Na+ <135mmol/L
• Hypernatraemia: Serum Na+ >150mmol/L
• Metabolic acidosis: Serum bicarbonate <20mmol/L
With ORS!
Old ORS consists of?
New ORS consists of?
90mmol/L of sodium
111mmol/L of glucose
80mmol/L of chloride,
20mmol/L of potassium
10mmol/L of citrate (equivalent to about 30mmol/L of bicarbonate) , giving a total osmolarity of 311 mmol/L.
75mmol/L of sodium,
75mmol/L of glucose,
and 65mmol/L of chloride
20mmol/L of potassium,
10mmol/L of citrate (equivalent to about 30mmol/L of bicarbonate)
, giving a total osmolarity of 245 mmol/L.
Reduced stool output and vomiting during treatment
How to prepare SSS
SSS is prepared by adding 6 level teaspoons of sugar and half level teaspoon of salt to one litre of water.
Other treatments of diarrhea
Zinc: 10-20mg for 10-14days
Antibiotics in dysentery and cholera
Vitamin A supplements in severely malnourished children
Antibiotics
Cholera: erythromycin, azithromycin
Shigella: ceftriaxone
Amoebic dysentery: metronidazole
Giardiasis: metronidazole
Methods of transmitting malaria
Mosquitoes ingest? Inject?
Bite of a female anopheles mosquito
Blood transfusion
Congenital malaria
Gametocytes
Sporozoites
Diagnosis of severe malaria
Asexual forms of p. Falciparum on a blood film: trophozoites and schizonts
With any of the clinical or lab findings
cns: unarousable coma, multiple convulsions, prostration
Hematology: severe anaemia: haemoglobin concentration <5g/dL or a haematocrit of <15%
– haemoglobinuria: cola/dark coloured urine
circulatory collapse or shock
– jaundice
– abnormal spontaneous bleeding
Renal
– oliguria/ renal impairment
Metabolic
– hypoglycaemia: blood glucose <2.2mmol/L or <40mg/dl
Respi
– respiratory distress/ metabolic acidosis
– pulmonary oedema
Diagnosis of malaria
PBF, stains, what they stain for?
Others?
PBF🥇: thick: presence of parasites, giemsa stain
Thin: species of parasites, leishman stain
RDT: detect specific antigens produced by malaria parasites
PCR:
Recommended ACTs
Artemether + Lumefantrine (aka Coartem, Lonart, combisunate etc).
Artesunate + Amodiaquine (aka Camosunate).
Dihydroartemisinin-piperaquine (aka P- Alaxin).
Artesunate-Pyronaridine
Artesunate-Mefloquine • Artemisinin-Piperaquine
What is the dose of AL
Given twice daily (bd) for 3 days. Each tablet contains 20mg Arthemeter and 120mg Lumefantrine.
●Weight 5-14kg: 1 tablet bd
●Weight 15-24kg: 2 tablets bd
●25-34kg: 3 tablets bd
●≥35kg: 4 tablets bd
2nd dose, 8hrs after first dose on day 1. Subsequent doses 12hrs apart
Does of AA
4.5kg- <9kg (or 2-11 months): 25mg/75mg satchets
● >9kg- <18kg (or 1-6 years): 50mg/150mg satchets
● 18kg- <36kg (or 7-13 years): 100mg/300mg tablets; 1 tablet daily.
● ≥36kg (or ≥14 years): 100mg/300mg tablets; 2
Indications for admission of uncomplicated malaria
Recurrent vomiting
To pacify parental anxiety
Principles of treatment of severe malaria
Specific antimalarial treatment:
Treatment of specific complications.
Supportive treatment.
What is the dose of IV artesunate
• For children < 20 kg: 3.0 mg/kg per dose.
• For children > 20 kg and adults: 2.4 mg/kg per dose.
• Give at 0 hr, 12 hr and 24 hr, then once daily thereafter. i.e.
– Dose 1: on admission (0 hr)
– Dose 2: 12 hours later.
– Dose 3: 12 hours after second dose.
– If still very ill after 24 hours, give same dose daily until patient can tolerate oral
After which a full 3day course of ACT should be given as follow on treatment
Alternatives to IV artesunate
Intramuscular Artesunate injection.
– Intramuscular Arthemether injection: 3.2mg/kg daily for 3 days.
– Intravenous Quinine: given as infusion. Loading dose of 20mg/kg Quinine
IM quinine
Complications of quinine use
Treatment of complications and supportive treatment
To diagnose cerebral malaria
Coma: GCS<11, BCS:<3
Confirmation of asexual forms of P. falciparum on a peripheral blood smear.
• Exclusion of other causes of encephalopathy/coma
Complications of cerebral malaria
– Cortical blindness⭐️
– Motor spasticity: hemiplegia, quadriparesis
– Ataxia and dystonia
– Aphasia⭐️
– Behavioural disorders⭐️
– Impairment in attention and learning, including ADHD.⭐️
– Mental subnormality
– Seizure disorder.⭐️
Poor prognostic factors
Age <2yrs
– Repeated seizures: Seizures that are difficult to control.
– Deep and prolonged coma.
– Papilloedema/Raised intracranial pressure.
– Hypoglycaemia.
– Metabolic acidosis,