Week 8 Advanced CIED Follow-Up - Advanced Follow Up
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
Troubleshooting: Identifying Issues
Patient symptoms
Syncope/presyncope
Palpitations
Fatigue
Return of pre-implant symptoms
ECG abnormalities
Failure to capture
Failure to sense
Failure to output
Variations in pacing rate
Magnet rate indicates ERI/EOS
Remote monitoring
Arrhythmias
Device malfunctions
Heart failure
Advisory/recall
Patient-Related
Underlying disease state
Electrolyte imbalance
Medications
Tissue substrate changes
Address patient-related issues first!
System-Related
Generator
Header/connection
Lead integrity
Lead tissue interface (also a patient issue)
Pacemaker Troubleshooting Process
Gather information
Run PUBLSTOP
Review diagnostic data
Simplify device settings
Optional:
Evaluate chest x-ray
Invasive evaluation of the system
Determine the cause - review
Take corrective action
Gather Information
Pulse generator
Leads
Implant data
Patient symptoms
Complete device check
Gather Information: Pulse Generator
Manufacturer
Model #
Device capabilities
Advisory/recall
Chambers
Rate response
Special features
Date of implant
Gather Information: Leads
Manufacturer
Model #
Date of implant
Capped leads
Leads may have different manufacturers/dates
Recalls/advisories
Unipolar/bipolar
Fixation
Gather Information: Patient Information
Implant data
Medical records
CIED indication
May need to turn off alerts for known condition
Gather Information: Patient Symptoms
Current symptoms?
Duration?
Past symptoms?
Correlation to activities/time of day?
Make differential diagnosis
Differential Diagnosis: Palpitations
Pacemaker mediated tachycardia - VA conduction test
DDD tracking of AF/Flutter - evaluate mode switching
Tracking EMI - unipolar leads?
VT - analyze episodes/alerts
PVCs - track frequency
Differential Diagnosis: Weakness
Failure to capture
Inappropriate base rate
Need for rate response
Pacemaker syndrome
Differential Diagnosis: Dyspnea
Pacemaker syndrome
Need for rate response
Underlying cardiac disease (eg. heart failure)
Differential Diagnosis: Syncope
Pacemaker syndrome
Underlying disease (Vascular disease, VT, etc.)
Crosstalk - check refractory periods/sensitivity
Loss of capture - threshold test
Differential Diagnosis: Hiccups
Diaphragmatic pacing
Phrenic nerve stimulation
Differential Diagnosis: Muscle Twitching
Lead insulation failure
Unipolar pacing
Differential Diagnosis
Before running tests/making changes, note current programmed settings:
Mode
LRL
MTR/MSR
AV delays
Rate response
Lead polarity
Intervals
Algorithms
Loss of Capture
Pacing that fails to lead to myocardial depolarization when it otherwise should have captured
Excludes functional non capture: pseudo malfunction
True loss of capture: identify underlying cause and correct
Lead Dislodgement
Most likely in acute phase of lead implant (within 3 months)
Interview patient
Confirm lead type
Compare current data to implant data
Macro Dislodgment
can be seen on x-ray
Micro Dislodgment
cannot be seen on x-ray
More common with passive fixation
Lead Dislodgement Characteristics
Intermittent loss of capture
Different morphology when capturing
Sensing abnormalities
Far field oversensing
Undersensing
Normal impedance values
Cross-Chamber Stimulation
Lead from one chamber stimulates the opposite chamber
Atrial lead dislodgement across tricuspid valve
Ventricular depolarization in response to atrial pacing
Cross-Chamber Stimulation Testing
Pace AAl or AOO to confirm ventricular activation
Verify with VVI
Differential diagnoses
Lead dislodgement
Unipolar pacing
Atypical lead placement
Leads reversed in header
Perforation
Lead penetrates through cardiac tissue
Cathode no longer in contact with myocardium
Reported in 1-5% of patients
Chest x-ray or cardiac CT
Acute perforation: hemodynamically unstable due to tamponade
Late-occurring perforation: asymptomatic
Perforation Signs and Symptoms
More likely in patients with weaker heart walls (apical MI)
Failure to sense
Loss of capture
Hematoma
Pneumonia
Muscle twitching
Liver perforation
Hiccups
Loss of Lead Integrity
May cause change of impedance: systemic impedance determined by several factors
Conductor wires
Lead tip
Lead-header interface
Clavicular crush: common cause
Lead Safety Switch
Automatically changes to unipolar in response to high impedance
Coaxial leads: eliminates outer conductor
Only in brady leads
Loose Set Screw
Usually acute
Set screw can work loose over time
Manifests differently depending on degree of contact
Failure to output
Failure to sense
Intermittent loss of capture
Intermittent oversensing
Dislodgment Impedance
no change in impedance
Loose Set Screw Impedance
impedance rises
Check unipolar vs. bipolar impedances
Loose anodal set screw: high bipolar, normal unipolar
Loose cathodal set screw: high bipolar, high unipolar
Manipulate pocket: may cause
Electromyocardial Interface Patient Related
Myocardial infarction
Infiltrative cardiomyopathy (ARVD)
Post-shock pacing threshold rise (cardioversion, defibrillation)
Pacemaker Exit Block
system-related issue
Virtual electrode: fibrous capsule that forms around lead tip
Excessive fibrous can cause chronic high thresholds
Reduced by steroid-eluting leads
Attributed to unknown causes
Difficult to differentiate from dislodgement: exit block usually more chronic (> 3 months)
Other Causes of High Thresholds
Metabolic abnormalities
Electrolytes
Medications
Diabetes
Hemodialysis
Dehydration
Antiarrhythmics
Pseudomalfunctions
Fusion
Pseudofusion
Functional non-capture
Latency
Pacing location (LV, His, epicardial)
Near loss of capture
Isoelectric lead
Loss of Capture Troubleshooting Steps
Reestablish capture
Max outputs
Threshold test
Reprogram
Check bipolar impedance
High impedance: conductor fracture, loose set screw
Low impedance: insulation break
Check for normal unipolar impedance
Outer insulation break
Outer conductor fracture
Loose anodal set screw
Chest x-ray: look for macrodislodgement
Undersensing
Device fails to sense and time off of intrinsic signals: any condition that causes change to intrinsic complex
Metabolics/medications
Abnormal rhythms
Myocardial infarction
Lead dislodgement
Magnet application
Battery depletion
Component failure
Header abnormalities
Functional undersensing
Undersensing Effects
Overpacing: device fails to inhibit
Competitive pacing: shortly after intrinsic signal
Undersensing Secondary Effects
Functional non capture
PAV rather than SAV
Safety pacing off of intrinsic QRS
Mislabeling of intrinsic QRS as PVC
Medications and Metabolics causing Undersensing
Class IC antiarrhythmics (flecainide): most common medication issue
Hyperkalemia: most common metabolic issue
Functional Undersensing
Intrinsic event falls within blanking/refractory period
Not sensed or tracked: may influence mode switch
Pseudomalfunction
Undersensing Troubleshooting
Determine underlying cause
Run sensing test: measure intrinsic amplitude
Fix underlying cause if possible
If not, make device more sensitive by lowering mV value
Be careful to avoid oversensing
Check unipolar sensing if needed
Check impedance and capture
Oversensing
Device inappropriately senses and times off of signals other than intrinsic depolarizations
Inappropriate inhibition of pacing: underpacing
Inappropriate triggering of algorithms
Inappropriate triggering of ICD therapy
Noise
noncardiac signals sensed by CIED
Artifact
noncardiac signals seen on EGM by not sensed by CIED
EMI
Electromagnetic interference
Usually in 30-300 Hz range
Commonly cyclical appearance
60 Hz: standard frequency
Pacemakers: atrial channel more sensitive
ICDs: ventricular channel more sensitive
Myopotentials
Extracardiac muscular activity
Typically only in one channel
Can be initiated by physical maneuvers: be careful with pacemaker dependent/ICD patients
Conductor Fractures
usually on one channel
Sensing Conductor Fracture vs. Loose Set Screw
Loose set screw presents similarly:
More acute
Test with pocket manipulation
Check impedance to differentiate from dislodgement
Causes of T Wave Oversensing
Sensing of ventricular repolarization as depolarization
Long QT syndrome
Hyperkalemia
Brugada syndrome
Inappropriate programming
Troubleshooting T Wave Oversensing
Extend VREF
Adjust sensitivity value
Other sensing parameters
Switch to integrated bipolar
R Wave Double Counting
Sensing ventricular depolarization twice
Delays in ventricular conduction
Bundle branch block
Class IC antiarrhythmics
Hyperkalemia
Loss of capture
R Wave Double Counting Fix
Address underlying cause
Adjust blanking period if needed
Farfield Oversensing
Intrinsic signals in one chamber sensed in opposite chamber
R wave/T wave oversensing on atrial channel: most common cause of inappropriate mode switching
P wave oversensing on ventricular channel: His bundle lead
Farfield Oversensing Fix
Run sensing test
Decrease sensitivity by increasing mV value
Increase PVAB/PAVB if necessary
Crosstalk
VA crosstalk: sensing V pacing pulse on atrial channel
AV crosstalk: sensing A pacing pulse on ventricular channel
Run sensing test
Decrease sensitivity
Increase blanking period
Increase PVAB to prevent VA crosstalk
Increase PAVB to prevent AV crosstalk
Lower outputs if possible
ICD Leads
All leads vulnerable
Millions of cardiac cycles
Hostile environment
ICD leads: particularly vulnerable
More components
Higher voltages
Multilumen design
Single or dual coil
Dedicated or integrated bipolar
IS-1/DF-1 or DF4
ICD Lead Recalls
Medtronic Sprint Fidelis
Highly flexible
Conductor fractures of tip electrode coil and ring electrode cable
St. Jude Riata Family
Large-diameter lumens
Inside-out insulation breach
Externalized cables
Connections between conductors
Pace-Sense Failure
Seen with conductor fractures and insulation breaches
Oversensing of fast nonphysiologic signals
Inhibition of pacing
Inappropriate therapy
Loss of capture
Undersensing
Shock Component Failure
Likely underreported
Failed defibrillation
Complete pulse generator failure
Hopefully catch beforehand
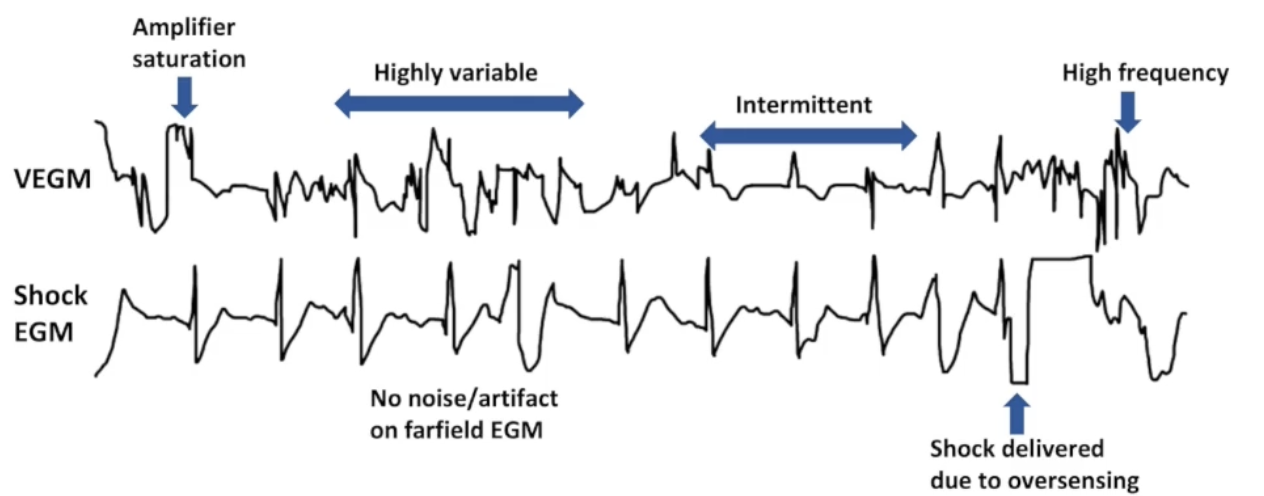
Analyzing EGMs
Signals on sensing channel but not farfield: usually noncardiac
Look at stored episodes
Use real time EGMs
Pocket manipulation to rule out poor lead-header connection
Exercises to rule out myopotentials
Insulation Breaches: Outside-in
myopotentials
EGMs less fully studied
Abnormal signals generated by secondary effects
Insulation Breaches: Inside-out
spikes on sensing and shock channels from cables rubbing against each other
Lead Impedance
Effective resistance of an electric component to alternating current, arising from combined effects of ohmic resistance and reactance
Higher impedance: lower current flow at same voltage
Ohm's law: V = IR
Pacing impedance: measured through subthreshold impulse
Lead-tissue interface (most of systemic impedance)
Conductors
Lead-header interface
Normal range: 300-1800 ohms
Changes to impedance more indicative of failure
Shock Impedance
Measured through low-energy shock
Shock circuit:
Lead-header connection
High-voltage conductors
Shocking coils
Anatomical features
Single coil leads: 30-110 ohms
Dual coil leads: 20-70 ohms
Low-voltage measurement not very accurate
High Voltage Conductor Fracture
Abrupt impedance increase
Absolute value > 100 ohms
High Voltage Insulation Breach
May cause impedance decrease
Difficult to diagnose with low voltage pulses
Can cause catastrophic short-circuit
Lead Failure Algorithms
Rapid oversensing
Impedance changes
Lead Failure Algorithms: Lead Safety Switch
change to unipolar
Cathodal conductor only
Works best with coaxial brady leads
Lead Failure Algorithms: Lead Integrity Alert
ICD leads
Impedance changes
Frequent isolated rapid intervals
Nonsustained VT with rapid intervals
Audible tone, RM alert, extends detection durations
Some algorithms withhold shocks for nearfield-only signals
Impedance Troubleshooting
Impedance not very sensitive or specific, especially low-voltage shock impedance
Monitor single out of range impedance or gradual rise over time
Reprogram to unipolar/integrated bipolar
Assess time frame
Chest x-ray if needed
Patients with at-risk leads
Education
Remote monitoring
Programming changes
Often replace during gen. change
Pacemaker Syndrome Definition
Initially associated with RV pacing
Later associated with several factors:
Loss of AV synchrony
Loss of V-V synchrony
Retrograde VA conduction
Lack of rate response
Loss of AV Synchrony
Atrial systole: 10-30% cardiac output
Ventricles contract too late: blood flows backward
Ventricles contract too early: atria contract against closed valve
Symptoms:
Dizziness
Syncope
Dyspnea
Fatigue
Palpitations
Distended neck veins
Hypotension
Heart failure
Pacemaker Syndrome Causes: VVI Devices
No AV synchrony
Retrograde VA conduction
Only indicated for permanent AF w/SVR or ICD patients with no pacing indications
Pacemaker Syndrome Causes: DDD Devices
Chronotropic incompetence with no rate response
RV pacing: V-V dyssynchrony
Algorithms to promote intrinsic conduction: AV dyssynchrony
Pacemaker Syndrome Symptoms
Dyspnea on exertion
Decreased CO
Chronotropic incompetence
Worsening heart failure
Heart failure:
Nocturnal dyspnea
Orthopnea
Edema
Weight gain
Lung sounds
Vascular symptoms
Hypotension
Syncope/presyncope
Related to decreased CO
Fatigue
Headache
Dizziness
Physical Examination
Palpitations
Drop in systolic BP of > 20 mmHg when turning pacing on
Cannon A waves
Atria contract against closed AV valves
Blood regurgitates backward
Pulsation in neck/abdomen
Waveform on central venous pressure tracing
Seen with RVAC, CHB, pulmonary HTN, VT
Pacemaker Syndrome at Follow Up
Run tests in a way that feels best for patients
DDD maintains AV synchrony
Be careful when coming on pacing
Monitor patient for symptoms
Programming Considerations: VVI
reduce pacing
Decrease rate
Rate hysteresis
Rate response off
Programming Considerations: Permanent AF
compensate for loss of atrial kick
Increase base rate
Turn rate response on
Programming Considerations: DDD
balancing act
Algorithms that promote intrinsic conduction reduce RV pacing, can cause AV dyssynchrony
CHB and CRT patients should have shorter AV delays
Rate response drives pacing in the atrium: physiologic
CRT: algorithms to promote BIV pacing
P Wave Abnormalities: Right Atrial Abnormality
change to beginning of P wave
Tall, peaked P wave
COPD
Pulmonary HTN
Congenital heart disease
RVHF
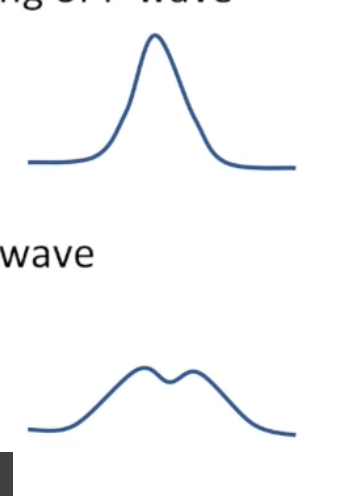
P Wave Abnormalities: Left Atrial Abnormality
change to end of P wave
Wide, notched P wave
CAD
Cardiomyopathy
HTN
Valvular heart disease
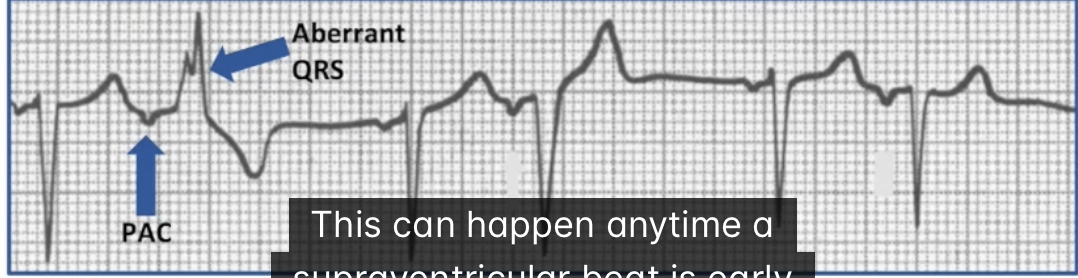
Aberrancy
Abnormal intraventricular conduction of a supraventricular impulse
One or more components of distal conduction system refractory when impulse arrives
Different conduction pathway
Any supraventricular impulse that is early enough
PACs: Three Possible Outcomes
A: Nonconducted PAC
B: Aberrant RBBB Pattern
C: Normal QRS Complex
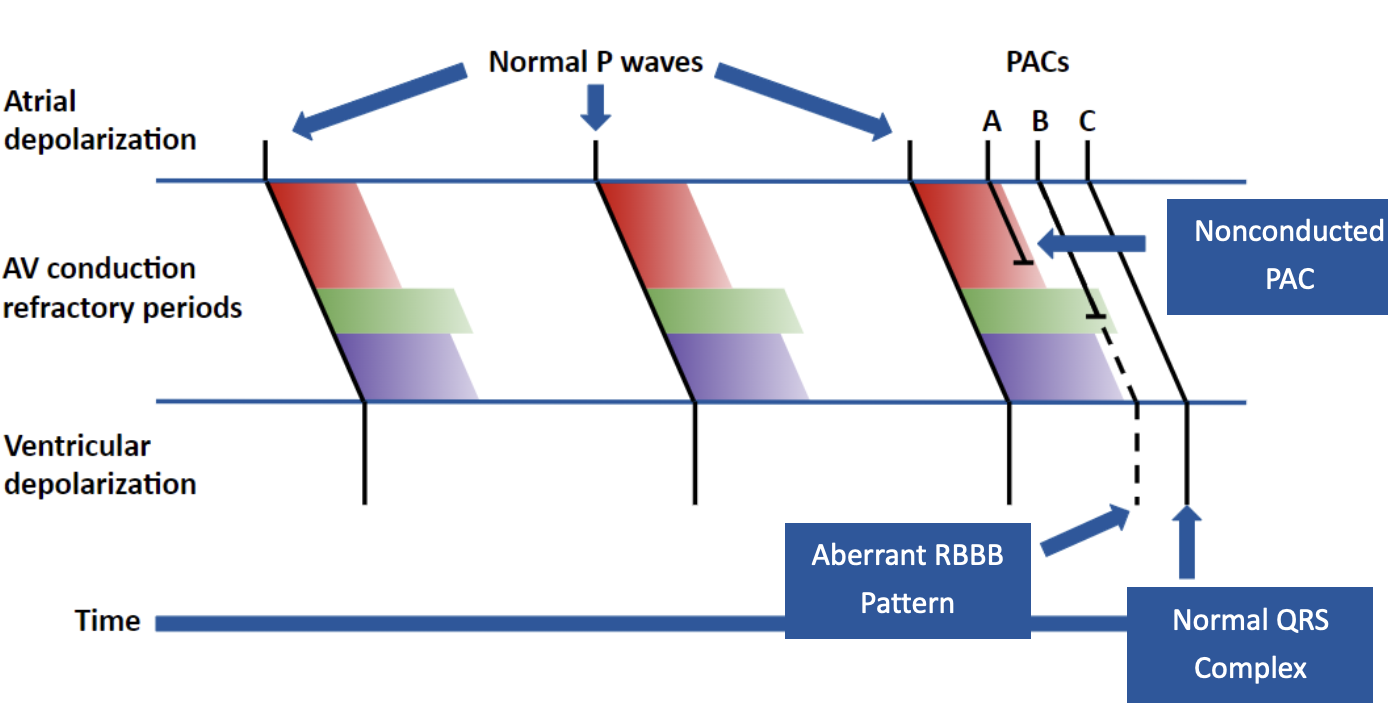
Importance of Underlying Rate
Refractory periods determined by heart rate
Slower rate: longer
Faster rate: shorter
Longer PAC intervals will cause aberrancy at slower rates
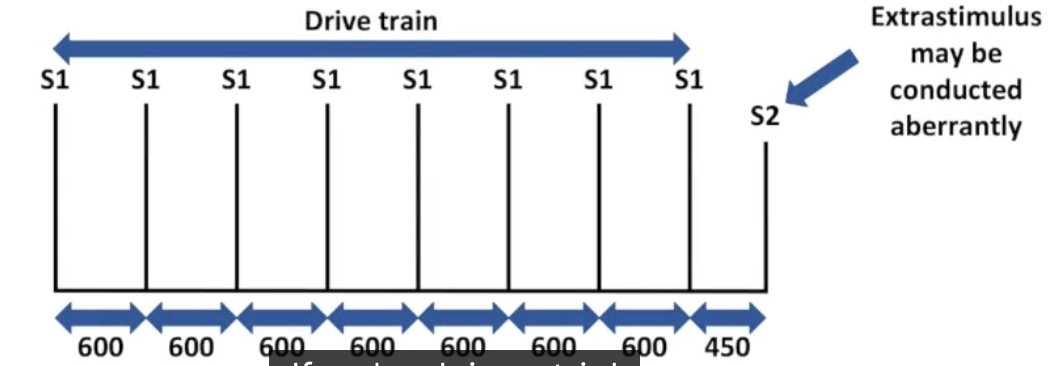
Atrial Extrastimulus Pacing
Mimics PAC: can cause aberrancy
Drug Toxicity and Electrolytes
Anything that alters the action potential can cause aberrancy:
Electrolyte abnormalities
Hypocalcemia
Hypercalcemia
Hyperkalemia
Medications
Class IC antiarrhythmics (flecainide)
Rate Related Aberrancy
can result from rapid acceleration and deceleration as well as high overall rates
Rate related bundle branch block:
Every beat falls within bundle branch refractory period
Usually RBBB pattern
Occurs at critical rate: similar to Wenckebach
Rate is lower in diseased hearts
Aberrancy in ICDS: Transvenous
morphology discriminator
Patient exercising: sinus rate reaches VT zone
Morphology discriminator will label aberrancy as VT
Turn morphology off or turn on other discriminators
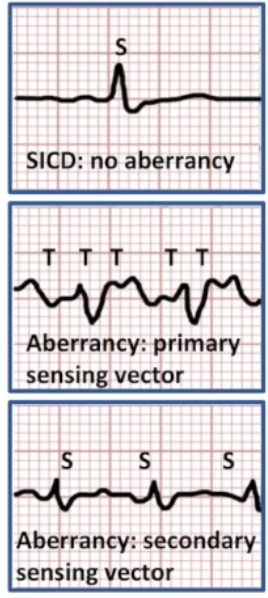
Aberrancy in ICDS: SICD
subcutaneous ECG
Aberrancy can cause R wave double-counting
Changes to T wave can cause T wave oversensing
Rate appears double
Change sensing vector
Ashman Phenomenon
Aberrant ventricular conduction due to changes in QRS cycle length
Associated with AF: irregularly irregular conduction
Long-short rule: the earlier in the cycle the PAC occurs and the longer the preceding cycle, the more likely the PAC will be conducted aberrantly

Rhythm Differentiation
VT, SVT with aberrancy, or antidromic AVRT?
12 lead: AV relationship, axis, R wave progression, durations
EGMs: more difficult
Don't assume one or the other
Physician may want additional testing

Rhythm Control
Prevent arrhythmias
Terminate arrhythmias
Restore normal sinus rhythm
Rate Control
Slow conduction through the AV node
Reduce ventricular rate during supraventricular arrhythmias
Mechanisms of Tachycardia
Antiarrhythmics target different mechanisms: most commonly reentrant circuit by altering conductivity/refractoriness
Reentry: electrical impulse caught in self-propagating loop
Abnormal automaticity: non-pacemaker cells display automaticity
Triggered activity: afterdepolarizations trigger new action potential

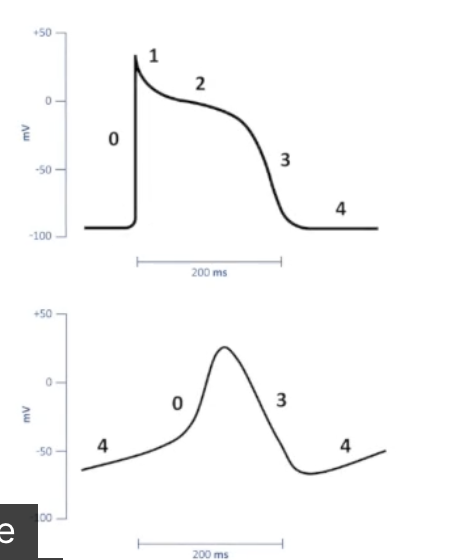
Antiarrhythmic Actions
Phase 0: increase/decrease conduction velocity
Phase 3: change duration of ERP
Phase 4: suppress abnormal automaticity and triggered activity
Autonomic tone: chronotropy, inotropy, dromotropy
Vaughan-Williams Classification
Class I: sodium channel blockers
Class II: beta blockers
Class III: potassium channel blockers
Class IV: calcium channel blockers
Class V: parasympathetic stimulation
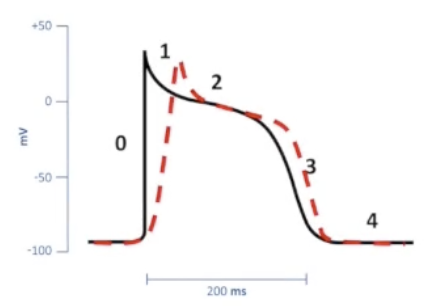
Class I: Sodium Channel Blockers - Class IA
Class IA: moderate influence on phase 0
Slow conduction velocity
Prolong repolarization
Extend AP duration
Procainamide, quinidine, disopyramide
Risk of Torsades de Pointes, GI upset, enhanced AV conduction, hypotension
Class I: Sodium Channel Blockers - Class IB
Class IB: weak influence on phase 0
Little impact on conduction velocity
Shorten repolarization
Decrease AP duration
Lidocaine, mexiletine, phenytoin, tocainide
Class I: Sodium Channel Blockers - Class IC
Class IC: strong influence on phase 0
Repolarization unchanged
No effect on AP duration
Slow conduction to break or prevent arrhythmias
Flecainide, propafenone, encainide, moricizine