Series 1 Form B Part 5
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Which of the following instruments is MOST appropriate for measuring patients' quality of life?
1.Lysholm knee rating scale
2.Oswestry low back pain disability index
3.Goal Attainment Scale (GAS)
4.Medical Outcomes Study 36-item short form (SF-36)
2,4
1. The Lysholm knee rating scale is a condition-specific instrument, not a quality-of-life assessment tool
2. The Oswestry low back pain disability index is a condition-specific instrument, not a quality-of-life assessment tool
3. The Goal Attainment Scale (GAS) measures achievement of self-identified goals but does not indicate the impact of goal attainment on quality of life
4. The Medical Outcomes Study (MOS) resulted in development of the 36-item short form for measuring patient's quality of life. It is a self-report that covers eight domains of physical functioning, role limitation due to physical problems, role limitations due to emotional problems, fatigue, and general health perceptions.
While walking with a prosthesis, a patient with a right transtibial amputation fails to flex the right knee in early stance. This gait pattern is MOST likely due to excessive:
1.dorsiflexion of the prosthetic foot.
2.posterior displacement of the socket relative to the foot.
3.medial displacement of the socket relative to the foot.
4.lateral rotation of the prosthetic foot.
2,2
1. Excessive plantar flexion, not dorsiflexion, is a cause of insufficient knee flexion.
2. Insufficient knee flexion can be due to a socket that is too posterior to the foot.
3. Socket placement too far posteriorly, not medially, is cause for insufficient knee flexion in the early stance phase.
4. Socket placement too far posteriorly, not laterally, is cause for insufficient knee flexion in the early stance phase.
Which of the following patient factors would MOST increase the risk for an adverse drug reaction?
1.Male gender
2.Age 55 years
3.Use of herbal compounds
4.Presence of irritable bowel syndrome
3,3
1. Female gender is considered to be a risk factor for experiencing a serious adverse drug reaction.
2. Being over age 75 years is considered to be a risk factor for experiencing a serious adverse drug reaction.
3. Concomitant use of herbal compounds is considered to be a risk factor for experiencing a serious adverse drug reaction.
4. Hepatic or renal insufficiency, not irritable bowel syndrome, is considered to be a risk factor for experiencing a serious adverse drug reaction.
A physical therapist is at a community pool leading a class for patients who have arthritis. The therapist observes an adult patient suddenly fall to the ground. Which of the following sequences of actions is MOST appropriate?
1.Assess the airway, breathing, and circulation of the patient.
2.Begin cardiopulmonary resuscitation and activate the emergency response system.
3.Give two quick breaths, activate the emergency response system, and get an automated external defibrillator.
4.Check responsiveness, activate the emergency response system, check pulse, and begin chest compressions.
4,4
1. The physical therapist should check for responsiveness and then activate the emergency medical system. Assessing breathing and pulse would happen after those steps.
2. Resuscitation is initiated after assessing responsiveness and then activating the emergency medical system
3. The physical therapist should check for responsiveness and then activate emergency medical system. Rescue breathing would occur after determining the patient has a pulse but is not breathing normally.
4. The physical therapist should check for responsiveness and then activate emergency medical system. Assessing breathing and pulse would happen simultaneously after those steps. Beginning with chest compressions is recommended if the patient is not breathing or only gasping and has no pulse.
A patient is referred to physical therapy with a diagnosis of myositis ossificans in the quadriceps muscle after sustaining a contusion. The MOST appropriate treatment for the patient is:
1.progressive resistance exercises through full range.
2.active range of motion in the pain-free range.
3.passive range of motion into resistance.
4.transverse friction massage.
3,2
1. Initially strengthening should be avoided; the focus should be on range of motion
2. Once rehabilitation can begin, initial treatment is geared toward range of motion
3. Passive range of motion into resistance should not be done initially in the treatment of myositis ossificans
4. Initial treatment is geared toward range of motion. Transverse friction massage is contraindicated in the presence of acute inflammation, hematomas, debilitated or open skin, and decreased sensation. Massage should be avoided early in the treatment of myositis ossificans.
Which of the following factors has the GREATEST effect on closure and healing of an open wound?
1.Amount of wound drainage
2.Type of wound dressing
3.Overall size of the wound bed
4.Arterial perfusion to the wound area
4,4
1. The amount of wound drainage does not have as strong an effect on wound closure and healing as does the level of arterial perfusion to the wound area.
2. The type of wound dressing does not have as strong an effect on wound closure and healing as does the level of arterial perfusion to the wound area.
3. Although wound size can affect the time required to close a wound, it does not have as much effect as vascular patency in the body's ability to close a wound. Many factors affect the rate of wound healing (i.e., nutrition, wound environment, etc.), but the overall prognosis for ability to heal is worst when vascular flow is absent or severely diminished.
4. Adequate delivery of blood and therefore nutrition and oxygen to the wound tissue is vital for healing and will determine the wound healing prognosis.
A patient who reports neck pain radiating to the elbow is treated with cervical traction. During the treatment, the patient reports increased neck pain with radiating pain into the ring finger (4th digit) and little finger (5th digit) of the right hand. Which of the following actions is MOST appropriate for the physical therapist to take?
1.Stop the intervention and reevaluate.
2.Refer the patient back to the physician.
3.Change the angle of pull of the traction.
4.Reduce the traction force.
1,1
1. Traction is contraindicated if peripheralization of signs and symptoms occurs during and following therapy.
2. The change described in the stem is consistent with the current presentation and does not warrant referral to physician.
3. Because progression of symptoms from central to a peripheral area indicates worsening nerve function and increased compression, changing the angle is insufficient.
4. Because progression of symptoms from central to a peripheral area indicates worsening nerve function and increased compression, reducing the poundage is insufficient.
A patient is initiating a pelvic floor strengthening program. Which of the following positions would be considered gravity assisted?
1.Trendelenburg
2.Sitting
3.Quadruped
4.Standing
4,1
1. The Trendelenburg position, with the hips positioned higher than the heart, is considered a gravity-assisted position for this exercise, given the location of the pelvic floor muscles and the action of these muscles when tightened, which pull upward toward the abdomen.
2. The sitting position is a progression to improve strength and proprioception of the pelvic floor muscles. Gravity will be working against the pelvic floor.
3. The quadruped position is a progression to improve strength and proprioception of the pelvic floor muscles.
4. The standing position is a progression to improve strength and proprioception of the pelvic floor muscles. Also, this would be considered the gravity position.
Which of the following factors is MOST linked to the development of osteoporosis and a greater risk of fracture?
1.Abnormally high body mass index
2.Abnormally low body mass index
3.Low cholesterol levels
4.Vegetarian diet or low intake of animal protein
1,2
1. A high body mass index is not associated with osteoporosis.
2. Body build is related to bone fragility, with thin patients having less cortical bone and a higher risk for fracture.
3. High cholesterol levels and atherosclerosis are associated with loss of calcification of bone.
4. Meat protein and fat provide acid precursors, with higher animal protein proportions leading to more rapid femoral neck bone loss.
The patient who has the wound shown in the photograph has received conservative care for 2 months without improvement. To promote wound healing, which of the following treatments is MOST appropriate to add at this time?
1.Antibiotic treatment
2.Total contact casting
3.Daily dressing changes
4.Sharp debridement of the callus
2,2
1. Antibiotic treatment is generally not indicated for uninfected wounds. While the foot wound in the photograph is not progressing, there are not signs of infection present. Off-loading pressure areas is important to facilitate wound healing.
2. Total contact casting is the accepted standard for off-loading pressure areas on the plantar surface of the foot.
3. Daily dressing changes may make the total contact casting impractical. Daily dressing changes may prevent a patient from taking advantage of the increased healing rates associated with total contact casting.
4. While periodic callus removal is important, the foot in the photograph does not demonstrate significant callus formation. Long-term pressure relief from total contact casting may help prevent callus formation.
Which of the following conditions would MOST likely be experienced by a 7-year-old patient who has a tethered spinal cord?
1.Upper extremity hypertonicity
2.Bladder dysfunction
3.Blurred vision
4.Headache
2,2
1. Upper extremity hypertonicity is consistent with shunt dysfunction, not tethered cord
2. A tethered spinal cord occurs when adhesions anchor the spinal cord at the site of the lesion as individuals with spina bifida grow. The tethering of the spinal cord can result in rapidly progressive scoliosis, hypertonicity in the lower extremities, changes in gait, and changes in urologic function.
3. Blurred vision is consistent with shunt dysfunction, not tethered cord
4. Headache is consistent with shunt dysfunction, not tethered cord
A physical therapist is initiating intervention with a postoperative patient who has just taken a 20-mg dose of oral oxycodone (OxyContin) for pain relief. In planning an intervention for this patient, the physical therapist should anticipate that:
1.the patient may be hypertensive.
2.the medication may trigger cardiac arrhythmias in the patient.
3.the patient will have an increased likelihood for developing diarrhea.
4.the patient may demonstrate respiratory depression.
2,4
1. Orthostatic hypotension is a potential side effect of oxycodone, so the patient is unlikely to be hypertensive.
2. Arrhythmias are not listed as a recognized side effect of opioids.
3. Regarding developing diarrhea, gastrointestinal motility is decreased, so the opposite effect of constipation is a frequent problem. Constipation is a listed side effect.
4. Opioids tend to make the medullary chemoreceptors less responsive to carbon dioxide, thus slowing down the respiratory rate and inducing a relative hypoxia and hypercapnia. The respiratory response to exercise may be blunted.
On the basis of the history and objective assessment of a patient with knee pain, a physical therapist suspects a ligamentous lesion. Which of the following diagnostic tests should the therapist request to confirm these findings?
1.Myelography
2.Radiography
3.Magnetic resonance imaging (MRI)
4.Computed tomography (CT) scan
3,3
1. Myelograms are used to help diagnose pathological conditions of the spine
2. Radiography is best for detecting fractures, arthritis, or degeneration. Non-weight-bearing, stress x-rays may be used to identify ligamentous instability, but radiographs do not provide the most accurate image of soft tissue structures, such as muscles, tendons, ligaments, and intervertebral discs.
3. Magnetic resonance imaging (MRI) has the ability to show soft tissue as well as bone tissue without the need to expose the patient to the ionizing radiation needed for computed tomography scans
4. Computed tomography (CT) scans are used to view soft tissue as well as bone, although a contrasting agent must be used. Magnetic resonance imaging has largely replaced CT scans for knee evaluations.
A patient reports worsening medial foot and ankle pain. Examination reveals a loss of arch height, excessive pronation during walking, and pain with palpation of the posterior aspect of the medial malleolus. Which of the following combinations of movements is MOST likely to be weak?
1.Dorsiflexion and eversion
2.Dorsiflexion and inversion
3.Plantar flexion and eversion
4.Plantar flexion and inversion
1,4
1. Dorsiflexion and eversion are performed by fibularis (peroneus) tertius, which is not implicated by the impairments identified in the stem.
2. Dorsiflexion and inversion are performed by the tibialis anterior, which is not implicated by the impairments identified in the stem
3. Plantar flexion and eversion are performed by the fibularis (peroneus) longus, which is not implicated by the impairments identified in the stem
4. Plantar flexion and inversion are performed by the tibialis posterior. The tibialis posterior tendon is implicated by the impairments identified in the stem.
Which of the following describes the use of a physical restraint for an older adult living in a long term care facility that can be used by a physical therapist without a physician's order?
1.A wheelchair tray used for proper positioning of the upper trunk that can be removed by the patient
2.A vest restraint while in bed for a patient who may wander away from the residence
3.For a patient who self propels with the lower extremities, elevating the wheelchair seat so the patient's feet do not reach the ground
4.Removing a patient's ambulatory device to control disruptive behavior
1,1
1. A wheelchair tray is a physical support that the patient is able to remove when it is not in use. It does not require a physician order because it is being used for positioning.
2. Use of a vest restraint is not consistent with patients' rights under Omnibus Reconciliation Act (OBRA) because it restricts a patient's mobility and requires a physician order.
3. Elevating the wheelchair seat is not consistent with patients' rights under Omnibus Reconciliation Act (OBRA) because it restricts a patient's mobility and requires a physician order.
4. Removing an ambulatory device is not consistent with patients' rights under Omnibus Reconciliation Act (OBRA) because it restricts a patient's mobility.
Which of the following strategies would be MOST appropriate when measuring the size and shape of a partial-thickness wound?
1.Hold a tape measure above the wound surface and measure the diameter.
2.Insert a cotton-tipped applicator into the wound at its deepest point and measure the distance from the wound bed to the level of the skin surface.
3.Place a sheet of plastic wrap on the wound and use a marking pen to draw a tracing of the wound's perimeter on the plastic.
4.Place normal saline in the wound, using a measured syringe to fill the wound to the level of the skin surface.
3,3
1. This technique can be used to measure size, but it is not useful for measuring the shape of the wound
2. This technique can be used to measure depth but not to measure size and shape. It is not accurate and is difficult to reproduce measurements. A partial-thickness wound has no measurable depth.
3. This is the only option in the list that measures size and shape
4. This technique is called fluid instillation and is used to measure wound volume rather than size and shape
Which of the following BEST describes the huffing technique of airway clearance?
1.Cough while holding a pillow against the chest.
2.Forcefully exhale while keeping the mouth open.
3.Forcefully exhale through pursed lips.
4.Take two normal breaths, then cough firmly on the third exhalation.
2,2
1. Coughing while holding a pillow against the chest refers to splinting the incision and is most commonly used by surgical patients to reduce pain while coughing
2. Huffing consists of taking a deep inspiration followed by forceful exhalation without closing the glottis. Keeping the mouth open facilitates this.
3. Exhaling through pursed lips is a technique for dyspnea, not airway clearance
4. Huffing involves taking one deep inspiration, not two normal breaths
Which of the following findings BEST describes a positive result of the Median Nerve Tension Test?
1.Elicitation of numbness in the cubital fossa
2.Elicitation of numbness in the hypothenar eminence
3.Reproduction of symptoms in the dorsal and ulnar side of the hand
4.Reproduction of symptoms in the volar (palmar) and radial side of the hand
1,4
1. Numbness in the cubital fossa is incorrect. Although the median nerve courses through the cubital fossa, its sensory branches supply only the palmar and radial side of the hand.
2. The median nerve does not innervate the hypothenar region, which is innervated by the ulnar nerve.
3. The location of symptoms and the wrist position are descriptive of radial nerve tension, not median nerve tension.
4. This option correctly states the location of symptoms (palmar and radial side of hand) when there is tension on the median nerve.
Which of the following conditions would BEST explain the characteristics of the patient's knees shown in the photograph?
1.Long patellar tendon
2.Short patellar tendon
3.Femoral retroversion, lateral (external) tibial rotation
4.Femoral anteversion, medial (internal) tibial rotation
4,4
1. A long patellar tendon could result in a height change of the patella, but the patella would not appear to be facing inward ("squinting patella") as shown in the photograph. An inward patella ("squinting patella") could indicate femoral anteversion.
2. A long patellar tendon could result in a height change of the patella, but the patella would not appear to be facing inward ("squinting patella") as shown in the photograph. An inward patella ("squinting patella") could indicate femoral anteversion.
3. The position of the patella appears inward ("squinting patella"), which could indicate femoral anteversion. In the photograph, the right patella appears to be facing inward, which suggests femoral anteversion, not retroversion.
4. The position of the patella appears inward ("squinting patella"), which could indicate femoral anteversion. In the photograph, the right patella appears to be facing inward, which suggests femoral anteversion and medial (internal) tibial rotation

Which of the following clinical findings is MOST likely to be associated with a C7 nerve root lesion?
1.Pain in the medial aspect of the upper arm
2.Diminished light touch on the volar forearm
3.Inability to extend the elbow against gravity
4.Inability to supinate the forearm
3,3
1. The medial side of the arm is innervated by C8 and T1
2. The volar surface of the entire arm is innervated by C5- C6 and T1
3. A C7 nerve root lesion will affect the triceps, which is an elbow extensor
4. The biceps and supinator (both responsible for supination of the forearm) are innervated by C5-C6
The medical record indicates that a patient is taking a beta-blocker for a cardiac condition. The physical therapist should expect that this medication will:
1.decrease angina pectoris and increase blood pressure.
2.increase heart rate and lower blood pressure.
3.decrease heart rate and lower blood pressure.
4.decrease heart rate and increase oxygen demand.
3,3
1. This option is incorrect because beta-blockers decrease angina and also decrease blood pressure
2. This option is incorrect because beta-blockers decrease heart rate
3. This option is correct because beta-blockers decrease heart rate and blood pressure
4. This option is incorrect because beta-blockers decrease oxygen demand
A patient who underwent a hernia repair should AVOID which of the following activities?
1.Walking at a metabolic equivalent of 3 or more during the 1st week after surgery
2.Performance of tasks using a Valsalva maneuver for 4-6 weeks after surgery
3.Stretching of the posterior spinal and hip musculature before the incision is fully healed
4.Active adduction or flexion of the lower extremities before the incision is fully healed
3,2
1. Walking is encouraged within the first week following repair. Walking at a metabolic equivalent of 3 is equivalent to a walking speed of 2.6 mph, a relatively slow speed. A 1-week delay in walking would place the patient at risk for additional comorbidities.
2. Patients are advised to avoid straining for 4-6 weeks following repair, regardless of the procedure
3. Hernias are repaired through an anterior incision, and thus stretching of the abdominal wall or groin region should be avoided, but stretching the posterior structures should not be an issue.
4. Surgical repairs are anterior. Thus flexion or adduction does not affect the incision and would not be necessary to avoid. Moreover, some programs allow isometric adduction in the first week.
A physical therapist should withhold resistive exercise for a patient who has which of the following laboratory test results?
1.Platelet count of 18,000/mm3
2.White blood cell count of 8000/mm3
3.Hemoglobin of 12 g/dL
4.International normalized ratio (INR) of 1
1,1
1. This is a very low platelet count. With a low platelet count, the patient's blood is not clotting properly and severe bleeding can occur. A patient will usually need a transfusion at this level, and exercise should be limited to just activities of daily living. A normal platelet count is 150,000-400,000/mm3.
2. A normal white blood cell count is an indicator of immune system function. Normal count is 4500-11,000/mm3, so this is at an acceptable level for resistance exercise.
3. The normal range for hemoglobin is 12-18 g/dL, and resistance training is typically acceptable even at a level of 10 g/dL
4. The international normalized ratio (INR) indicates blood's ability to clot. The normal range for people who are not taking anticoagulant medications is 0.9-1.1. When patients are at a higher risk of blood clots or have mechanical heart valves, they take anticoagulants to thin their blood, thus increasing their INR to a necessary range of 2-3.5. When the INR is over 3-3.5, the patient is at a higher risk of bleeding and it may be necessary to limit exercise.
On the basis of the test result shown in photograph, tightness is MOST likely present in which of the following structures in the left lower extremity?
1.Iliopsoas
2.Hamstrings
3.Iliotibial band
4.Gluteus maximus
1,1
1. When the iliopsoas length is normal, the lumbar spine should flatten and the test leg should remain flat on the table
2. The hamstring muscles are tested with the patient in supine position using a combination of hip flexion and knee extension
3. The iliotibial band is most appropriately tested in sidelying with the test leg on top and with the examiner moving the hip into adduction
4. The gluteus maximus only crosses the hip joint, and the length would not be tested with the hip in extension

The photograph depicts a patient's arm that was recently removed from an immobilizer after an upper extremity laceration. Based on the position of the wrist, which of the following nerves was damaged and where did the damage occur?
1.Median nerve in the carpal tunnel
2.Radial nerve in the anatomic snuffbox
3.Radial nerve in the radial groove of the humerus
4.Ulnar nerve posterior to the medial epicondyle of the humerus
2,3
1. The image indicates wrist drop, which results from injury to the radial nerve. The most common radial nerve injury is damage to the radial nerve in the radial groove of the humerus. The median nerve enters the hand by passing through the carpal tunnel.
2. The image indicates wrist drop, which results from injury to the radial nerve. The most common radial nerve injury is damage to the radial nerve in the radial groove of the humerus. The distal branches of the superficial branch of the radial nerve run over the tendon of the extensor pollicis longus in the anatomic snuffbox, but damage to these branches is of little consequence because they supply only a small area of the skin.
3. The image indicates wrist drop, which results from injury to the radial nerve. The most common radial nerve injury is damage to the radial nerve in the radial groove of the humerus, which produces a global paralysis of the muscles of the posterior compartment and results in wrist drop.
4. The image indicates wrist drop, which results from injury to the radial nerve. The most common radial nerve injury is damage to the radial nerve in the radial groove of the humerus. This answer is incorrect because the ulnar nerve lies posterior to the medial epicondyle at the elbow.
A patient had an open cholecystectomy 2 days ago and is currently having difficulty moving from supine to sitting position due to pain. Before the patient's next attempt to move, which of the following interventions would be MOST appropriate?
1.Bracing an abdominal pillow to splint
2.Using an incentive spirometer
3.Instruction in huffing
4.Tilt table regimen
1,1
1. Splinting is an appropriate method for pain control with mobility.
2. An incentive spirometer is used for pulmonary interventions and would not help with pain.
3. Huffing is a method for pulmonary clearance when coughing is too painful. It would not help with the pain while moving.
4. Typically a tilt table regimen is used for patients who are restricted to prolonged bed rest and who have persistent orthostatic hypotension. It would not help with pain.
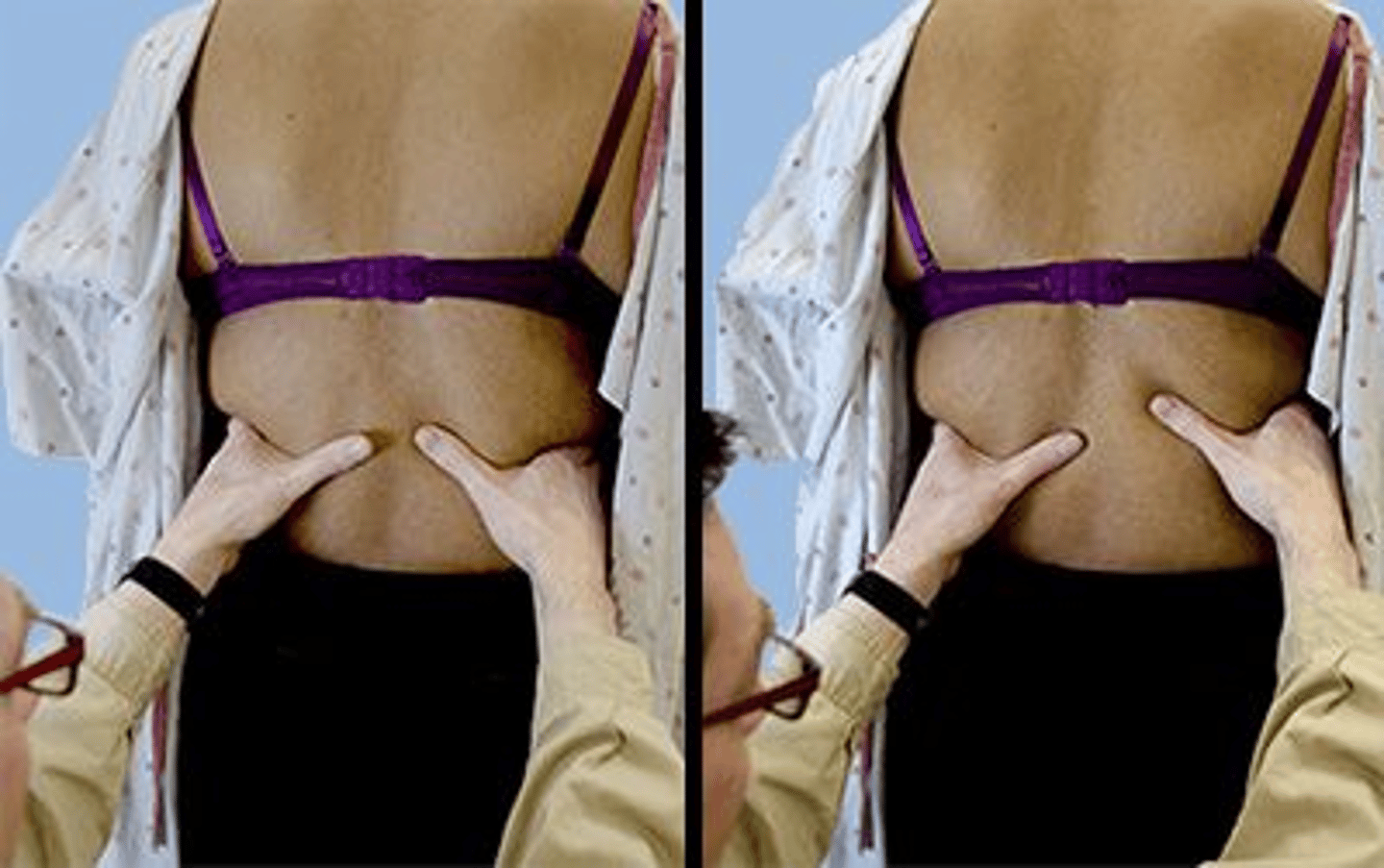
Based on the findings of the assessment during inspiration shown in the photographs, the patient MOST likely has restriction involving which of the following lung segments?
1.Left lingula
2.Left lower lobe
3.Right lower lobe
4.Right upper lobe
2,2
1. The image shows the technique for palpating the lower lobes. To assess the right middle lobe and lingular segment, the therapist places his/her widely outstretched fingers of both hands over the posterior axillary folds and his/her palms over the anterior chest wall.
2. The image clearly shows the technique for palpating the lower lobes. The therapist's thumbs and hands do not move the same distance from each other, indicating restriction on the left side. With unilateral restriction, there is evidence of diminished movement on only one side.
3. The image clearly shows the technique for palpating the lower lobes. The therapist's thumbs and hands do not move the same distance from each other, indicating restriction on the left side and not the right side. With unilateral restriction, there is evidence of diminished movement on only one side.
4. The image clearly shows the technique for palpating the lower lobes. To assess the upper lobes, the therapist places his/her palms anteriorly over the first four ribs with the fingertips extended over the trapezius muscle.
A patient who reports back pain has increased lumbar lordosis. The MOST appropriate exercises for this patient are:
1.abdominal strengthening and iliopsoas stretching.
2.hip flexor strengthening and hamstring stretching.
3.hip flexor strengthening and erector spinae stretching.
4.erector spinae strengthening and iliopsoas stretching.
1,1
1. A lordotic posture contributes to weak or inhibited abdominals and gluteus maximus. It also contributes to tight iliopsoas and erector spinae. Therefore, the abdominals should be strengthened, and the iliopsoas should be stretched.
2. The hip flexors should be stretched, not strengthened.
3. The hip flexors should be stretched, not strengthened.
4. The erector spinae should be stretched, not strengthened.
A physical therapist is treating a patient with urge incontinence. Which of the following outcomes of the intervention program are MOST desirable?
1.Decrease in bladder capacity and decrease in urinary frequency
2.Increase in bladder capacity and decrease in urinary frequency
3.Decrease in bladder capacity and increase in urinary frequency
4.Increase in bladder capacity and increase in urinary frequency
2,2
1. Decreases in both of these features are characteristic of urge incontinence and a decrease in bladder capacity is undesirable.
2. With an urge incontinence, the desire is to improve the ability to inhibit automatic detrusor contractions. The body is trained to respond to a specific voiding schedule. An increase in bladder capacity and a decrease in the frequency of urination are features of improved bladder control.
3. A decrease in bladder capacity and an increase in urinary frequency are the opposite of what is desired with training for urge incontinence.
4. Although an increase in bladder capacity is desirable, the goal is to decrease the frequency of urination, not increase it.
A physical therapist is examining a patient following open reduction internal fixation of the distal tibia and fibula. The physical therapy examination reveals active range of motion of the involved ankle from 10° of dorsiflexion to 0° of plantar flexion. What phase of gait is MOST likely affected?
1.Heel strike (initial contact)
2.Midstance
3.Toe off (preswing)
4.Acceleration (initial swing)
3,3
1. At heel strike (initial contact), the ankle is in a neutral position, so only having 10° of movement at the ankle would not affect this phase of gait.
2. The ankle will move from plantar flexion to dorsiflexion during midstance, but the greatest plantar flexion occurs at toe off (preswing).
3. The greatest amount of plantar flexion is needed in the ankle during the toe off (preswing) phase of gait. The patient has 0° of plantar flexion, so this phase of gait would be most affected.
4. The ankle remains in a neutral position during acceleration (initial swing). Since the patient has 10° of dorsiflexion, this phase of gait would not be affected.
A patient who had an uncomplicated vaginal delivery 3 months ago has a 3-cm diastasis recti and Fair minus (3-/5) strength of the abdominal muscles. Which of the following therapeutic exercises, performed with arms bracing the abdomen, is MOST appropriate for the patient INITIALLY?
1.Head lift
2.Partial sit-ups
3.Lower trunk rotation
4.Bilateral straight leg raises
1,1
1. With a 3-cm diastasis, the head lift is the most appropriate exercise initially. The patient braces the abdomen toward the midline to approximate the diastasis while performing the head lift. This will help to keep the separation of the abdominal muscles to a minimum, minimize the action of the obliques, and control intraabdominal pressure.
2. Given the strength of this patient's abdominal muscles in addition to the extent of the diastasis, this activity would be too strenuous and may further compromise the diastasis. The head lift should be performed exclusive of all other abdominal exercises until the diastasis is 2 cm or less.
3. Lower trunk rotation should be avoided until the diastasis is 2 cm or less. Due to the angle of attachment of the obliques into the linea alba, there is a possibility that trunk rotation exercises will perpetuate the diastasis.
4. With an abdominal strength of Fair minus (3-/5) and a diastasis of 3 cm, bilateral straight leg raises could cause a further separation of the diastasis by increasing intraabdominal pressure as the patient tries to stabilize while lifting the legs. The head lift corrective exercise should be performed exclusive of all other abdominal exercises until the diastasis is reduced to 2 cm or less.
A patient who had a recent carpal tunnel decompression surgery is referred to physical therapy. The patient also had a first rib resection and a pronator teres release on the same extremity within the past 2 years. The patient now reports burning pain in the wrist and dorsal forearm and that the wrist and hand often feel cold. These signs and symptoms MOST likely indicate:
1.T4 syndrome.
2.ulnar neuropathy.
3.cervical radiculopathy.
4.complex regional pain syndrome.
4,4
1. The distribution of the symptoms is not consistent with the level innervated by T4 (p. 1664).
2. The distribution of the ulnar nerve is not consistent with the description of symptoms (pp. 1664, 1669).
3. A radiculopathy is involvement of a nerve root as it emerges from the spinal cord (p. 1667). The distribution of symptoms is not consistent with a cervical nerve root distribution, and no weakness is reported.
4. The primary clinical features of complex regional pain syndrome are burning or aching pain, autonomic nervous system dysfunction, edema, and movement disorders. In the final stage, the affected limb is cooler.
The patient in the video is MOST likely to display which of the following gait compensations? {weak L hip abd)
1.Backward trunk leaning
2.Forward trunk leaning during stance phase
3.Trunk side leaning to the left side during stance phase
4.Trunk side leaning to the right side during stance phase
3,3
1. This patient presents with weak hip abductors. This impairment will lead to a Trendelenburg gait, which includes trunk leaning to the ipsilateral side of the weak hip abductor. Backward trunk leaning is related to weak hip extensors.
2. This patient presents with weak hip abductors. This impairment will lead to a Trendelenburg gait, which includes trunk leaning to the ipsilateral side of the weak hip abductor. Forward trunk lean is related to weak quadriceps.
3. This patient presents with weak hip abductors as evidenced by the compensatory movement into hip flexion. This impairment will lead to a Trendelenburg gait, which includes trunk leaning to the ipsilateral side of the weak hip abductor.
4. This patient presents with weak hip abductors. This impairment will lead to a Trendelenburg gait, which includes trunk leaning to the ipsilateral side of the weak hip abductor
Which of the following gait parameters are MOST important for independence in community mobility for an individual who had a cerebrovascular accident?
1.Stride length and knee flexion strength
2.Speed and knee extension strength
3.Endurance and knee flexion strength
4.Stride length and ankle dorsiflexion strength
4,2
1. The relationship between impairments and gait parameters is very complex, however velocity was found to be the only single measure that predicted walking classification. A combination of gait velocity and knee extension control was found to be highly predictive of mobility function in patients who have had a cerebrovascular accident. Therefore stride length and knee flexion strength are incorrect.
2. Gait velocity and knee extension control were found to be highly predictive parameters of gait performance.
3. A combination of gait velocity and knee extension control was highly predictive of functional mobility in patients who have had a cerebrovascular accident. Endurance and knee flexion strength are not the most critical determinants of independence in community mobility in subjects with hemiplegia.
4. A combination of gait velocity and knee extension control was highly predictive of functional mobility in patients who have had a cerebrovascular accident. Stride length and ankle strength are not the most critical determinants of independence in community mobility in subjects with hemiplegia.
To conduct an experimental study on pain in postsurgical orthopedic patients, a physical therapist randomly assigns patients to two groups. One group is treated with transcutaneous electrical nerve stimulation, heat, and exercise; the second receives heat and exercise only. In this experimental design, transcutaneous electrical nerve stimulation is the:
1.continuous variable.
2.dependent variable.
3.discrete variable.
4.independent variable.
2,4
1. "Continuous" is a classification of variables based on the method of quantifying the variable, not based on the role of the variable in the experimental design. Continuous variables may theoretically be measured to a finer and finer degree.
2. The dependent variable can be thought of as the effect or response, which in this case is pain.
3. "Discrete" is a classification of variables based on the method of quantifying the variable, not based on the role of the variable in the experimental design. A discrete variable is one that can assume only distinct values.
4. The independent variable can be thought of as the cause or treatment. In this case, the transcutaneous electrical nerve stimulation is the treatment or independent variable.
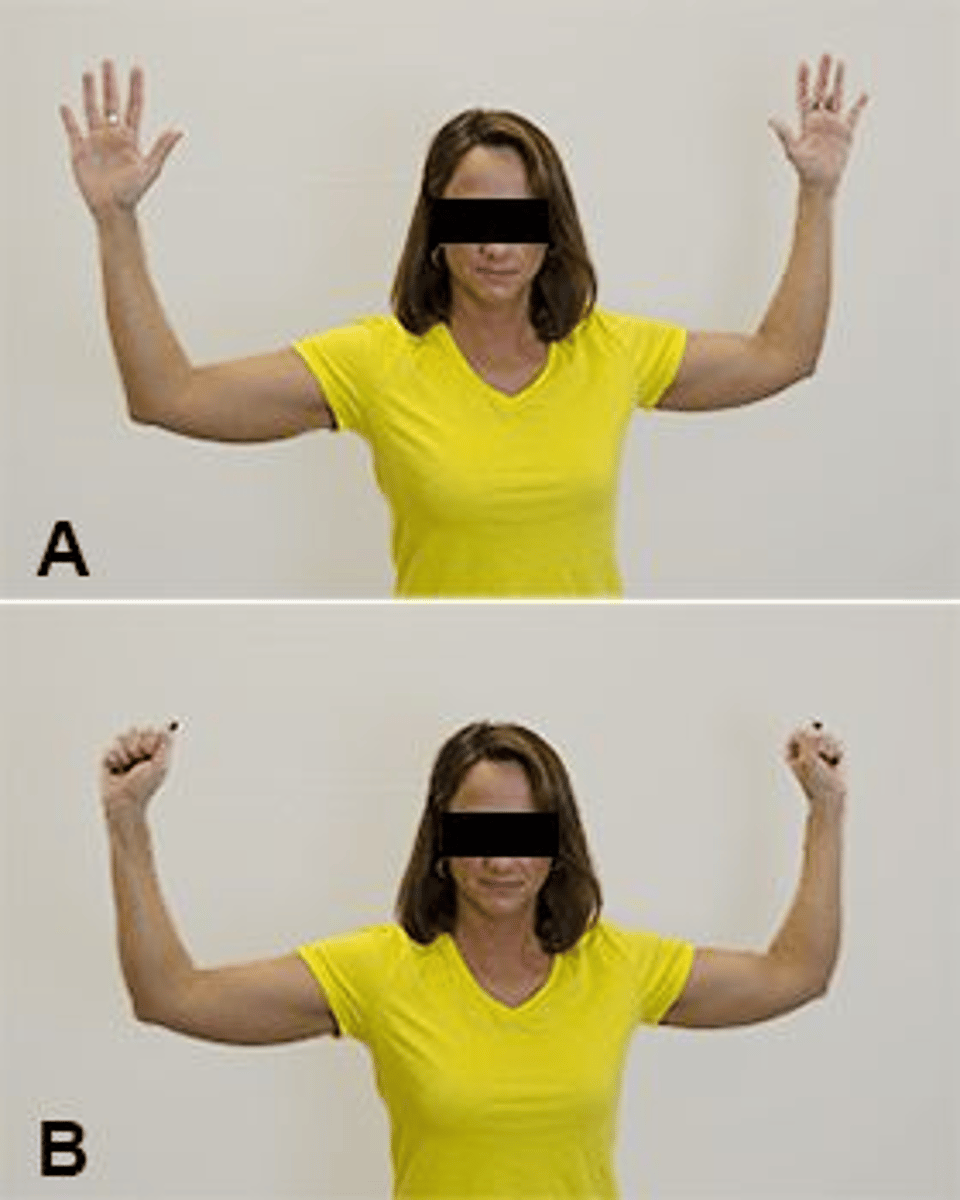
A patient has a positive result after 1 minute on the test depicted in the photographs. Which of the following additional tests is MOST appropriate to perform to establish a firm diagnosis?
1.Adson Test
2.Empty Can Test
3.Cervical Compression Test
4.Acromioclavicular joint palpation
1,1
1. The Roos Test, shown in the photographs, is used to test for the presence of thoracic outlet syndrome. The Adson Test is also used to test for thoracic outlet syndrome.
2. The Empty Can Test is used to assess for rotator cuff tear. The Roos Test, shown in the photographs, is used to test for the presence of thoracic outlet syndrome.
3. The Roos Test, shown in the photographs, is used to test for the presence of thoracic outlet syndrome. A positive Cervical Compression Test is more suggestive of other pathologies, including disc herniation, nerve root irritation, or vertebral fractures, but not thoracic outlet syndrome.
4. The Roos Test is used to test for the presence of thoracic outlet syndrome. AC joint palpation tests for AC joint involvement
Which of the following interventions is MOST important to perform in conjunction with manual lymphatic drainage?
1.Muscle strengthening
2.Muscle stretching
3.Joint mobilization
4.Diaphragmatic breathing
4,4
1. While strengthening exercise is recommended for lymphedema, it is not required for manual lymphatic drainage to be successful.
2. Muscle stretching is important for maintaining flexibility and range of motion, it is not required for manual lymphatic drainage.
3. While there are times when joint mobilization is indicated with this diagnosis, it is not a requirement for a successful outcome with manual lymphatic drainage.
4. Diaphragmatic breathing is necessary to create changes in intrathoracic pressure that results in increased lymphatic drainage in the thoracic lymphatic duct. It is recommended to be performed after manual lymphatic drainage.
Which of the following test findings is MOST consistent with a diagnosis of idiopathic pulmonary arterial hypertension?
1.VO2 max of 25 mL/kg/minute
2.Cardiac index of 0.8 L/minute/m2
3.Right atrial pressure of 15 mm Hg
4.Six-Minute Walk Test result of 1640 ft (500 m)
3,3
1. A VO2 max of 25 mL/kg/minute is associated with no to only mild impairments. This is unlikely to be observed in patients who have idiopathic pulmonary arterial hypertension.
2. A cardiac index of 0.8 L/min/m2 is inconsistent with this diagnosis. A lower cardiac index is expected.
3. A right atrial pressure of 15 mm Hg is indicative of idiopathic pulmonary arterial hypertension and is an indication for lung transplantation. Normal atrial pressures are 0-8 mm Hg.
4. The ability to walk 500 meters during a Six-Minute Walk Test is inconsistent with this diagnosis. This is a normal distance for this test.
A patient recovering from Guillain-Barré syndrome exhibits Poor (2/5) quadriceps strength. The BEST therapeutic exercise would be active knee extensions with which of the following parameters?
1.Multiple repetitions in sidelying, maximally stressing the quadriceps
2.Limited number of repetitions in sidelying, avoiding fatigue of the quadriceps
3.Limited number of repetitions in sitting, avoiding fatigue of the quadriceps
4.Multiple repetitions in sitting, maximally stressing the quadriceps
1,2
1. In patients recovering from Guillain-Barré syndrome, overwork will delay recovery.
2. In patients recovering from Guillain-Barré syndrome, overwork and fatigue should be avoided.
3. In patients recovering from Guillain-Barré syndrome, poor strength would prohibit knee extension against gravity.
4. In patients recovering from Guillain-Barré syndrome, overwork will delay recovery, and poor strength would prohibit knee extension against gravity.
For a patient who takes a thiazide medication (hydrochlorothiazide), which of the following combinations of signs may indicate an adverse effect of the medication?
1.Agitation, dizziness, dyspnea, and hyperventilation
2.Abdominal cramps, agitation, dyspnea, and numbness
3.Clammy skin, dizziness, hyperventilation, and hypotension
4.Abdominal cramps, clammy skin, hypotension, and numbness
1,3
1. Thiazide diuretics increase secretion of sodium, so an adverse drug effect is too much secretion, which leads to hyponatremia. Agitation and dyspnea are signs of hypernatremia
2. Thiazide diuretics enhance secretion of sodium and potassium in the urine, leading to hyponatremia and hypokalemia. The signs given are for hypernatremia and hyperkalemia
3. Thiazide diuretics enhance secretion of sodium and potassium in the urine, leading to hyponatremia and hypokalemia. Clammy skin and hypotension are signs of hyponatremia, and dizziness and hyperventilation are signs of hypokalemia
4. Abdominal cramps and numbness are signs of hyperkalemia. Potassium is excreted along with sodium in patients who are taking thiazide diuretics, so hypokalemia rather than hyperkalemia may result
Which of the following integumentary system observations is consistent with skin cancer?
1.Dark, raised spot that bleeds with minimal contact
2.Redness, scaling, and edema of the skin
3.Red fluid-filled vesicles that vary in size
4.Ring-shaped pigmented patches covered with scales
1,1
1. These observations are classic signs of malignant melanoma
2. These observations are signs of contact dermatitis
3. These observations are signs of herpes zoster
4. These observations are signs of tinea corporis, also known as ringworm
44 y/o female
Gradual onset of numbness & pain 3/10 in the left medial ankle & plantar aspect of the foot starting 2 mos ago
Pain & numbness worse at night when resting or after standing continuously for 45 minutes
DM II (hemoglobin A1c of 6.8%)
Elementary school teacher required to stand most of the day
Pain Catastrophizing Scale score of 12
Patient has goal of beginning a walking program but has been unable to start due to increased symptoms with walking 30 minutes or longer
Physical Therapy Examination(s)
Decreased light touch & pin prick sensation on plantar aspect of L foot
2+ L1 and S1 reflexes bilaterally
AROM of left ankle: PF 54°, DF 17°, inversion 33°, eversion 18° with reproduction of numbness
Strength: left ankle plantar flexors Normal (5/5), left dorsiflexors Normal (5/5)
Which of the following pain presentations is BEST reflected by the symptoms?
1.Nociplastic
2.Nociceptive
3.Neurogenic
4.Psychogenic
1. Nociplastic pain is associated with symptoms that do not have a clear anatomical correlate, is widespread, and/or not consistent. The current patient has symptoms that have a clear anatomical correlate and are localized to a region. Therefore, nociplastic is not the most appropriate response.
2. Nociceptive pain refers to pain resulting primarily from stimulation of nociceptors, often with a clear stimulus-response relationship between movement and symptoms. The patient has medial ankle and foot pain that is increased with active ankle eversion and activity; however, pain radiates, occurs with rest at night, and the patient has loss of sensation which are not consistent with nociceptive pain. Therefore, nociceptive is not the most appropriate response.
3. The patient has symptoms that are consistent with neurologic involvement, including radiating ankle and foot pain, pain with rest at night, and loss of sensation. Therefore, neurogenic pain is the most appropriate response.
4. Psychogenic pain is pain that is associated with cognitive or emotional context. The current patient has normal ratings of pain catastrophizing. There is no indication that the patient's pain is psychogenic.
Which of the following tests is MOST likely to reproduce the patient's symptoms?
1.Tinel Test
2.Windlass Test
3.Royal London Hospital Test
4.Fibular (peroneal) nerve tensioning
1,1
1. The Tinel Test assesses for neurological symptoms. The patient has numbness, radiating pain, and loss of sensation which is consistent with neurological involvement. Therefore, the Tinel's Test is likely to reproduce symptoms.
2. The Windlass Test assesses the plantar fascia and is likely to be positive for a patient with plantar fasciitis. The current patient has heel and foot pain symptoms; however, the positive dermatome findings and presence of numbness are not consistent with plantar fasciitis.
3. The Royal London Hospital Test is likely to be positive for a patient with Achilles tendinopathy, which is not consistent with the patient presentation.
4. Fibular nerve tensioning assesses for neurological symptoms. The patient has symptoms consistent with neurological involvement however the symptoms are located medially and reproduced with ankle eversion which is not consistent with fibular nerve entrapment.
Which of the following conditions is MOST consistent with the patient's presentation?
1.Plantar fasciitis
2.Tarsal tunnel syndrome
3.Achilles tendinopathy
4.Medial tibial stress syndrome
2,2
1. Plantar fasciitis presents as medial heel pain and pain along the plantar aspect of the foot that is reproduced with activity and can result in decreased mobility. The current patient has medial heel and foot pain that increases with activity; however, the patient also has loss of sensation and numbness which are not consistent with plantar fasciitis.
2. Tarsal tunnel syndrome is an entrapment of the tibial nerve and may result in increased pain with repetitive/strenuous activities. The current patient has symptoms that are consistent with neurological involvement, and tarsal tunnel syndrome.
3. Achilles tendinopathy presents as pain proximal to the calcaneus that is reproduced with activity and can result in decreased mobility. The current patient has symptoms that come on with activity, at night, and pain and numbness into the plantar foot which is not consistent with Achilles tendinopathy.
4. Medial tibial stress syndrome presents is lower leg pain that increases with exercise. Pain is typically located over the distal two-thirds of the posteromedial tibia and often results in decreased ankle mobility. The current patient does not have pain that is consistent with medial tibial stress syndrome.
Which of the following interventions is MOST appropriate for the patient?
1.Anterior glide of the tibiofibular joint
2.Concentric single-leg heel raises with resistance
3.Repeated passive ankle dorsiflexion with eversion
4.Repeated passive ankle plantar flexion with inversion
3,3
1. A common intervention for a nerve entrapment is joint mobilization; however a distal tibiofibular anterior glide is most likely to be associated with ankle plantar flexion and the fibular nerve. The patient has full active plantar flexion and the symptoms are consistent with tibial nerve involvement making this an inappropriate response.
2. The patient has full ankle plantar flexion strength, therefore a concentric single leg heel raise is not the most appropriate response.
3. The patient has symptoms consistent with a tibial nerve entrapment at the tarsal tunnel. A common intervention for a nerve entrapment is nerve gliding/flossing. Repeated passive ankle dorsiflexion with eversion is a nerve gliding/flossing technique that is appropriate for the tibial nerve.
4. Repeated passive ankle plantarflexion with inversion is a nerve gliding technique for the fibular nerve. The patient has symptoms consistent with tibial nerve involvement, not fibular nerve.