Palladini craniofacial anomalies
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
108 Terms
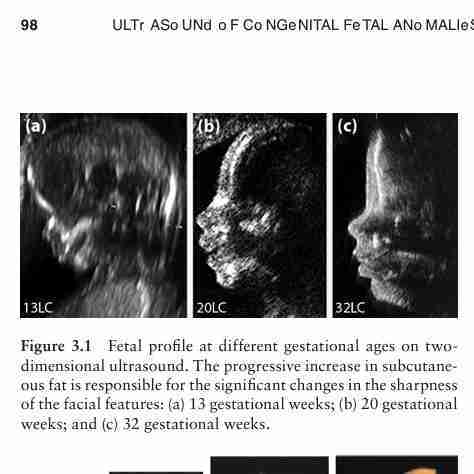
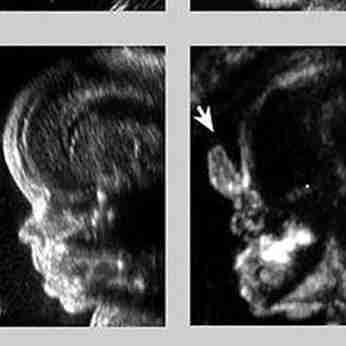
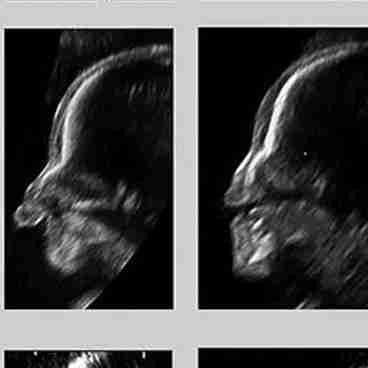
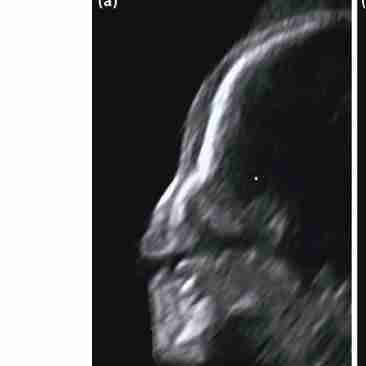
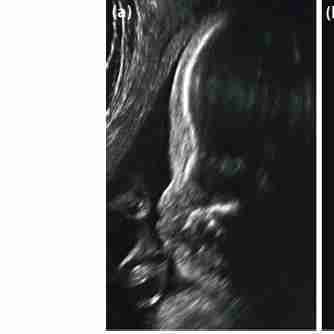
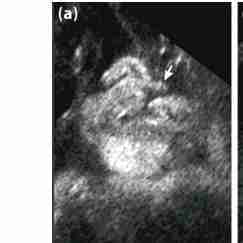
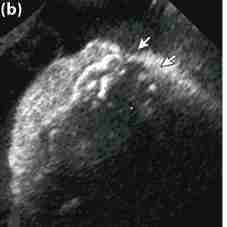
Fetal profile at different gestational ages on two- dimensional ultrasound. The progressive increase in subcutaneous fat is responsible for the significant changes in the sharpness of the facial features: (a) 13 gestational weeks; (b) 20 gestational weeks; and (c) 32 gestational weeks.
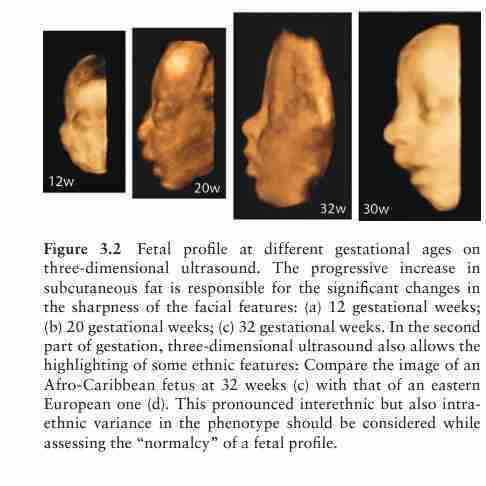
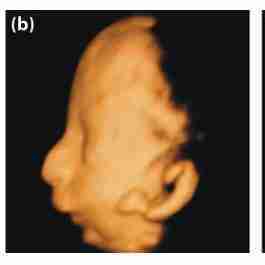
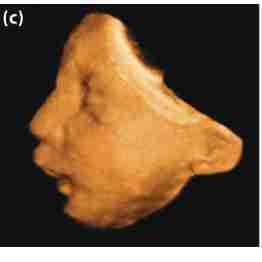
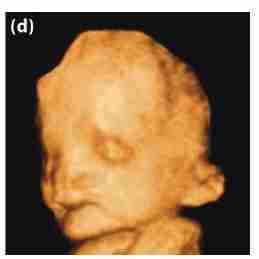
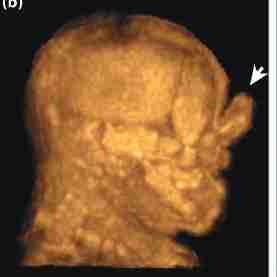
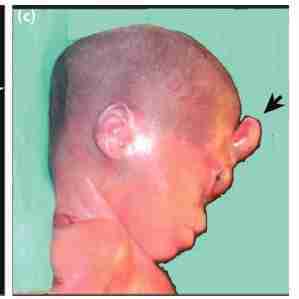
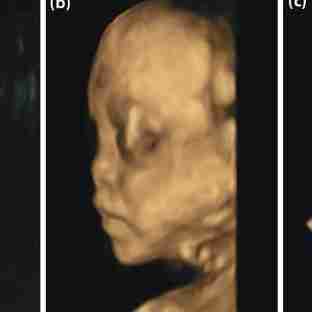
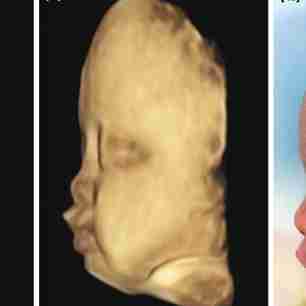
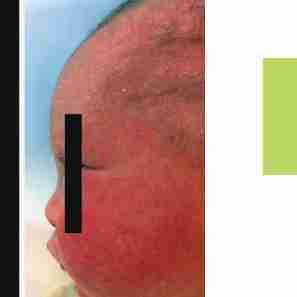
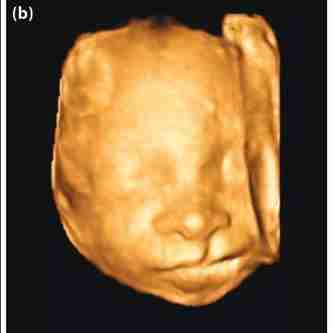
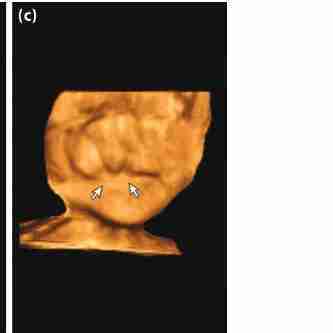
Fetal profile at different gestational ages on three-dimensional ultrasound. The progressive increase in subcutaneous fat is responsible for the significant changes in the sharpness of the facial features: (a) 12 gestational weeks; (b) 20 gestational weeks; (c) 32 gestational weeks. In the second part of gestation, three-dimensional ultrasound also allows the highlighting of some ethnic features: Compare the image of an Afro-Caribbean fetus at 32 weeks (c) with that of an eastern European one (d). This pronounced interethnic but also intraethnic variance in the phenotype should be considered while assessing the “normalcy” of a fetal profile.

Orbits ,ventral

Orbits,lateral
Maxilla lips

Tongue pharynx
Lower alveolus

Mandible

Thyroid
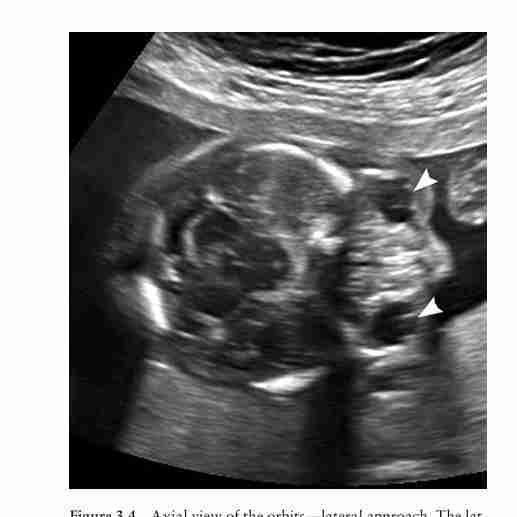
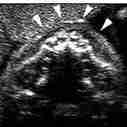
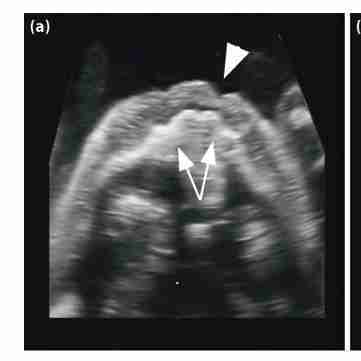
Axial view of the orbits—lateral approach. The lateral walls of the orbits and the midline structures (ethmoid) are clearly displayed. The lenses (arrowheads) are also visible in this case, though they are better displayed with a ventral approach
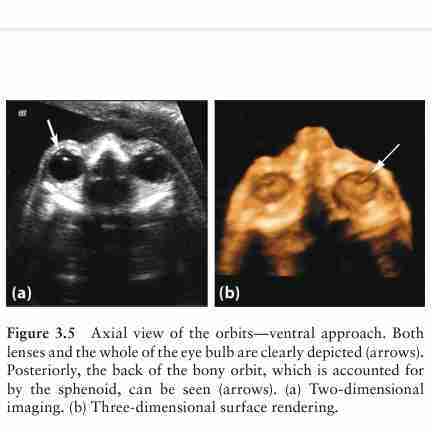
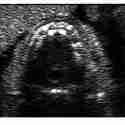
Axial view of the orbits— ventral approach. Both lenses and the whole of the eye bulb are clearly depicted (arrows). Posteriorly, the back of the bony orbit, which is accounted for by the sphenoid, can be seen (arrows). (a) Two-dimensional imaging. (b) Three-dimensional surface rendering.
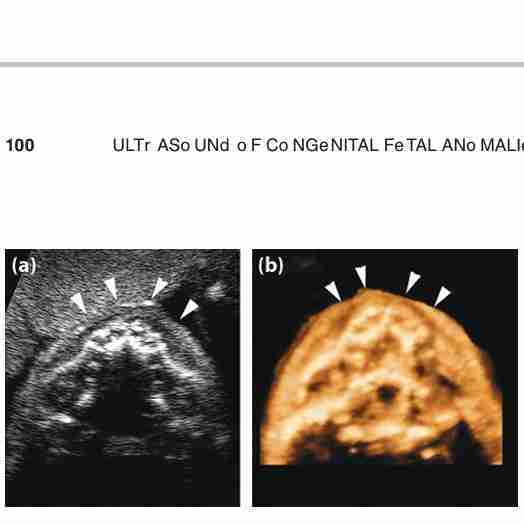
Lower maxilla/upper alveolar ridge—ventral approach. The alveoli of the upper teeth are positioned symmetrically in relation to the midline and the maxillary sinuses. In front of the upper alveolar ridge, the upper lip, displayed cross-sectionally, is visible (arrowheads). (a) Two-dimensional imaging. (b) Three-dimensional surface rendering.

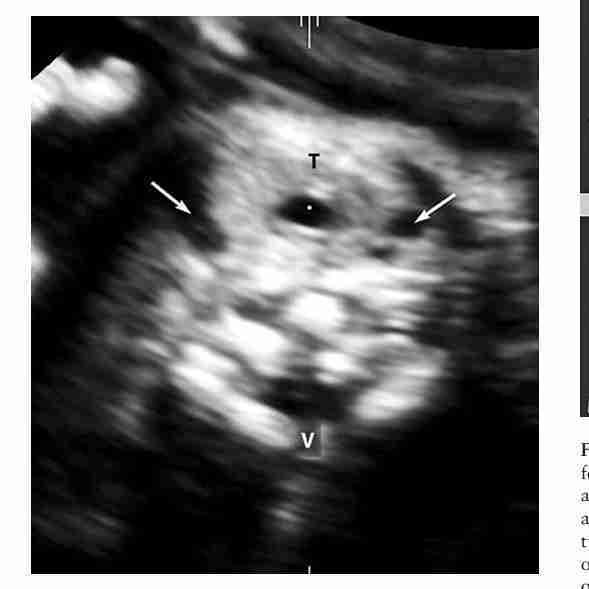
Tongue/pharynx—ventral approach. Just caudal to the upper alveolar ridge, the tongue (T) can be seen in the mouth. The oropharynx (arrows) is visualized posteriorly, in the prevertebral area. Lateral to the tongue, the two mandibular rami are seen in cross-section (arrowheads). Anteriorly, the upper lip is visible only if the plane is obtained with the mouth shut. (a) Twodimensional imaging. (b) Three-dimensional surface rendering.
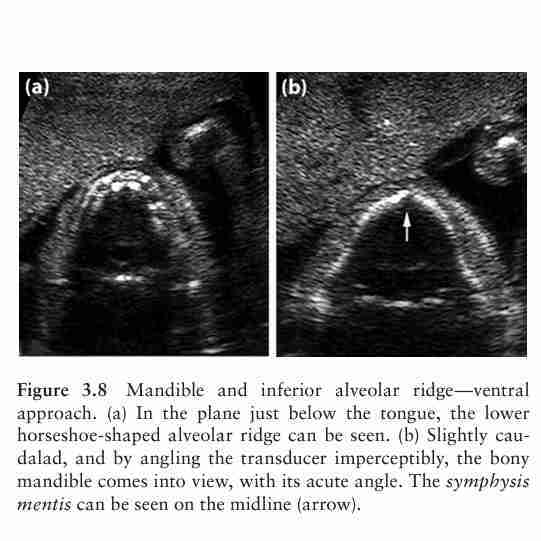
Mandible and inferior alveolar ridge—ventral approach. (a) In the plane just below the tongue, the lower horseshoe-shaped alveolar ridge can be seen. (b) Slightly caudalad, and by angling the transducer imperceptibly, the bony mandible comes into view, with its acute angle. The symphysis mentis can be seen on the midline (arrow).
Thyroid—ventral approach. In this plane, the thyroid (T) appears as a weakly hyperechoic midline round structure surrounding the trachea (reference dot). This appears as a small round sonolucent area. The two jugular veins can be seen laterally, as small round sonolucent areas (arrows); posteriorly, the vertebral body (V) is visible
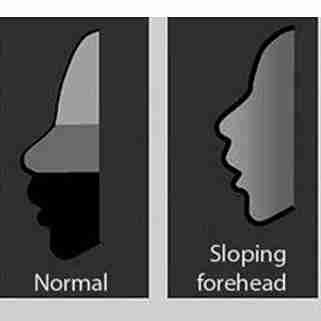
A sloping forehead is typical of microceph
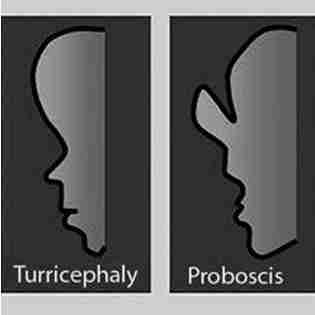
Proboscis and arhinia are associated with holoprosencephaly
Turricephaly, due to early closure of the coronal suture, is typical of Apert syndrome (acrocephalosyndactyly)

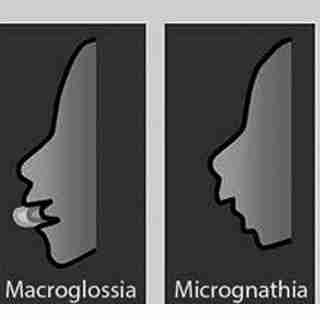
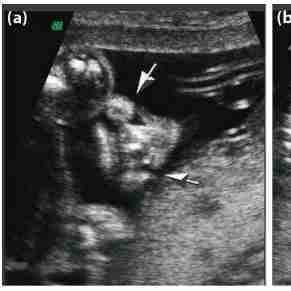
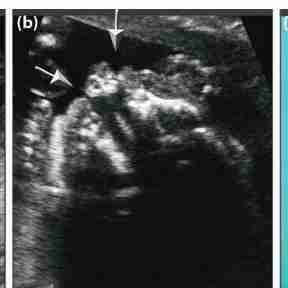
Mild macroglossia can be found in trisomy 21 (Down syndrome), whereas severe macroglossia is typical of Beckwith–Wiedemann syndrome
Micrognathia is associated with trisomy 18 and with a considerable number of nonchromosomal syndromes (fetal akinesia deformation sequence [FADS], skeletal dysplasia, etc.).
![<p>Mild macroglossia can be found in trisomy 21 (Down syndrome), whereas severe macroglossia is typical of Beckwith–Wiedemann syndrome</p><p></p><p></p><p>Micrognathia is associated with trisomy 18 and with a considerable number of nonchromosomal syndromes (fetal akinesia deformation sequence [FADS], skeletal dysplasia, etc.).</p>](https://knowt-user-attachments.s3.amazonaws.com/731d64ff-df6c-4882-9aec-ac79641464a6.jpg)

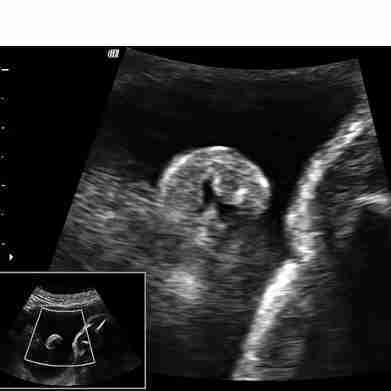
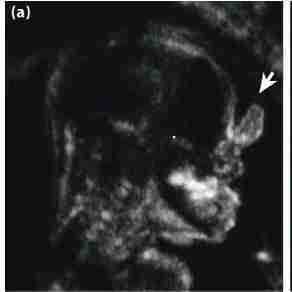
Midsagittal view of the fetal facial profile. In this view, the following structures can be recognized: the frontal area, the nasal root, the nose with the nasal bone (arrow), the lips with the bony palate (bp) in cross-section, and the chin, with the mandible (m) in cross-section. It should be noted that if the view is perfectly on the midline, as in this case, the orbits cannot be seen, this being a symmetric organ. In addition, due to the yet- unossified metopic suture, the ultrasound beam penetrates deep in the fetal head, allowing a good view of the corpus callosum (CC) with the cavum septi pellucidi beneath, the quadrigeminal plate, lamina quadrigemina (lq), and the cerebellar vermis (v).
Parasagittal view at the level of the external ear. This view, which is often difficult to obtain with two- dimensional ultrasound, allows visualization of the external ear, which is abnormal or wrinkled in some syndromic conditions. The whole anatomy of the external ear is visible. This image was obtained in a 29-week-old fetus.
Forehead, turricephaly:
Increased vertical diameter of the forehead, due to early closure of the sutures
Nose, arhinia:
Absence of the nose (bones and soft tissues, nostrils included); midline defect, associated with the holoprosencephaly sequence
Nose, proboscis:
Midline soft tissue appendix, protruding from the nasal root area; midline defect, associated with the holoprosencephaly sequence
Mouth, bilateral cleft:
Additional tissue on the philtrum, common in bilateral clefts
Mouth, macroglossia:
Increased volume of the tongue, usually protruding between the lips
Chin, micrognathia:
Hypoplasia of variable degree of the bony mandible, both in the anteroposterior diameter (retrognathia) and in the latero-lateral one

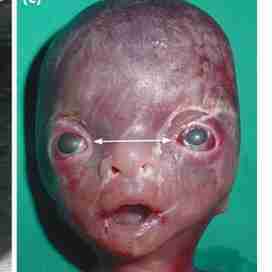
Coronal view of the face. (a) Normal fetus.
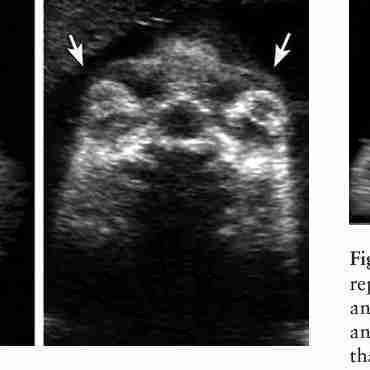
Syndromic fetus (22 weeks) with evident proptosis (arrows).


Oblique view of lips (a) and palate (b). (a) This represents the classic plane for assessment of the lips in normal and abnormal conditions: the lips, the nose with the nostrils, and the chin are displayed.

This plane is cut slightly deeper than the previous one; therefore, it allows recognition of the bony palate and its defects.
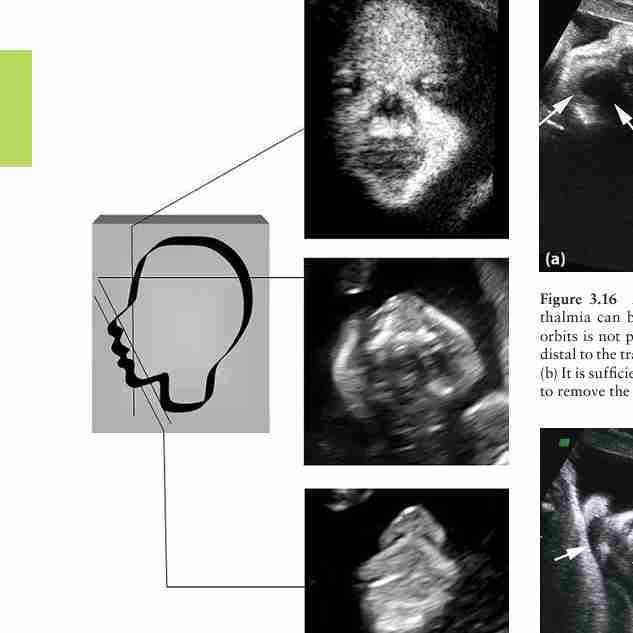
Coronal and oblique ultrasound views for the assessment of the splanchnocranium. This figure illustrates the level of the scanning plane and the corresponding two- dimensional ultrasound image. All views are illustrated in detail in Figures 3.13 and 3.14.
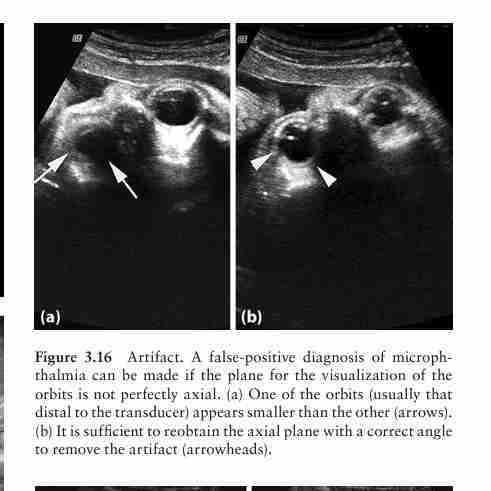
Artifact. A false-positive diagnosis of microphthalmia can be made if the plane for the visualization of the orbits is not perfectly axial. (a) One of the orbits (usually that distal to the transducer) appears smaller than the other (arrows). (b) It is sufficient to reobtain the axial plane with a correct angle to remove the artifact (arrowheads).
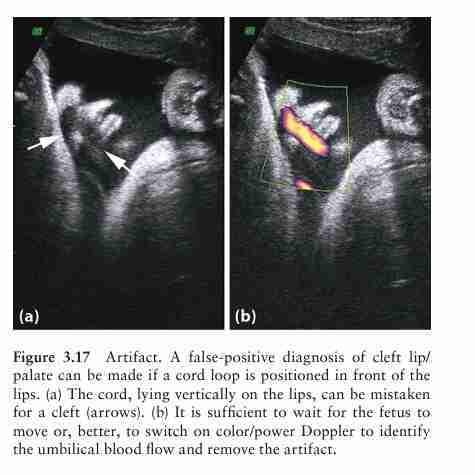
Artifact. A false-positive diagnosis of cleft lip/ palate can be made if a cord loop is positioned in front of the lips. (a) The cord, lying vertically on the lips, can be mistaken for a cleft (arrows). (b) It is sufficient to wait for the fetus to move or, better, to switch on color/power Doppler to identify the umbilical blood flow and remove the artifact.
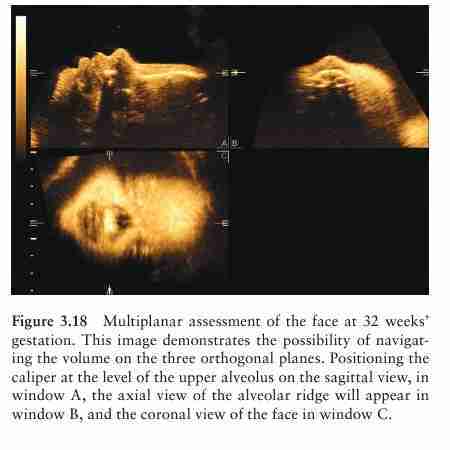
Multiplanar assessment of the face at 32 weeks’ gestation. This image demonstrates the possibility of navigating the volume on the three orthogonal planes. Positioning the caliper at the level of the upper alveolus on the sagittal view, in window A, the axial view of the alveolar ridge will appear in window B, and the coronal view of the face in window C.
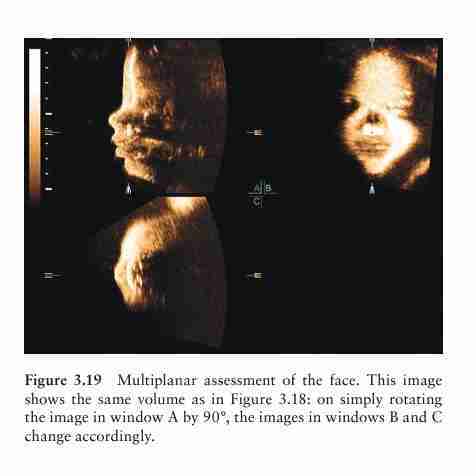
Multiplanar assessment of the face. This image shows the same volume as in Figure 3.18: on simply rotating the image in window A by 90°, the images in windows B and C change accordingly.
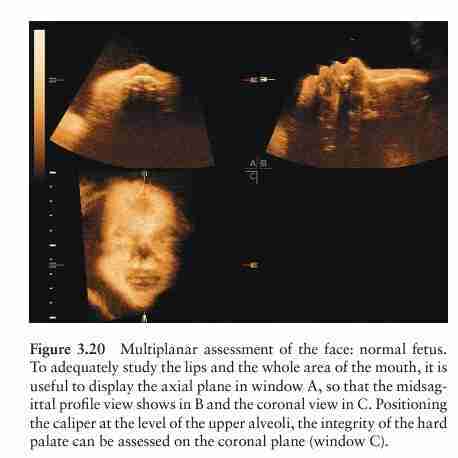
Multiplanar assessment of the face: normal fetus. To adequately study the lips and the whole area of the mouth, it is useful to display the axial plane in window A, so that the midsagittal profile view shows in B and the coronal view in C. Positioning the caliper at the level of the upper alveoli, the integrity of the hard palate can be assessed on the coronal plane (window C).
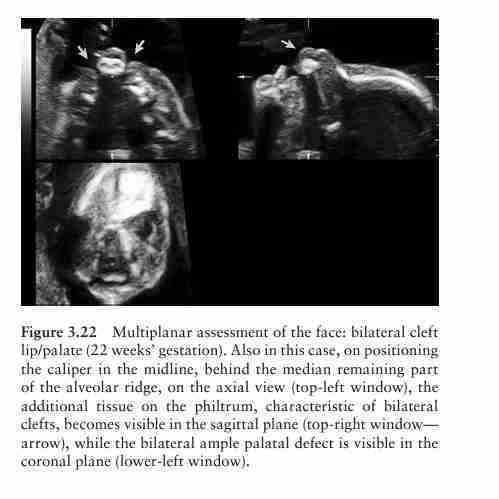
Multiplanar assessment of the face: bilateral cleft lip/palate (22 weeks’ gestation). Also in this case, on positioning the caliper in the midline, behind the median remaining part of the alveolar ridge, on the axial view (top-left window), the additional tissue on the philtrum, characteristic of bilateral clefts, becomes visible in the sagittal plane (top-right window— arrow), while the bilateral ample palatal defect is visible in the coronal plane (lower-left window
Multiplanar assessment of the face: unilateral cleft lip/palate (27 weeks’ gestation). In this case, on positioning the caliper at the level of the bony defect (arrow) in the axial plane (top-left window), the abnormal communication between mouth and nose becomes visible in the coronal plane (lower-left window), with the caliper at the level of the palatal defect
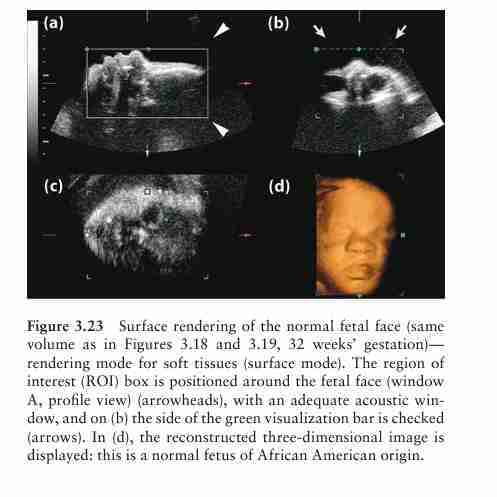
Surface rendering of the normal fetal face (same volume as in Figures 3.18 and 3.19, 32 weeks’ gestation)— rendering mode for soft tissues (surface mode). The region of interest (ROI) box is positioned around the fetal face (window A, profile view) (arrowheads), with an adequate acoustic window, and on (b) the side of the green visualization bar is checked (arrows). In (d), the reconstructed three-dimensional image is displayed: this is a normal fetus of African American origin.
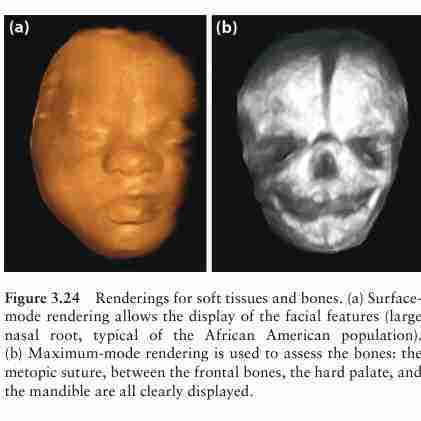
Renderings for soft tissues and bones. (a) Surfacemode rendering allows the display of the facial features (large nasal root, typical of the African American population). (b) Maximum-mode rendering is used to assess the bones: the metopic suture, between the frontal bones, the hard palate, and the mandible are all clearly displayed.
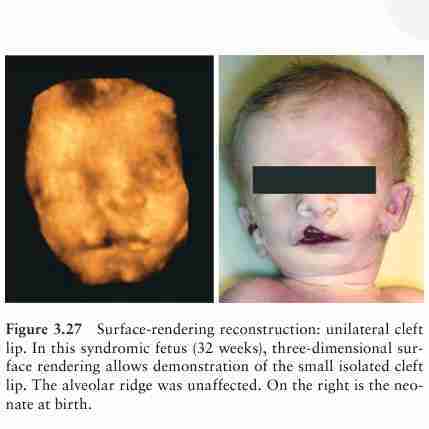
Surface-rendering reconstruction: unilateral cleft lip. In this syndromic fetus (32 weeks), three-dimensional surface rendering allows demonstration of the small isolated cleft lip. The alveolar ridge was unaffected. On the right is the neonate at birth.
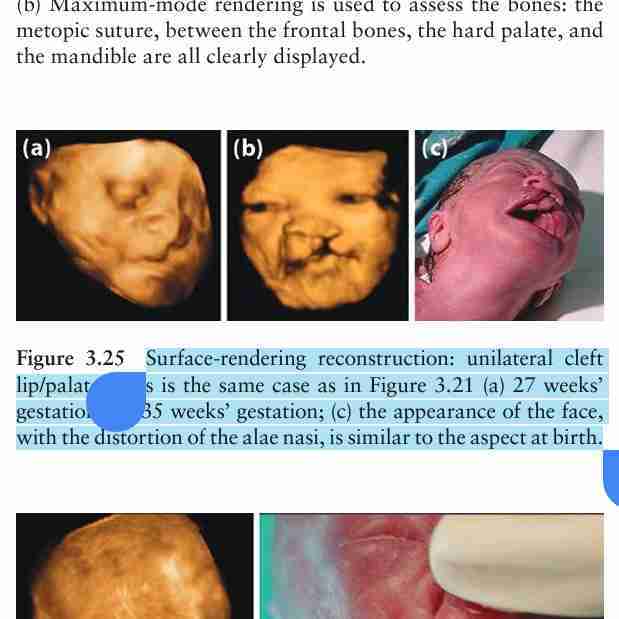
Surface-rendering reconstruction: unilateral cleft lip/palate. This is the same case as in Figure 3.21 (a) 27 weeks’ gestation; (b) 35 weeks’ gestation; (c) the appearance of the face, with the distortion of the alae nasi, is similar to the aspect at birth.
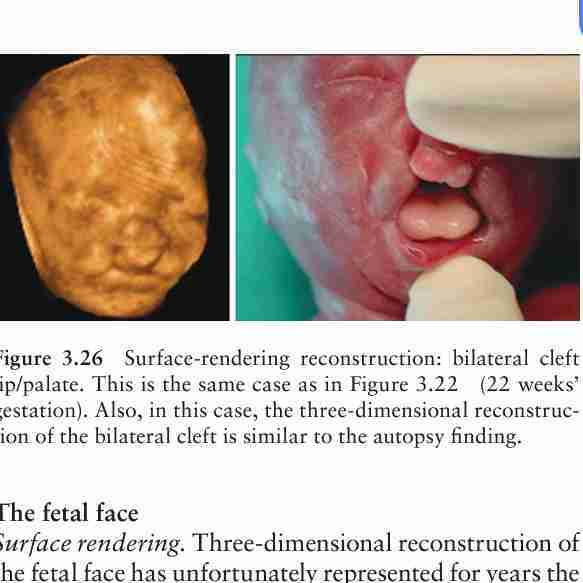
Surface-rendering reconstruction: bilateral cleft lip/palate. This is the same case as in Figure 3.22 (22 weeks’ gestation). Also, in this case, the three-dimensional reconstruction of the bilateral cleft is similar to the autopsy finding.
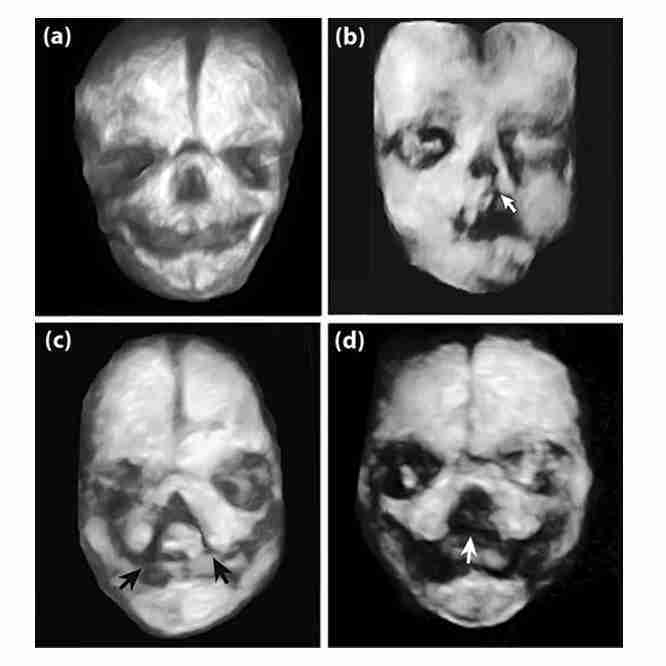
Maximum-mode rendering for the bones. The same volumes used for the images in Figures 3.20 through 3.22 are now processed with the maximum mode, in order to show the bony defects associated with cleft/palate (arrows): (a) normal palate; (b) unilateral cleft lip/palate; (c) bilateral cleft lip/ palate; (d) large midline defect in a fetus with holoprosencephaly (21 weeks’ gestation)
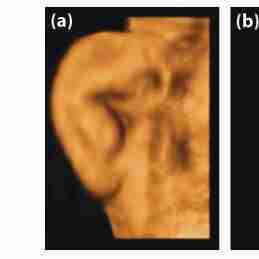
Surface-rendering reconstruction: external ear. (a) Magnification of a normal ear at 32 weeks’ gestation;
syndromic fetus: low-set ears with preauricular tag
syndromic fetus: low-set ears;
syndromic fetus: low-set ears and facial dysmorphism.
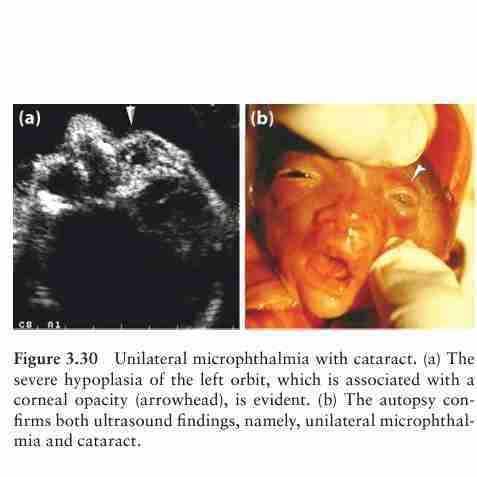
Unilateral microphthalmia with cataract. (a) The severe hypoplasia of the left orbit, which is associated with a corneal opacity (arrowhead), is evident. (b) The autopsy conf irms both ultrasound findings, namely, unilateral microphthalmia and cataract.
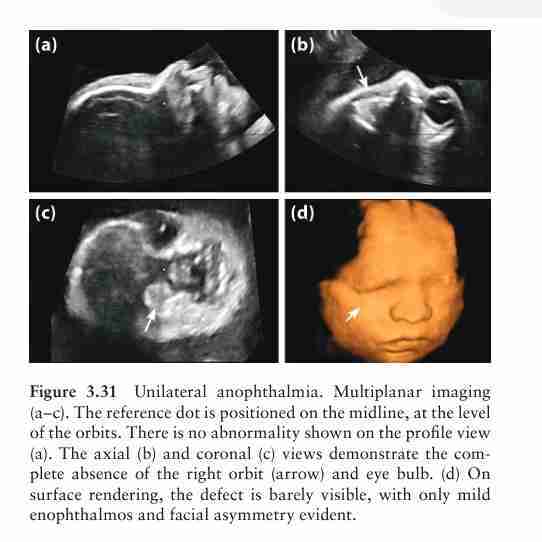
Unilateral anophthalmia. Multiplanar imaging (a–c). The reference dot is positioned on the midline, at the level of the orbits. There is no abnormality shown on the profile view (a). The axial (b) and coronal (c) views demonstrate the complete absence of the right orbit (arrow) and eye bulb. (d) On surface rendering, the defect is barely visible, with only mild enophthalmos and facial asymmetry evident.
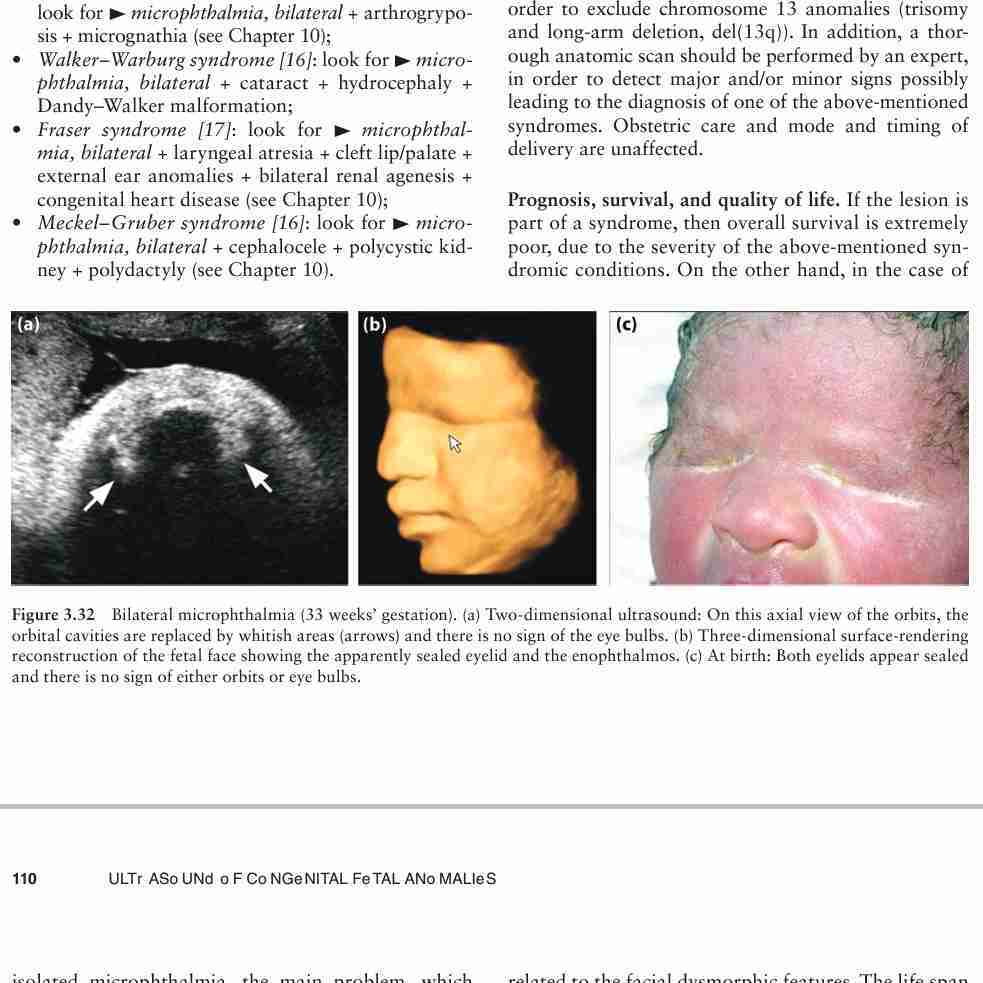
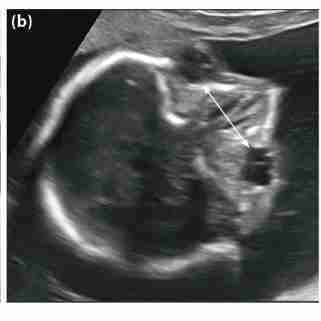
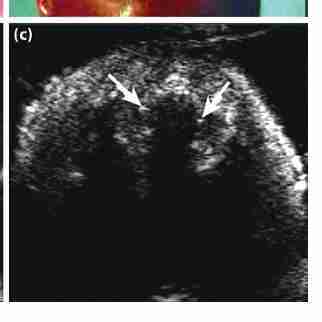
Bilateral microphthalmia (33 weeks’ gestation). (a) Two-dimensional ultrasound: On this axial view of the orbits, the orbital cavities are replaced by whitish areas (arrows) and there is no sign of the eye bulbs. (b) Three-dimensional surface-rendering reconstruction of the fetal face showing the apparently sealed eyelid and the enophthalmos. (c) At birth: Both eyelids appear sealed and there is no sign of either orbits or eye bulbs.
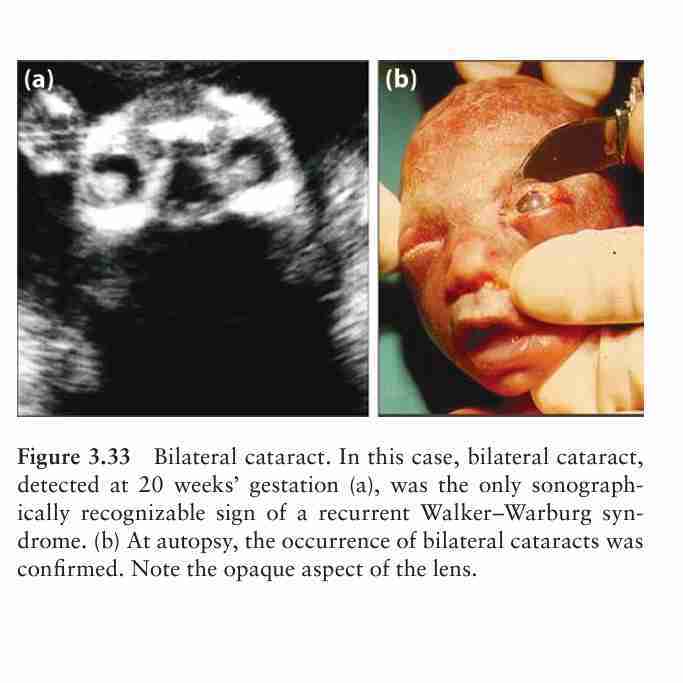
Bilateral cataract. In this case, bilateral cataract, detected at 20 weeks’ gestation (a), was the only sonographically recognizable sign of a recurrent Walker–Warburg syndrome. (b) At autopsy, the occurrence of bilateral cataracts was confirmed. Note the opaque aspect of the lens.

NOrmal fetus at 22 weeks’ gestation (arrowheads: lenses);
Hypertelorismwith evident hypertelorism at 21 weeks’ gestation. This fetus also had constantly open hands, leading to the final diagnosis of restrictive dermopathy. (
autoptic confirmation after termination of pregnancy. Note

Hypotelorism. Three degrees of hypotelorism, which is in most instances associated with holoprosencephaly, are shown: (a) moderate hypotelorism associated with a single nostril (cebocephaly);

Hypotelorism. Three degrees of hypotelorism, which is in most instances associated with holoprosencephaly, are shown: (a) moderate hypotelorism associated with a single nostril (cebocephaly);

b) a single eye socket with two adjacent eye bulbs, associated with arhinia and proboscis;

b) a single eye socket with two adjacent eye bulbs, associated with arhinia and proboscis;
cyclopia (single orbit and eye bulb), also associated with arhinia and proboscis.
cyclopia (single orbit and eye bulb), also associated with arhinia and proboscis.
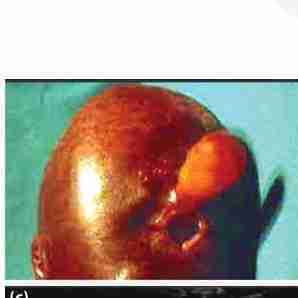
Proboscis in alobar holoprosencephaly. This midsagittal view of the facial profile shows the appendix (arrow) arising from the forehead: (a) two-dimensional ultrasound
Proboscis in alobar holoprosencephaly. This midsagittal view of the facial profile shows the appendix (arrow) arising from the forehead: (a) two-dimensional ultrasound; (b) three-dimensional maximum-mode rendering
Proboscis in alobar holoprosencephaly. This midsagittal view of the facial profile shows the appendix (arrow) arising from the forehead: (a) two-dimensional ultrasound; (b) three-dimensional maximum-mode rendering; and (c) confirmation at autopsy.
Arhinia in semilobar holoprosencephaly. On the midsagittal view, the absence of the nose with the completely flat profile is evident: (a) two-dimensional imaging;

Arhinia in semilobar holoprosencephaly. On the midsagittal view, the absence of the nose with the completely flat profile is evident: (a) two-dimensional imaging; (b) three-dimensional surface-rendering imaging; (

Arhinia in semilobar holoprosencephaly. On the midsagittal view, the absence of the nose with the completely flat profile is evident: (a) two-dimensional imaging; (b) three-dimensional surface-rendering imaging; (c) autoptic confirmation.

Arhinia in semilobar holoprosencephaly (ethmocephaly). The absence of the nasal bones is also evident on this axial view of the orbits: Note the depressed area between the orbits (arrow)

Figure 3.39 Single nostril in semilobar holoprosencephaly (cebocephaly). This oblique view of the lips allows demonstration of the single nostril. The confirmation at autopsy is shown on the right; also note the hypotelorism and microphthalmia.

Figure 3.39 Single nostril in semilobar holoprosencephaly (cebocephaly). This oblique view of the lips allows demonstration of the single nostril. The confirmation at autopsy is shown on the right; also note the hypotelorism and microphthalmia.
Binder syndrome. Midsagittal profile view. (a) Two-dimensional ultrasound, showing the flat profile and the small, vertical nose;
Binder syndrome. Midsagittal profile view. (a) Two-dimensional ultrasound, showing the flat profile and the small, vertical nose; (b) three-dimensional surface-rendering at 24 weeks
Binder syndrome. Midsagittal profile view. (a) Two-dimensional ultrasound, showing the flat profile and the small, vertical nose; (b) three-dimensional surface-rendering at 24 weeks; (c) three-dimensional surface-rendering at 34 weeks; a
Binder syndrome. Midsagittal profile view. (a) Two-dimensional ultrasound, showing the flat profile and the small, vertical nose; (b) three-dimensional surface-rendering at 24 weeks; (c) three-dimensional surface-rendering at 34 weeks; and (d) the neonate at birth.
Isolated cleft lip. (a) On two-dimensional imaging, the axial view of the upper alveolar ridge shows an intact alveolus (arrows) and the small lateral cleft lip (arrowhead) in a 24-week-old fetus.
Isolated cleft lip. (a) On two-dimensional imaging, the axial view of the upper alveolar ridge shows an intact alveolus (arrows) and the small lateral cleft lip (arrowhead) in a 24-week-old fetus. (b) The corresponding three-dimensional surface-rendered image;
Isolated cleft lip another case of bilateral isolated cleft lip (arrows) at 28 weeks’ gestation
Unilateral cleft lip/palate. Unilateral cleft determining distortion of the alae nasi (27 weeks’ gestation). (a) Oblique view, demonstrating the lip defect and the distortion of the alae nasi (arrow
Unilateral cleft lip/palate. Unilateral cleft determining distortion of the alae nasi (27 weeks’ gestation). (a) Oblique view, demonstrating the lip defect and the distortion of the alae nasi (arrow); (b) axial view, demonstrating the extent of the bony defect (arrows);

Unilateral cleft lip/palate. Unilateral cleft determining distortion of the alae nasi (27 weeks’ gestation). (a) Oblique view, demonstrating the lip defect and the distortion of the alae nasi (arrow); (b) axial view, demonstrating the extent of the bony defect (arrows); (c) coronal view, demonstrating the abnormal communication between nose and mouth (arrow)

Unilateral cleft lip/palate. Unilateral cleft determining distortion of the alae nasi (27 weeks’ gestation). (a) Oblique view, demonstrating the lip defect and the distortion of the alae nasi (arrow); (b) axial view, demonstrating the extent of the bony defect (arrows); (c) coronal view, demonstrating the abnormal communication between nose and mouth (arrow); (d) the appearance of the defect at birth.
Bilateral cleft lip/palate. (a) Bilateral cleft lip/palate with additional tissue on the philtrum (22 weeks’ gestation). Oblique view, demonstrating the double defect of the lip (arrows), and the additional tissue on the midline
Bilateral cleft lip/palate. (a) Bilateral cleft lip/palate with additional tissue on the philtrum (22 weeks’ gestation). Oblique view, demonstrating the double defect of the lip (arrows), and the additional tissue on the midline; (b) axial view of the same case, demonstrating the double bony defect (arrows);

Bilateral cleft lip/palate. (a) Bilateral cleft lip/palate with additional tissue on the philtrum (22 weeks’ gestation). Oblique view, demonstrating the double defect of the lip (arrows), and the additional tissue on the midline; (b) axial view of the same case, demonstrating the double bony defect (arrows); (c) the appearance of the defect after termination of pregnancy;

Bilateral cleft lip/palate. (a) Bilateral cleft lip/palate with additional tissue on the philtrum (22 weeks’ gestation). Oblique view, demonstrating the double defect of the lip (arrows), and the additional tissue on the midline; (b) axial view of the same case, demonstrating the double bony defect (arrows); (c) the appearance of the defect after termination of pregnancy; (d) another case of syndromic bilateral cleft lip/palate. This coronal view demonstrates the double bony defect.

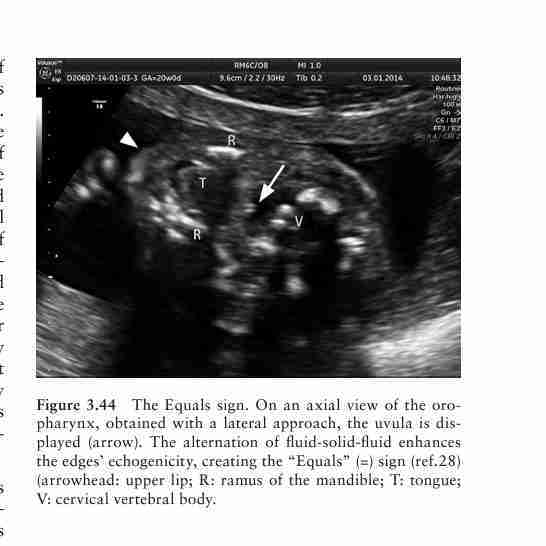
The Equals sign. On an axial view of the oropharynx, obtained with a lateral approach, the uvula is displayed (arrow). The alternation of fluid-solid-fluid enhances the edges’ echogenicity, creating the “Equals” (=) sign (ref.28) (arrowhead: upper lip; R: ramus of the mandible; T: tongue; V: cervical vertebral body.
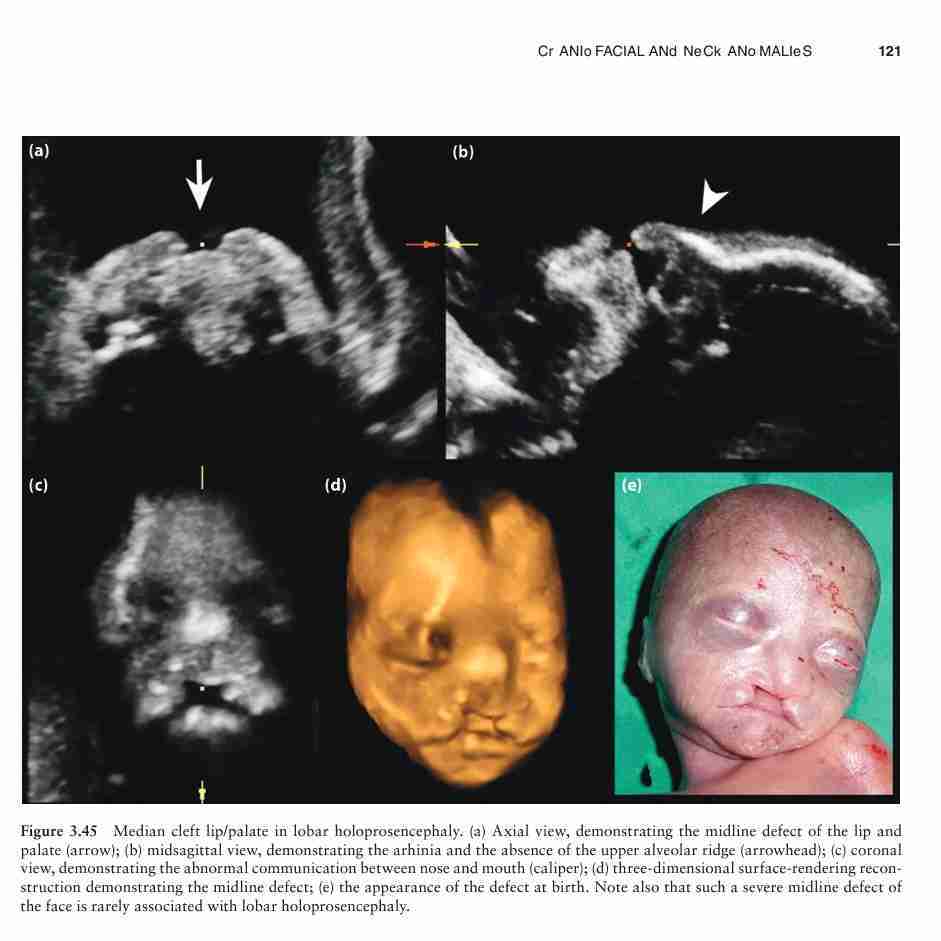
Median cleft lip/palate in lobar holoprosencephaly. (a) Axial view, demonstrating the midline defect of the lip and palate (arrow); (b) midsagittal view, demonstrating the arhinia and the absence of the upper alveolar ridge (arrowhead); (c) coronal view, demonstrating the abnormal communication between nose and mouth (caliper); (d) three-dimensional surface-rendering reconstruction demonstrating the midline defect; (e) the appearance of the defect at birth. Note also that such a severe midline defect of the face is rarely associated with lobar holoprosencephaly.
Bilateral cleft lip/palate. In these two cases, due to the presence of the additional tissue on the philtrum, the midsagittal view of the fetal facial profile is also abnormal, unlike in unilateral clefts, where it is unremarkable. (a–c) 21 weeks’ fetus with trisomy 13: (a) the frontal approach shows bilateral microphthalmia and bilateral CLP;
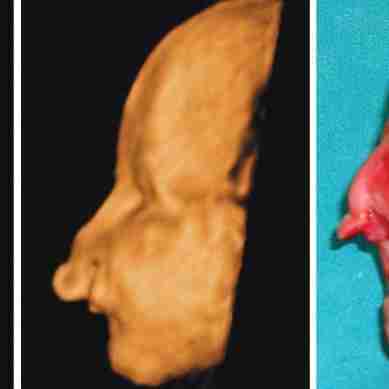
Bilateral cleft lip/palate. In these two cases, due to the presence of the additional tissue on the philtrum, the midsagittal view of the fetal facial profile is also abnormal, unlike in unilateral clefts, where it is unremarkable. (a–c) 21 weeks’ fetus with trisomy 13: (a) the frontal approach shows bilateral microphthalmia and bilateral CLP; (b) on the profile view, the additional tissue on the philtrum is markedly evident;

Bilateral cleft lip/palate. In these two cases, due to the presence of the additional tissue on the philtrum, the midsagittal view of the fetal facial profile is also abnormal, unlike in unilateral clefts, where it is unremarkable. (a–c) 21 weeks’ fetus with trisomy 13: (a) the frontal approach shows bilateral microphthalmia and bilateral CLP; (b) on the profile view, the additional tissue on the philtrum is markedly evident; (c) autoptic confirmation after termination of pregnancy
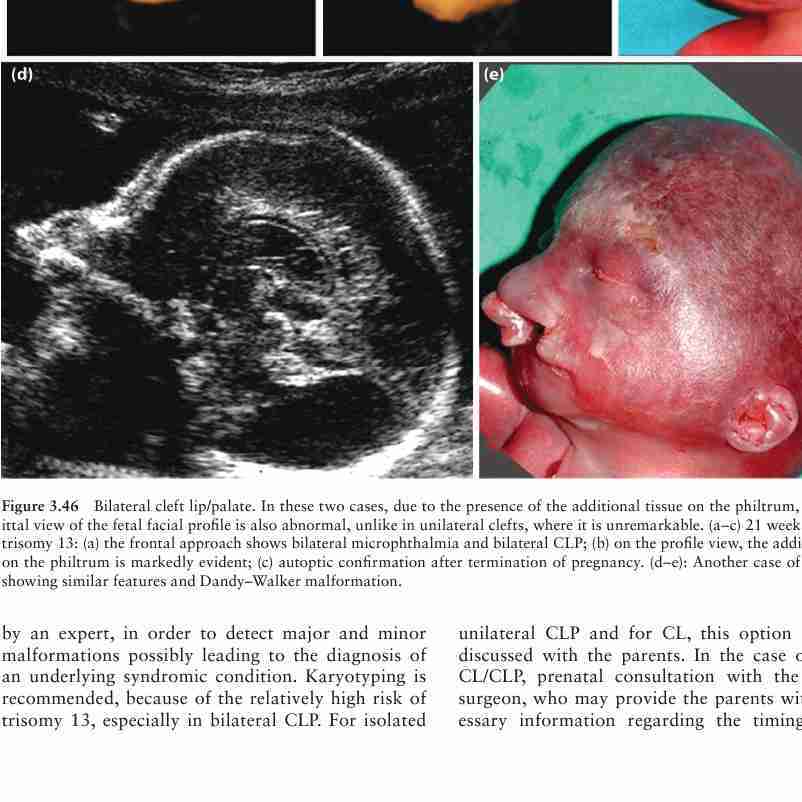
Another case of trisomy 13, showing similar features and Dandy–Walker malformation
Clear diagnosis of cleft extent and depth .
Feasible only with the fetus in a favorable position

Axial lateral
Good assessment of the extent of the lip defect, less of the bony component
In bilateral clefts, inadequate definition of the defect located distal to the transducer
Oblique lips
Excellent assessment of the lip defect and of possibly associated anomalies of the alae nasi
Feasible only with the fetus in a favorable position
Oblique palate
Good assessment of the bony defect and of the relationships with the nasal cavity. It completes the previous view Feasible only with the fetus in a favorable position.
Does not give information on the lip component