Looks like no one added any tags here yet for you.
what symptoms needed to diagnose CAP?
symptoms of a lower respiratory tract infection.
cough, sputum , breathlessness, chest pain.
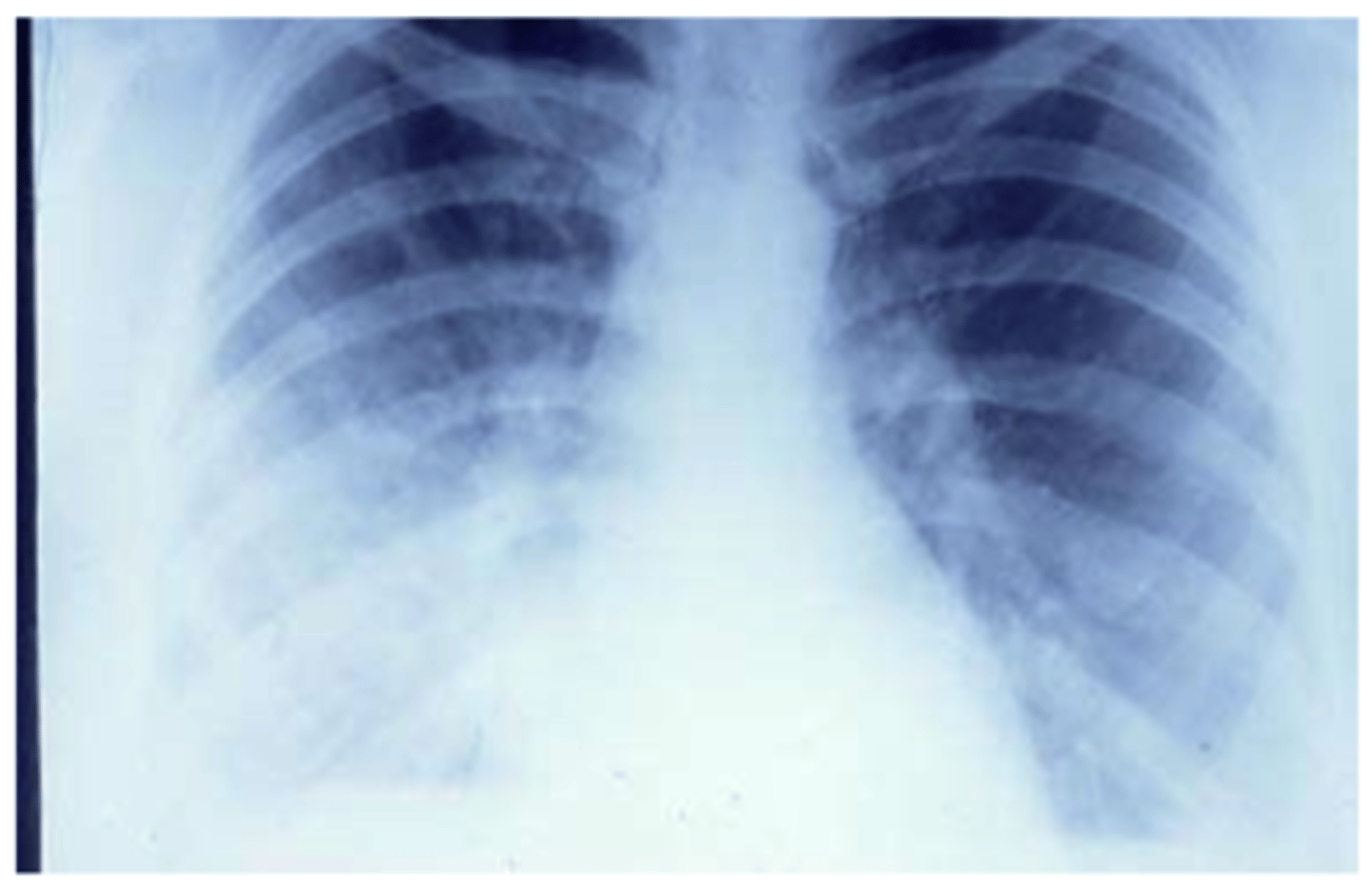
CXR evidence of pneumonia.
what group is CAP most common in?
the elderly
what is the normal O2 stat for a healthy person?
above 94%
what causes 60-80% of CAP cases?
conventional bacterial
what causes 10-20% of CAP?
viruses
Aetiology of CAP? (4 microbes)
bacteria
- S. pneumoniae
- H. influenzae
virus
- M. pneumoniae
- L. pneumophilia
S. pneumoniae (bacteria)
most common cause of CAP in those who don't have COPD.
Capsular polysaccharide is the major virulence factor.
S, pneumoniae relative resistance to penicillin?
MIC >0.1 and <2.0mgs/l.
it is becoming more common as a resistance.
H. influenzae (bacteria)
capsulated H. influenzas is the primary cause of CAP in children who have no received HIB.
non capsulated H. influenzae is an important cause of disease in COPD.
M. pneumoniae (atypical)
mycoplasma is the second most common cause of CAP.
causes >40% of CAP in 17-44 age group.
infection has characteristic extra-pulmonary features.
can cause epidemic CAP.
steven Johnson's syndrome
Life threatening
Skin: blistering, rash, detachment of epidermis
Meds that can cause: carbamazepine, lamotragine
L. pneumophila (atypical)
cause of both sporadic and outbreak CAP.
can cause severe disease particularly in immunocompromised and those who smoke.
Highest mortality, doesn't respond to usual treatments.
L. pneumonia serogroup 1 causes almost all human infection.
L. pneumophilia treatment?
specific treatment with high dose fluoroquinolone or macrolide antibiotics.
How is CAP investigated?
- confirm diagnosis
- assess severity of disease
- define aetiological agent
- identify complications
what microbiological investigations occur for CAP?
- sputum analysis and culture
- immunofluorescence on sputum samples
- blood cultures
- urinary pneumococcal and legionella antigen
what is antimicrobial management for CAP based on?
-assessment of the likely pathogen
-severity of the illness
-likelihood of drug resistance
CAP risk stratification?
CURB65
new confusion (MMT of 8 or less)
urea (>7mmol)
respiratory rate (>30 per min)
blood pressure (<90mmhg for systolic or <60mmHg for diastolic)
65 or more years old
what is low severity CAP?
score of 0 or 1 on CURB 65 scale.
should be managed in community.
treatment of low severity CAP?
oral antibiotics (amoxicillin 500mgs qds for 5 days)
OR
doxycycline 200 mgs loading them 100mg od.
only IV if unable to take oral therapy.
how to treat low severity CAP if there is a penicillin allergy?
ciprofloxacin 400mgs bd + vancomycin.
what level is moderate severity CAP?
score of 2 of CURB65.
managed in hospital.
how to treat moderate severity CAP?
amoxicillin 500mgs qds (standard) for 7 days with clarithromycin 500 mgs bd for 7 days.
OR
doxycycline 200mgs loading then 100mg od.
only IV if unable to take oral.
what score is severe CAP?
3 on CURB65 scale.
how to treat severe CAP?
co-amoxiclav 1.2g tds and amoxicillin 1g tds and clarithromycin 500mgs bd iv for 10 days.
how to treat severe CAP if there is a penicillin allergy?
levofloxacin 500mgs bd and vancomycin 1g bd.
what occurs when CAP score is over 3 (might be legionella?)?
continue co-amoxiclav 1.2 g tds and amoxicillin.
1g tds and clarithromycin 500 mgs db iv for 10 days.
Add levofloxacin 500 mgs bd for 14 days.
Ensure legionella antigen in urine requested and culture sputum (alert lab)
what symptoms hint at legionella?
confusion, diarrhoea, low sodium.
on top of CURB65 level 3 symptoms.
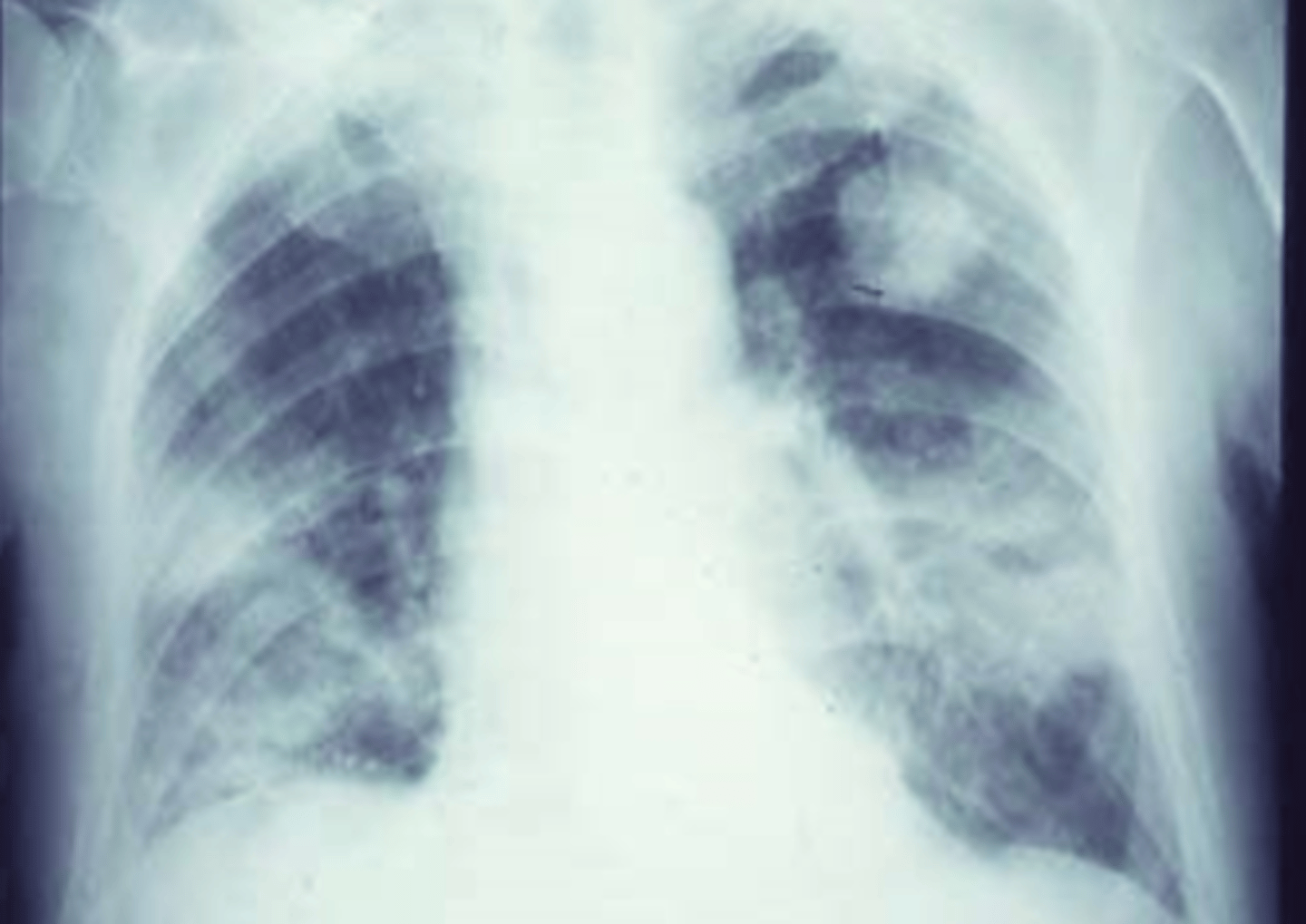
X ray of typical staphylococcus pneumonia
causes abscesses.