#3: Cellular regulation
1/292
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
293 Terms
Genetics
General mechanisms of heredity and variation of inherited single-gene traits
Genomics
Function of all of the human DNA
Heritability
Risk for developing a disorder that is transmitted to one’s children in a recognizable pattern
Gene
segment of DNA containing specific code for the order of the correct amino acid sequence within a designated protein
Genome
the entire set of human nuclear genes
Gene expression
selective activation of a gene to direct the production of its specific protein
Types of alleles
Dominant and recessive
Phenotype
Genetic trait or characteristic that can be observed or determined by a laboratory test
Genotype
The actual alleles for a certain trait (not just what can be observed)
Somatic variations
occur in cells after the child is born – Loss of cellular regulation (ex: Cancer)
Germline variations
Variations in sex cells
Susceptibility genes
DNA Variations that increase the chance for a disorder
Protective or resistance genes
Variations that decrease the chance for a disorder
Single nucleotide polymorphism (SNP)
base in one person’s gene for a specific protein is different
Polymorphism
base of gene changes allow the protein to be made but a difference in how it works
Mutation
base of gene causes a LOSS of protein function and impaired cellular regulation
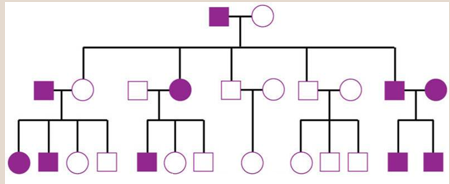
Pedigree
Graph of family history for specific trait or health problem over several generations
Complex inheritance and familial clustering
-Higher rate than normal diseases in families without a specific pattern
-Gender, environment, can also play a part
Penetrance
how often or how well, within a population, a gene is expressed when it is present
Expressivity
degree of expression an individual has when a dominant gene allele or pair of recessive alleles is present
Benefits of genetic testing
Confirm diagnosis, or identify at-risk individuals
Risks of genetic testing
-Genetic testing results do not change
-Psychological or social risks
-Risk for family disruption
-Expensive
-Testing may identify a great risk for a future serious health risk that is incurable
-Depression, blame, guilt
-Discrimination
Direct to consumer testing
-Marketing by for-profit companies without the involvement of a health care professional
-23andMe cleared by FDA; others are not cleared
-Lack of true, in-depth genetic counseling is a problem in interpretation of true risk
Genetic counseling
-Counseling before, during, and after testing is critical
-Health care provider counsels the patient
-The right to know versus the right to not know is the individual patient’s choice
-Results must remain confidential to the patient
Role of medical surgical nurse
-Assists during assessment, testing, and counseling
-Does not provide in-depth counseling, yet can clarify information
-Recognizes patients at risk for genetic disorder
-Ensures clear communication, privacy and confidentiality
-Acts as patient advocate
-Directs patients to accurate sources of information
Specific morphology
Distinct and recognizable appearance, size, and shape
Smaller nuclear-to-cytoplasmic ratio
Nucleus of a normal cell occupies a relatively small amount of space inside the cell
Differentiated function
Every cell has at least one function
Tight adherence
bind closely to other cells
Non-migratory
No wandering throughout the body (Except Blood)
Orderly and well-regulated growth
Cell Cycle with checkpoints to ensure proper division and growth
G1
Growth
S
DNA synthesis
G2
Growth and preparation for mitosis
M
Mitosis (cell division)
Neoplasia
-any new or continued cell growth not needed for normal development or replacement of dead/damaged tissue
-Cellular Regulation has been lost
Benign tumor cells
-Normal cells growing in the wrong place or at the wrong time
-Moles, uterine fibroid tumors, skin tags, endometriosis, nasal polyps
Cancer cells
-Abnormal
-Serve no useful function
-Harmful to normal body tissue
Anaplasia
-Differentiation
-Loss of specific appearance of their parent cells (Poorly Differentiated)
Features of cancer cells
-Anaplasia (Differentiation)
-Large nuclear-to-cytoplasmic ratio
-Nucleus is larger than that of normal cells
-Specific functions lost
-Loose adherence
-Migration (metastasis)
-No contact inhibition
-No regulation of growth – invasive to other cells/organs
-Rapid or continuous cell division (Proliferation)
-Abnormal chromosomes (aneuploidy)
Cancer development
-Carcinogenesis, oncogenesis, malignant transformation
-Initiation → Promotion → Progression (Primary Tumor) → Metastasis
Metastasis
-Metastatic or secondary tumors
-Spread to nearby tissues
-Circulation through blood to new site
-Lymphatic spread
Common cancers for AFAB patients (5)
-Breast
-Lung
-Colorectal
-Uterine
-Melanoma
Common cancers for AMAB patients
-Prostate
-Lung
-Colorectal
-Bladder
-Melanoma
Common cancer risk factors (7)
-Age
-Smoking
-Alcohol consumption
-Excess body weight
-Sedentary lifestyle
-Dietary habits
-Viruses
Physiological impact of cancer
-Pain
-Fatigue
-Infections
-Gastrointestinal
-Lymphedema
-Peripheral neuropathy
-Fertility
Cognitive impact of cancer
-Sleep disturbances
-Delirium
-Concentration problems
-Decreased organizational abilities
-Impaired memory
Oncologic complications of cancer
-Hypercalcemia
-Spinal cord compression
-Superior vena cava syndrome
-Malignant pericardial effusion
-Tumor lysis syndrome
-Syndrome of inappropriate antidiuretic hormone
Psychosocial stressors from cancer
-Distress in cancer
-Depression
Impact of cancer on immunity and clotting function
-Starts to occur when cancer invades the bone marrow and reduce the production and function of WBCs.
-Anemia and Thrombocytopenia
Impact of cancer on GI function
-Appetite Loss
-Alterations in taste
-Constipation/gastric stasis/intestinal obstruction
Impact of cancer on peripheral nerve sensory function
Neurotoxic chemotherapy agents – reduced sensory perception
Impact of cancer on central motor and sensory function
-Bone metastasis results in thinner bones and increased fractures
-Bone metastasis = Hypercalcemia
Impact of cancer on respiratory function
-Lung Tumors or Tumor compression of vasculature
-Radiation and Chemo – pericarditis, valvular disease, loss of myocardial muscle
Impact of cancer on comfort
Pain
Cancer classification
-Grading
-Ploidy
-Staging (clinical, surgical, pathologic)
-TNM
T—Tumor
N—Node
M—Metastasis
-Doubling time and mitotic index
Breast cancer stages
Stage 0, I, II, III, IV
TNM
-T= Tumor size/grade
-N = Lymph nodes
-M = Metastasis
Tumor staging
-TX: Unable to evaluate the primary tumor
-TØ: No evidence of primary tumor
-Tis: Tumor in situ
-T1, T2, T3, and T4: Size and extent of tumor
Node staging
-NX: Unable to evaluate regional lymph nodes
-NØ: No evidence of regional node involvement
-N1, N2, and N3: Number of nodes that are involved and/or extent of spread
Metastasis staging
-MX: Unable to evaluate distant metastasis
-MØ: No evidence of distant metastasis
-M1: Presence of distant metastasis
Cancer grading
-GX – Grade cannot be Determined
-G1: Tumor cells are well differentiated
-G2: Tumor cells are moderately differentiated
-G3: Tumor cells are poorly differentiated, but the tissue of origin can be established
-Tumor cells are poorly differentiated, and determination of the tissue of origin is difficult.
Noninvasive (in situ) breast cancer types
-Ductal carcinoma in situ (DCIS)
-Lobular carcinoma in situ (LCIS)
Ductal carcinoma in situ (DCIS)
-Increased detection with mammogram screenings
-No way to determine if this will progress into invasive carcinoma, but it is a possible precursor
-DCIS cells lack the biologic capacity to metastasize
Lobular carcinoma in situ (LCIS)
-Abnormal cell growth occurs in the milk-producing glands
-Can increase risk of developing a separate breast cancer later
-Managed with observation
-When other risk factors exist, prophylactic treatment (tamoxifen, raloxifene, or mastectomy) can be considered: cancer originates in the mammary ducts and grows in the epithelial cells lining the ducts.
Invasive breast cancer types
-Invasive ductal carcinoma
-Inflammatory breast cancer (IBC)
Invasive ductal carcinoma
-Originates in mammary ducts and break through wall of ducts into surrounding tissue
-Once invasive the cancer grows into the tissue around it in a irregular pattern.
-Lump is irregular, poorly defined mass.
-Fibrosis develops around the cancer
-Results in shortened Cooper ligaments and dimpling in the skin
-Peau d’orange - edematous thickening of the skin.
Inflammatory breast cancer
-Diffuse erythema, swelling, and breast pain
-Seldom presents as a lump and might not be present on a mammogram
Triple negative breast cancer (TNBC)
-Lacks expression of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2).
-Grows rapidly
-Often found in with with BRCA mutation who are premenopausal
-African American women at higher risk for this type of breast cancer than other races
Breast cancer health promotion
-Foods with antioxidants and phytoestrogens are recommended for consumption (soy, whole grains, fruits and vegetables)
-Encourage mammogram screening based on scheduled recommendations
-Maintain healthy weight
-Engage in regular physical exercise
-Minimize alcohol intake
-Avoid hormone replacement therapy
Risk factors of breast cancer
-High genetic risk
-Inherited mutations of BRCA1 and BRCA2
-History of previous breast cancer
-Early age at diagnosis
-Female sex assigned at birth (less than 1% of males (sex assigned at birth) develop breast cancer)
-First-degree relative who has breast cancer
-Females (sex assigned at birth)
-Early menarche
-Late menopause
-Nulliparity or first pregnancy after age 30
-Hormone replacement therapy or hormonal contraceptives
-BMI greater than 30
-Excessive alcohol intake (possibly related to folic acid depletion)
Breast cancer physical assessment findings
-Skin changes (peau d’orange)
-Dimpling
-Breast tumors (usually small, irregularly shaped, firm, nontender, and nonmobile)
-Increased vascularity, erythema
-Nipple discharge
-Nipple retraction or ulceration
-Enlarged lymph nodes
-Male clients (sex assigned at birth) often report a mass around the areola that is hard and painless, nipple inversion, ulceration or swelling of the chest. Lymphedema and gynecomastia might be present.
Breast cancer laboratory assessment
-Genetic Testing
-BRCA1 & BRCA 2
-HER2
Breast cancer imaging assessment
-Mammography & Tomosynthesis (3D Mammography)
-Ultrasonography, MRI, CT scan, and Xray
-Nuclear imaging: breast-specific gamma
-Positron Emission Mammography (PEM) – type of PET scan
Stereotactic biopsy
Nonsurgical biopsy where affected tissue is visualized via client lying prone with mammogram machine underneath
Nonsurgical breast cancer management
-Symptoms: pain, nausea/vomiting, hot flashes, anxiety, depression, and fatigue
-Complementary and integrative health
-Prayer, guided imagery, massage, vitamins, cancer diets, herbal therapy
-Hormone Therapy
-Most effective in cancer cells with estrogen or progesterone
-Ovarian Ablation
-Selective estrogen receptor modulators
-Chemotherapy
-Radiation
Breast conserving surgery
-Lumpectomy or partial mastectomy to negative margins
-Drains may be placed, and radiation therapy typically follows
-Cosmetic surgery may not be needed
Total simple mastectomy
-Removal of the whole breast
-Indicated – multicentric disease, inability to have radiation, presence of a large tumor, genetic testing, and patient preference
Modified radical mastectomy
-Breast tissue, lymph nodes, and sometimes underlying chest wall tissue
-Drains placed
-Reconstruction may be performed at the time of surgery
Nursing considerations for breast cancer surgical management
-Have the client sit with the head of the bed elevated 30° when awake and support their arm on a pillow. Lying on the unaffected side can relieve pain.
-Have the client wear a sling while ambulating (to support arm).
-Avoid administering injections, taking blood pressure, or obtaining blood from the client’s affected arm. Place a sign above the client’s bed regarding these precautions. Emphasize the importance of a well-fitted breast prosthesis for a client who had a mastectomy.
-Provide emotional support to the client and family.
-Encourage the client to express feelings related to perception of sexuality and body image.
-Monitor surgical drains, which can be used with lumpectomy and modified radical mastectomy surgeries.
Client education for breast cancer surgery
-Care for the incision and drainage tubes. (Drains are usually left in for 1 to 3 weeks.)
-Avoid placing the arm on the surgical side in a dependent position. This position will interfere with wound healing.
-Perform early arm and hand exercises (squeezing a rubber ball, elbow flexion and extension, and hand-wall climbing) to prevent lymphedema and to regain full range of motion.
-Do not to wear constrictive clothing and avoid cuts and injuries to the affected arm.
-Conduct BSE
-Report numbness, pain, heaviness, or impaired motor function of the affected arm to the surgeon
-Discuss breast reconstruction alternatives with the surgeon
-Genetic counseling for clients who test positive for the BRCA1/BRCA2 genetic mutation includes recommendation of bilateral mastectomy and oophorectomy to prevent cancer occurrence. Clients who do not choose this option should have early, frequent, thorough screening for breast and ovarian cancer
-Community resources are available for emotional support, particularly regarding changes in body image.
-Discuss concerns about sexuality or sexual functioning following surgery. If sexual intimacy is desired, planning to engage in sexual activity when feeling less tired can be helpful, or using physical closeness to promote intimacy during times of fatigue
Breast reconstruction
-Reconstruction can begin during the original breast removal procedure or after some healing has occurred.
-A tissue expander (a saline-filled implant that has a port through which additional saline can be injected, gradually expanding the tissue prior to permanent implant) is often placed during the original procedure.
-Saline or silicone implants are used for permanent placement.
-Autologous flaps can also be used for reconstruction.
-Nipple reconstruction can be done using tissue from the labia, abdomen, or inner thigh
Types of skin cancer
-Basal cell
-Squamous cell melanoma
Risk factors for skin cancer
-Ultraviolet radiation
-Non-Hispanic white
-Family history
-Advanced age
-Moles
-Immunosuppression
Squamous cell cancer (epidermis)
Initially appears as a rough, scaly lesion with central ulceration and crusting
Bleeding (possible)
Usually present on sun-exposed areas
Course: Localized; can metastasize
Basal cell cancer (basal epidermis or nearby dermal cells)
-Open lesion that does not heal within 4 weeks
-Small, waxy nodule with superficial blood vessels, well-defined borders
-Erythema and ulcerations
-Usually present on sun-exposed areas
-Course: Invades local structures (nerves, bone, cartilage, lymphatic and vascular tissue); rarely metastatic but high rate of recurrence
Malignant melanoma (cancer of melanocytes)
-ABCDE System
-Irregular shape and borders with multiple colors
-New moles or change in an existing mole (can occur in intestines or any other body structure that contains pigment cells)
-Itching, cracks, ulcerations, or bleeding (possible)
-Common on upper back and lower legs, and on palms and soles for clients who have dark skin
-Course: Rapid invasion and metastasis with high morbidity and mortality
Skin cancer testing and diagnostics
-Biopsy (punch, shave, or excisional)
-Expected findings: Cancerous cells
-Client Education
-Monitor for infection.
-Conduct wound care, including care of sutures (punch, excisional biopsy).
-Lymph node biopsy/dissection
-Expected findings: Tissue examined microscopically for the spread of cancer
-Nursing actions
-Monitor site of lymph node biopsy or removal for bleeding or infection.
-If melanoma is diagnosed, blood tests are prescribed (CBC, CMP, liver) to check for organ involvement.
Skin cancer therapy and treatment
-Chemotherapy
-Targeted therapy
-Biotherapy – Monoclonal antibody therapy
-Radiation
-Cryosurgery
-Curettage and electrodessication
-Surgery
-Excision
-Mohs Surgery
Leukemias
-Cancers within the bone marrow that causes an increase production of immature WBCs.
-WBCs invade and destroy bone marrow
-Lymphocytic or myelogenous
ALL
-Occurs most frequently in children. Various factors influence the prognosis for children, but the 5-year survival rate is approximately 91% (age at diagnosis, gender, cell type involved); 68% survival rate of children and adults combined.
AML
-Most common leukemia among adults; prognosis is poor. The 5-year survival rate is 26%
CLL
Most cases involve people older than 50 years of age. This is the most common adult leukemia.
CML
Most prevalent after age 50 years. The disease is uncommon in children. Three phases: chronic (slow growing with mild manifestations); accelerated (more rapid growing with severe manifestations and failure to respond to therapy); and blast (very aggressive with metastasis to organs)
Lymphomas
-cancers of lymphocyte cells
-The lymphocyte cells overgrow and multiply and causes tumors within the lymph nodes (which produce antibodies and fight infection)
-Lymphomas can metastasize to almost any organ
Hodgkin’s lymphoma
-Peaks in two age groups: teens and young adults; adults in their 50s and 60s
-Possible causes include viral infections and exposure to chemical agents
-Typically starts in a single node or chain of nodes that contain the Reed-Sternberg cell. HL spreads predictably from one group of lymph nodes to the next
-One of the most treatable types of cancer with a survival rate of 86% at 5 years
Non-Hodgkin’s Lymphoma
-More common in males (sex assigned at birth) and older adults
-Possible causes include viral infections and autoimmune disease
-There is an increased incidence in clients exposed to pesticides, insecticides, and dust
Leukemia and lymphoma
-Immunosuppression
-Exposure to chemotherapy agents
-Genetic
-Ionizing radiation
-Viral infections (Epstein-Barr, HIV)
Acute leukemia S/S
-Bone Pain
-Joint Swelling
-Enlarged Liver and spleen
-Weight loss
-Fever
-Poor Wound Healing
-Pallor, fatigue, tachycardia, DOE
-Ecchymosis, hematuria, bleeding gums
-Headaches, behavior changes, and decreased attention
Hodgkin’s and Non-Hodgkin’s lymphoma S/S
-Lymphadenopathy – typically in the neck
-Fever, night sweats, unplanned weight loss, fatigue, and infections
-Abdominal fullness or prolonged swelling of lymph nodes