Looks like no one added any tags here yet for you.
clinical presentation of viral hepatitis
symptomatic
jaundice - build up of bilirubin
fever
malaise/flu like illness
dark urine - bilirubin
pale greasy stools - need to absorb fats
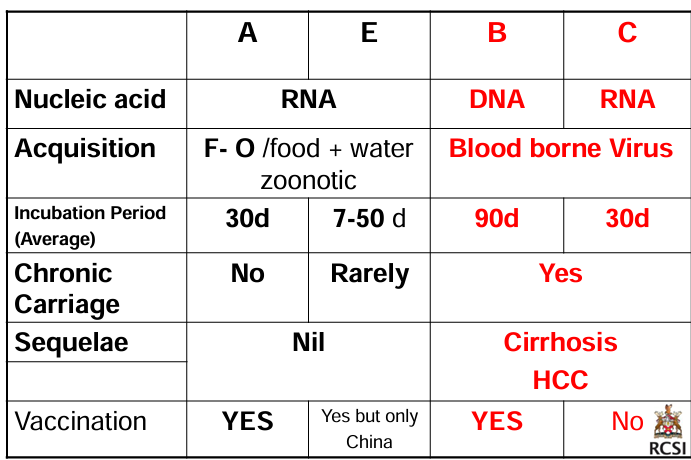
summary of hepatitis viruses
hepatitis D
small enveloped RNA virus
needs HBV to replicate so you cant have it unless you have hepatitis b - coinfection or superinfection, worse prognosis
transmission route as HBV but highest risk is bloodborne e.g. shared needles IVDU rather than sexual
prevention, treatment and management of Hepatitis A
immunization: inactivated (not live) vaccine, passive immunization indicated in those with no history of HepA (within 2 weeks of exposure)
prevention: avoiding risk factors e.g. contaminated food, water in endemic areas
prevention, treatment and management of Hepatitis E
immunization: only in China
antivirals: Ribavirin indicated in transplant patients, reduce immunosuppression also
prevention: avoiding risk factors (as above)
prevention, treatment and management of hepatitis B
varies from low to high prevalence
immunization: of cloned surface antigen (HBsAg), three shots required, requires antibody titer monitoring, booster in 10% needed, High risk groups e.g. HCWs
prevention: avoiding risk factors e.g. clean needles, condoms. Patient education
antivirals: role limited as cant eradicate - interferon alpha
patients are also monitored for cancer and ultimately may need transplant
prevention, treatment and management of Hepatitis C
immunization: none
prevention: avoiding risk factors e.g. clean needles, condoms. Patient education
antivirals: always changing - interferon combined with Ribavirin antiviral. Previous mainstay of treatment 6-12 months
Measles
measles is an RNA virus with 1 stereotype, a member of the genus morbillivirus
humans, the only natural host
measles transmitted by direct contact with infectious droplets or less commonly, by the airborne speed
measles clinical features
initial viraemia with increases temperature (39 degrees)
miserable child, sore eyes, Koplik spots
rash: 2-4 days after prodo,e or 14 days after exposure, becomes confluent, begins on face and head, persists for 5-6 days and fades in the order of its appearance
lab diagnosis involving PCR
Koplik spota
minute bluish-white spots on an erythematous base of the buccal mucosa
resembling salt crystals
complications of measles
morbidity is approx. 10% of cases
measles associated pneumonia
involvement of CNS resulting in encephalitis - can have neurological sequalae, fatality rates increase
mumps epidemiology
transmission - respiratory droplets
temporal pattern - peak in late winter/spring
incubation period - 16-18 days
communicability - 3 days before to 4 days after onset of illness
mumps clinical features
non-specific prodrome of low-grade fever, headache, malaise, myalgias
Parotitis (swelling of partoid gland) in 30%-40%
up to 20% of infections are asymptomatic
may present as lowers respiratory illness, particularly in pre-school childeren
lab diagnosis-PCR
complications of mumps
CNS involvement
orchitis
pancreatitis
deafness
death
Rubella clinical features
prodrome of low grade fever
lymphadenopathy in second week
maculopapular rash 14-17 days after exposure
rubella epidemiology
transmission - respiratory
temporal pattern - peak in late winter and spring
incubation period - 14-23 days
communicability - 7 days before to 5-7 days after rash onset
Rubella complications
arthralgia and arthritis (mainly adult females)
post-infectious encephalitis
hemorrhagic manifestations
conjunctivitis
orchitis
congenital rubella syndrome
prevention and management of measles, mumps and rubella
prevention
measles: single room isolation, with air borne precautions as highly transmissible
mumps and rubella: droplet precautions
vaccination
live MMR vaccine highly protective against measles
in childhood schedule of vaccinations
contradicted in
patients that experienced allergic reaction to previous does noted
pregnant women
immunosuppressed or immunocompromised
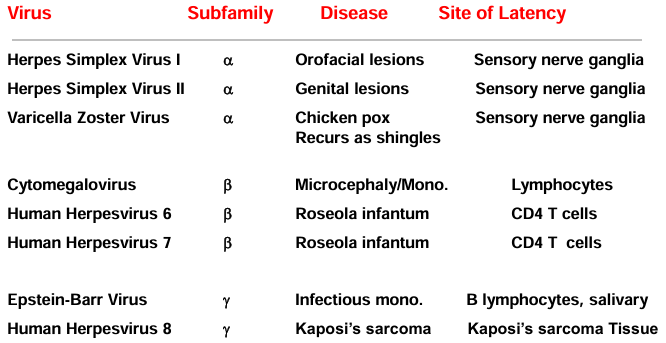
herpes viruses - classification
1. Herpes simplex virus, type 1 (HSV1)
2. Herpes simplex virus, type 2 (HSV2)
3. Varicella zoster virus (VZV)
4. Cytomegalovirus (CMV)
5. Epstein Barr virus (EBV)
6.Human herpes virus 6 (HHV 6)
7.Human herpes virus 7 (HHV 7)
8.Human herpes virus 8 (HHV 8)
herpes basic features
latency characteristic
re-activation and recurrent infections precipitated by immunosuppression, stress and other infections
HSV and VZV in nerve cells e.g. trigeminal
EBV and CMV in lymphocytes
large enveloped double standard DNA viruses
DNA core surrounded by icosahedral capsid
enclose by glycoprotein-containing envelope
herpes viruses genome encode enzymes e.g. DNA polymerase that promotes viral DNA replication
some genes homologous with human chromosome
DNA replication and assembly of capsid; nucleus
virus released by exocytosis or lysis of cell
can cause: lytic, latent or immortalizing (EBV) infections
huma hyperviruses
herpes simple virus 1
vesicular lesions
painful and filled with white fluid
the lesions ulcerate rapidly
associated with painful local lymphadenopathy
primary herpes
fever, malaise, myalgia, painful local lymphadenopathy; vesicular lesions can be widely distributed
recurrent herpes
localized lesions typically at the mucutaneous junction. recurrent episodes are typically less severe than the primary episode