Exam 3
1/133
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
134 Terms
Drug approval steps
preclinical testing
Investigational New Drug Application (NED)
Phase 1
Phase 2
Phase 3
Phase 1
In Phase 1, the drug is tested in a small group of healthy volunteers to evaluate its safety, determine a safe dosage range, and identify side effects. (20-80 people)
Pharmacokinetics = 2nd goal
only 5% of drugs move end up being approved
Phase 2
In Phase 2, the drug is tested in a larger group of people (tens to hundreds of people) who have the condition it aims to treat. This phase focuses on assessing the drug's effectiveness and further evaluating its safety.
phase 3
In Phase 3, the drug is tested in a large group of patients (hundreds to thousands) to confirm its effectiveness, monitor side effects, and compare it to commonly used treatments. This phase provides a more comprehensive understanding of the drug's benefits and risks.
Note that participants are healthier than in real life.
Drug Generics
Produced/marketed once a drug’s patent has ended.
How do drug companies attempt to prevent generics
“pay to delay”
patent infringement suits
Product hopping
Product Hopping
A strategy used by brand-name drug manufacturers to change or reformulate a drug shortly before its patent expires, (includes altering dosage, formulation, routes of administration, or dosing schedule) incentivizing consumers to switch to the new version, thereby delaying generic competition.
Components of stress
stressful expirenceexperience
processing
adaptation
Components of anxiety
fear or worry of future
increase muscle tension
restfulness
impaired concentration
increased irritability
activation of autonomic nervous system aka “fight-or-flight”
steroids: cycling pattern
A method used by bodybuilders or athletes where they alternate between periods of steroid use ("cycles") and periods of abstaining to minimize side effects/tolerance and maintain gains.
typically 6-12 weeks long between cycles.
cycling + pyramiding
is a technique used in steroid use where athletes gradually increase the dose (pyramiding) during a cycle before tapering off to prevent side effects.
aids in reducing possible withdrawal.
Metabolic tolerance
is the body's reduced response to a drug or substance after repeated use, often resulting in the need for higher doses to achieve the same effect.
There is an increase in p450 liver microsomal enzymes that metabolize alcohol
Cross-tolerance
is a phenomenon where tolerance to one substance leads to a reduced response to another pharmacologically similar substance.
ie> due to upregulation of p450 in the livers of smokers —> they can break caffeine down faster.
Cross-tolerance can be @ the receptor level: GABAA
Pharmacodynamic tolerance
neurons adapt to the continued presence of drugs by making compensatory changes in cell function
All addictive drugs BLANK dopamine levels in the BLANK
increase, nucleus accumbens
What type of information do glutamatergic neurons carry, and where do they originate? (addiction lecture)
sensory motor information from cerebral cortex
What type of information do dopaminergic neurons carry, and where do they originate? (addiction lecture)
reward related information, from ventral tegmental area
What is the role of the Nucleus Accumbens (NAc) in this process?
The Nucleus Accumbens plays a crucial role in the reward circuitry of the brain, integrating signals related to pleasure and reinforcement from various areas and facilitating motivated behavior.
What is the significance of the co-incidence of glutamate and dopamine signals?
It strengthens the synaptic connection between the glutamatergic input (cue or action) and the NAc neuron, which is a cellular mechanism of associative learning.
Dopamine release serves as a prediction error signal
burst of dopamine signifies a reward that hasn’t been predicted
When monkey learns cues that predict a reward, DA release begins with the cue in expectation of reward and ceases once reward is presented
if reward fails to occur, DA neurons cease firing, generating a decrease in DA levels that correlates with the time when the expected reward did not come.
Once environmental cues for rewards are learned, DA-ergic neurons fire back to baseline level.
What makes addictive drugs differ in reward pathways/DA
They also cause a DA release, to the brain interprets them as “better than expected” which maximizes drug seeking.
3 key factors of relapse
delivering a small dose
subjecting subject to stress
environmental cues previously paired with the drug
Pharmacokinetics of Methamphetamine
Liver metabolism:
chief metabolite: amphetamine
both are active
peak plasma concentrations at 3-6hrs (oral)
half life is approx. 12 hours
When taken via IV or smoked —> an initial rush followed by euphoria
Mechanisms of action of amphetamines
causes several transporters for NTs to reverse (different than blocking as it causes actual release into synaptic cleft)
DA, 5-HT, and NE spill into synapse
Also blocks MAO, so more DA available for packing into vesicles
GHB PD/PK
usually sold as a solution in water
is rapidly absorbed from the GI tract
readily crosses the BBB
Low doses produce an alcohol-like experience
mild euphoria
relaxation
social disinhibition
Higher doses of GHB? Overdosing
lethargy
ataxia
slurred speech
dizziness
nausea
vomiting
ODing
respiratory depression
potential for seizures
Receptor target for GHB
likely some action through GABAb
metabotropic GABA receptor (gpcr)
tendency to inhibit signaling in neurons
action is often presynaptic- inhibits NT release
GABAb knockoutmich have high affinity GHB binding sites but don’t respond to GHB treatment —> most effects of GHB are blocked by GABAb antagonists
Inhalants: Behavioral and neural effects:
CNS depressant
is best explained by the effects on ionotropic receptors —> enhance function of inhibitory GABAa receptors
Inhibit the activity of excitatory NMDA glutamate and nicotinic cholinergic receptors
Inhalants reduce CNS excitability and cause behavioral impairment in much the same way as alcohol.
Binge eating disorder and Lisdexamfetamine
vyvanse
increases monoamine NTs in the synaptic cleft
via inhibiting reuptake, MAO, and disrupting vesicular release
ghrelin: production site and effect (relevant for feeding)
stomach and neurons in the hypothalamus
appetite
Anadamide: production site and effect (relevant for feeding)
small intestine
appetite
Insulin: production site and effect (relevant for feeding)
pancreas
satity & glycogen/lipid storage
leptin: production site and effect (relevant for feeding)
adipose tissue (long term) & Stomach (short term)
satiety
Regulates the amount of fat stored in the body
reduced in sleep deprivation
CCK: production site and effect (relevant for feeding)
produced in the small intestine
stimulates digestion ( release of digestive enzymes from exocrine pancreas, bile from gallbladder, and H+ from pariertal cells in stomach) and promotes satiety
PYY: production site and effect (relevant for feeding)
produced in the intestine (ileum and colon)
promotes satiety
Vagal mechanism of satiety
afferent signals in the vagus conveyed to the brain function to limit meal size
information from stretch receptors in the stomach wall
sensors in the portal blood vessels for
cck
glucose
osmolality
pH
Bilateral lesions placed in the region of the ventro____ hypothalamus INCREASE appetite
medial
Bilateral lesions placed in the region of the ventro____ hypothalamus DECREASE appetite
lateral
Leptin infused in the brain ventricles of insulin-deficient diabetic animals dose WHAT to blood glucose
normalizes blood glucose
Glucose transporters and its location
GLUT-1: Erythrocytes and BBB
GLUT-2: beta cells, renal tubular cells, liver, and intestinal epithelial cells
GLUT-3: Neurons and placenta
GLUT-4: striated muscle and adipose tissue, aka INSULIN REGULATED GLUCOSE
Types of herbal remedies
Infusions: Hot water extracts of herbs
Tinctures: 100% alcoholic extracts of herbs
elixirs: alcoholic extracts of herbs (12-38%)
syrups: extracts of herbs with syrup or honey
Concentrations of “active ingredients” in herbs very depending on
geographic location: soil, climate, UV exposure, and plant comp.
time of harvest: ripeness
enhancer use: pesticides, herbicides, and fertilizers (organic vs. natural vs conventional)
harvesting method
storage/shipping conditions: shelf life
Cocaine metabolism:
Metabolized by butyrylcholinesterase through hydrolysis, liver cholinestrases, and liver cytochrome p450 34A
using cocaine with alcohol can lead up to a 30% increase in cociain levels in the blood —> half life is 1 h in the plasma
liver cytochrome p450 34A
Inhibited by grapefruit juice
Substrates include acetaminophen, codeine, cyclosporin, diazepam, erythromycin, and chloroquine
6 common adverse effects of cocaine in pregnancy use
Common Adverse Effect of Cocaine use in Pregnancy |
1- Restricts blood flow to the uterus, cause fetal hypoxia. |
2- Uterine contractions, CNS infarction, Heart defects. |
3- Persistent neonatal arterial hypertension. |
4- Decreased neonatal weight and size (¯ head circumference). |
5- Sudden infant death syndrome, Intellectual disability. |
6- Babies may be irritable at birth and exhibit symptoms such as: tremor, hypertension, abnormal reflexes, tachypnea, autonomic instability, vomiting, diarrhea, seizures and poor feeding. |
True or false: Neuroinflammation is ALWAYS a negative thing
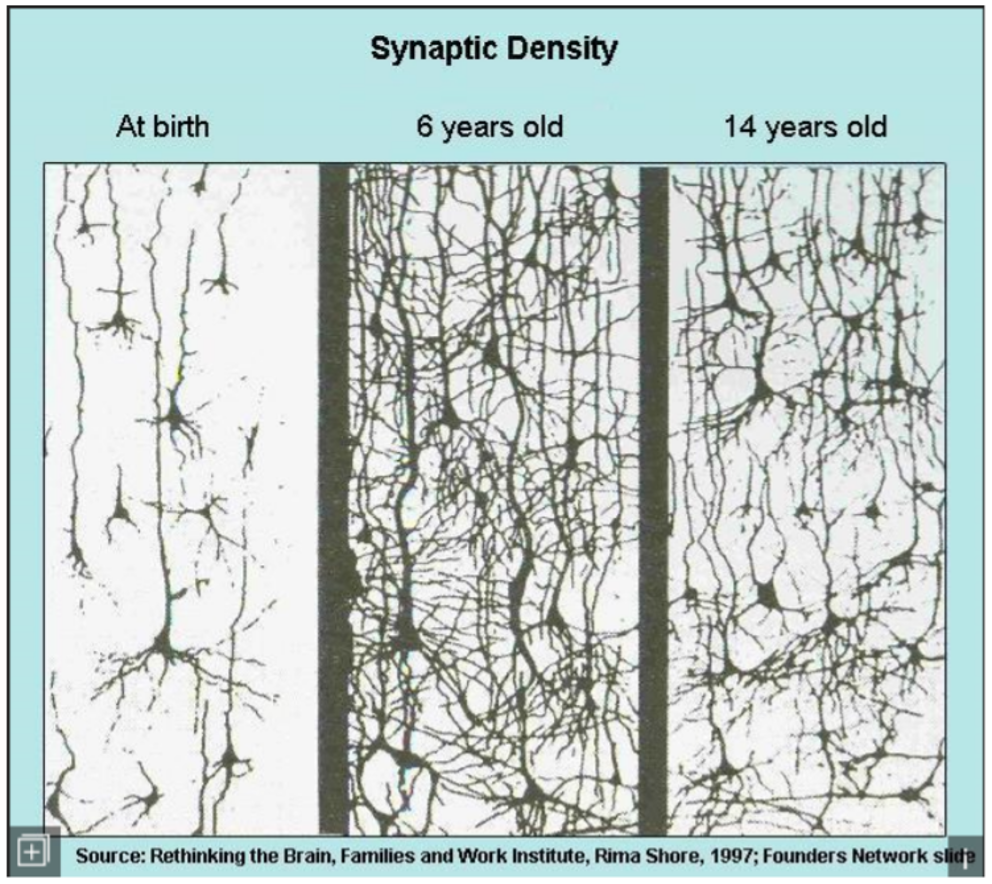
FALSE: example: synaptic pruning
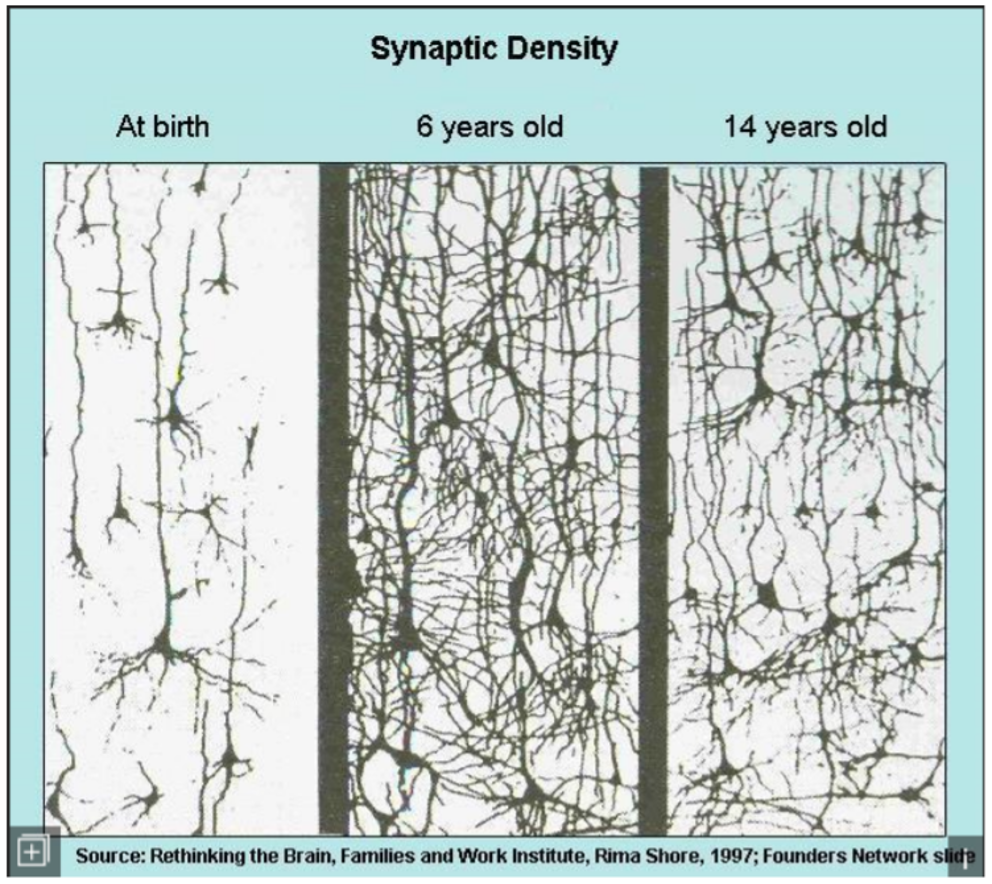
synaptic pruning
is a natural process in the brain that removes excess neurons and synapses, allowing for more efficient neural connections.
TBI mouse models: what reduces inflammation and improves functional recovery
Anti-inflammatory treatments minocycline can help reduce inflammation and promote recovery in TBI mouse models.
Borrelia Burgdorferi aka Lyme disease
bacterial infection
red rash, fever, headaches, tiredness
Later can lead to —> loss of ability to move one or both sides of the face, joint pains, severe headaches with neck stiffness, or heart palpitations stiffness
Treatments: antibiotics- first choice, usually doxycycline
Treatment for brain eating amoebas
anti fungal drug: amphotericin b
binds to cell membrane’s sterols of the pathogen
cell disruption and death
fatality is still greater than 95% even with treatment.
Multiple sclerosis
autoimmune disease
presence of T cells that recognize oligodendrocyte myeline specific antigens
activated t-cells cross the bbb and secrete pro-inflamatory cytokines, leading to demyelination and neurodegeneration in the central nervous system.
Anoctamin 2 and MS
protein in oligodendrocytes that is involved in myelin regulation and may contribute to nerve repair processes in multiple sclerosis.
is the target in MSand is implicated in disrupting normal myelin function.
Disease modifying treatments of MS focus on…
Reducing frequency and severity of relapses and accumulation of lesions
Interferon beta (1a and 1b) in MS
Increases suppressor T cell function
these t cells maintain tolerance to self antigens and decrease the self attack of MS
Drug treatment of MS: Copaxone (glatiramer acetate)
synthetic protein
random combination of four amino acids that are found in myelin
May work as acting as a decoy target for the immune system
Drug treatment of MS: Novantrone (mitoxantrone)
chemotherapy
Suppresses components of the immune system like T & b cells and macrophages
Drug treatment of MS: Tysabri (natalizumab)
monoclonal antibody (lab-produced protien designed to mimic the function of natural antibodies) against cell adhesion molecule alpha4-intergrin
hinders movement of t cells across the bbb
the side effects makes this reserved as a second line drug
Drug treatment of MS: Gilenya (fingolimod)
sphingosine 1-phosphate receptor modulator
GPCR
causes retention of lymphocytes ( a kind of white blood cell) in lymph nodes
prevents their entry to the CNS
SMA: common signs and symptoms
movement difficulties (walking, sitting up, carrying objects)
Problems with breathing
Problems with swallowing
Flaccidity
atrophy
hypotonia
fasciculations
hyporeflexia
4 types of SMA:
Type 1: onset before 6 months, no sitting
Type 2: onset 6-18 months, sitting but no walking
Type 3: onset after 12 months, walking
Type 4: onset after 30 years, normal
What causes SMA?
Mutation in the survivor motor neuron gene 1.
SMN2 plays a secondary role in symptom severity.
Purpose of SMN1 gene
creates a protein that supports the motor neurons.
SMN genes in healthy individuals vs people with SMA
SMA: both copies of SMN1 are either missing or mutated
healthy: have 2 copies of SMN1 and about 1-2 copies of SMN2 in each cell
SMN genes and severity of SMA
most severe types of SMA have only one copy of SMN2 while less severe cases have 4+ copies of SMN2 in each cell.
More copies of SMN2 compensate for the loss of SMN1’s protein making power.
Spinraza
antisense oligonucleotides
only for 5q SMA
targets the SMN2 gene and enables it to produce more functional, full length SMN proteins.
Cannot cross BBB so it is directly injected into the CSF via lumbar puncture
Risdiplam
small molecule drug that targets the “back up” SMN2 to produce more SMN protein
only used to treat 5q SMA —> can be taken orally but oral solution can only be stored at room temp for more than a total of 120 hours
is incompatible with reproductive function
Zolgensma
gene therapy that delivers a working copy of the SMN1 gene to motor neurons
made from parts of AAV9 (cannot make copies of its self so it does not spread from person to person)
Different Variants of ALS
SOD1, C9ORF72, TARDBP, and FUS
SOD1 gene:
implicated in approx 20% of familial ALS
SOD1 serves as an antioxidant
may protect against superoxide produced by mitochondria
110 SOD1 mutations linked to ALS
C9ORF72 gene:
present in 40% of familial and 10% of sporadic ALS
abnormal expansion of a GGGGCC hexanucleotide repeat is common genetic cause of ALS —> loss of function of this gene
TARDBP and FUS
DNA binding/repair/regulation
Mechanisms that contribute to cell death:
Excitotoxicity from excessive glutamate signaling
Aggregation of proteins
Breakdown of axonal transport w/ loss of neurofilament structure
Reduced production of ATP
Neuroinflammation
Triggering of cell death pathways
Primary hits of ALS
inherited or sporadic mutations in related genes
negatively affect the initial anti-inflammation phase
Secondary hits of ALS
aging
toxicity
traumatic injuries
CNS inflammation
Sets off the rapidly progressive stage marked with uncontrollable inflammation
FDA approved drug for ALS
only one!
Riluzole: presynaptic inhibitor of glutamate release —> blocks glutamate-mediated excitotoxicity
mechanism of action: blocks Na channels, reducing AP
may reduce symptoms severity
doesnt effect muscle strength
may delay the need for intubation and ventilatory support.
Edaravone
used for stroke & ALS
an antioxidant —> VERY expensive in the US (145k)
2024 study: drug was associated with SLIGHTLY slower progression, mortality rates decreased SLIGHTLY
side effects: confusion, gait disturbance, headache, eczema , and contacy dermatitis
AT-1501 (now ‘tegoprubart’)
early stage clinical trial for ALS
phase 2a trails as of 2022
Antibody against the ligand of CD40
CD40: receptor that is present on many cell types —> target seems to be macrophages
Secondary activation pathway for macrophages
Macrophages play an important role in cleaning up dead cells
But they are sources of microbicidal reactive oxygen species
Binding to ligand to cut down on immune cell activation
Tuberous Sclerosis Complex (TSC)
rare multisystem autosomal dominant genetic disease that causes noncancerous tumors to grow
brain and eyes
kidneys and heart
Liver and Lungs
Skin
Combination of symptoms: seizures, intellectual disability, developmental delay, skin abnormalities, lung disease, and kidney disease.
Treatments for TSC
mTOR inhibitors: slows down tumor growth and prevent complications
i.e., Everolimus: selective for mTORC1 protein complex —> mRNA translation is hindered so tumor growth is inhibited
Anti seizure medications: control seizures
medications: treat skin lesions
surgeries: to remove tumors
HD symptoms:
develops between 30-50 years but they can appear as early as age 2 and as late as 80
Hallmark: uncontrollable movement of the arms, legs, head, face and upper body “chorea” aka dance
caused decline in thinking and reasoning skills
causes brain changes that lead to alterations in mood
OCD is another common symptom
HD degeneration of the brain
Striatum: key player in motor control
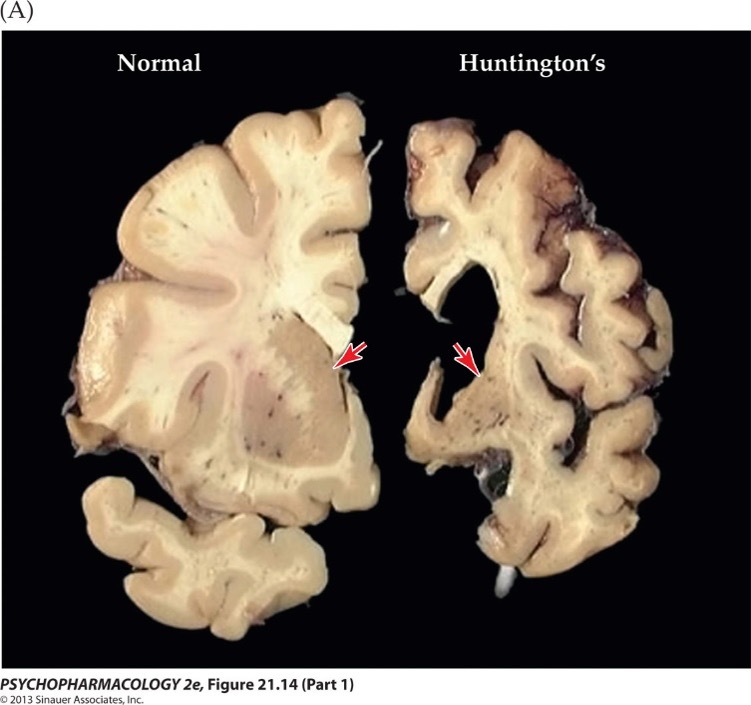
“dying back” pattern: Neuronal degeneration in HD
Affected neurons begin to exhibit signs of synaptic and axonal alterations early in the disease process:
abnormalities in the phosphorylation of axonal proteins
abnormal accumulation of membrane-bounded organelles (blue circles) in axons
Axonal degeneration steadily advances in a retrograde fashion, and nuclear/neuritic Htt aggregates (red stars) become evident
First line treatments for HD
They try to REDUCE DA-ergic signaling
Tetrabenazine:
blocks VMAT2
Prevents the uptake of catecholamines into vesicles
Monoamine levels are reduced because they are not packaged into protective vesicles
Potential side effects since depletion of monoamines can lead to increased psychological symptoms
DA antagonists may also be used to supresse unwanted movements
Anticonvulsants, anxiolytics and antidepressants are also prescribed to deal with psychological aspects of the disease
Early stages HD: the aggregates delay axonal transport resulting in…
failed delivery of GABA(A) —> hyperkinesia
In the late stage, trafficking of NMDA receptors in ___ is affected, what doe this cause?
striatal neurons —→ bradykinesia
AMT-130
Used for HD
reduce the production of normal and mutated huntingtin protein by targeting the HTT gene’s mRNA
uses AAV5 to deliver microRNA
is administered directly into the caudate nucleus and the putamen
Two-year trial update:
12 people
was shown to significantly slow the progression of the disease by a mean of 80%
Rabies
transmitted via bites —> or “inhalation” of the virus
symptoms occur within 1 week- 1 year of contact
RETROGRADE TRAVEL FROM SITE TO BRAIN
universally fatal
Post-exposure prophylaxis with vaccine is very effective when administered with first 24h post-exposure
one dose of human rabies immunoglobulin (HRIG) and four doses of rabies vaccine over a 14-day period
very $$$ (600$ after insurance in 2005 in IU health center/ or several thousands in hospital)
Peru and rabies
In 8 people in peru antibodies are found with no explanation…
We think that these people were lightly bitten during the night, but were not exposed to enough of the virus to develop a full infection
Signs and symptoms of rabies
light or partial paralysis
Hydrophobia (larynx)
anxiety
insomnia
Confusion
agitation
abnormal behavior
paranoia
terror
hallucinations
delirium
Coma
Death
Two types of HSV and what HSV is as a whole
HSV: double stranded DNA virus
HSV-1: oral infections
HSV-2: genital infection
HSV and associations
Postive status: associated with cognitive defects, bipolar, and AD
APOE-epsilon4 allele carriers are predisposed to AD once infected
HSV infection
virus enters the nerves at the site of primary infection, migrates to the cell body of the neuron and becomes inactive in the ganglion
the body produces antibodies to that particular type of HSV as a tool to prevent a 2nd infection of that type at a different site.
HSV-1: seroconversion after an oral infection prevents additional HSV-1 infections such as whitlow, genital herpes, and herpes of the eye —> seems to reduce symptoms if the person has HSV-2 later (can still be contracted)
Stages of PD
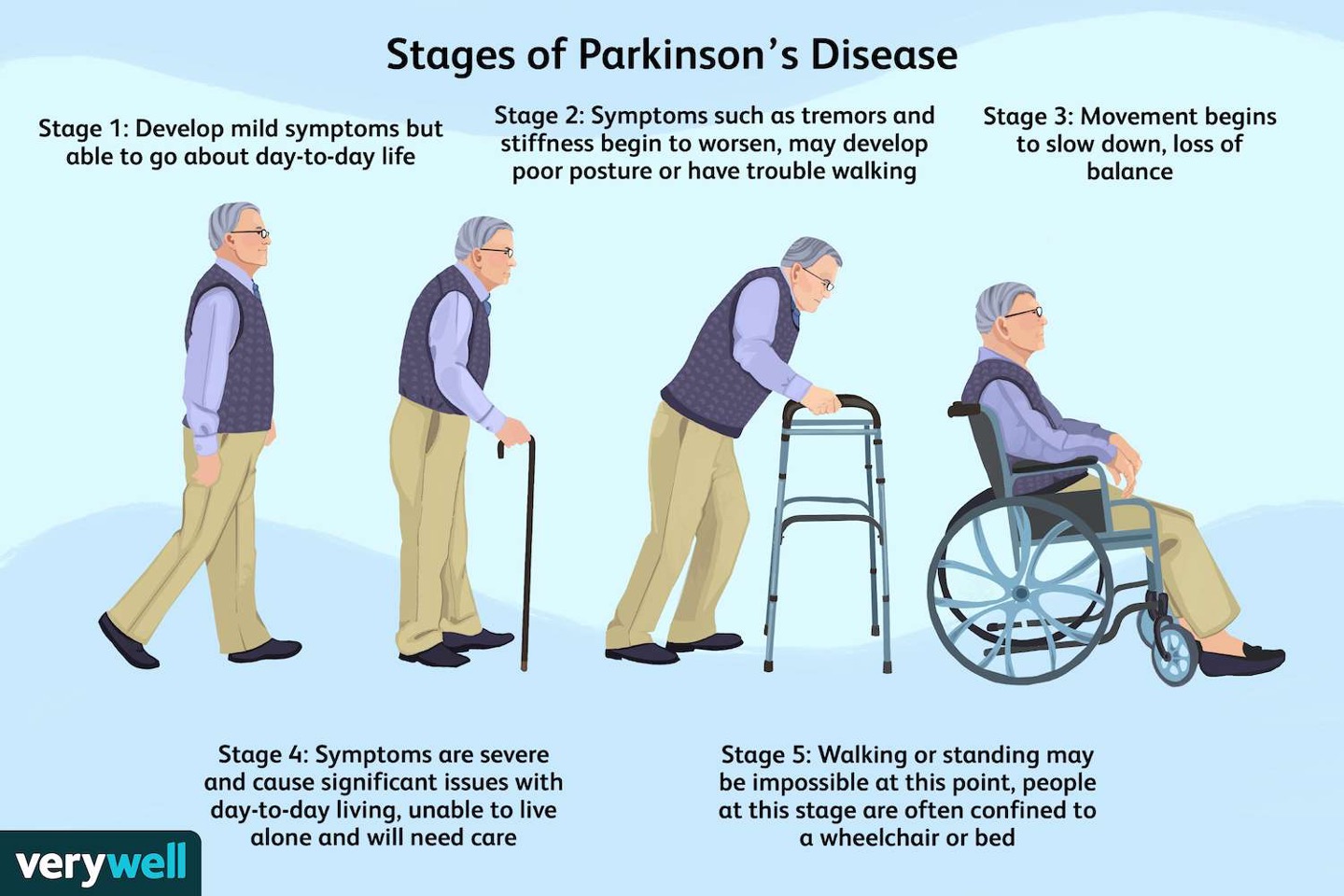
Identifiers of PD
less movement of facial muscles —> reduced facial expression = “mask like”
bradykinesia —> also results in small handwriting, decreased speaking volume and monotone speech
rigidity in the joints is another common symptoms —> shuffling gait
Key component in PD:
protien aggregation
lewy bodies consist of α-synuclein and other proteins
healthy cells: a-synuclein mediates vesicle movement at axon temrinals
lewy bodies are formed by protien misfolding and proteasomal dysfunction
they interrupt cell function and trigger apoptotic cell death
6-OHDA
neurotoxin in PD models
doesn’t cross BBB —> selective for DA neurons —> stereotaxic injections
Causes rapid apoptosis —> difficult to study disease progression of PD
lots of neuro inflammation
Abscisic acid:
phytohormone (plant hormones) found in various brain regions of several mammals
exhibits neuroprotective properties
MPTP
dopamine neurotoxin used to produce animal models of PD
formed by MAO-B
in astrocytes and 5-HT ergic neurons
transported by dopamine transporter into cells
MitoPark mouse model
mitochondrial transcription factor was inactivated in mice models
depletion in mitochondrial DNA
loss of gene transcripts
deficiency in respiratory chain
ends with cell death
Symptoms were reversed by L-dopa treatment —> doesn’t prevent cell death but replaces DA that dead neurons are no longer producing
Levodopa (L-DOPA)
metabolite of tyrosine and is the immediate precursor of DA
pathway continues to form NA and EPI
can cross BBB but not dopamine
advantage: it leaves neurons in the driver seat -→ DAergic neurons fire as before contrast to agonist