Behavioral Theories & Strategies for Promoting Exercise
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
25 Terms
exercise research in general + demographic factors
-Research has identified consistent correlates to engaging in regular exercise/PA.
-Numerous demographic factors are consistently related to the likelihood that an individual will exercise on a regular basis.
oAge, gender, socioeconomic status, education, ethnicity
-Although these factors are not amenable to intervention, they do suggest who might benefit most from the exercise intervention.
exercise research Rx: frequency and time
-Reviews of randomized trials showed that there is no difference in exercise adherence when different combinations of frequency and time are used to achieve the same total volume of PA.
*ex: everyday vs every other day for longer
-Allowing individuals to self-select frequency and time may best influence adherence to exercise interventions.
*but hard to quantify for research
exercise research Rx: intensity
-Emerging evidence suggests that any inverse relationship between intensity and adherence is not particularly strong and may be moderated by prior exercise behavior.
*ex: no dif if easy or really intense
-There is evidence that individuals with more exercise experience fare better with higher intensity programs (65%–75% HRR), whereas those adopting exercise for the first time may be better suited to, and self-select, moderate intensity programs (45%–55% HRR).
*more positive feedback
exercise research Rx: type
-There is no compelling evidence that exercise mode is related to adherence.
-Little is known about the characteristics of those that adopt and maintain resistance training and flexibility-exercise programs.
-Studies have shown comparable or greater adherence to home-based, or lifestyle, programs within certain populations, including remotely delivered compared to structured, center-based programs.
-Interventions delivered entirely or predominantly via telephone have been shown to be effective in increasing PA.; Other tech-delivered interventions hold promise for promoting PA.
*** interview patient and find out what they like to do!
theoretical foundations for understanding exercise behavior (intro + list the different models)
-Theories and models provide frameworks for understanding exercise participation.
-Many theories share a common, conscious decision-making basis focused on individual’s expectancies and values.
-People intend to engage in a behavior in which they think they can expect to succeed and have a valued, positive result.
•Social cognitive theory
•Transtheoretical model
•Health belief model
•Theory of planned behavior
•Social ecological models
Social Cognitive Theory and Self-Efficacy
-SCT: reciprocal determinism: the individual, the behavior, and the environment all interact to influence behavior.
-Self-efficacy: One’s beliefs in a capability to successfully complete a task, such as exercise.
Task self-efficacy: An individual’s belief to actually do the behavior in question.
Barriers self-efficacy: Whether an individual believes he or she can regularly exercise in the face of common barriers such as lack of time, poor weather, or feeling tired.
-The higher the sense of efficacy, the greater the effort, persistence, and resilience an individual will exhibit, especially when faced with barriers or challenges.
oSelf-efficacy is one of the most consistently found correlates of PA in adults and youth.
-Outcome expectations and expectancies, are anticipatory results of a behavior and the value places on these results.
-If specific outcomes are valued, then behavior change is more likely to occur.
-Example: An overweight adults wants to lose weight and believes that walking will help. This adult is more likely to start and maintain a walking program.
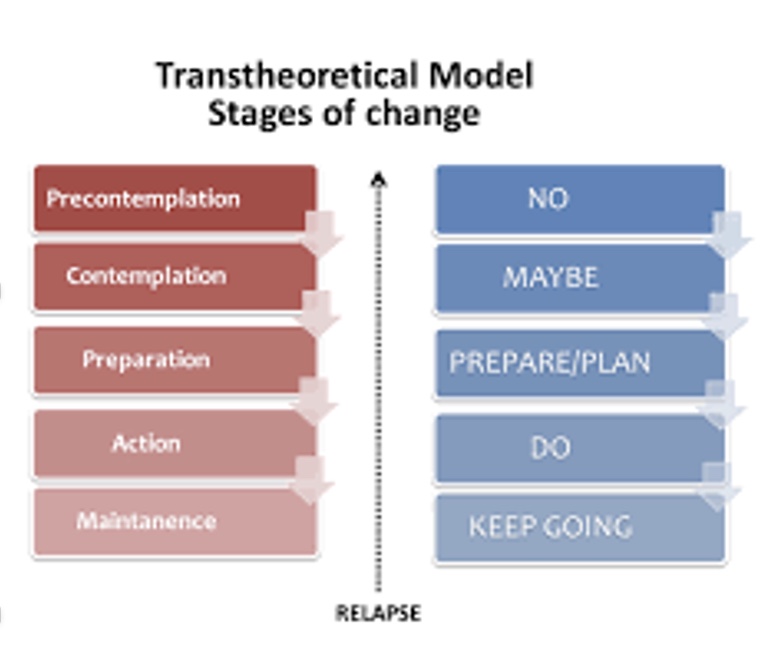
Transtheoretical Model
-TTM was developed as a framework for understanding behavior change and is one of the most popular approach for promoting exercise behavior
-The popularity of the use of stages of change from the TTM stems from the intuitive appeal that individuals are at different stages of readiness to make behavioral changes and thus require tailored interventions. (*where someone starts)
The stages of change
oPrecontemplation(no intention to be regularly active in the next 6 mo)
oContemplation (intending to be regularly active in the next 6 mo)
oPreparation (intending to be regularly active in the next 30 d) (*where start to initiative exercise Rx)
oAction(regularly active for <6 mo)
oMaintenance(regularly active for ≥6 mo)
*6 months based of ACSM 6 months and 150 minutes
Health Belief Model
-An individual’s beliefs about whether or not they are susceptible to disease
*often increases as get older
oindividual perceptions of the benefits of trying to avoid disease, influence an individual’s readiness.
-An individual needs to believe he/she is susceptible to a disease and believe that the benefits of taking action outweigh the perceived barriers.
-HBM may be most suitable for understanding and intervening with populations that are motivated to be physically active primarily for health reasons, such as cardiac rehabilitation and diabetes mellitus prevention and management.
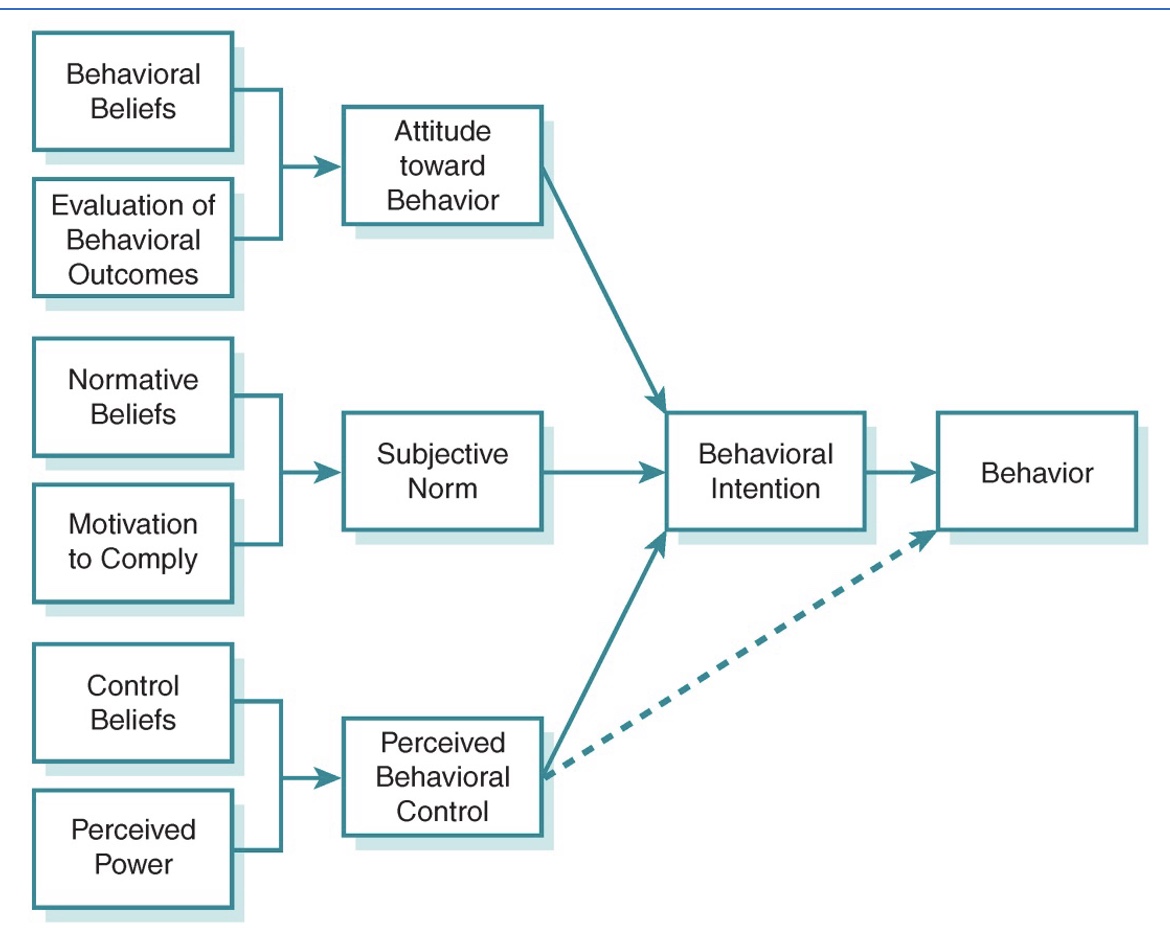
Theory of Planned Behavior
-intention to perform a behavior is the primary determinant of actual behavior.
-Intentions reflect an individual’s probability that she or he will exercise but do not always translate directly into behavior because of issues related to behavioral control.
-Attitudes are the degree to which an individual has a favorable or unfavorable evaluation of behavioral outcomes.
-Subjective norms are about whether an individual believes important people in their life value a behavior.
-Perceived behavioral control is the perceived ease or difficulty in engaging in a behavior.
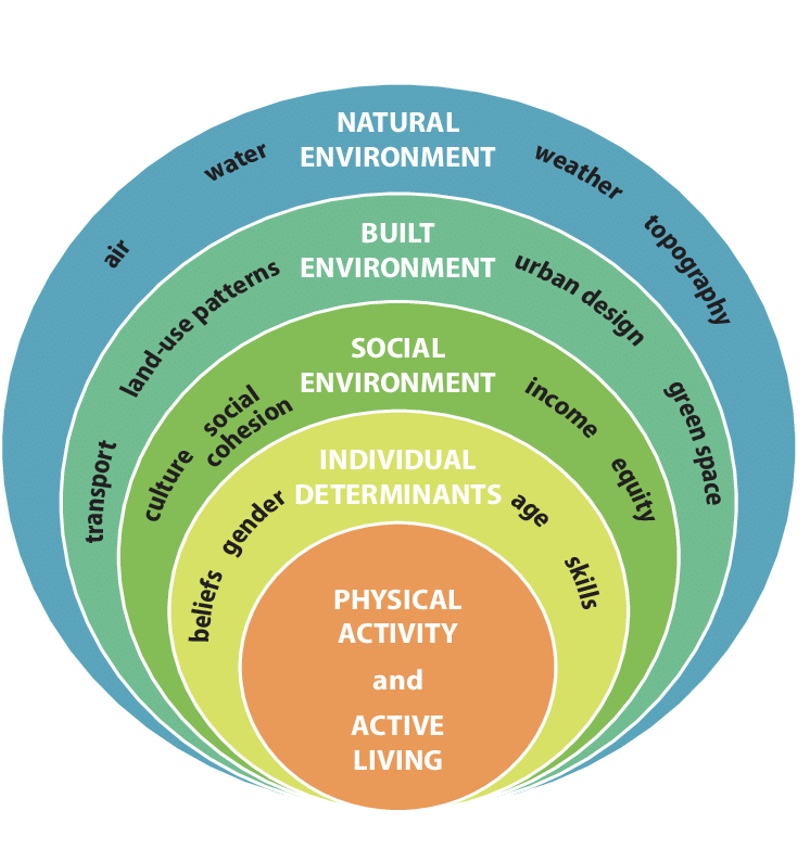
Social Ecological Models
-explicit recognition of relations between individuals and their physical environments.
-Ecological models posit that behavior results from influences at multiple levels. (multiple factors to success)
-Environmental factors influence behavior directly and indirectly through an individual’s perceptions.
-If a physical environment is not conducive to change, then the exercise intervention will not be successful.
-A key belief is that interventions are most likely to be effective when they target multiple levels
hedonic motivation
-people will tend to seek out experiences that are pleasurable and enjoyable and avoid those which bring displeasure.
*where get “no pain no gain”; displeasure common w/ exercise due to pain, injury, soreness, etc.
strategies/appraoches for increasing PA: self-efficacy and self-monitoring
-Enhancing self-efficacy
-Self-monitoring
*how view and monitor self; how make patient an active participant who has power/control
oSelf-monitoring involves observing and recording behavior and has been shown to be important in exercise behavior change.
oSelf-monitoring can be useful for tracking progress toward goals, identifying barriers to changing behavior, and as a reminder to exercise.
oSelf-monitoring is most effective when paired with other strategies, such as goal setting, as merely monitoring behavior by itself may only have limited, short-term effects.
strategies/approaches for increasing PA: SMART goals
-Specific
-Measurable
-Action-oriented
-Realistic
-Timely
+Self-determined
strategies/approaches for increasing PA: intention
*do it with a reason, then more likely successful
-May enhance the link between exercise intentions and behavior
-individual’s specific and detailed plans to exercise such as where they will exercise, when they will exercise, and with whom they will exercise
-Evidence has supported that the addition of implementation intentions improves exercise behavior outcomes beyond standard motivational interventions.
strategies/approaches for increasing PA: reinforcement
*positive feedback/encourage/reward
-Individuals should be encouraged to reward themselves for meeting behavioral goals.
-These rewards can be especially effective for initiating PA.
-Environments promoting intrinsic motivation focus on (a) providing positive feedback to increase feelings of competence, (b) acknowledging individual difficulties within the program, and (c) enhancing sense of choice and self-initiation of activities to build feelings of autonomy
*bad incentives ex: $
strategies/approaches for increasing PA: social support
-Social support can be a powerful motivator.
-Social support can come from an instructor, family members, workout partners, coworkers, neighbors, as well as exercise and other health professionals.
-Providing social support in the form of guidance is most common when working with individuals.
strategies/approaches for increasing PA: problem solving
*always going to have barriers
oProblem solving can assist individuals in identifying strategies to reduce or eliminate barriers.
oProblem solving includes (a) identify the barrier, (b) brainstorm ways to overcome the barrier, (c) select a strategy generated in brainstorming viewed as most likely to be successful, and (d) analyze how well the plan worked and revise as necessary.
oSolutions to barriers should be generated by the individual, not the exercise professional.
*common for kids to say “there is no one to exercise with me”

strategies/approaches for increasing PA: relapse prevention
*have made changes when barriers came up
-An important part of helping individuals maintain their PA levels is developing strategies to overcome setbacks.
-Relapse prevention can be implemented across all behavioral approaches.
-Relapse prevention strategies include being aware of and anticipating high-risk situations and having a plan to ensure that a lapse does not become a relapse.
-A varied exercise routine or creating new goals may prevent a relapse.
-Don’t get discouraged when missing a session; therefore, avoiding “all-or-nothing” thinking.
strategies/approaches for increasing PA: brief counseling and motivational interviewing
-Brief counseling approaches can be based on any of the theories previously discussed.
-MI explores why people aren’t active, asks open-ended questions, uses empathic responses and reflective listening skills, and recognizes that individuals may be resistant.
-MI involves exploring and resolving ambivalence about behavior change.
-MI encourages the use of “change talk.”
special populations: older adults
oOlder adults may lack knowledge about the benefits of PA or how to set up a safe and effective exercise program so health/fitness and clinical exercise professionals need to provide some initial education.
oAlthough typically viewed as beneficial, social support is not necessarily positive, especially in older adults...
oFamily and friends may exert negative influences by telling them to “take it easy” and “let me do it.”; “self-limit”
oThe implicit message is that they are too old or frail to be physically active.
oSeveral specific barriers: lack of or indifferent social support; increased social isolation; fear of falling/safety; and physical ailments. (*where movement screen can come into play)
oThe largest potential barrier to exercise: fear that exercise will cause (something worse) injury, pain, and discomfort or exacerbate existing conditions.
oOlder women (now) may have had little early-life exposure to PA .
oRecommendations include finding enjoyable activities, start low and go slow, and being aware of chronic conditions that might be present
what is similar between giving information/Rx to older kids and adults?
-not much different
-want simple and small chuncks
special populations: youth
oWhen working with children, determine if their interest is from extrinsic motivation (e.g., parents), as this typically requires tangible forms of social support (e.g., transportation, payment of fees).
oTo help them maintain exercise behavior over their lifetime, children need help shifting toward a sense of autonomy and to feel a sense of self-efficacy and behavioral control.
oIt is imperative to work toward establishing a sense of autonomy and intrinsic motivation through the creation of a supportive environment.
oFamilies and schools can both be used for creating autonomy.
special populations: individuals with obesity
oMay face weight-related barriers such as feeling being uncomfortable exercising in public.
oMay have had negative mastery experiences with exercise and will need to enhance their self-efficacy so that they will believe they can successfully exercise.
oThey may also be quite deconditioned and perceive moderate intensity exercise as challenging; keep activities fun and at a low enough intensity to promote positive PA perceptions. (*but might not see tons of change with low intensity)
oMay need help setting realistic weight loss goals and identifying appropriate levels of PA to help them reach those goals.
special populations: individuals with chronic diseases and health conditions
oConsider focusing on enhancing task self-efficacy to ensure that individuals believe that they can do what is being asked of them.
oOnce individuals possess task self-efficacy, they often face barriers specifically related to their condition, such as individuals with arthritis reporting pain, fatigue, and mobility limitations.
oBe aware of the unique barriers and fears of individuals with chronic diseases and health conditions to help assure the physical activities chosen are appropriate and foster the individuals’ self-efficacy.
-A concern when working with individuals with chronic diseases and health conditions is their ability to do the exercise both from a task self-efficacy perspective as well as in the face of the barriers presented by their condition.
oSpecial consideration should be given to ensure activities are chosen to prevent, treat, or control the disease or health condition.
oBeing aware of the unique barriers and fears of individuals with chronic diseases and health conditions can help assure the chosen physical activities are appropriate.
special populations: individuals with mental illness
*where can get biggest barriers from fear; exercise may feel similar to anxiety for some, so education
oAdults diagnosed with mental health disorders cite perceived or actual lack of resources and social support, confidence (self-efficacy), fear, motivation, and affect, in addition to side effects associated with psychiatric medications, as barriers to PA.
oExercise reduces both state and trait anxiety, depression, depressive symptoms, schizophrenia, and attention deficit hyperactivity disorder.
oIndividuals with a mental illness can benefit from help in finding personally enjoyable activities and setting small, realistic goals to offset lack of energy or motivation.
oOther recommendations include being active with others, which can improve mood and reduce sadness or anxiety, and exercising outside, which has been shown to have positive effects on mood.