patho370 Study Guide Week 6 Ch. 27,28, 29, 31 & 33
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
82 Terms
Overview of Urinary System Functions: Waste management
excreting toxins, waste stuff, and excess electrolytes
Overview of Urinary System Functions: Acid/Base balance
2 organs in the body doing it: kidneys & lungs
Overview of Urinary System Functions: Fluid balance
well-balanced overall body, total fluid
o If too much excretion of water → dehydration
o If too little excretion → edema
If something is wrong with the Glomerulus →
Filtration issue
If something is wrong with the Renal tubular system →
absorption, excretion issue
Uremic Syndrome
HIGH waste (H+, Cr, UREA) + Hemolysis (LOW RBC life span) + LOW WBC + Skin disorders (Dermatitis, Uremic Frost)
Filtration
Filters waste materials → how much? = serum creatinine, rate (GFR)
Filtration: Urine
urine → urine output = 1% of total filtration (800-2000ml)
< 400-800 ml → Oliguria
> 2000 ml → Polyuria
FOR HEALTHY PEOPLE:
UO measured in REAL TIME → 24 HRS COLLECTION
FOR ADMITTED PATIENTS:
UO measured in PREDICTION WAY → usually measured in a 3-4 hrs time window ( F.ex: for 3 hrs = 60ml → for 24 hrs =480 ml)
Why prediction on patients? we want to evaluate the patient’s kidney status → RIFLE
Intrarenal Disorders:
- Congenital
- Neoplastic
- Infectious
- Obstructive
- Glomerular
Congenital: Agenesis
no development in the fetus
o Unilateral agenesis compensatory hypertrophy of functional kidney
o Bilaterial agenesis NOT compatible with life
Congenital: Hypoplasia
some fetal kidney development
o Can lead to pediatric end-stage renal failure
o A single normal kidney can maintain normal renal function
Cystic Kidney Diseases:
Mutation of 2 genes → resulting in fluid-filled cysts → LOW urine formation and flow
Autosomal recessive forms:
in kids
Autosomal dominant types:
in adults
Cystic Kidney Diseases: Pathogenesis
massive cysts formations in kidneys → put pressure on nephron function
- LOW GFR → LOW urine output → oliguria
- LOW GFR → LOW urine sodium (U-Na) → HIGH RAAS → HIGH BP → hypertension
- Cysts can invade intra-renal capillary → hematuria
→ 3-H
Renal Cell Carcinoma:
p53 mutation, smoking, obesity, and hypertension are some risk factors
Renal Cell Carcinoma: Pathogenesis
tumor puts pressure on nephron function →
- LOW GFR → LOW urine output → oliguria
- LOW GFR → LOW urine sodium (U-Na) → HIGH RAAS → HIGH BP → hypertension
- Tumors invade intra-renal capillary → hematuria
- Palpable mass
- Staging system: I-IV
Nephroblastoma (Wilms Tumor)
Kidney cancer in children
- Hypertension
- Palpable abdominal mass → abdominal palpitation
- Hematuria
UTI:
bacterial infection either in the bladder or urethra → asymptomatic or polyuria/dysuria
- Most common bacteria is E-Coli
Pyelonephritis:
infection of renal pelvis/ parenchyma,
- CVA tenderness (classic sign)
- Fever, chills, N/V
Pyelonephritis: Treatment
antibiotics
Obstruction:
conditions that interfere with the flow of urine → Urine stasis →
- Infection
- Structural damage
- Kidney stones
Stones:
Calcium oxalate, Uric acid, Struvite, Cystine
- Most common stones: Calcium oxalate
Tumors:
Tumors from urinary & abdominal organs
- Internal
- External (from other organs)
Prostatic hypertrophy:
BPH/ Prostate cancer
Sequala of Obstruction: Complete obstruction results in
- Hydronephrosis
- Decreased GFR
- Infection
- Ischemic kidney damage because of increased intraluminal pressure → ATN

Acute Kidney Injury (AKI):
- Prerenal
- Postrenal
- Intrinsic/ Intrarenal
Prerenal:
dimmish perfusion of the kidney, MOST COMMON TYPE
If < 6 hrs → NO NEPHRON DAMAGE
If > 12 hrs → NEPHRONE DAMAGE —> INTRARENAL INJURY
- Heart failure
- Hypovolemia
- Vomiting, diarrhea
- Burns
- Drugs
- Stenosis of renal artery
Postrenal Kidney Injury:
Obstruction within the urinary collecting system
If < 6 hrs → NO NEPHRON DAMAGE
If > 12 hrs → NEPHRON DAMAGE → INTRARENAL INJURY
- Kidney stones
- Tumor
- BPH
Intrinsic/ Intrarenal Kidney Injury:
dysfunction of the nephrons
Vascular
Glomerular
Interstitial
20%
o Drugs (NSAID, Antibiotics)
o Infections
- Tubular (80%) → ATN
- Ischemia (80%)
- Nephrotoxic (contrast)
Creatinine in the urine = Creatinine Clearence
Sequala of AKI:
- LOW glomerular filtration rate (GFR) → LOW urine output
- Volume overload
- HIGH serum creatine
- Retention of nitrogenous waste products effects (BUN) → azotemia/ uremia
o Severe case: uremic syndrome
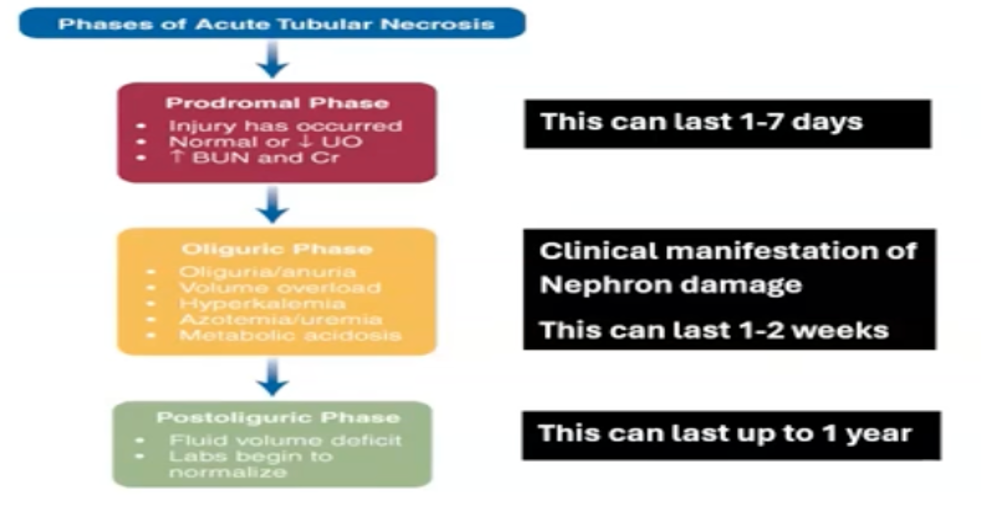
Clinical Presentation of Acute Tubular Necrosis:
Chronic Kidney Disease: Progressive/ irreversible loss of nephrons
- Decreased kidney function or kidney damage of 3 months’ duration based on blood tests, urinalysis, and imaging studies
- GFR < 60ml/minute/1.73 m2 for three months with or without indication of damage to the kidney
Chronic Kidney Disease: Risk Factors
- Diabetes
- Hypertension
- Recurrent pyelonephritis
- Glomerulonephritis
- Polycystic kidney disease
Progressive process (irreversible)
Chronic kidney disease (CKD) → Chronic renal failure (CFR) → end-stage renal disease (ESRD → dialysis
Hypertension and Cardiovascular disease
o Hypervolemia
o Increased RAAS and SNS activity
Uremic Syndrome
o Retention of metabolic wastes
o Pruritus/ Dermatitis/ Uremic frost
Metabolic acidosis
o Retention of acidic waste products
o Hyperkalemia
Electrolyte imbalances
o Retention of electrolytes potassium, phosphorus, magnesium
Bone and mineral disorders
o LOW produce active Vit D, Hyperkalemia
o Elevated phosphorus and PTH causes altered bone/ mineral
Anemia
o Lack of erythropoietin/ EPO
o Uremia shortens RBC life
Disorders of the Bladder
- Role is to transport urine formed by the kidneys and allow removal from the body
- Urine movement due to the effect of gravity and facilitated by peristatic movement of the ureters
Disorders of the Bladder: Diagnosis
- Urinalysis: for diagnosis of infection
- Ultrasonography: visualization of the urinary system
- Urodynamic testing: used for diagnosing voiding dysfunctions
Mechanics of Micturition Bladder innervation is supplied by
- Sympathetic nerves: allow relaxation and filling of bladder and contraction of internal urethral sphincter
- Parasympathetic nerves: contraction of the bladder relaxation of internal urethral sphincter
- Stomatic pudendal nerve: innervates the external bladder sphincter
Stress Incontinence:
involuntary leakage of urine during activities that increase intra-abdominal pressure, such as coughing, sneezing, laughing or physical exercise
Stress Incontinence: Etiology
weakening of the pelvic floor muscles and the urethral sphincter
- Commonly seen in women after childbirth, menopause
Urge Incontinence (Overactive Bladder):
Sudden and intense urge to urinate followed by involuntary loss of urine
Urge Incontinence (Overactive Bladder): Etiology
- Overactivity of the detrusor muscle
o Conditions take urinary tract infections, neurological disorders (e.g. Parkinson’s disease, multiple sclerosis)
Overflow Incontinence
Continuous dribbling of urine or feeling of incomplete bladder emptying
Overflow Incontinence: Etiology
Obstruction of the bladder outlet (e.g. enlarged prostate, urethral stricture) or weak bladder contractions (e.g. diabetic neuropathy, spinal cord injury) bladder becomes overly full. Causing urine to overflow
Mixed Incontinence:
Combination of stress and urge incontinence symptoms of both types are present
Bladder Cancer:
Fourth most common in males, eighth most common in females
Bladder Cancer: Risk Factors
- Age
- Smoking
- Carcinogenic chemicals
Bladder Cancer: Pathogenesis
Most tumors originate from the transitional epithelium (urothelium)
Bladder Cancer: Clinical manifestations
- Hematuria
- Frequency and urgency
Bladder Cancer: Treatment
- Surgery, radiation therapy, chemotherapy, wand immunotherapy
Disorders affecting:
- Penis and male urethra
- Scrotum and testes
- Prostate
Categories Disorders of the Penis & Male Urethra:
- Congenital
- Acquired
- Infectious
- Neoplastic
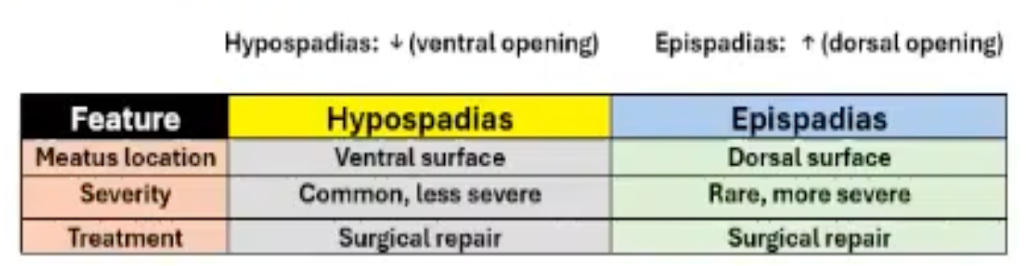
Disorders of the Penis & Male Urethra: Congenital Disorders
Acquired Disorders: Priapism
Painful, persistent erection
Acquired Disorders Priapism: Etiology
Sickle cell disease, leukemia, medications
Acquired Disorders Priapism: Treatment
Aspiration, a-adrenergic agents. Surgery
Phimosis vs Paraphimosis:

Erectile Dysfunction (ED): Primary
- Never achieved erection
- Often psychological
Erectile Dysfunction (ED): Secondary
- Previously normal erections
Erectile Dysfunction (ED): Etiology
- Vascular disease
- Diabetes
- Endocrine disorders (pituitary dysfunction (LOW luteinizing hormone, LOW testosterone)
- Medications (antihypertensives, antihistamines, some antidepressants)
- Surgery
Erectile Dysfunction (ED): Treatment
Determines psychogenic or organic cause
- PDE-5 inhibitors (Viagra, Cialis)
- Injections of Vasoactive medications: papaverine, phentolamine, prostaglandin E
- Penile prosthesis
Disorders of the Scrotum and Testes: Cryptorchidism
Undescended testes
- HIGH risk of infertility and cancer
Disorders of the Scrotum and Testes Cryptorchidism: Treatment
Orchiopexy, Human chorionic gonadotropin (hCG)
Hydrocele vs Spermatocele:

Testicular Torsion:
- Twisting of spermatic cord → compromised vascular supply and ischemia
- Medical emergency
Testicular Torsion: Clinical Manifestation
- Sudden severe pain
- Swelling, nausea
Testicular Torsion: Treatment
- Emergency surgery
- Salvage possible within 12 hours
Infectious Disorders: Epididymitis
Inflammation from infection or urine reflux
Infectious Disorders Epididymitis: Clinical Manifestation
- Fever, urethral discharge
- Enlarged, reddened, tender scrotum
- Scrotal pain with radiation into inguinal area
Infectious Disorders Epididymitis: Treatment
- Treat with antibiotics, bed rest
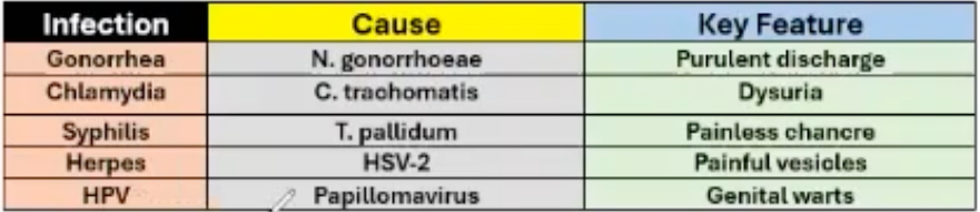
Sexually Transmitted Infections:
Neoplastic Disorders: Testicular Cancer
- Most common solid tumor in 20-34
Strongly associated with cryptorchidism