Sexology
1/180
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
181 Terms
Gender
the roles of cis and trans (any gender constructed in society)
Sexuality
sexual feelings, thoughts, attractions and behaviours towards others
Sexual behaviour
behaviour that produces arousal and increases chances of orgasms
Sexual identity
how one defines themselves with regard to sexual/romantic interests
Sexual orientation
what one actually does and likes
Sexual health
the ability to sexually adapt and self-manage in the face of life’s physical, psychological and social challenges
Sexual rights
basic inalienable rights regarding sexuality
Sexology
scientific study of human sexuality from bio-psycho-social perspective
Purpose of sex
→ progeny
→ please (bonding)
→ money/business
Sources of knowledge regarding sex
→ innate/own experience
→ family and friends
→ school, religion, government
→ media
→ health care professionals
Consequences of bias sex source
→ heteronormativity
→ norms in orgasms
→ shame and stigma
→ women tend to report lower numbers of sexual partners
Gametic union
union of sperm and egg
Sex (lit)
sexual anatomy and behaviour
Gender
male/female/trans - often gender binary
Communication theorists: 3 types of media influence
Cultivation Theory
Framing Theory/Agenda Setting
Social Cognitive Theory
Cohabitation
if you finish university, you’re more likely to marry the first romantic partner you live
longevity and sex
sexual activity inversely related to mortality and intimacy
Psycho-neuro-endo-hemo (vascular) dynamics
Desire
hormones
nerve/neurotransmitters
clitoris and penis have the same arousal
Excitement arousal
circulation
nerves/neurotransmitters
Orgasm
nerves/neurotransmitter
women can have only one, multiple, or no orgasm
Most important organs in sex
skin and brain
Gonads
primary reproductive organs
women: ovaries
men: testes
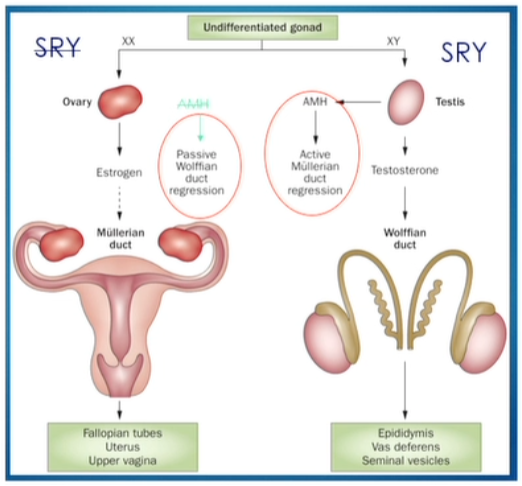
Development of Gonds
→ female development is the default
→ development depends on the presence of SRY gene (always on Y chromosome)
→ present SRY (sex-determining region) gene = testes
Sex development of gonads
in males @ 7th week, outer portions of gonads degenerate and inner portions develop into testes
in females @ 11th week, inner portions of gonads degenerate and outer portions develop into ovaries
Puberty
Development of Secondary sex characteristics
→ occurs when hypothalamus begins to secrete gonadotropin-releasing hormones (GnRH) causing pituitary to release
→ LH and FSH
Sexuality and 3 brain system
limbic system
hypothalamus
genital reaction
Limbic system and sexuality
important for controlling behaviour for survival
Hypothalamus and sexuality
hunger and thirst, circadian rhythm and sex (controller autonomic and endocrine output with different core regions)
Genital reaction and sexuality
Core regions in the hypothalamus project directly or via core regions in the brainstem into autonomous neurons in the spinal cord
Neurobiology of sexual drive and function
1) software - role of hormones, neurotransmitters and neuromodulator
2) hardware - how neural network process and modulate sexual responses
Dual control model
→ whether sexual desire increases from hormones or not, the mental state plays a part
→ as well as psychosocial, cultural and behavioural
Relevant innervation/vascularisation of penis
dorsal nerve → sensitivity
pudendal artery → function
Male sexual response stages
excitement phase
plateau phase
orgasmic phase
resolution phase
Erection types
psychogenic erections
reflexogenic erections
nocturnal erections
Psychogenic erections
→ the cortex which influences sacral centres and through hypogastric center creating of erection
Reflexogenic erection
→ signals from penis to pudenda nerve and to sacral region through reflex hypogastric plexus to the corpora of penis
Nocturnal erection
→ reflexogenic during REM sleep
Mechanism of erection
erotic stimuli: key neurotransmitter for erection: dopamine
neural initiation: parasympathetic oxytocinergic nerve fibres
cellular activated: activation of NO-L-Arginine cGMP pathway
PDE 5 releasing NO
relaxation of cavernous smooth musculature
erection
Role of Nitric Oxide
Stimuli → NO released → cGMP formation → vascular smooth muscle relaxation → influx of blood into sinusoids
Veno-occlusive mechanism in penile erection
→ penis and clitoris is the only organ in the body that moves from flaccid to erection
→ more blood goes in (arterial influx) and less blood comes out (venous efflux)
Erection enemies
Smoking - atherosclerosis, build-up of plaque and fatty materials in arteries
Alcohol - affects blood vessels and nerves responsiveness
Drugs - heart problems, irregular blood pressure, mental health
Stress - effects of cortisol and adrenaline
Obesity - atherosclerosis, build-up in arteries
Deadly Quartet
diabetes
obesity
hypertension
dyslipidemia (high cholesterol)
→ endothelial dysfunction (blood) → cardio vascular diseases and erectile dysfunction
Ejaculation
→ outcome of sexual arousal
→ often occurs simultaneously with orgasm
→ induced by nerve stimulation
→ expulsion of semen from outer urethral orifice
Anatomy involved in ejaculation
Brain - Spinal cord - Peripheral nerves (dorsal/pudendal nerve)
Composition of ejaculation
Volume (1.5-5 ml) = seminal vesicle (50-70%) + prostate (15-30%) + ampula vas deferens, cowper glands, urethral glands (<5%)
Cerebral control of ejaculation: key supraspinal centres
thalamus → hypothalamus (paraventricular nucleus + medial preoptic area) → midbrain (periaqueductal grey) → pons (nucleus paragigantocellularis)
Neurotransmitters and ejaculation
serotonin (5-HT)!!!
dopamine (DA)
gamma-aminobutyric acid (GABA)
noradrenalin
→ sympathetic process
Average time of ejaculation
5 minutes - from penetration to ejaculation
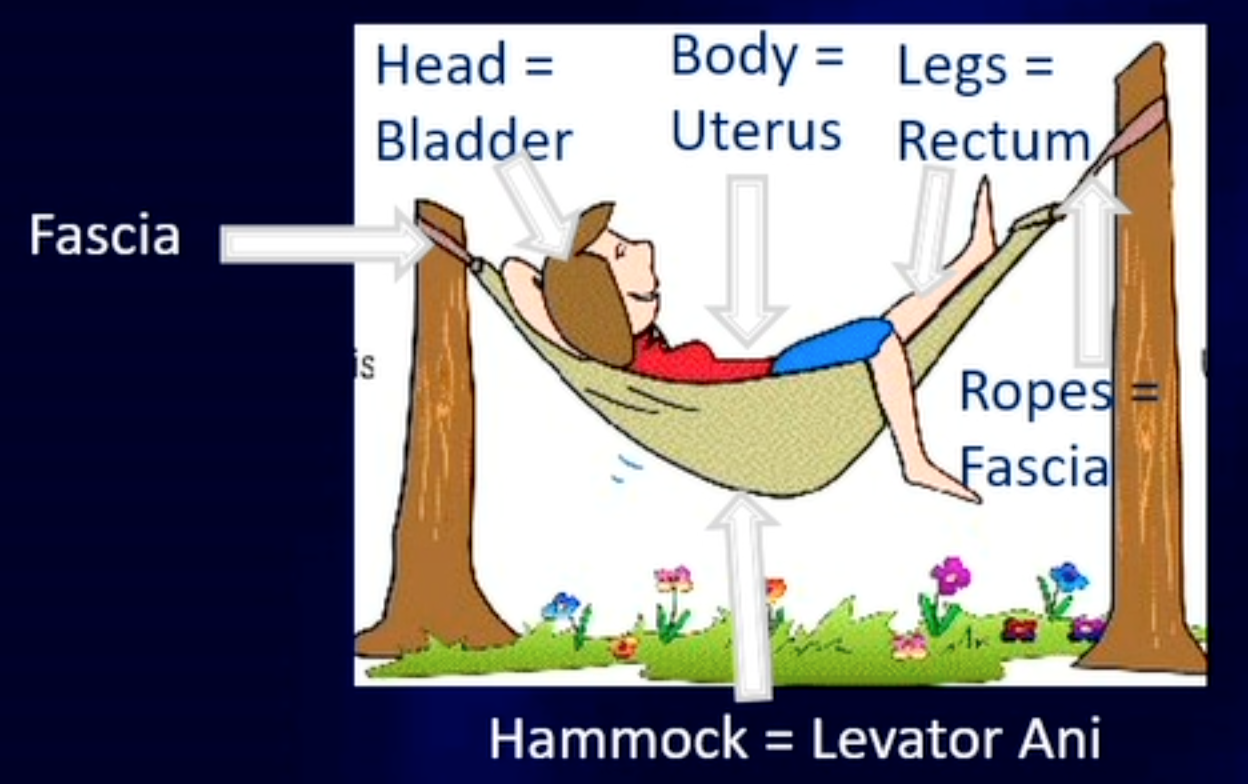
Pelvic floor: 3 function
supports bladder
part of sphincters mechanism
birth process
“complex web of muscle, fascia and fibrous tissue”
Pelvic floor: so much more
→ support
→ passage
→ mobility/stability
→ sex (respond to arousal and enhance enjoyment)
→ emotion
PF: hammock analogy
Involvement of pelvic floor
→ Enhancement of blood flow - ischiocavernosus muscle facilitates erection, bulbocavernosus maintaining the erection
→ inhibit ejaculation relaxation of bulbocavernosus and ischiocavernosus muscles
PF overactivity
dyspareunia
genital pain (vulvodynia, orchialgia, prostatodynia, radiating pain penis)
orgasmic pain, obstructive ejaculation
non-disappearing swollen feeling in the genitals (PGAD)
Sexual differentiation
Conditions for healthy sexual development
matching gender identity
women pedagogical climate
positive examples/messages of relations and sexuality
possibility to age-specific consensual sexual practice behaviour
skin contact
Puberty: secondary sexual characteristics
Onset:
men - first ejaculation
women - first period, breast
hair in pubic area
Hormones and sex
hypothalamus → GnRH
anterior lobe of pituitary → LH and FSH
gonads → estrogen, testosterone, progesterone
Fertility timeline
born - 1 million
puberty - 400,000
every ovulation - 1-2
menstruation - 400
Normal female organs variation
glans clitoris - 0.5-3.5 cm
vagina - 6.5-12.5 cm
hymen - 1-2.5 cm
labia minora - 0.7-5 cm
Labia
width: 7-50 mm
→ different lip sizes
→ congenital abnormal inner labia
NVOG guideline
mot interventions are cosmetic
Clitoris
8-10cm
→ only organ for sexual pleasure purpose
→ clitoris can act as pads during intercourse
Vaginaal vestibulum
→ sensitive lubrication (protection)
Internal genitals
Uterus - womb 6-7 cm length
Ovarium - ovary 1.5×2.5 cm
Tuba - fallopian tube max 5 cm
Genital arousal
→ increase in genital blood flow
transudate: lubrication from vagina wall
→ swelling of vulva and clitoris
→ erection and retraction of glans clitoris
→ elongation of vagina and ballooning
→ transudate: lubrication
→ rise of uterus
Physiology of sexuality
Peripheral responses
→ cardiovascular: heart beat increase
→ respiratory tract: frequency increase
→ skin: sex blush??
→ stiffness of nipples
Physiology of sexuality: orgasm
→ intense feeling of pleasure
→ some degree of altered consciousness
→ specific sensations in genital region and pelvis
→ muscle contraction in PF and uterus
→ other reactions: rhythmic movement, vocalisation
Congenital abnormal external genitals: hymen
intercourse not possible = primary vaginismus
→ hymen string
→ imperforate hymen
Other clinical problems: female genital
→ ovarian cyst
→ myoma/fibroid
→ vulvar carcinoma
Female genital mutilation (FGM)
→ >200 million girls
→ age 4-12 years
→ 30 countries in Africa, ME and Asia
→ mix of sociocultural factors within families and communities
→ nor religion association
→ views on clean, purity, beauty, femininity
4 types of FGM
clitoridectomy
excision
infibulation
all other harmful procedures
Congenital disorder of development: MRKH syndrome
Mayer-Rokitansky Kuster Hauser Syndrome
→ 46xx
→ no menstruation
→ infertile
→ intercourse not possible
Disorder of sexual development: AIS
Androgen Insensitivity Syndrome
→ 46XY
→ no hair (armpit/pubic)
→ external genitals are female
→ vaginal and uterus agenesis
→ no menstruation
→ infertile
Disorder of sexual development: AGS
Adrenogenital syndrome in women
→ 46xx
→ enzyme defect 21-hydroxylase
→ internal genitals female
→ clitoral hyperplasia
→ high testosterone levels
→ autosomal recessive
→ adrenal hyperplasia
Rate of penetrative orgasm
30%
→ due ot clitoris anatomy
Early sexual development
0-4: discovering your body (touching)
4-6: learning about social rules, first friendship
7-9: shame, fantasies and first infatuation
10-15: puberty
16-18: adolescence
18+: adulthood
Sexuality education
much more than sexual intercourse:
→ biological: body, reproduction, health
→ psychological: emotions, experience, thoughts, mental wellbeing
→ social: gender, education, expectation, culture, peer group
Principles comprehensive sexuality education
based on…
age
human rights
scientific facts
needs
positive approach
gender equality
view humans as sexual beings?
culturally sensitive
bio-psycho-social approach
Measuring sex
→ questionnaire
→ psychophysiological studies
Specific physiological sexual responses
Men
→ increase in volume of corpora cavernosa, erection
Women
→ increase in volume of corpora cavernosa, increase in blood flow to vaginal wall thus lubrication
Barlow strain gauge
→ assess different circumferences of the penis
Photoplethysmograph
→ assess changes in vaginal blood flow
Erotic stimuli
fantasy
tactile
photography
erotic film
Issues in psychophysiological sex research
objective assessment
small samples (selection bias)
ethics (private, intimate subject)
Automatic response to sex?
→ after an erotic film, the response is fast (increase in vaginal blood flow)
→ regardless of whether they are feeling aroused or not (and age)
Ledoux and Damasio
Emotional stimulus → sensory thalamus …..
"quick and dirty pathway →> amygdala
“neat and slow” pathway → sensory cortex +hippocampus → amygdala
fMRI study:sexual stimuli activate emotion motivation system?
→ is it influenced by dopamine?
→ 53 healthy young men
→ 3 groups: levodopa (high dopamine), haloperidol (low dopamine), placebo
→ unconscious sex stimuli
fMRI study: sexual stimuli activate emotion motivation system? - results
recognition task:
percentage of correct classification was below chance level
target picture was not consciously perceived
brain activity:
activation in ACC and nucleus accumbens
this was stronger with more dopamine
genital x sexual arousal correlations
men: high
women: low
hypothesis: womens sexual feelings are determine by evaluation of context rather genital response
Meaning of stimulus: study by Laan
meaning of sexual stimulus: regular vs women-oriented
film excerpt matched in terms of nature duration of portrayed sexual activities
measure genital and sexual arousal response in men and women
Meaning of stimulus: study by Laan - result
genital response:
no significant difference in genital response between films (for both genders)
subjective sexual response
men: sexual feelings equally strong
Iwomen: stronger for women-oriented film
Unconscious activation: implications
motivation process has been activated before the individual is conscious
helps understand why sexual response can be difficult to control
pharmacological regulation?
research on relationship between genital - subjective
automatic genital response is not evidence of positive sexual experience
reduced sexual arousal does not indicate disturbed genital response
meaning of stimulus is important (women)
viagra for women does not work
Criteria for diagnosing sexual disorder
must cause significant distress
must occur on 75-100% of occasions
minimum duration of 6 months
Presentation of sexual complaints (women)
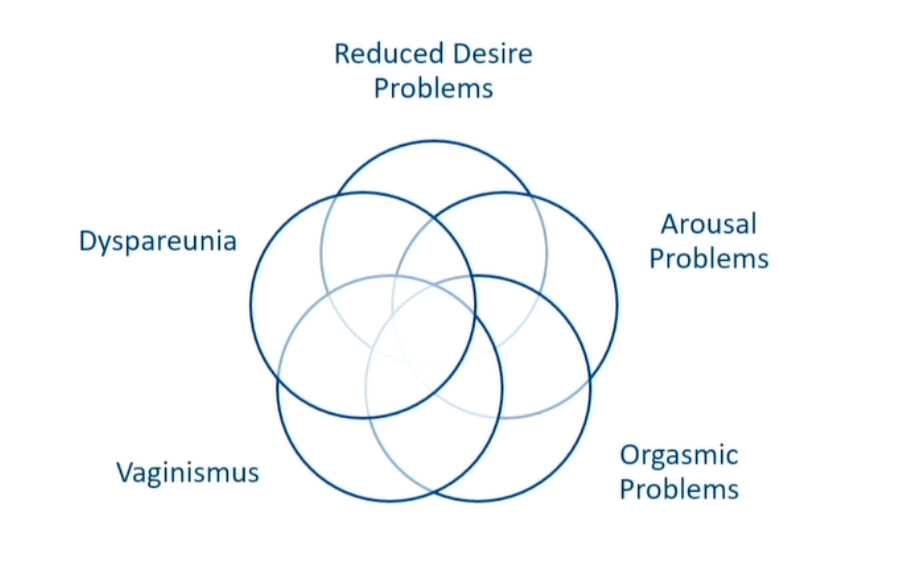
Female sexual arousal disorder
lack of:
interest
sexual thoughts/fantasy
initiation of sexual activity
sexual excitement
arousal to erotic cue
genital sensation
Gender difference in sex
men masturbate more
they fantasise more often about sex
experience sexual desire more often
report less often problems in lack of desire
Prevalence of problems in women
lack of sexual desire: 20-30%
sexual arousal problems: 11-31%
sexual distress as a criterion: decrease of 50%
high co-morbidity of desire and arousal problem
Orgasmic disorder
delay in, infrequency of, or absence of orgasm
reduced intensity of orgasmic reactions
Prevalence of female orgasmic problems
problems reaching orgasm: 3.5-35%
only 25-30% reach orgasm during intercourse
Etiology: Incentive motivation model (Toates)
Stimulus → (memory→sexual motivation←physical state) → behaviour and genital response/feelings
*regulation and inhibition plays a part
Arousability and effect
Hormone levels → cancer ovaries, surgical menopause
Somatic diseases → neurological and endocrine disorder
Medication → SSRI, anti-psychotics, anti-androgens
Arousability of healthy women with disorder (Laan)
laboratory study with healthy control vs sexual arousal disorder
genital and subjective sexual response to film
using photoplethysmography
Arousability of healthy women with disorder (Laan) - results
no difference in genital response
report lower subjective sexual response
but no difference in negative response