Weel 6 Trauma ABCDs: Part I Assessment and management
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Airway
Management of the airway is paramount in the successful resuscitation of the trauma patient.
Without a patent airway, all is lost.
However, the best airway for a particular patient may not be an advanced airway or endotracheal tube.
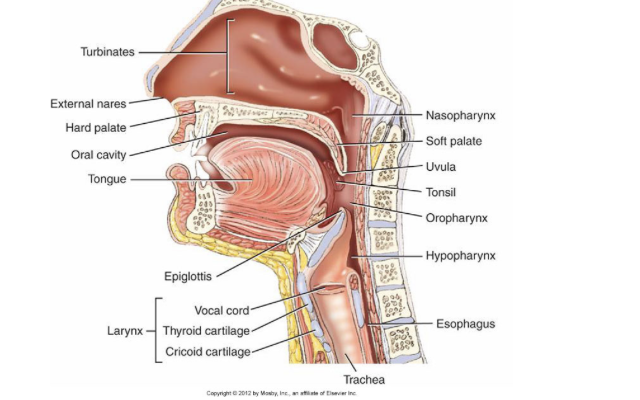
Upper anatomy of airway
Pediatric Considerations
Larger head and tongue
Special attention to positioning
Greater potential for airway obstruction
Trachea
Shorter and conical shape
Epiglottis
Proportionally larger
Floppier than adults’
Assessment
If the patient is talking, airway is open.
Look for:
Blood
Broken teeth
Foreign bodies
Vomitus
Hematomas
Listen for:
Snoring
Stridor (inspiratory)
Gurgling (expiratory)
Hoarseness
Feel for:
Crepitus in the neck - crunchy bones
Oxygen saturation
Injury and Dysfunction
Partial obstruction–some passage of air
Total obstruction–no passage of air
Common causes of obstructions
Tongue
Foreign body
Blood, vomit, teeth
Direct Trauma
Blunt
Swelling and edema
Fractured larynx
Crepitus (subcutaneous emphysema)
Hematoma
Penetrating
Bleeding into the airway
Crepitus (subcutaneous emphysema)
Hematoma
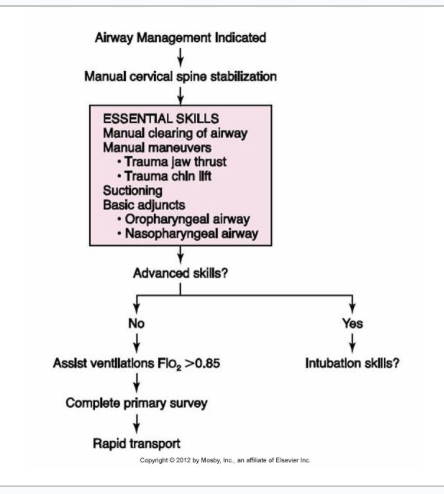
Airway Management
The goal in managing any patient’s airway is to maintain an open and patent airway that allows for adequate breathing, ventilation, and oxygenation.
Management progresses from basic to more advanced procedures and adjuncts.
Breathing, Ventilation, and Oxygen
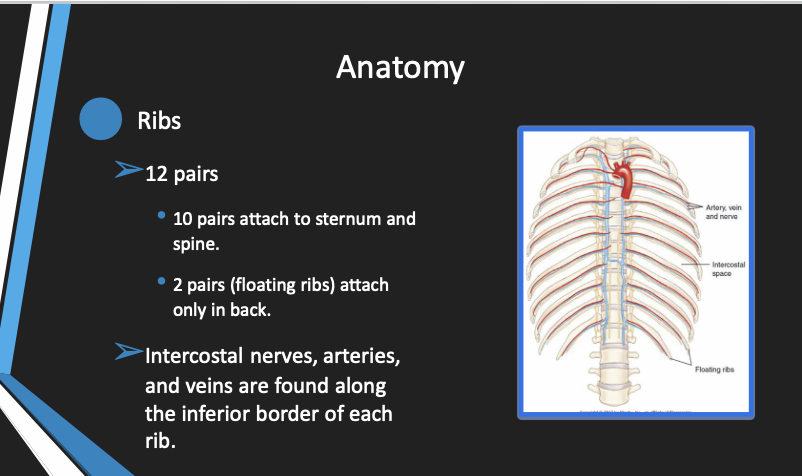
Anatomy
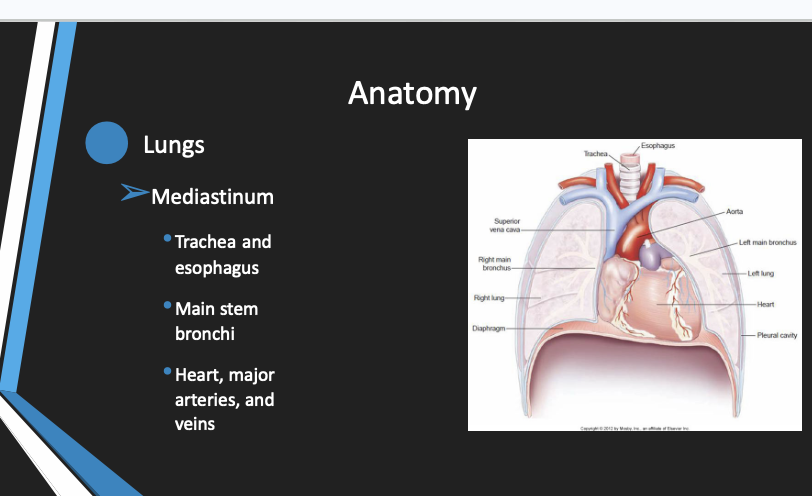
Anatomy
Assessment
If the patient’s breathing draws your attention, there is a problem until proven otherwise.
Some examples would be:
If you can hear them breathing from across the room
If they position themselves for easier breathing
Tripoding
Assessment
Look (observe)
Listen (auscultate)
Feel (palpate)
Pneumothorax
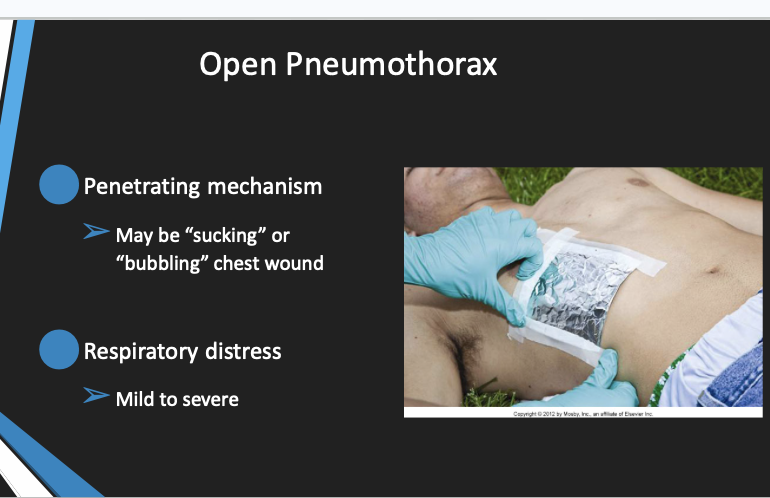
Present in up to 20% of severe chest injuries
Classified as simple, open, or tension
May progress from a simple to a tension
Tension pneumothorax is life-threatening.
Needle decompression may be needed.
May be associated with a hemothorax
Simple versus Tension Pneumothorax
Simple
Blunt or penetrating
BS decreased or absent
Mild to moderate ventilatory distress
Tension
Blunt or penetrating
BS decreased or absent
Marked ventilatory distress
Hemodynamic compromise
Assessment and Diagnosis
Open Pnuemothorax
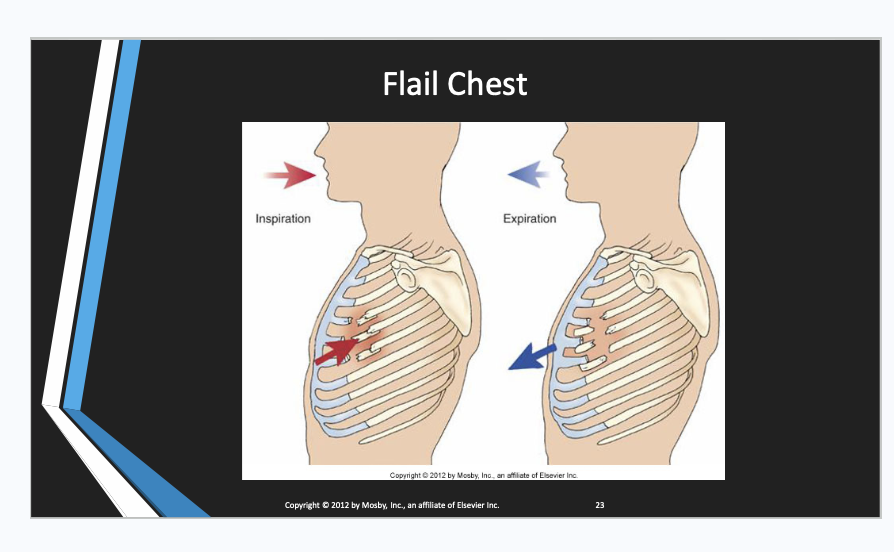
Flail Chest
Simple Rib Fractures
Most common thoracic injury
Usually in ribs 4 through 8, laterally
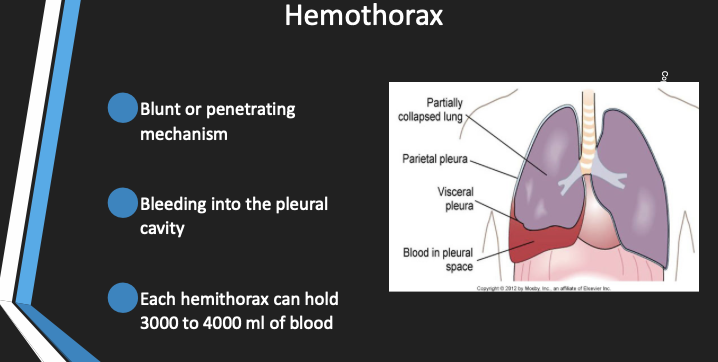
Most common cause of hemothorax
Simple rib fractures may be associated with injuries to liver and spleen.
Common complaints are chest pain and shortness of breath.
Management Goals
The goal of the treatment of injuries that affect breathing is to maintain adequate oxygenation and ventilation.
Administer supplemental oxygen, PRN.
Assist ventilations as necessary .
Seal open chest wounds.
Recognize and decompress tension pneumothorax.
Continuous assessment of breathing is essential.
When to Assist Ventilations
Respiratory rate, AND inadequate
More than 28
Fewer than 10
Insufficient spontaneous tidal volume
Poor chest rise
Use of accessory muscles
Decreased SaO2
Consider the need for airway management.
Circulation and Hemorrhage and Shock
Metabolism
All cells require energy to function, and that energy is stored in the form of ATP molecules.
Aerobic metabolism
Oxygen is required for efficient production of ATP (energy).
Anaerobic metabolism
Inadequate oxygen results in decreased ATP production and accumulation of lactic acid.
Shock
Shock is a result of inadequate energy production to sustain life.
Any condition that causes generalized cellular hypoperfusion
This leads to inadequate cellular oxygenation that does not meet metabolic needs.
Hypoperfusion
Hypoperfusion results from:
Loss of blood (either externally or internally)
Impaired pumping of blood
Dilatation of the blood vessels (increased vascular space)
The end result is a decrease in circulating volume and RBCs moving through the capillary beds to deliver oxygen to the cells.
Lack of oxygen impairs metabolism.
ATP (energy) production decreases.
Cell membrane dysfunction occurs.
Potassium and lactic acid enter the blood.
Low pH results in release of cellular enzymes that autodigest cells.
Autodigestion leads to cellular death and organ failure.
Sodium and water enter the cell.
Cellular edema (swelling) occurs.
INFLAMMATION
There is a further loss of intravascular (blood) volume
The cycle continues.
Consequences
With inadequate ATP, the patient does not produce heat.
Body heat is lost to the environment.
What little ATP is being produced is used to shiver.
Lactic acid production increases.
As body temperature drops, blood clotting becomes impaired and hemorrhage can increase.
Cells and organs do not function properly.
Organ Tolerance to Hypoxia
Brain 4 to 6 minutes
Heart 4 to 6 minutes
Lungs 4 to 6 minutes
--------------------------------------------------------------
Kidneys 45 to 90 minutes
Liver 45 to 90 minutes
Gastrointestinal tract 45 to 90 minutes
--------------------------------------------------------------
Muscle 4 to 6 hours
Bone 4 to 6 hours
Skin 4 to 6 hours
Hypovolemic Shock
The most common cause of shock in the trauma patient
Due to hemorrhage
Loss of RBCs impairs oxygen transportation
In any trauma patient with shock, assume hemorrhage is the cause until proven otherwise.
Distributive Shock
Distributive
Neurogenic
Decreased systemic vascular resistance due to vasodilatio
Cardiogenic Shock
Cardiogenic (in trauma)
Intrinsic
Blunt cardiac trauma leading to muscle damage and/or dysrhythmia
Valvular disruption
Extrinsic
Pericardial tamponade
Tension pneumothorax
Pathophysiology of Shock
Shock is progressive.
Events in shock include:
Hemodynamic changes
Cellular (metabolic) changes
Microvascular changes
Compensatory mechanisms are short-term
Patient Assessment for Shock
Assess
Hemorrhage
Level of consciousness
Skin
Pulse
Respiration
Blood pressure
Confounding factors
Confounding factors
Patient age
Medications
Pregnancy
Pre-existing medical conditions
Shock without Obvious Cause
The patient is bleeding somewhere, even if you can’t see it
Internal hemorrhage
Fracture
Penetrating Injuries
This type of injury occurs when a penetrating object traverses the chest, abdomen, or extremity.
The object injures organs, tissues, and blood vessels that bleed internally into the surrounding cavities or tissue, or externally.
As the amount of blood loss increases, signs of shock develop.
Blunt Injuries
Pathway for blunt injuries is less visible.
Force is applied to the trunk and extremities.
Force is transmitted to the thoracic and abdominal organs and bones.
Injuries Commonly Associated with Hemorrhagic Shock
Traumatic Aortic Rupture (Tear)
Traumatic aortic rupture usually occurs at the junction of the mobile and fixed portions of the aorta just beyond the left subclavian artery.
Eighty percent to eighty-five percent die prehospital.
Of those who survive, 50% die within 48 hours if not treated.
Hemothorax
Abdominal Organ Injury
Abdominal organ injury results from a blunt or penetrating mechanism.
Injury to solid organs (liver, spleen, kidney, pancreas) generally results in hemorrhage that varies from mild to life-threatening.
It is also associated with leak of enzymes, bile, or urine into abdomen
Injury to hollow organs (small and large bowel) is usually not a cause of major blood loss; instead, they leak their contents and cause peritonitis.
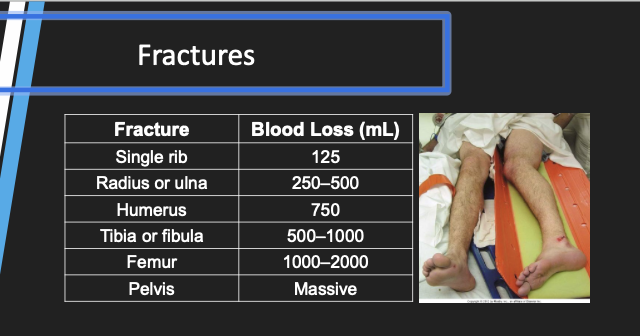
Fractures
Major or multiple fractures can lead to significant blood loss.
Femur or pelvic fractures are the most common cause.
Don’t underestimate blood loss due to multiple other fractures.
Injuries Commonly Associated
with
Distributive Shock
Neurogenic Shock
Secondary to spinal cord injury, usually cervical spine (down to T6)
Loss of sympathetic system vascular tone
Blood vessels dilate
Blood return to the heart decreases and cardiac output drops.
Perfusion and tissue oxygenation is usually maintained.
Skin remains warm and dry.
Injuries Common,y Associated with cariogenic shock
Blunt Cardiac Injury
Blunt mechanism
Direct injury to heart muscle, which rarely can cause valve rupture
Broad range of presentations
Dysrhythmia
New murmur
Sudden death
Pericardial Tamponade
Penetrating mechanism most common
Blood in pericardial sac
Increasing amount of blood in the sac compresses the heart, preventing adequate filling; thus, cardiac output decreases
Shock Management - keep them warm
Four questions guide management:
What is the cause of shock in this particular patient?
What is the care for this type of shock?
What can and should be done between now and the time the patient reaches definitive care?
Where is the best place for the patient to get definitive care?
Reduced cardiac output and impaired tissue oxygenation occur before the blood pressure drops.
Proper shock management improves the oxygenation of RBCs and improves the delivery of RBCs to the tissues.
Airway–what are the needs?
Ventilation–does it require assistance?
Oxygenation
Circulation
Patient positioning- supine
Hemorrhage control
Direct pressure will control most external hemorrhage
Tourniquet
Immobilization of fractures
Topical hemostatic agents may be recommended for prolonged transport situations
Distributive (neurogenic)
Must rule out hemorrhage as the primary cause of shock
Spine movement restriction (immobilization)
Transport considerations
Transport without delay to appropriate destination
Maintain body temperature
Patient compartment temperature should be 85 °F (29 °C)
Considerations in prolonged transport
Ensure airway and optimize ventilatory status.
Maintain external hemorrhage control.
Prevent body heat loss.
Reassess, reassess, reassess.
Minimizing complications
Assess for shock.
Assume hemorrhagic shock until proven otherwise.
Remember: Cardiac output and tissue oxygenation are impaired early.
Restore and/or maintain airway, ventilation, oxygenation, and circulation.
Hypothermia creates a cycle of worsening shock and hypothermia.
Transport without delay.
compensated vs decompensated shock
Compensated and decompensated shock are sequential stages of the same medical emergency. Compensated shock occurs when the body successfully uses its own regulatory mechanisms (like a racing heart rate and narrowed blood vessels) to maintain normal blood pressure. Decompensated shock represents a critical failure of these mechanisms, causing blood pressure to plummet and vital organs to suffer inadequate perfusion