4: cartilage, bone and disorders
1/133
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
134 Terms
trachea
thin wall. rigid tube ringed by C shaped hyaline cartilage.
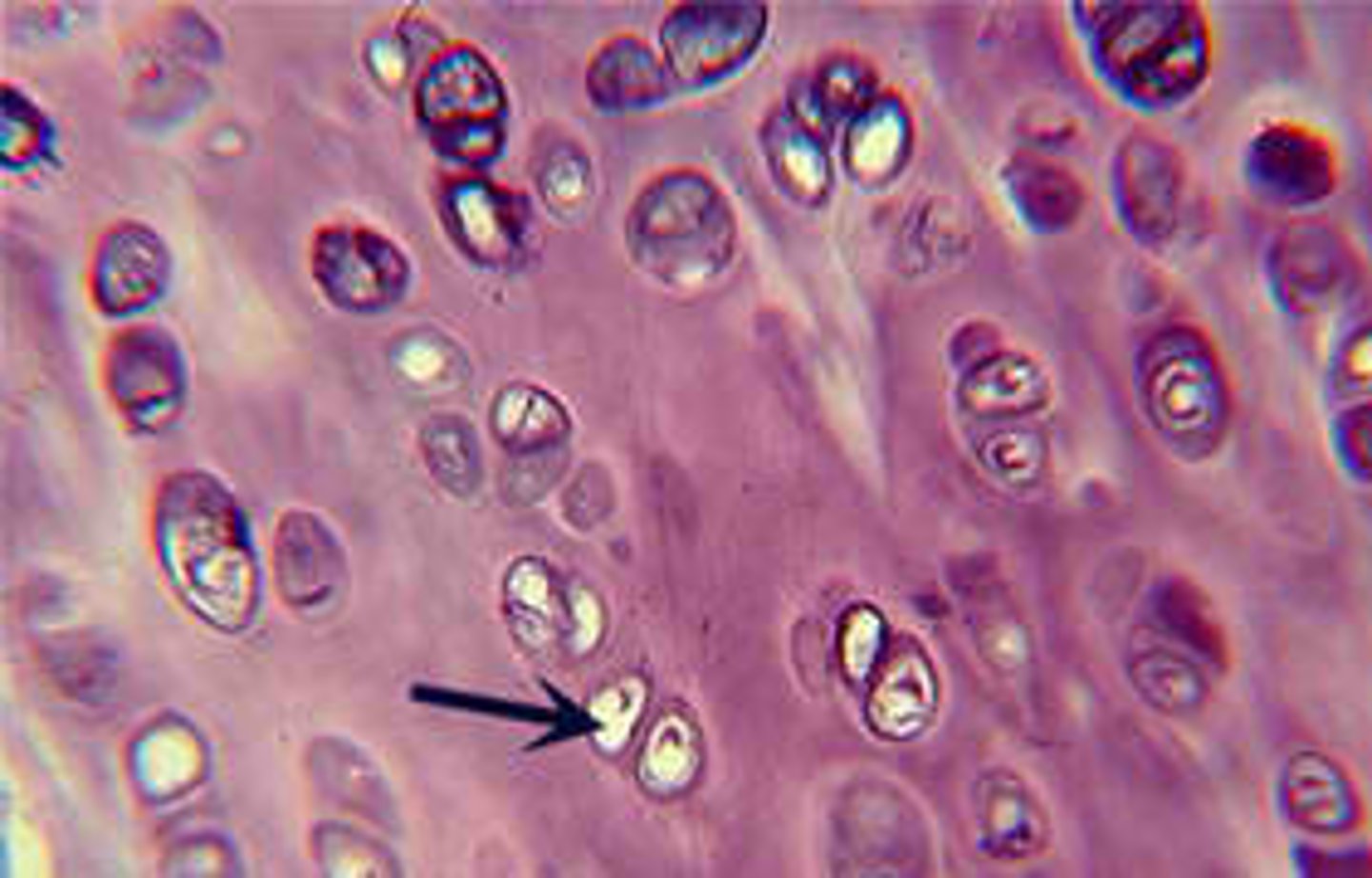
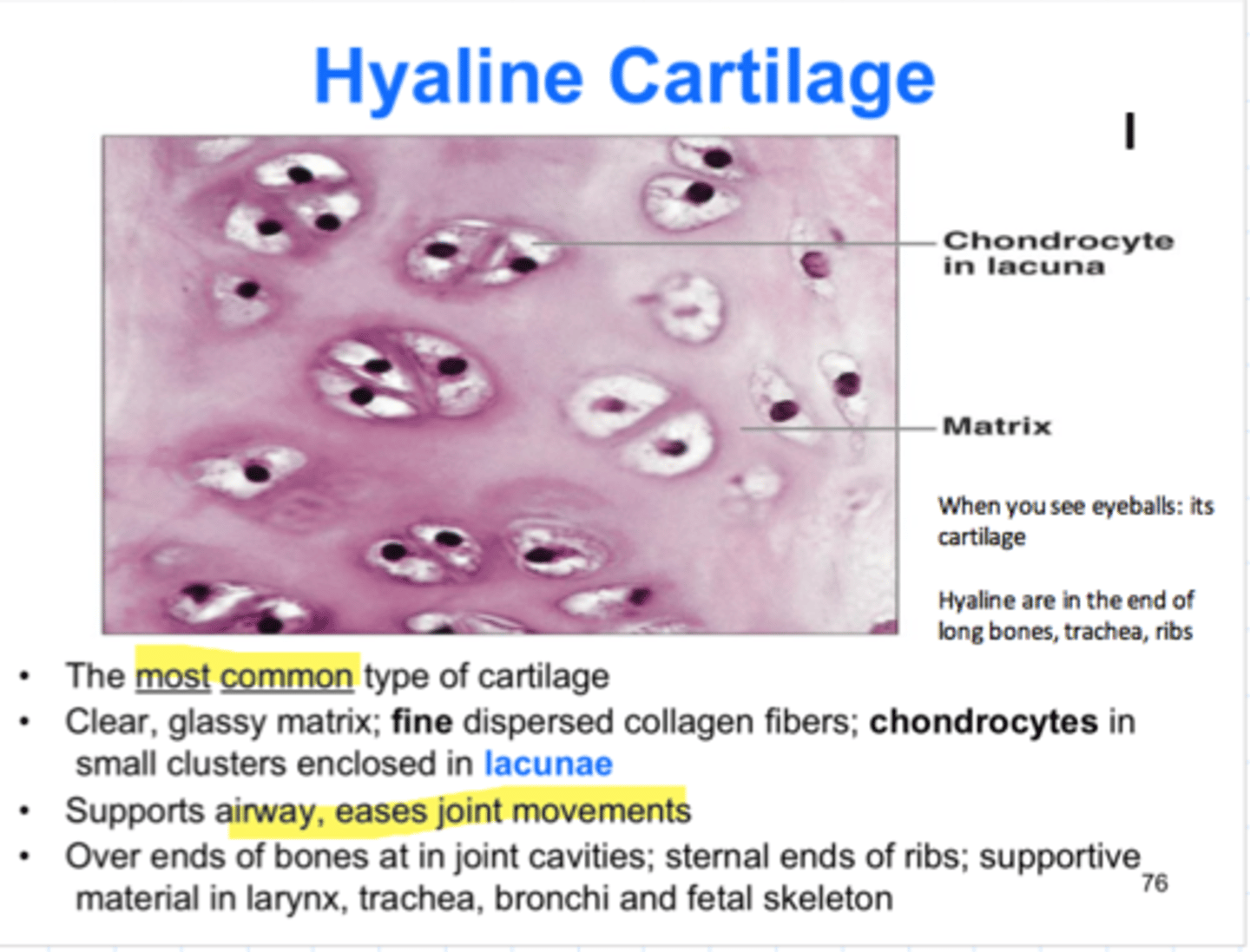
chondrocytes position
exist in lacunae which is rimmed by strongly basophilic (blue) territorial matrix with high conc of acidic sulphated GAGs secreted by chondrocytes
GAGs (glycosaminoglycans)
unbranched chains of glycoproteins. most common is hyaluronic acid
Hyaline matrix. why is it glassy?
matrix between chondrocytes (inter-territorial matrix) contains more collagen fibrils and less GAG. highly hydrated and hence does not stain strongly. gives it a glassy appearance
articular cartilage
hyaline covers the surfaces of bones where they come together to form joints. gets nutrients from synovial fluids.
why hyaline (esp articular) does not heal well
low capacity of chondrocytes for replication; poor blood supply
major long bone in the upper limb and major bone in lower limb whose articular ends covered in hyaline
upper: humerus, radius, ulna
lower limb:
femur, tibia, fibula
theory behind using hyaluronic acid injections for osteoarthiritis
HA major component of synovial fluid and help lubricate joint and reduce pain
malignant tumours of cartilage called
chondrosarcomas.
sarcoma
cancer of mesenchymal origin
smoking on morphology of respiratory epithelium
metaplasia. epithelium changes from pseudostratified columnar to stratified squamous
explain why PAS identifies goblet cells effectively
identify glycoproteins, stains mucins in goblets
adenocarcinoma
tumour of glandular resp epithelium
smoking on cilia of resp epithelium
paralysis. infection. increased exposure of epithelium to carcinogens
single nucleotide polymorphism
variation in a DNA sequence occurring when a single nucleotide in a genome is altered
insertions and deletions
additions or losses of nucleotide pairs in a gene
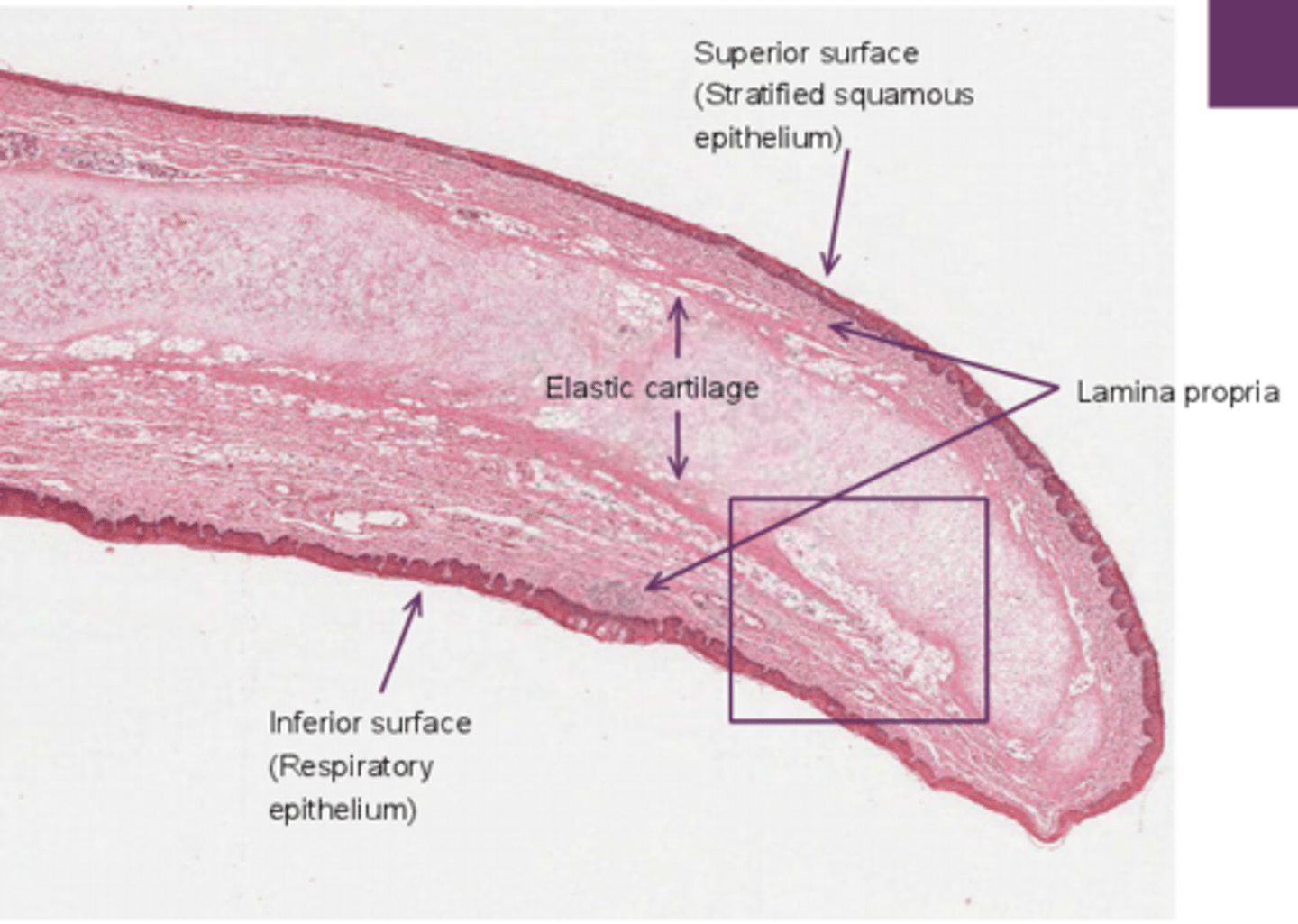
histology of elastic cartilage
dense aggregations are eosinophilic. dark pink bundles against lighter pink of ECM
Perichondrium
Dense irregular connective tissue membrane covering cartilage
why is respitory epithelium unique in epiglottis
particularly thick.
two major components of elastic fibres
elastin and fibrillin
epiglottis unique feature and why
SSNKE buccal epithelium on one side and PSCE on the respiratory side. this is because it is normally in an upright position and resp e is continuous with the airway . epiglottis closes to cover trachea on swallowing and the aspect lined with SSNKE provides protection from abrasion from boluss
elastic cartilage location
epiglottis, outer ear, auditory tube, external auditory meatus
cartilage is maintained by what type of growth
appositional: differentiation of stem cells from supporting CT (chondroblasts in perichondrium) and interstitial: division of cells within a tissue (chondrocytes within a cartilage)
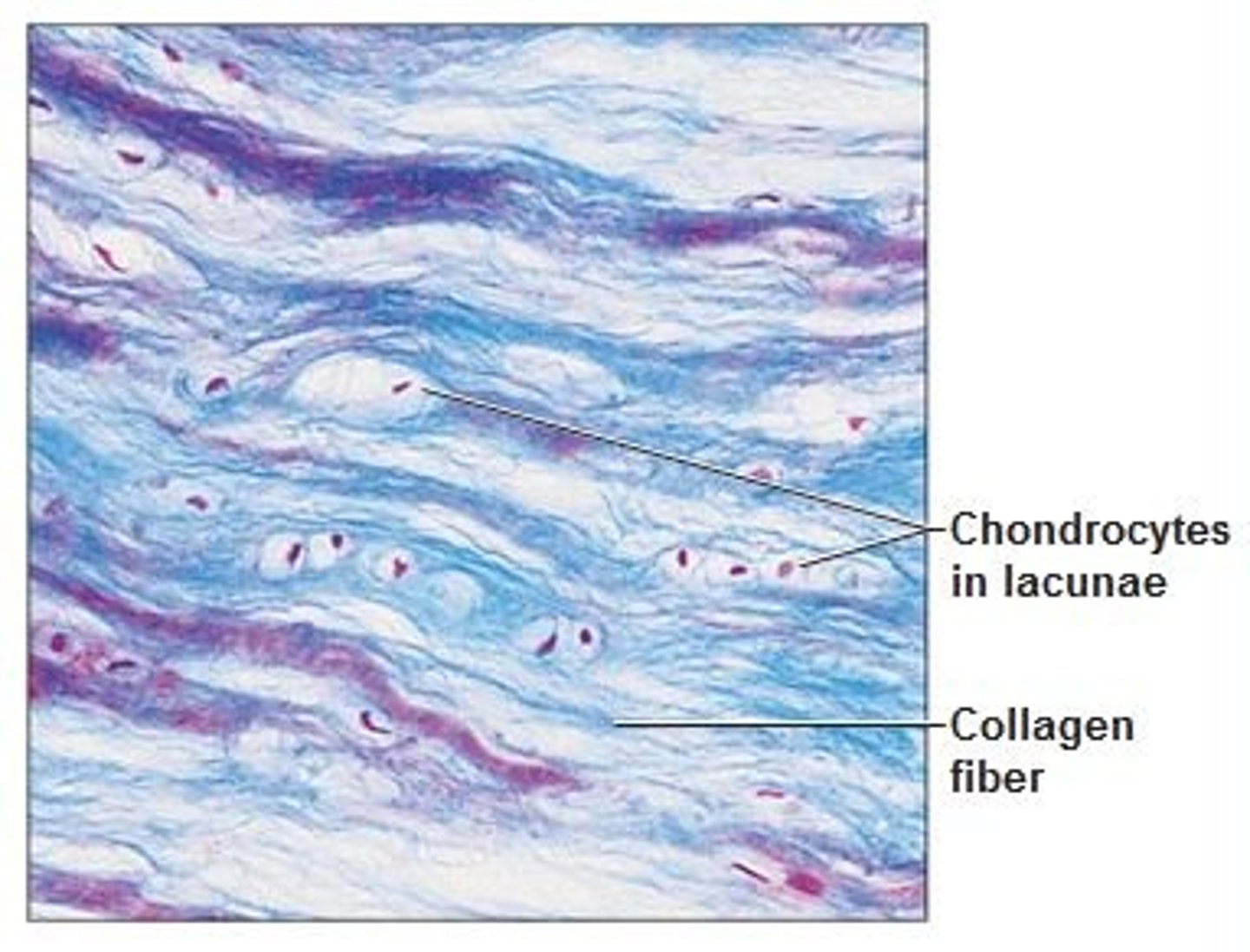
Fibrocartilage
comprised of DRCT and hyaline cartilage and contains fibroblasts as well as chondrocytes.
cartilage that contains fibrous bundles of t1 collagen, such as that of the intervertebral disks in the spinal cord. sternoclavicular and temporomandibular joints.
intervertebral disk
trabecular bone, skeletal muscle. inside, annulus fibrosus (fibrocartilage). nucleus pulposus
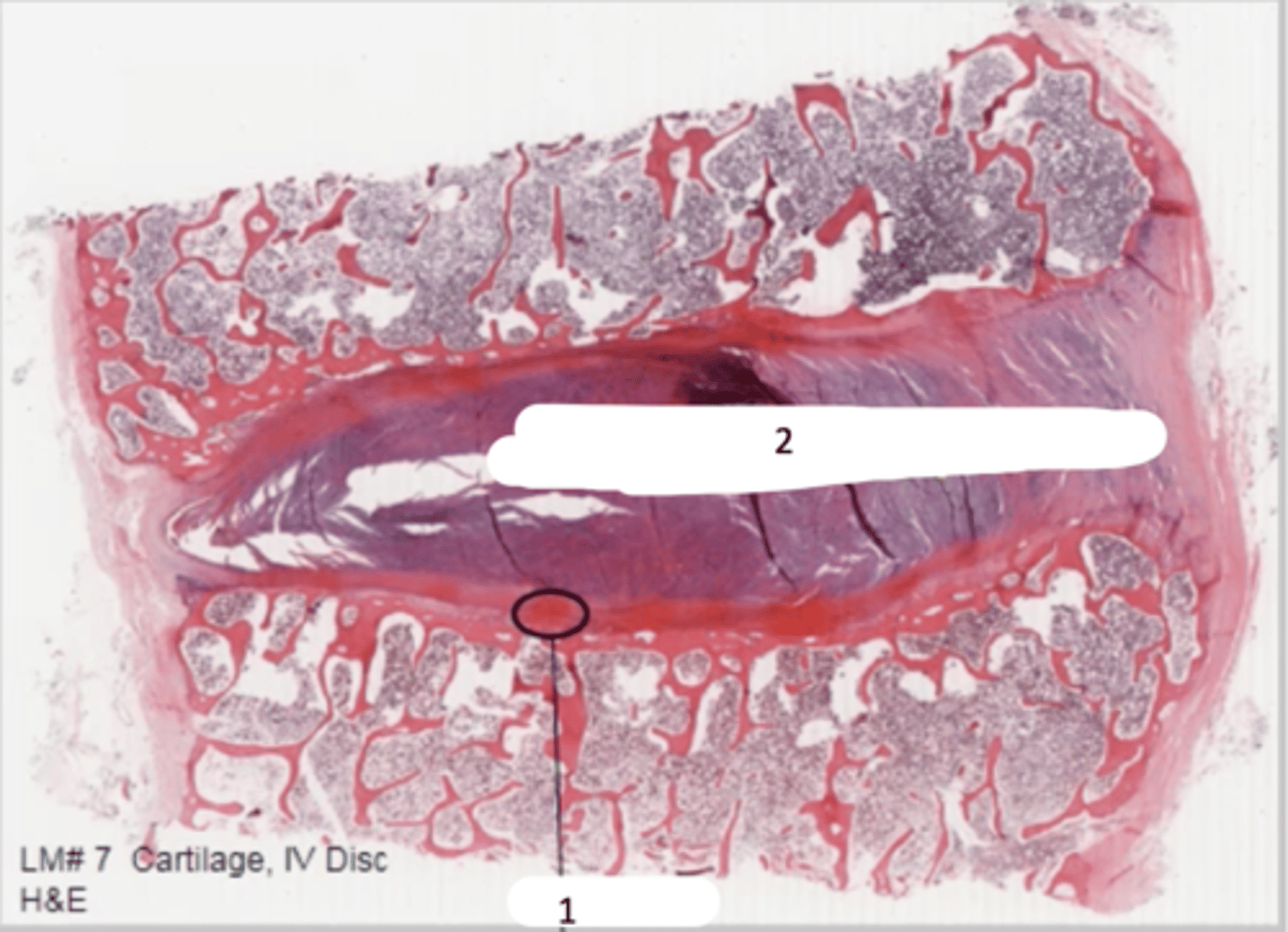
fibrocartilage adaptation for its position
shock absorbance, resistance to shearing
what structures hold the annulus fibrosus in place
ligaments
what is the nucleus pulposus comprised and what is its function
gel matrix (water and hyaluronic acid) acts as a shock absorber
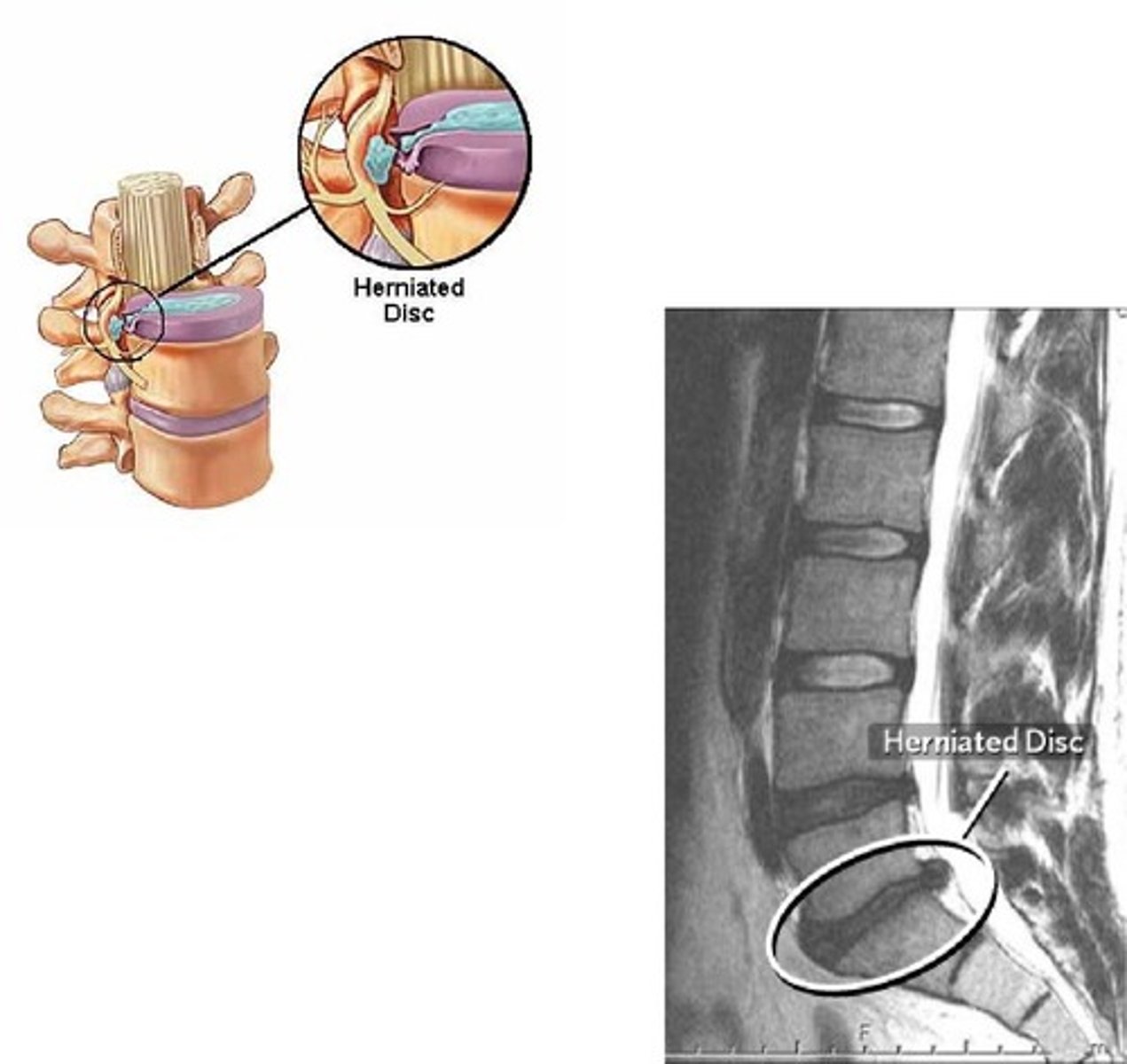
Slipped (herniated) disc
displacement of nucleus pulposus due to weakness of annulus fibrosus (which cracks with age and under excess force) displaced disk can put pressure on adjacent nerves.
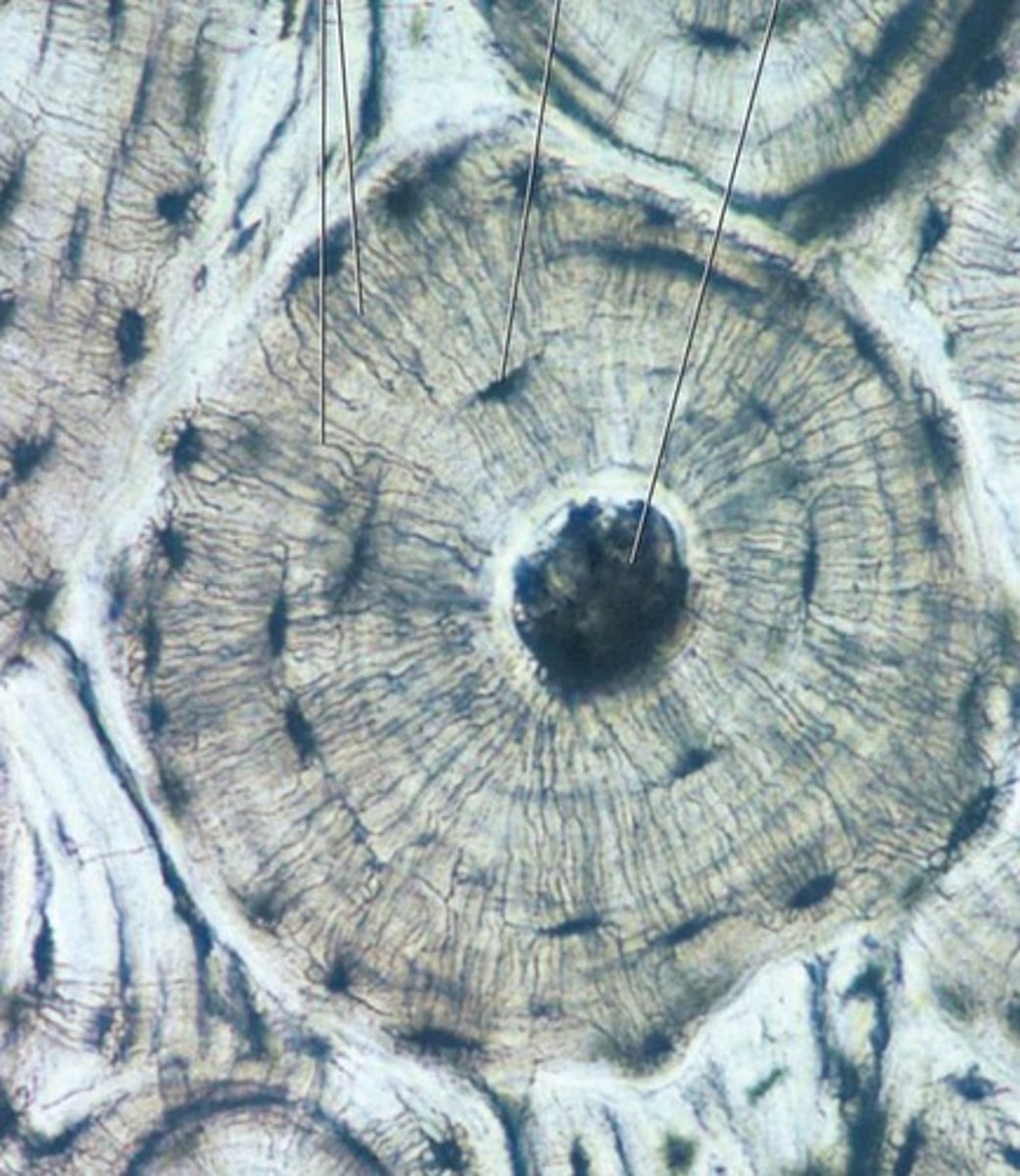
ground bone
Osteons-
Central Canal (haversian)- middle dark hole
osteocytes in Lacunae- (black dots)
Canaliculi- spider web allows communication between lacunae
intersitial lamella- outside
outer lamella of osteon
Osteon
structural unit of compact bone. slender cytoplasmic processes that reach to adjacent osteocytes via canaliculi. processes connect via gap junctions to allow for passage of nutrients. connect to haversian canals.

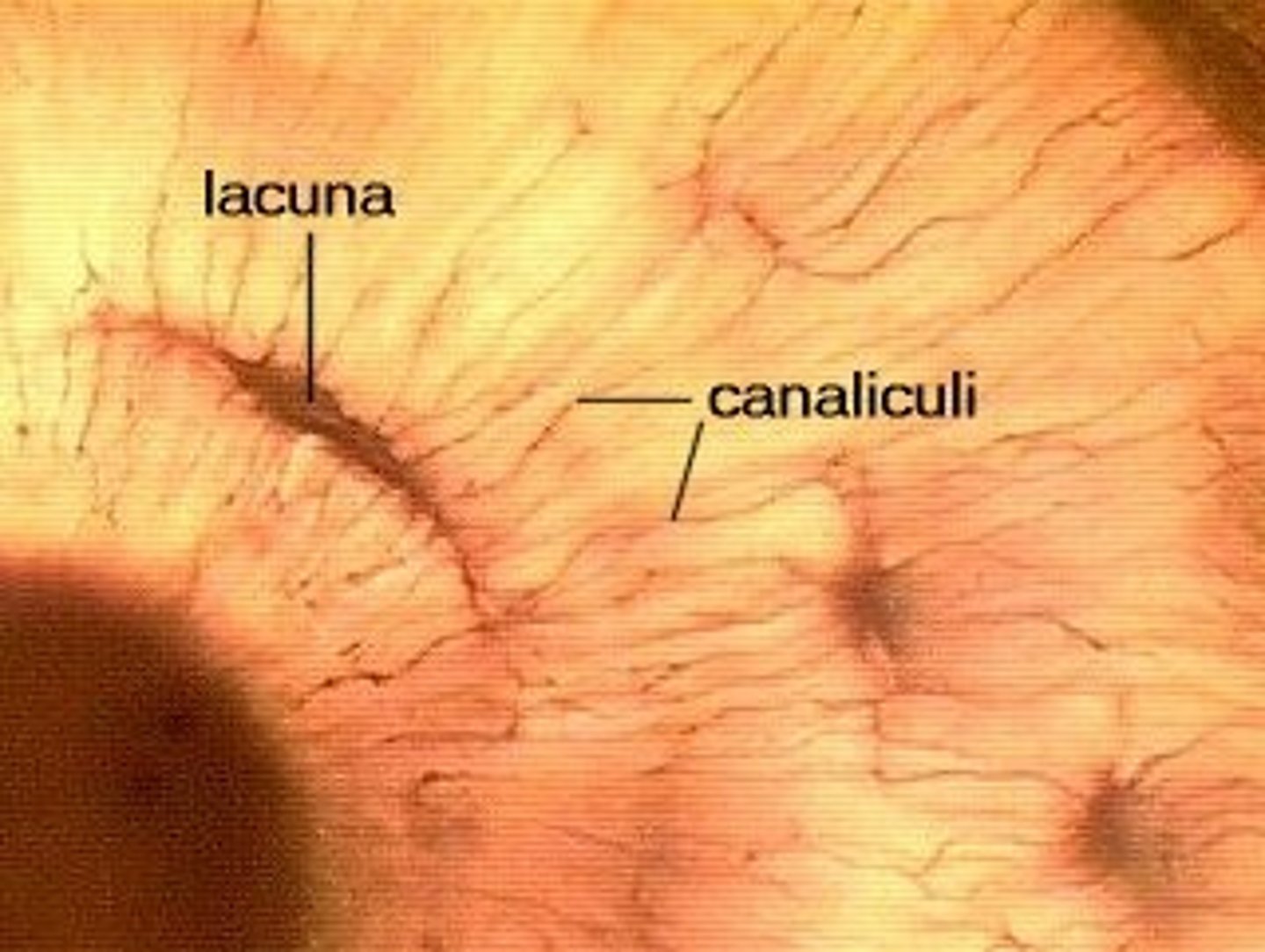
canaliculi
Hairlike canals that connect lacunae to each other and the central canal provides channel for osteocyte communication
haversian canals
blood, lymph and nerve channels
Volkmann (perforating) canals
transverse canals that connect haversian canals
interstitial lamellae
fill spaces between osteons. remnants of old osteons created during remodelling

how does lamellar in bone contribute to bone strength
lamella are organised into different planes to provide increased strength with slippage planes between lamellae to allow some degree of flexion before a bone breaks.
tumours of bone cells. why are they rare but tumours are found in bone
osteosarcomas. tumours of lung and breast frequently metastasize to bone
flat bones
sternum, scapulae, ribs, (most) skull bones, clavicle
irregular bones
vertebrae, bones of pelvis (ileum, sacrum and coccyx but don't form from membranes of mesenchymal tissue), facial bones
long bones
phalanges, metacarpals, femur, humerus
sesmoid bones
patellas
short
carpals, talus, calcaneus
endrochondral ossification
bone is formed from hyaline cartilage template. most bones. ends of long bones remain covered by hyaline cartilage. not covered by perichondrium.
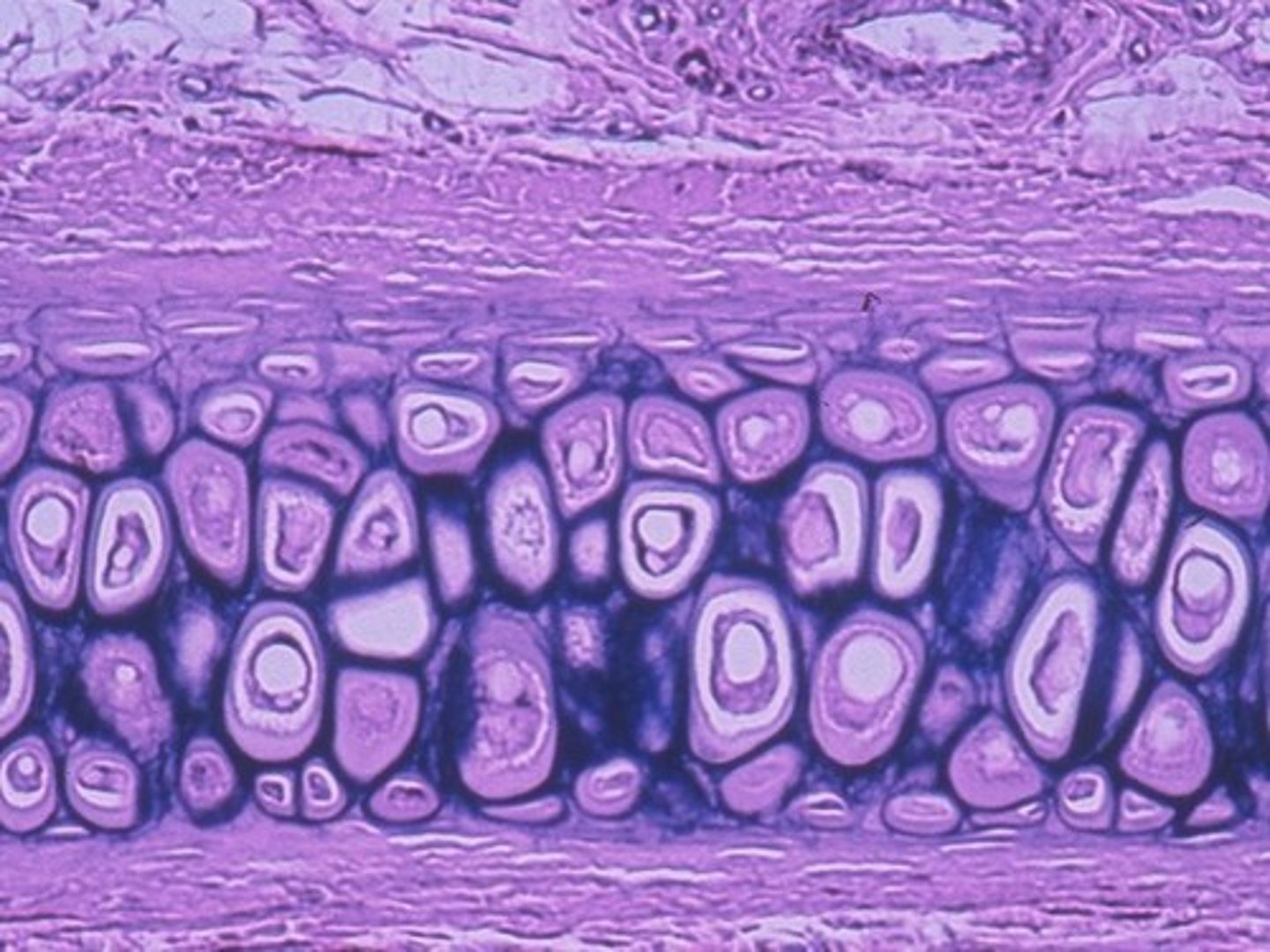
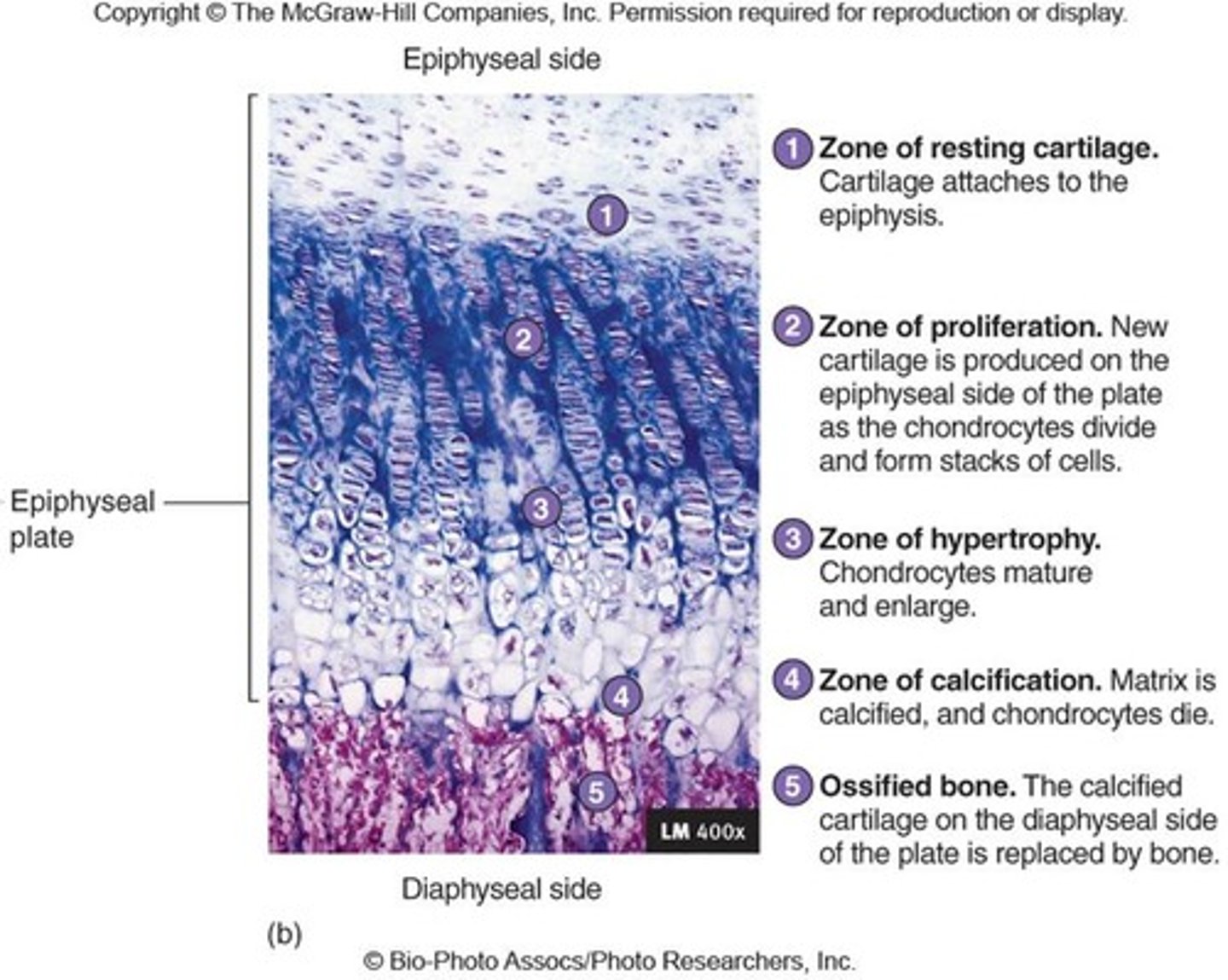
growth at epiphyseal plate
resting chondrocytes proliferate, forming columns. chondrocytes increase in size in the zone of hypertrophic cartilage and begin to calcify. breakdown in zone of cartilage degeneration before osteoblasts recruited to sites of calcified cartilage to begin bone formation (zone of ossification)
Rickets
Vitamin D deficiency in children

achondroplasia
autosomal dominant. lethal in homozygous form. results from mutations in fibroblast growth factor 3 gene. leads to decreased endochondral ossification, reduced proliferation of chondrocytes, decreased cellular hypertrophy and decreased cartilage matrix production. and premature closure of growth plates causing shortened long bones
pituitary dwarfism
diminished stature as a consequence of reduced activity at epiphyseal growth plates resulting from underactive pituitary gland before puberty
lack of growth hormone.
acromegaly
excess of GH post puberty. not gigantism bc growth plates have closed. periosteal growth. appositional. hands and feet are broadened.
Gigantism
a condition produced by hypersecretion of growth hormone pre-puberty.
intramembranous ossification
most flat bones. condensation of mesenchymal CT. begins in ossifications centres where mesenchymal progenitors develop into osteoblasts. secrete osteoid that becomes calcified to form spicules of woven bone
principle component of osteoid
t1 collagen
progenitor are osteoblasts
mesenchymal CT
immediate progenitor cell type of osteoclasts
monocytes. arise from fusion of macrophages
osteogenesis imperfecta
genetic abnormalities in t1 collagen synth. tII may die around time of birth from multiple fractures. legal importance bc confusion with multiple fractures caused by deliberate injury
vitamin d importance
dietary and synth under influence of UV. normal ossification. absence causes poorly mineralised. pliable matrix known as osteoid. bend under body weight. rickets
osteomalacia
adult rickets. vitamin D or calcium deficiency. bone pain, back ache, muscle weakness, increased risk of fracture.
bone become pliable during remodelling. individuals who are unable to go outdoors and whos diet lacks VD.
osteoporosis
more women and elderly ; >50. loss of bone matric and structural density. fractures of spine, hip and wrist. DEXA scan for bone density. post menopausal .
manifestation of achondroplasia
short limbs in proximal, normal trunk, enlarged skull vault, small face. sporadic mutation.
Paget's disease
a bone disease of unknown cause characterized by the excessive breakdown of bone tissue, followed by abnormal bone formation. skull, spine, legs. infection/genetics.
Menisci
flattened, shock-absorbing pads of fibrocartilage between the articulating surfaces of some joints
entheses
where tendons or ligaments join bone. fibrocartilage.
elastic cartilage
matrix comprised of t2 collagen, GAGs and elastic fibres
Fibrocartilage components
matrix t1 and t2 collagen
hyaline components
t2 collagen and abundant GAG for nutrients
proginator cells of cartilage
fibrous outer perichondrium
fracture repair
torn vessels bleed forming a haematoma. clot removed by macrophages ad replaced by a mass of procallus tissue comprised of fibroblasts and collagen. callus invaded by blood vessels and osteoblasts. fibrocartilage replaced by woven bone. woven bone remodelled as compact and spongy bone.
fracture repair type of ossification
endochondrial and intramembranous
osteoclasts
fused macrophages that destroy bone
osteocytes
a bone cell, formed when an osteoblast becomes embedded in the matrix it has secreted. trapped in lucunae
osteoblasts
deposit osteoid
Chondrocytes
Cells that secrete cartilage. trapped in lacunae
compact bone
Hard, dense bone tissue covered in periosteum. osteons. lamellar organisation. t1 and calcium hydroxyapatite.
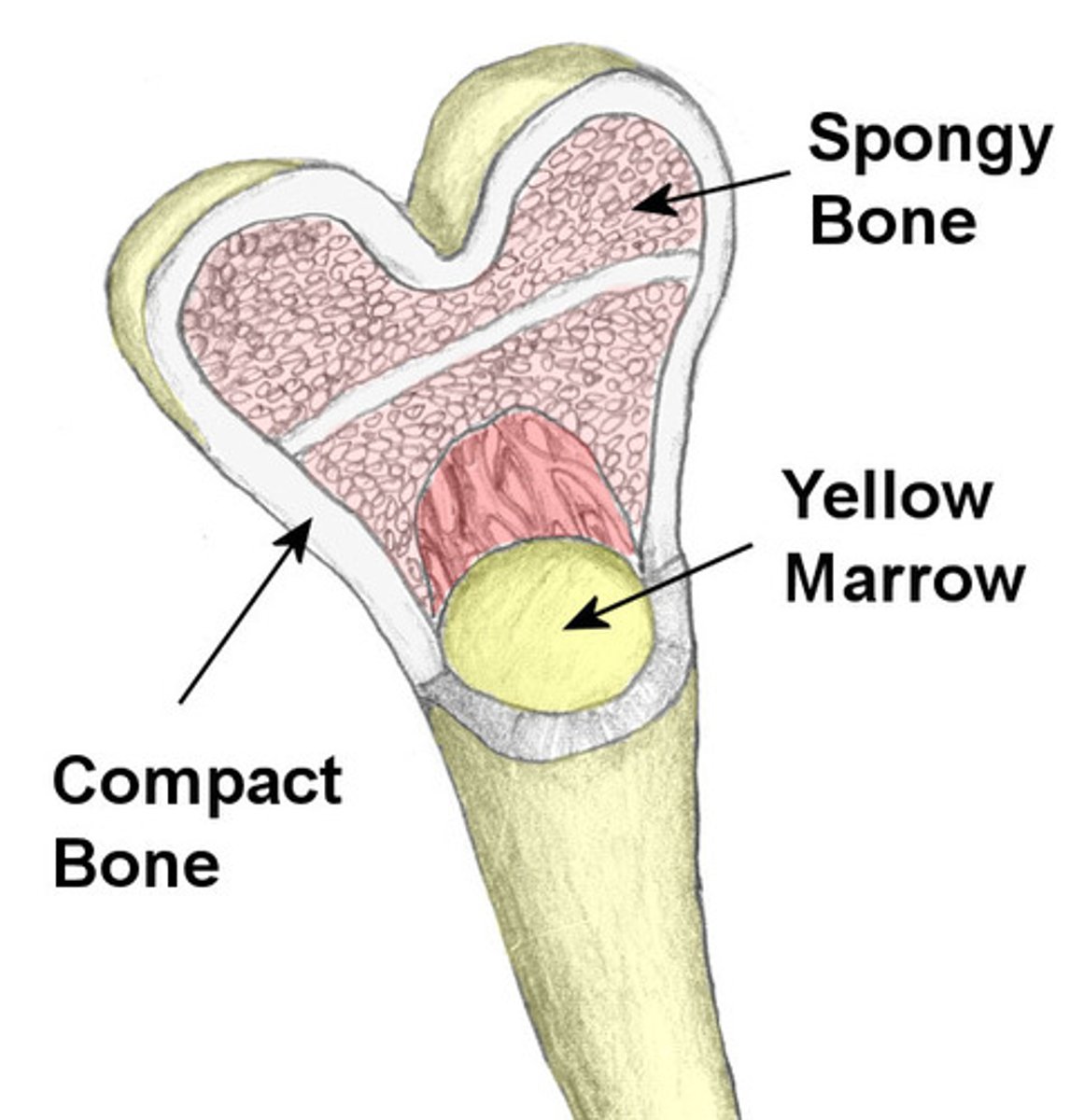
spongy bone
no harversian or volkmanns canals. osteocytes in lacuna between lamellae (more irregular than cortical). remodelling by osteoblasts/clasts located on surface of trabeculae
trabecular organisation; high turnover rate, not covered by periosteum, lamellar organisation, niche for bone marrow, osteocytes in lacunae
how can decalcified bone be stained by h&e
because t1 collagen left behind
reduce of gravitational force on bone
bone reabsorption increases,
bone resist fracture
rigidity and flexibility. lamellae can slip relative to eachother to help disperse forces
sport on bone
hypertrophy of corticol bone
remodelling unit
cutting cone of osteoclasts, reversal zone of containing osteoprogenitors, closing cone where osteoblasts secrete osteoid accompanied by angiogenesis.
gigantism
increased structure as a result of enhanced activity of epiphyseal growth plate stimulated by over active pituitary before puberty
t1 osteoporosis
loss of bone density as a result of overactive osteoclasts following menopause
sex hormones effect on ossification
precocious sexual maturity (can be due to tumour producing growth hormones) retards bone growth because of premature closure of epiphyseal growth plates. if sex hormones are deficient, epiphyseal plates may persist later into life, leading to prolongued bone growth and tall stature.
Osteoporosis t2
loss of bone density due to diminished osteoblast function with age
thyroid hormones on bone
neonatal hypothyroidism: intellectual impairment, short stature. heel prick.
describe bone formation by intramembranous ossification
method by which most flat bones are formed. condensations of embryonic mesenchymal cells at ossification centres. these cells differentiate into osteoprogenitor cells which proliferate to form layer of osteoblasts. secrete osteoid that calcifies to form woven bone, neighbouring ossification centres fuse and undergo mature remodelling to form mature bone
rheumatoid arthritis
can run in families. affects joints of hand and wrist and small joints of feet. systemic causing fatigue, malaise and depression. chronic autoimmune disorder in which the joints and some organs of other body systems are attacked.
Osteoarthritis
inflammation of the bones and joints as a result of cartilage damage. most common. increased risk with obesity. degenerative disorder. knees and hips
endochondral ossification describe process
method most bones esp long bones are formed. takes place within hyaline cartilage. late in first trimester, periosteal bone collar surrounds cartilaginous template causing cartilage to become ischaemic. degenerating cartilage invaded by new blood vessles and osteoprogenitors to create a primary ossification centre, osteoblasts deposit osteoid which undergoes mineralisation. remodelling of the resulting woven bone leads to formation of mature bone, around time of birth, secondary ossification centres form in epiphyses. separate an epiphyseal growth plate which allows the bone to grow until puberty when growth plate closes
what type of bone is disproportionately affected in osteoporosis
spongy
most common fractures in osteoporosis
neck of femur and vertebrae
risk factor in development of osteoporosis
smoking, family history, low dietary calcium intake and mobility
what age does bone mass reach its peak
25-35
secondary osteoporosis
loss of bone density as a result of disease (multiple myeloma) or long term steroid usage
how many genes contribute to development of osteoporosis
polygenic many genes
Bisphosphonates
inhibit bone resorption used in osteoporosis. two phosphate groups that bind calcium ions allowing drug to accumulate at bony surfaces. bisphosphonates taken up by osteoclasts and reduce bone loss by reducing their action.
cell produce ECM
chondroblasts
types of cartilage
hyaline: ECM, proteoglycans. HA. T2 collagen
elastic: similary but elastic fibres
fibrocartilage: similar to hyaline but matrix contains abundant T1 collagen
Describe hyaline cartilage
covered by fibrous perichondrium, except articular surfaces of synovial joints. abundant ECM and t2 collagen which forms fibrils that don't form into fibres. large amounts of HA hyaline is well hydrated. pliant and reliable under pressure. large ration of GAGs to collagen in ECM facilitates diffusion of subtances between chondrocytes and BV surrounding the cartilage.
hyaline cartilage growth
perichondrium allow oppositional growth.
chondroblasts become chondrocytes.
dividing cells form a isogenous group. lay down more territorial matrix and separate leading to interstitial growth. pressure and stress to cartilage creates mechanical, electrical and chemical signals that increase chondrocyte activity.
epiphyseal plate
formed by hyaline. chondrocytes undergo cell division and hypertrophy followed by death and ossification by invading osteoblasts.
Fibrocartilage in intervertebral disc shock absorbing
annulus fibrosus, chondrocytes in lacunae are embedded in large bundles of T1 collagen fibres. more cartilaginous matrix in pubic symphysis or menisci.