Week 6: Addressing fine motor & Visual Motor barriers to occupational performance
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
components of hand skills
•Reach: Extension and movement of the arm for grasping or placing objects
•Grasp: Attainment of an object with the hand
•Carry: Transportation of a handheld object from one place to another
•In-hand manipulation: Adjustment of an object in the hand after grasp
•Bilateral hand use: Use of two hands together to accomplish an activity
•Voluntary release: Intentional letting go of a handheld object at a specific time and place
Factors that contribute to hand development & Function
Hand skills
Social & Cultural Factors
Sensory
Somatosensory functions
Sensory integration
Visual Perception
Musculoskeletal Integrity
Scars/wounds
skin integrity
ROM
Strength, tone
Neuromaturation theory
General sequence of motor milestones; development is pre-programed; motor development driven by the CNS & primitive reflexes considered building blocks of development
Dynamic Systems Developmental Theory
Each child has a unique development trajectory widely influenced by the affordances available in their environment
The Progression of Reach
Once infants can reach, they work on dissociating the 2 sides of their body or unilateral reaching
Bilateral arms movements are the predominant patterns of movement throughout the 1st year of life
They refine unilateral reaching so that they are using less abduction/internal rotation and are doing more purposeful hand opening and begin to use shoulder flexion
Finally, babies are able to reach with trunk rotation, full elbow extension, slight forearm rotation, and wrist stability

Typical Trajectory of Hand Skill Development
Primitive and transitional grasps
Purposeful grasp
Automatic release
Purposeful release
Coordinated bimanual skills
Picture this as a continuum more than a hierarchy
Primitive & Transitional Grasps
Initially the infant’s fisted hand is due to the predominance of physiologic flexor tone that dominates upper and lower extremity movements
In the first week, the grasp reflex has not emerged
Grasping reflex
First seen at week 2-4
Infant will close fingers around an object placed in palm
By week 8 there we see 2 phases of this reflex
Catching phase (immediate flexion of fingers & thumb)
Holding phase
Grasp
The grasping reflex lays the synergistic foundation for grasps. The first grasp to emerge looks like the grasping reflex
Palmar grasp (0-5 mos.)
Fingers flex around object and press into palm
Ulnar palmar grasp
Used to think this came first. Research indicated that index finger is active first
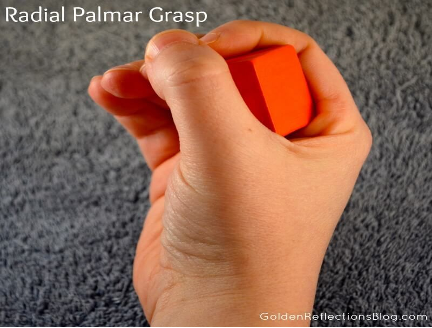
Radial palmar grasp
Fractionated grasp: at 4-6 months one to two fingers begin to flex in isolation from the others
Different types of Grasp
reflexive

palmar

radial palmar
ulnar palmar

Raking Grasp (7-8 months)
vReaching for and grasping a small object using a raking motion
vAll of the fingers flexed at the IP joint
vHand may need support from a solid surface to be successful

Radial Digital Grasp (8-9 months
Thumb opposition to the radial fingers
Object is held proximal to the pads of the fingers with space visible between the object and the palm
Object is held away from the palm, giving the child greater manipulative control. Yet, this grasp is not a fingertip grasp, because the object is held proximal to the pads of the fingers

Inferior Pincer Grasp (8-9 months)
Object being secured between the adducted thumb and radial side of the flexed index finger
The thumb is not opposed, but slides over in a pattern of adduction to trap an object against the side of the index finger

Pincer Grasp (10-12 months)
Object being held between the opposed thumb and pad of the index or middle finger
No longer needs external support to successfully grasp an object

Three Jaw Chuck (10-12 months)
•Thumb opposition to the index and middle fingers
•The object is held at the pads of the index and middle fingers, as well as the pad of the thumb
•The IP joints of the index and middle fingers range from extended to slightly flexed, with flexion of the MCP joints
•To oppose the digits, the thumb rotates and flexes toward the fingertips
•The ulnar two digits do not participate in grasping the cube, but provide support to the radial side of the hand

Automatic Release
Reflexive behavior: Fingers extend as infant withdraws and abducts fingers
Avoiding reaction: When the dorsum of the hand is touched, the fingers abduct and extend

Purposeful Release
Infant transitions from automatic release to purposeful release around 5-6 months
By 6 months, baby can activate release for two-handed play or finger feeding
By 7 months, baby can transfer object from one hand to the other
By 1 year, child can grade hand opening

Evaluation of Hand Skills in Children
Screening for Hand Skill Problems
Evaluation content
Measurement of active and passive ROM
Evaluation of strength
Evaluation of tactile functioning
Assessment of posture
Administration of a standardized developmental test (including motor test, VMI test)
Assessment of hand skills in prevocational and work tasks

Guidelines for intervention
Setting goals: Occupation based; functional goal
Role of OTA: Consider the roles of OT assistant and others in intervention
Preparation:
Positioning the child
Improving postural tone and control
Improving muscle strength
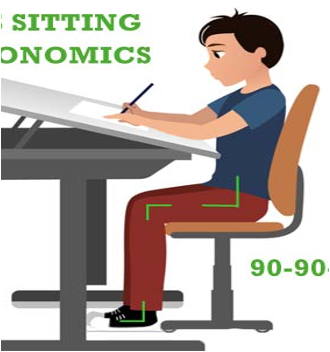
guidelines for intervention: Preparation: Positioning the child
Optimal positioning
Position to facilitate optimal movements
Stable chair with adequate foot support
Appropriate size chair and table for good posture
Adequate support if posture is unstable
Considering standing position while participating in FM tasks

guidelines for intervention: Preparation: Improving postural tone and control
Upper extremity weight-bearing to encourage co-contraction
Weight-bearing in prone position
Use splints during weight-bearing
Pressure on hand/palm to relax or stabilize
guidelines for intervention: Preparation: improving muscle strength
Strengthening programs
Use of neuromuscular electrical stimulation

Intervention: Preparatory Activities
OTs might have the child participate in a variety of preparatory activities
Modulate muscle tone: activities increase, decrease, or balance muscle tone
E.g.s- chair push ups to “wake up” the muscles, slow and rhythmic rocking from side to side (to relax high tone)
Promote proximal stability & strength: activities that encourage stability of joints and strengthening of muscles
E.g.s- animal walks, resistive band exercises, putty exercises
Little evidence to support their use without engagement in occupations
Intervention: biomechanical approach
Primary focus- improve ROM, strength/endurance, postural alignment, joint stability
Beneficial for children with musculoskeletal & neuromotor disorders
Intervention ideas using this model-
Child’s postural stability (standers, wheelchair, side-lying, prone, supine, sitting, standing)
Tools such as grippers, adapted pencils/markers, etc.
Paper positioning/writing surface
Intervention: motor learning approach
Primary focus- to help achieve motor skills through practice, and experience
Beneficial for any child who can follow instructions & engage in repetitive practice
Examples of intervention techniques typically used using this model-
Practice, mental rehearsal, feedback, reinforcement, error based learning
P-CIMT
Research connection
Evidence shows that children with DCD, CP and adults with brain injury benefitted from intervention that specifically used motor learning approach (Ketelaar, M., Vermeer, A., Hart, H., et al. (2003)
Since 2000, >50 studies published on the effectiveness of P-CIMT
Evidence shows positive effects on hand function for children with unilateral CP
Intervention: sensorimotor approach
Primary focus- to enhance and reinforce motor learning by providing multisensory input through selected activities
Beneficial for any child who may not be motivated or frustrated trying to learn a fine motor skill
Examples of intervention techniques typically used using this model-
Writing tools (e.g. felt-tip pens, scented crayons/markers, paintbrush, weighted pencil, vibratory pens, etc.)
Raised lines or colored lines, thick margin on L side, etc.
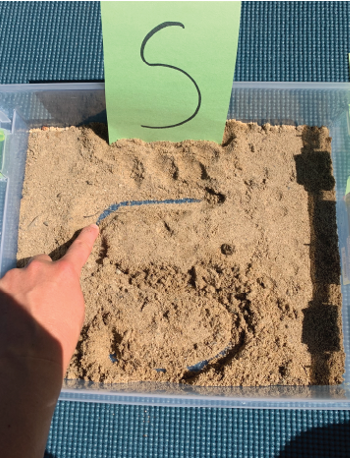
Practice writing on shaving cream, food, paint, etc
Research connection
Not enough evidence demonstrating improved hand skills using sensorimotor approach
One study showed that children demo. improved handwriting performance with repetitive practice compared to sensorimotor interventions (Denton, P., Cope, S., & Moser, C., 2006)
Intervention: cognitive approach
Primary focus- to facilitate motor skill acquisition using highly individualized problem solving techniques
Beneficial for any child with cognitive limitations (however not limited to that!)
Examples of intervention techniques typically used using cognitive approach:
Using mask to uncover 1 line at a time during FM task, pneumonic, colored lines, one finger space, tongue depressor, etc.
Research connection
Cognitive strategies shown to improve handwriting when combined with “therapeutic practice” (Candler, 2019)
Hand function & writing
Based on the progression of grasps, there are 6 underlying components of handwriting
Upper extremity support
Wrist stabilization
Open and stable thumb web space
Stable arches of the hand
Radial-Ulnar dissociation (Separation of 2 sides of the hand)
Precise in hand manipulation
Upper Extremity support
Upper extremity support is required for handwriting because the proximal stability of the trunk, shoulder, elbow, and forearm allows the wrist and fingers to engage in tasks that require precise dexterity
Proximal stability/support promotes distal mobility/function
Wrist stabilization
Wrist position influences the position of the joints of the fingers and thumb, as well as overall performance
Optimal wrist posture for precise finger movements:
Neutral with slight wrist extension
Being able to maintain slight extension and a position in neutral allows the thumb to be aBducted and opposed to the fingers
Activities to facilitate wrist stabilization
Games that promote wrist strengthening like “Restaurant game”
Fun Gross motor exercises like “animal walks”
Using Vertical surfaces to promote wrist extension
Using toys and games promoting wrist extension such as “Ants in the Pants”
Functional activities such as help clean vertical surfaces or wipe whiteboard
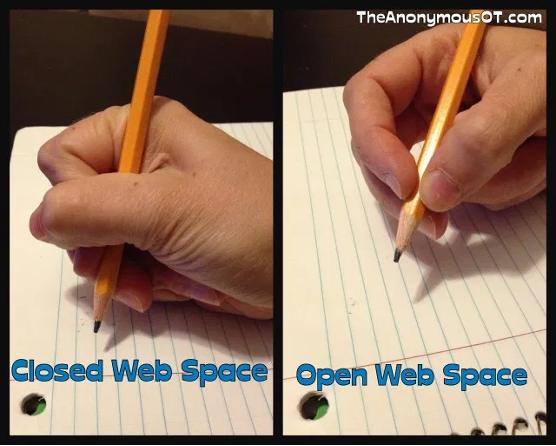
Open & stable thumb web space
Point to your web space
This looks like the a-OK sign
An open web space allows for thumb and finger opposition
A stable open web space allows for optimal manipulation of objects
Hold your pencil as you normally do
Is it resting in you’re a-OK space?
If it is, you might be writing with a “closed” or “semi-closed” web space
vFM Activities to facilitate open webspace:
Beading Activities
Finding beads in putty
Threading beads
Lacing activities
Tweezer activities
Puzzles (Pegboard)

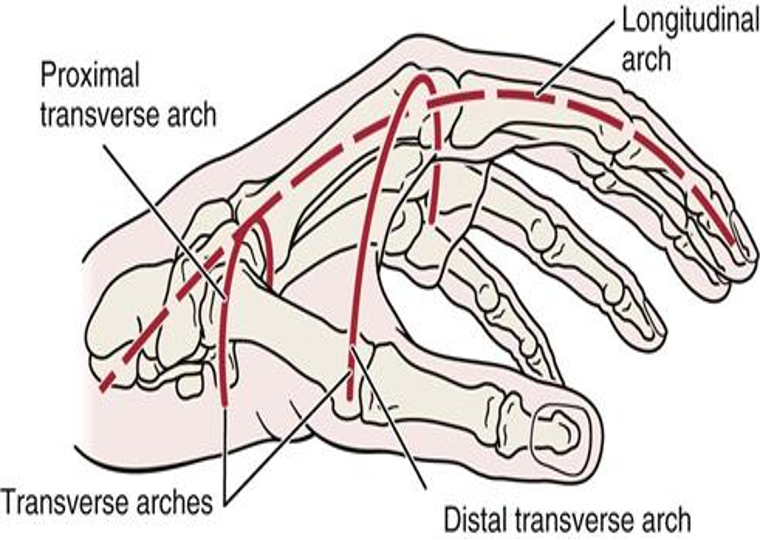
Arches of the hand
Grasp depends on the integrity of mobile units of the arches
The structure allow for the flattening & cupping of the hand
Longitudinal arch: wrist to fingers
Distal transverse arch: along the metacarpals of the digits
Proximal transverse arch: along the wrist
The thenar & hypothenar eminence use the instrinsic muscles for cupping & arching
Underdeveloped arches could impact mobility- lead to decreased function
Activities to improve arch development:
Activities that facilitate intrinsic muscle strengthening such as playing with tongs
Squirt toys
Construction play such as playing with Legos
Playing with squish balls/hand fidgets

Radial-Ulnar dissociation
Radial-Ulnar dissociation is required for precise movements
Stability of the ulnar fingers allows for manipulation of objects with thumb & radial fingers
Ulnar digits assist with power
Radial digits are stabilized by ulnar digits for precise handling

Activities to facilitate radial-ulnar dissociation:
Squeeze spray bottle with 2nd and 3rd digits only
Games like “feed the frog” with waterbeads, cereal, coins, etc.
Hold on to a small object with last 2 digits while coloring
Tearing paper
Playing games like “Lite Bright” puzzles
Games like finger puppet or finger soccer
Playing with stickers

In-hand manipulation
Handwriting also depends on precise in-hand manipulations
It’s the adjustment of an object in the hand after grasp

Activities to facilitate in-hand manipulation:
Activities facilitating translation (palm-to-finger and vice-versa)
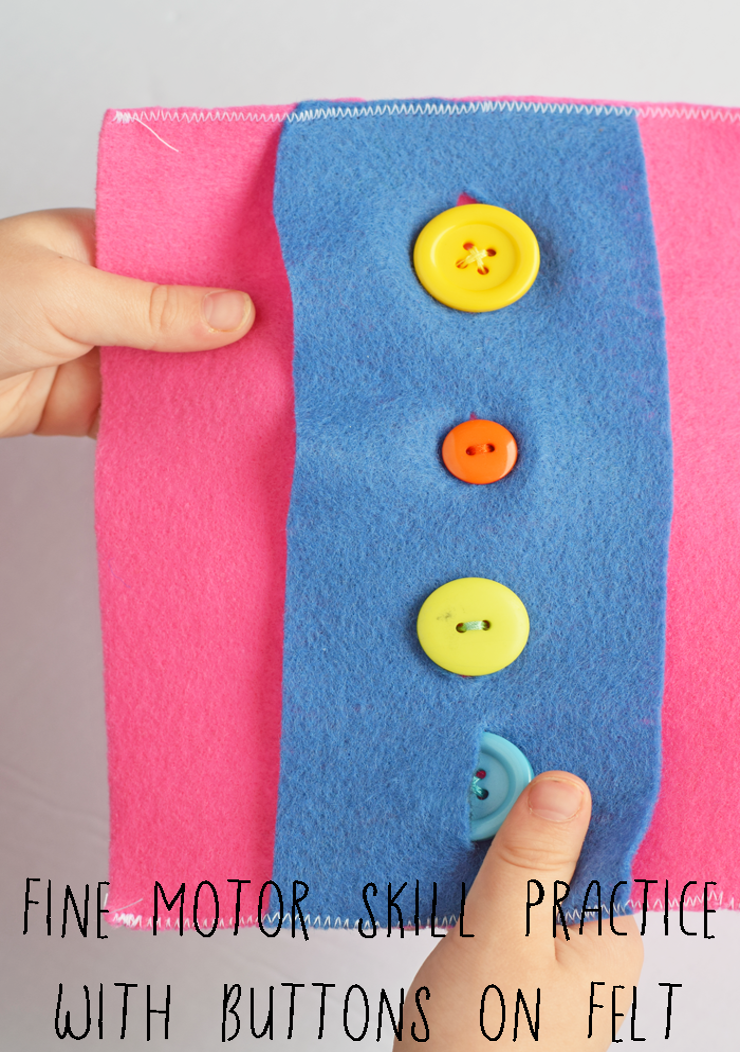
Activities facilitating shifting of fingers manipulating fasteners
Activities facilitating rotation such as flipping crayons for a different color, rotating bottle top
Handwriting grasp: primitive
Before 3 years
Pencil in palm, 5 fingers
Movement generated more from shoulder/elbow (whole arm movements)
Handwriting grasp: transitional
Between 3-6 years
Pencil held more distally (with less control)
Movement generated more from elbow/wrist (forearm movements)
Handwriting grasp: mature
After 6 years
Only using 3-4 fingers
Clear radial-ulnar dissociation
Movement generated more from wrist/fingers
OT’s Role in Supporting Handwriting Skills: Foundational Readiness Skills:
Postural stability, shoulder control
Fine motor skills (grasp, dexterity, bilateral coordination)
Visual-motor integration
Sensory processing (tactile, proprioceptive input)
OT Programs Used:
Learning Without Tears (previously referred to as HWT)
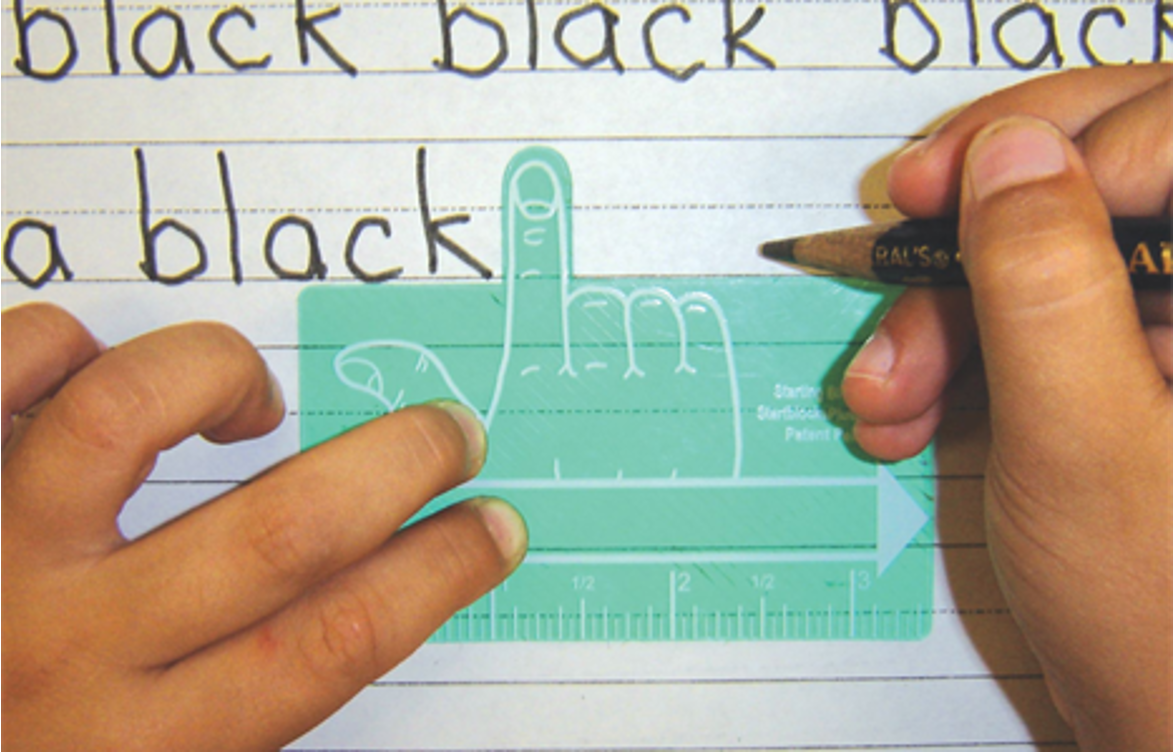
Size Matters
Common OT Interventions: (IMP TO KNOW WHERE TO START)
Play-based tasks, vertical surface work, tactile exploration
✏ Pre-Writing Skills: start here!
Vertical → horizontal → circle → cross → square → diagonal → triangle
Tools: dry erase boards, sensory bins, Roll-A-Dough letters
🔠 Uppercase First:
Easier due to uniform size, starting points
Focus on stroke sequence (top to bottom)
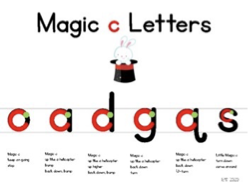
🔡 Lowercase Letters:
Taught in formation groups (Magic C, tall, short, fall)
Tools: use lined paper & visual supports
📝 Word & Sentence Formation:
Emphasize spacing, alignment
Scaffold: copy → dictated → original writing
🔄 Functional Goals:
Speed, legibility, and endurance
Use assessments, introduce AT if needed
OT’s ROLE: Enhance Visual Efficiency and information processing through structure visual tasks
Vision Components:
Refraction:
Eye Health of structures
Visual efficiency
Oculomotor
Fixation
Smooth Pursuits
Saccades
Accommodation
Sustain/Change Focus
Binocularity
Convergence
Divergence
Visual processing
Discrimination
Closure
Figure Ground
Spatial Relations
Memory
Comorbidities
•Cerebral palsy
•Neurological insults or brain abnormalities
•Chromosomal abnormalities and genetic conditions
•Learning disabilities
•Cognitive impairments
•Prematurity and developmental delays
•Fetal Alcohol Syndrome
•ADD/ADHD
•Autism
•Sensory Processing Disorder
•Cortical Visual impairment
•CHARGE syndrome
Development of Visual Motor Integration (VMI)
•3 Months- Track rattle while lying on back
•6 Months- Extends arm to reach for the rattle
•9 Months- Move towards and reach for toy
•12 Months- Pick up and place cheerios
VMI is a specific motor skill that allows for coordination of visual input with a corresponding motor response
Development of Prewriting
Scribbles on paper | 10–12 months |
Imitates horizontal, vertical, and circular marks | 2 years |
Copies vertical and horizontal lines and circles | 3 years |
Copies cross, right oblique line, diagonal left oblique cross, some letters and numerals; may write own name | 4–5 years |
Copies triangle, prints own name, copies most lower and uppercase letters | 5–6 years |
writing skills Development
Pre-K to 5th grade
Progression from LARGE to small
Progression from straight to curvy
Speed is a combo of motor skills and cognition
Progression from imitate, copy, draw from memory
Measuring Handwriting Performance
domains of handwriting
legibility
writing speed
ergonomic factors
Domains of handwriting
•Near-point copying
•Far-point coping
•Writing dictated words
•Composition
•Writing alphabet
•Legibility
•Alignment
•Spacing
•Size
•Readability
•Letter formation
vWriting speed
•Number of words per minute
•Consider within context of classroom, assignment, child
•Ergonomic factors
Posture
•Upper extremity stability
•Mobility
•Pencil grip
Assessments
•Beery VMI
•DTVP-3
•BOT-2
•TVPS-4

BOT-2
Fine Motor Precision
Fine Motor Integration
Handwriting Components
Legibility
Baseline Orientation
Alignment
Spacing
Size
Slant
Collaboration with Developmental Optometrist.
Role of OT
Screen for Visual Deficits
Refer to vision care Specialist for Evaluation and Diagnosis
Child may be recommended for Vision Therapy
OT can then develop appropriate compensatory & instructional strategies to facilitate access to school curriculum
Intervention: Oculomotor Skills
Central/Peripheral Vision, Pursuits, Saccades
Flashlight tag
Alphabet Tracking
Reading
Mazes, Connect the Dots.
Where’s Waldo/ I Spy
Consider use of equipment
Mirror
Distance
Spacing

Retained Asymmetrical Tonic Neck Reflex
Poor Reading Comprehension
Poor Visual Tracking & Eye Pursuits
Poor Handwriting
Poor Hand Eye Coordination
Poor bilateral coordination
Writing compensations: tight pencil grasp, turning paper, decreased fluency, extended arm, writing w/ slant, letter reversals
Intervention: Eye patching to improve Oculomotor Skills
Common treatment for Lazy Eye (Amblyopia)
Rec. 2-6 hours

Intervention: Oculomotor Skills: Marsden Ball
Intervention: Accommodation
Highlights – Find it
Spot it
Copying from the Board
Zingo
Shape Sorting Games
Stack and Sort Board
Bean Bag Toss
Any Reaching/Put in Task
UNO
Spot THE DIFFERENCE

Intervention: Eye Teaming
Consider Laterality, Bilateral Coordination, Convergency/Divergence
Pen in Cap game
Paper tearing
Arm and leg raises
Arrow Chart
Scissor Skills
Zoom Ball

Visual Perception Impact from Cortical Visual Impairment
Decreased Visual Attention and Visual Recognition
Decreased ability to use central vision
Compensation with Peripheral Vision
Drawn to bright lights
Prefer Objects Close to Face
Visual Motor Skills: Typing
•Text to Speech
•Electronic spell check
•Picture supported text
•Abbreviated expansion
•Word prediction
•Voice recognition software
•Large Print
•Zoom
•Display
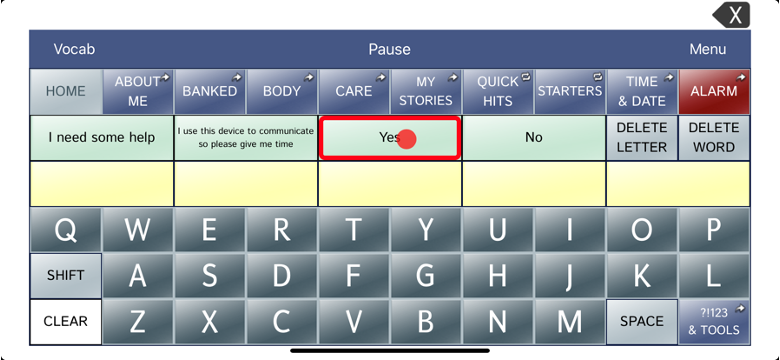
Visual Motor Skills: Alternative and Augmentative Communication Devices
•Use of Keyguard
•# of icons per Page set
•Visual Feedback
•Display Contrast
•“Masking”
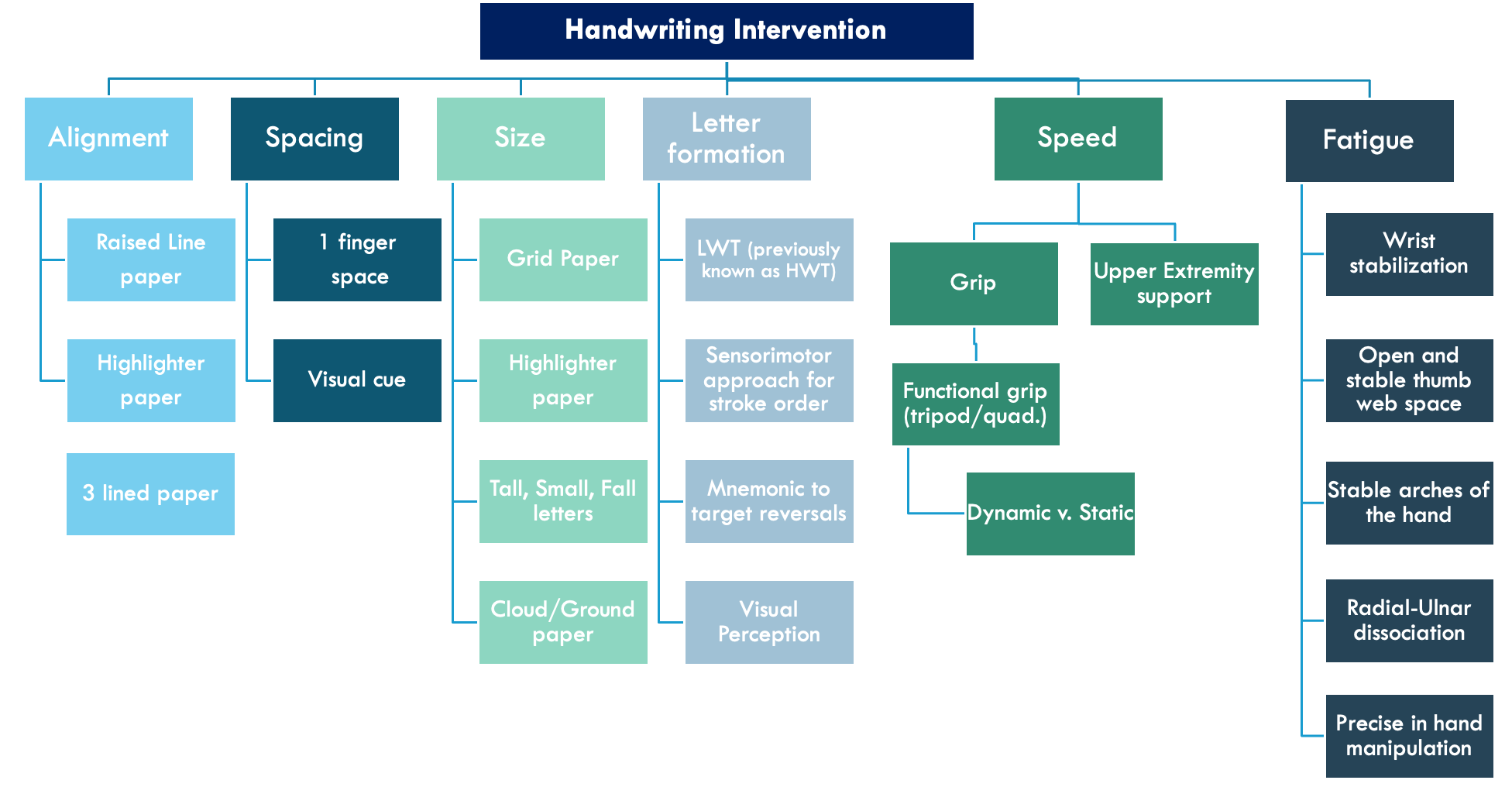
Key take away message
diff types of handwriting intervention
Intervention: Vision + Vestibular Systems
