Non-communicable diseases (NCD)
1/30
Earn XP
Description and Tags
Week 6
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Define non-communicable diseases (NCD)
Diseases that are non-communicable - meaning that the disease is not transmittable from one person to another.
Sometimes referred to as silent diseases as there are no clear signs of developing the disease. Typically first discovered when the disease is presents - especially in low-income countries where they do not screen.
Many NCDs are chronic - but not all!
NCDs include a wide range of diseases!
external causes: injuries, poisonings ect.
Mental disorders - including dementia
Systemic diseases: diabetes, cancer, CVD, kidney and respiratory diseases
What are the four main NCDs?
Hypertension and other cardiovascular diseases (CVDs)
Cancers
Chronic respiratory diseases
Diabetes
What is a communicable disease?
Infections - A disease that can be transmitted from one person to another.
Disease is directly due to the action of a communicable agent.
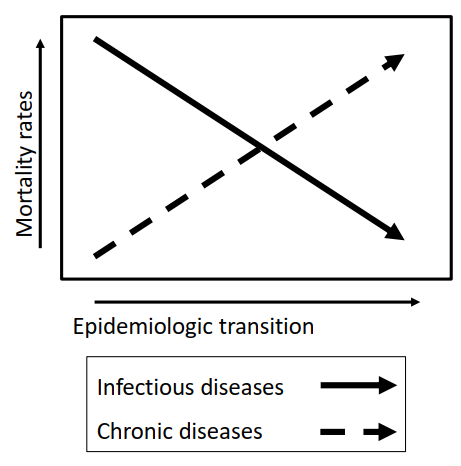
Explain the epidemiologic transition - regarding motality rates between the infectious and chronic diseases
Motality rates of infectious diseases decrease and chronic disease motality rates increase.
But it is important to remember that these two interact. Bidirectional connections can be seen between many infections and NCDs - meaning that one can cause the other in both directions.
Describe and discuss the impact of physical activity on development of NCD in low-income settings
Physical activity has a preventative effect on the development of NCD - among many reasons:
Insulin sensitive tissue
Possibility to change body composition
Helps maintain energy balance
Discuss the impact on the development of NCDs:
Decrease in physical activity due to (likely because motorbikes available, more sedentary jobs, bad infrastructure and no green areas ect.)
Physical activity may be a more feasible way to intervene and prevent NCD rather than diet because:
Changes in diet can be impossible due lack of other food choices or economy.
Describe and discuss the impact of nutrition on development of NCD in low-income settings
Malnutrition early in life affects development of NCD:
A diet can be nutrient poor but energy dense – thereby inducing overweight and malnutrition at the same time. Evident as an adequate BMI but a poor body composition (bad bone and muscle development/health).
Both over- and under-nutrition can lead to NCDs
Globally over-nutrition is a larger problem compared to under-nutrition.
Malnutrition and lack of important nutrients impacts development of NCDs in many ways:
Immune function
Reflect on the challenges related to obtaining evidence on the aetiology (cause) of NCDs
NCDs are multifactorial diseases:
So many different factors can influence the development of NCD. There is not one single cause that can be attributed the cause of NCD these diseases are multifactorial.
Develops over time:
NCDs can take a long time to develop – to explore the cause we would need to follow a person/population for a very long time which is really expensive and resource demanding
Issues in studies of NCDs
Recruitment issues in low-income countries:
The control: if controls a those who receive standard care – the standard care can be very different from community to community and sometimes no care is available
Infrastructure:
There can be long distance between clinics or homes in studies. In low-income countries infrastructure is often not very good. This makes it hard for participants to reach clinics or hard for investigators to reach their homes or clinics. Furthermore, if samples need to be transported it can be hard also keeping samples on -80 degrees which is often required.
Name some of the behavioral risk-factors often shared between NCDs
The behavioural risk factors are also the modifable risk factors. These include:
Tobacco
Alcohol
Inactivity
Diet
Name some of the metabolic risk-factors often shared between NCDs
The metabolic risk factors are like the behavioral modifiable.
These include:
Blood pressure
Weight
Blood glucose
Name some of the non-modifiable risk-factors often shared between NCDs
Age, gender and genetics
Mention risk factors for NCDs that are more prominent in low-income countries compared to high-income countries
Generally NCDs in low-income settings are often related to exposure to under-nutrition and infections (HIV, malaria).
These are both risk factors that are more prominent in low-income countries compared to high-income countries.
What is the relation between foetal environment and the environment exposed to to in later life?
Mismatch between foetal environment and environment living in as an adult increase the risk of T2D.
Staying in the same environment decrease the risk.
The change in environment can happen because of two reasons:
Moving
Change of an environment: ex urbanization of a rural area.
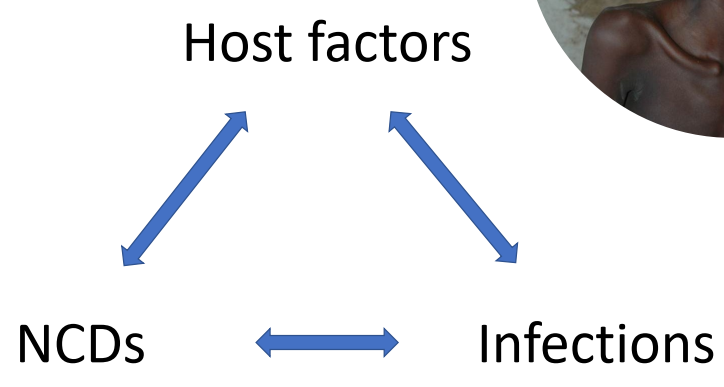
In low-income countries non-communicable disease and communicable diseases are present at the same time in these populations and often also at the same time in the same individual. For example tuberculosis and diabetes that persists in the same individual.
What term can be used to describe this?
Double-burden of disease
In societies in fast transition, there may be a high burden of both simultaneously, a double burden
Mention some underlying causes of malnutrition in low-income settings
Poor health care infrastructure
Lack of education about hygeine and poor hygeine in general
Inadequate access to health care
Infections (often as a consequence of poor hygeine)
What can the long-term consequences of child malnutrition be?
· At risk of not meeting their developmental potential
· Despite nutritional recovery, malnutrition leads to impaired attention, school performance, lower education, and income levels as adults
Malnutrition as an adult
Which is currently a larger global health burden: overnutrition or undernutrition?
Globally, overnutrition is a larger burden than undernutrition. However, undernutrition is still a major global health problem. Be aware, that under- and overnutrition can co-exist.
What is the purpose of psychosocial stimulation in the care of children with severe acute malnutrition?
Malnourished children often lack opportunities for play, interaction, and emotional support, which are crucial for their cognitive and emotional development. Stimulation—like play, interaction, and responsive care—can improve recovery and development outcomes in malnourished children.
Mention some study challenges related to obtaining evidence in low-income settings
· Recruitment bias
o Only few SAM cases at clinics – clinics may not see enough cases making it difficult to recruit enough participants
o Many children may not make it to the clinic – they could be left untreated in the community and may lead to underrepresentation of the true disease burden
· Quality of care
o Inconsistent standards of care: The quality of medical care varies greatly across different facilities—some may follow proper protocols, while others lack treatment options entirely. Affect generalizability of outcomes.
o No treatment available
· Study logistics
o Multiple clinics involved – adds complexity in ensuring consistent protocols
o Long distances, congested roads – transportation can be slow and difficult causing delays in sample collection, patient follow-up etc.
o Some studies require biological samples that must stay cold. Maintaining a cold chain in hot, remote settings can be difficult.
Define physical activity and give some examples
Physical activity is any body movment that works your muscles and uses more energy than you use when you are resting
Walking
Swimming
Define exercise and give some examples
Exercise is a type of physical activity that are structured and planned
Lifting weights
Sports games
Badminton
Swimming
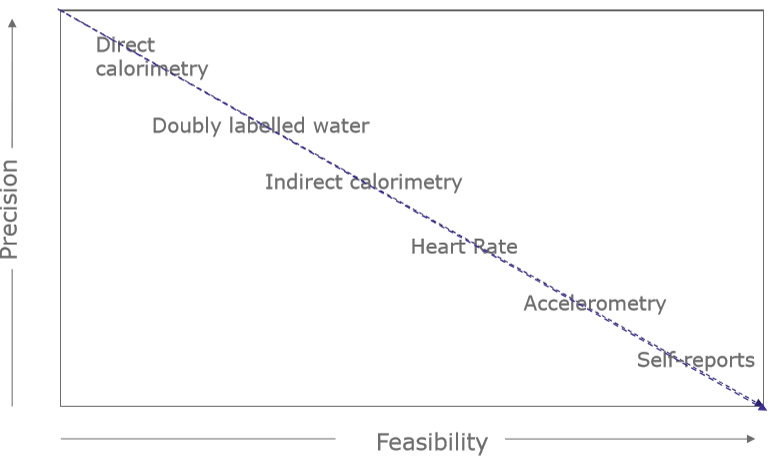
Estimating PA in population-based studies is a trade-off between feasibility and precision. Mention some methods in each end of these “scales” - which methods are precise but not that feasible in population based studies and opposite?
Feasible: self-reported questionnaires on PA, heart rate measures etc.
Precise: doubly labelled water and direct calorimetry.
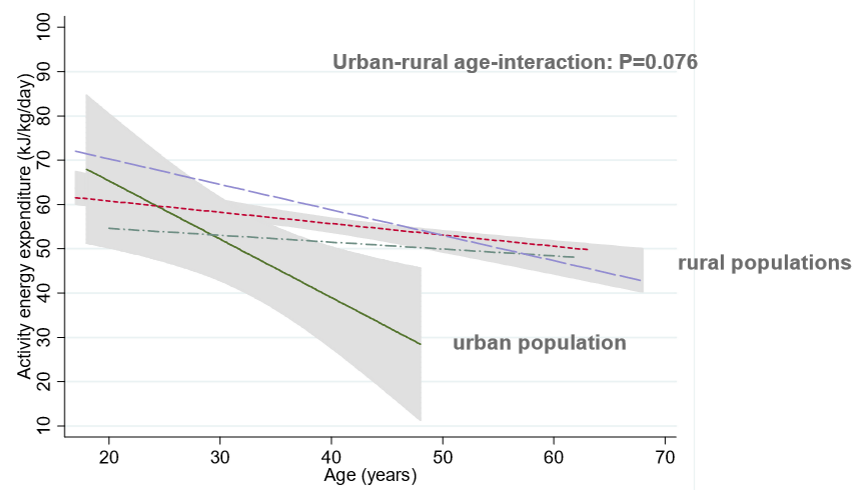
Explain the global variation in energy expenditure (EE) from physical activity?
According to:
Age: young vs. old individuals
Residence: urban vs. rural
Age: Young people have a higher EE from physical activity compared to older.
Residence: Individuals living in rural areas have a higher EE from physical activity compared to individuals living in the urban areas.
Explain why there are a different in EE from activities between contry side and urban in low income contry.
In low income contry the reason why people in urban area are less activ is dou three factores:
They have less time in the day
More acces to poplic transport
The infrastructure
Not safe to be in the traffic
Less green areas
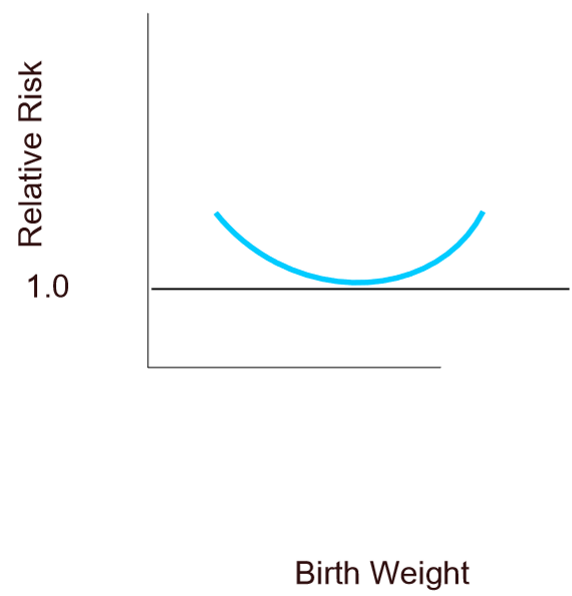
How is birth wieght influencing the risk for develop NCDs?
There are challenges/risks at both ends of the normal distribution of birth weight but:
The lower the birth weight, the higher the risk of developing NCDs.
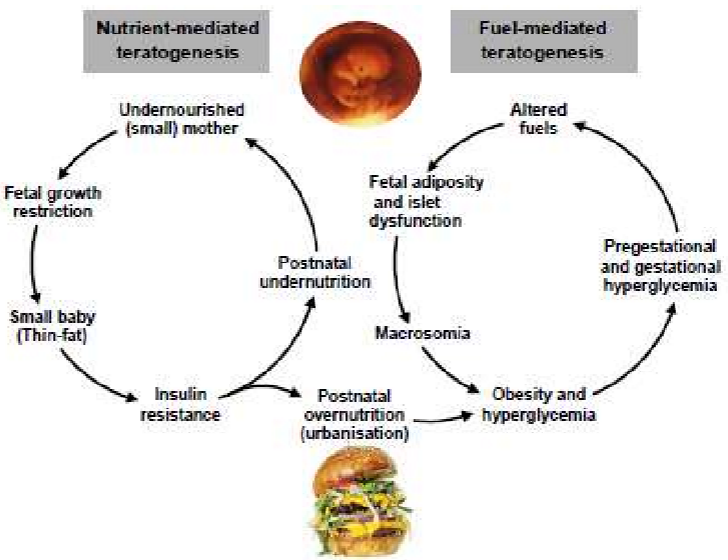
Explain the consequensesog maternal under- and overnutrition on featal programing.
If the mother is small (undernutrition) and she get pregnet with a girl baby, the girl baby will have a low birth weight. When she is get pregnet her baby will have high birth weight.
Low birth weight affect body composition and an antropometric later in life - which?
Height and lean mass
Low birth weight increase the risk of lower values in these two measures later in life.
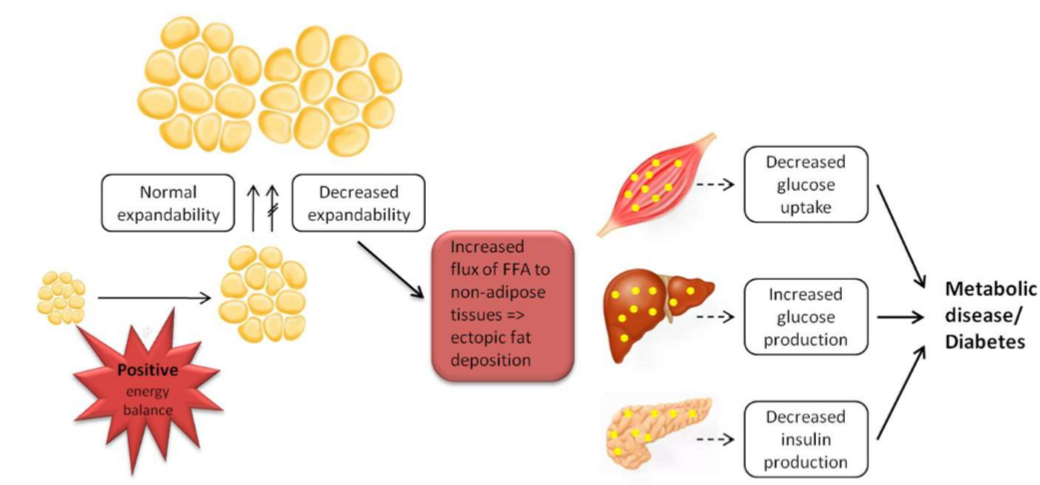
Explain the adipose tissue expandability hypothesis.
When adipose tissue has the capacity to expand and store fat safely, metabolic complications are minimized. However, if this capacity is exceeded, excess fat spills over into non-adipose tissues.
A positive energy balance lead to increased fat mass and at some point the adipose tissue is no longer able to expand → the extra fat will be stored in non-adipose tissues e.g. muscle, liver and pancreas → increase insulin resistance→ lead to metabolic diseases e.g. T2D and CVD
How is physical activity intensity (in MET) distributed in low-income countries (Kenyan)?
Most women and men (58%) are at low/moderate intensity (1.5 MET) for longer times rather then being physically active at higher intensity (3.5 MET) in a shorter time (11-13 %).
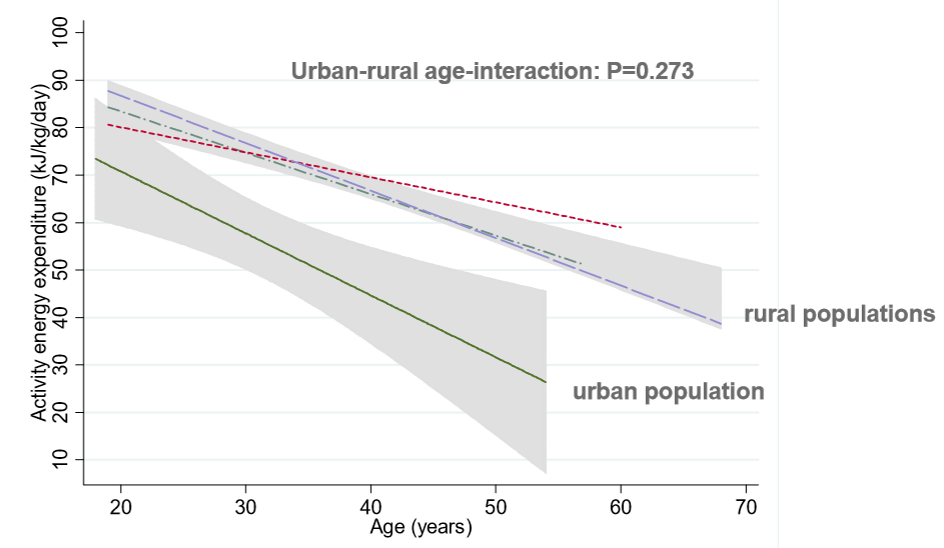
How is the relationship between age, residence (urban vs. rural) and EEPA for women?
There is a decrease in EEPA in relation to age development independent of where they live.
The variation of EEPA is large between those who live in the urban areas and those who live in in rural areas.
Urban - large variation in EEPA and a faster/steeper decrease in relation to age development.
Rural - small variation in EEPA and slower decrease in relation to age development
How is the relationship between age, residence (urban vs. rural) and EEPA for men?
There is a decrease in EEPA with advancing age independent of where a person live.
The variation in EEPA is large between those who live in urban areas vs. rural areas.
Urban - large variation in EEPA and a faster decrease in relation to age development.
Rural - small variation in EEPA and slower decrease in relation to age development
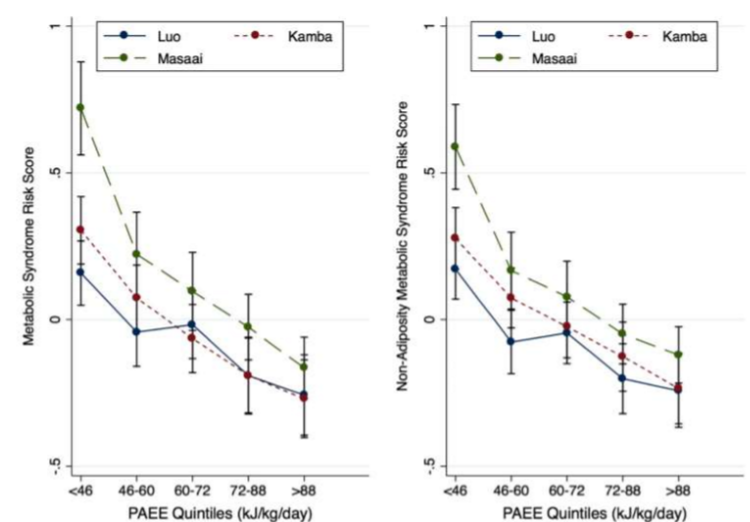
How does EEPA influence the risk of cardio-metabolic health?
Higher EEPA lowers the risk for developing metabolic syndrome and non-adiposity metabolic syndrome.