[TOXICOLOGY] Common Major Pathophysiologic Mechanisms
1/85
Earn XP
Description and Tags
Proverbs 16:3
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
d. respiration → o₂ transport → cellular respiration
[INTERFERENCE WITH O2 UTILIZATION]
In normal physiology, oxygen follows which correct pathway?
a. respiration → cellular respiration → o₂ transport
b. o₂ transport → respiration → cellular respiration
c. cellular respiration → respiration → o₂ transport
d. respiration → o₂ transport → cellular respiration
d. glycolysis → kreb’s → etc
[INTERFERENCE WITH O2 UTILIZATION]
Which sequence correctly represents cellular energy production?
a. kreb’s → glycolysis → etc
b. glycolysis → etc → kreb’s
c. etc → glycolysis → kreb’s
d. glycolysis → kreb’s → etc
b. atp, co₂, water
[INTERFERENCE WITH O2 UTILIZATION]
The final products of cellular respiration include:
a. oxygen, glucose, water
b. atp, co₂, water
c. protein, co₂, oxygen
d. glucose, atp, nitrogen
a. complete combustion of fuel
[INTERFERENCE WITH O2 UTILIZATION]
Carbon monoxide is commonly produced from:
a. complete combustion of fuel
b. incomplete combustion
c. cellular respiration
d. photosynthesis
b. inhibition of cytochrome oxidase
[INTERFERENCE WITH O2 UTILIZATION]
The main mechanism of toxicity of carbon monoxide is:
a. activation of cytochrome oxidase
b. inhibition of cytochrome oxidase
c. stimulation of ATP production
d. increased oxygen diffusion
c. cherry red skin
[INTERFERENCE WITH O2 UTILIZATION]
A classic sign of carbon monoxide poisoning is:
a. cyanosis
b. jaundice
c. cherry red skin
d. petechiae
a. vertigo and headache &
c. pallor
[INTERFERENCE WITH O2 UTILIZATION]
Which symptom is commonly seen in early carbon monoxide poisoning?
a. vertigo and headache
b. abdominal rigidity
c. pallor
d. nausea and vomiting
c. hemoglobin
CO + Hgb → methemoglobin (↑affinity to O2) = hypoxia
[INTERFERENCE WITH O2 UTILIZATION]
Carbon monoxide causes hypoxia mainly by binding to:
a. myoglobin only
b. plasma proteins
c. hemoglobin
d. albumin
b. o₂ supplementation
[INTERFERENCE WITH O2 UTILIZATION]
First-line management of carbon monoxide poisoning includes:
a. vitamin k administration
b. o₂ supplementation
c. activated charcoal
d. dialysis
b. hyperbaric oxygen therapy (100% O2)
[INTERFERENCE WITH O2 UTILIZATION]
Definitive treatment for severe carbon monoxide poisoning is:
a. hemodialysis
b. hyperbaric oxygen therapy
c. bronchodilators
d. corticosteroids
c. blocking cytochrome and oxygen utilization
[INTERFERENCE WITH O2 UTILIZATION]
The main mechanism of toxicity of hydrogen sulfide is:
a. stimulation of cytochrome oxidase
b. blocking oxygen transport in blood only
c. blocking cytochrome and oxygen utilization
d. increasing ATP production
a. hot springs odor &
b. rotten egg odor
[INTERFERENCE WITH O2 UTILIZATION]
Hydrogen sulfide is commonly described as having a:
a. hot springs odor
b. rotten egg odor
c. ammonia-like odor
d. odorless gas
b. highly toxic and colorless
[INTERFERENCE WITH O2 UTILIZATION]
Hydrogen sulfide is best described as a gas that is:
a. colored and non-toxic
b. highly toxic and colorless
c. mildly toxic and colored
d. only toxic when dissolved in water
b. irritation of mucous membranes and respiratory depression
[INTERFERENCE WITH O2 UTILIZATION]
A key effect of hydrogen sulfide exposure is:
a. increased liver enzymes
b. irritation of mucous membranes and respiratory depression
c. renal failure only
d. increased hemoglobin production
b. sulfmethemoglobin
Methemoglobin + Sulfide Ion → Sulfmethemoglobin + hypertonic O2
[INTERFERENCE WITH O2 UTILIZATION]
In hydrogen sulfide toxicity, methemoglobin reacts with sulfide ion to form:
a. carboxyhemoglobin
b. sulfmethemoglobin
c. oxyhemoglobin
d. deoxyhemoglobin
b. amyl nitrite (inhalation)
[INTERFERENCE WITH O2 UTILIZATION]
First-line antidotal therapy for hydrogen sulfide poisoning includes:
a. atropine
b. amyl nitrite (inhalation)
c. naloxone
d. flumazenil
a. sodium nitrite (NaNO₂)
[INTERFERENCE WITH O2 UTILIZATION]
Which IV treatment is also used in hydrogen sulfide poisoning?
a. sodium nitrite (NaNO₂)
b. sodium bicarbonate
c. calcium gluconate
d. potassium chloride
b. hyperbaric oxygen (100% O₂)
[INTERFERENCE WITH O2 UTILIZATION]
Definitive supportive management for severe hydrogen sulfide poisoning includes:
a. dialysis
b. hyperbaric oxygen (100% O₂)
c. insulin infusion
d. activated charcoal
a. cassava
[INTERFERENCE WITH O2 UTILIZATION]
Cyanide may be found in which food source?
a. cassava
b. milk
c. spinach
d. fish
a. prunus spp.
[INTERFERENCE WITH O2 UTILIZATION]
Which plant group is associated with cyanide exposure?
a. prunus spp.
b. brassica spp.
c. poaceae spp.
d. fabaceae spp.
a. bitter almond
[INTERFERENCE WITH O2 UTILIZATION]
Which of the following is a source of cyanide?
a. bitter almond
b. apple juice
c. coconut water
d. lettuce
d. yogurt
[INTERFERENCE WITH O2 UTILIZATION]
Cyanide can be found in all EXCEPT:
a. apricot
b. lima beans
c. silver jewelry cleaner
d. yogurt
b. wild blackberry
[INTERFERENCE WITH O2 UTILIZATION]
contains cyanide
a. toothpaste
b. wild blackberry
c. shampoo
d. sunscreen
b. CNS
[INTERFERENCE WITH O2 UTILIZATION]
Cyanide poisoning commonly causes disturbances in the:
a. gastrointestinal system
b. CNS
c. musculoskeletal system
d. endocrine system
c. seizure and central respiratory depression
[INTERFERENCE WITH O2 UTILIZATION]
Death from cyanide poisoning commonly results from:
a. hepatic failure and intestinal perforation
b. severe dehydration and cns depression
c. seizure and central respiratory depression
d. intestinal perforation and severe dehydration
b. hypotension, seizure, respiratory depression
[INTERFERENCE WITH O2 UTILIZATION]
Which triad is classic for cyanide poisoning?
a. fever, edema, rash
b. hypotension, seizure, respiratory depression
c. hypertension, tremor, confusion
d. cyanosis, jaundice, bradycardia
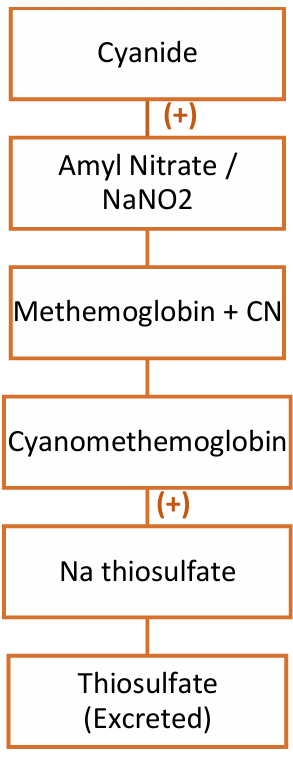
b. methemoglobin
[INTERFERENCE WITH O2 UTILIZATION]
The first step in cyanide treatment aims to produce:
a. oxyhemoglobin
b. methemoglobin
c. sulfhemoglobin
d. deoxyhemoglobin
a. amyl nitrate and sodium nitrite (NaNO₂)
[INTERFERENCE WITH O2 UTILIZATION]
Which agents are used to induce methemoglobin formation in cyanide poisoning?
a. amyl nitrate and sodium nitrite (NaNO₂)
b. atropine and naloxone
c. calcium gluconate and insulin
d. activated charcoal and lactulose
b. sodium thiosulfate
[INTERFERENCE WITH O2 UTILIZATION]
After cyanomethemoglobin formation, which agent helps detoxify cyanide for excretion?
a. sodium bicarbonate
b. sodium thiosulfate
c. potassium chloride
d. calcium carbonate
b. excreted from the body
[INTERFERENCE WITH O2 UTILIZATION]
Sodium thiosulfate converts cyanide into a form that is:
a. stored in fat tissue
b. excreted from the body
c. permanently bound to hemoglobin
d. metabolized into oxygen
b. hydroxycobalamin (B12)
[INTERFERENCE WITH O2 UTILIZATION]
Which vitamin-based antidote binds cyanide to form cyanocobalamin?
a. vitamin a
b. hydroxycobalamin (B12)
c. vitamin d
d. vitamin e
c. produce methemoglobin
[INTERFERENCE WITH O2 UTILIZATION]
High-dose methylene blue may be used to:
a. reduce blood pressure
b. induce vomiting
c. produce methemoglobin
d. increase oxygen saturation directly
a. potassium nitrate (KNO₃)
[INTERFERENCE WITH O2 UTILIZATION]
Which of the following is an inorganic nitrate preservative?
a. potassium nitrate
b. atropine
c. potassium nitrite
d. sodium nitrite
b. chile saltpeter
[INTERFERENCE WITH O2 UTILIZATION]
Sodium nitrate (NaNO₃) is also known as:
a. table salt
b. chile saltpeter
c. baking soda
d. salt peter
d. salt peter
[INTERFERENCE WITH O2 UTILIZATION]
Potassium nitrate (KNO₃) is also known as:
a. table salt
b. chile saltpeter
c. baking soda
d. salt peter
c. sodium nitrate = NaNO3
[INTERFERENCE WITH O2 UTILIZATION]
Which of the following is an inorganic nitrate preservative?
a. naloxone
b. atropine
c. sodium nitrate
d. sodium nitrite
c. isosorbide dinitrate (ISDN)
[INTERFERENCE WITH O2 UTILIZATION]
An organic nitrate
a. sodium nitrite
b. potassium nitrate
c. isosorbide dinitrate (ISDN)
d. sodium chloride
d. glyceryl trinitrate
[INTERFERENCE WITH O2 UTILIZATION]
An organic nitrate
a. sodium nitrite
b. potassium nitrate
c. sodium chloride
d. glyceryl trinitrate
b. sodium nitrite (NaNO₂)
[INTERFERENCE WITH O2 UTILIZATION]
An inorganic nitrite
a. NaNO3
b. NaNO₂
c. KNO₃
d. ISDN
b. methemoglobin formation
[INTERFERENCE WITH O2 UTILIZATION]
The main mechanism of nitrite/nitrate toxicity is:
a. ATP depletion
b. methemoglobin formation
c. cytochrome activation
d. calcium channel blockade
b. vasodilation through smooth muscle relaxation
↑ cGMP → desphosphorylate myosin light chain → smooth muscle relaxation → vasodilation
[INTERFERENCE WITH O2 UTILIZATION]
Increased cGMP in nitrite/nitrate exposure leads to:
a. smooth muscle contraction leading to vasoconstriction
b. vasodilation through smooth muscle relaxation
c. platelet aggregation
d. bronchospasm
a. cyanosis
[INTERFERENCE WITH O2 UTILIZATION]
Which clinical manifestation is common in nitrite/nitrate toxicity?
a. cyanosis
b. jaundice
c. hematuria
d. edema
a. dizziness, headache, lightheadedness &
d. nausea and vomiting with diarrhea
[INTERFERENCE WITH O2 UTILIZATION]
Commonly seen in nitrite/nitrate toxicity
a. dizziness, headache, lightheadedness
b. rash, fever, edema
c. tremor, rigidity, hallucinations
d. nausea and vomiting with diarrhea
b. methylene blue
[INTERFERENCE WITH O2 UTILIZATION]
The treatment for significant methemoglobinemia from nitrite/nitrate toxicity is:
a. atropine
b. methylene blue
c. naloxone
d. flumazenil
b. 1–2 mg/kg
[INTERFERENCE WITH O2 UTILIZATION]
Recommended dose of methylene blue in nitrite/nitrate toxicity
a. 0.1–0.5 mg/kg
b. 1–2 mg/kg
c. 5–10 mg/kg
d. 20 mg/kg
b. coma
[CNS CAUSING COMA / CONVULSION]
CNS depression commonly results in:
a. convulsions
b. coma
c. hypertension only
d. tremors
c. sedatives and hypnotics
[CNS CAUSING COMA / CONVULSION]
Which type of substance is associated with CNS depression?
a. sympathomimetics
b. cocaine
c. sedatives and hypnotics
d. stimulants
b. coma due to CNS depression
[CNS CAUSING COMA / CONVULSION]
Alcohol (OH) toxicity primarily causes:
a. CNS stimulation
b. coma due to CNS depression
c. seizure from overstimulation
d. increased reflexes
b. convulsions
[CNS CAUSING COMA / CONVULSION]
CNS stimulation commonly leads to:
a. coma
b. convulsions
c. respiratory alkalosis only
d. jaundice
b. cocaine
[CNS CAUSING COMA / CONVULSION]
CNS stimulant that may cause convulsions
a. diazepam
b. cocaine
c. phenobarbital
d. alcohol
b. CNS stimulation and convulsions
[CNS CAUSING COMA / CONVULSION]
Sympathomimetics are most associated with:
a. CNS depression and coma
b. CNS stimulation and convulsions
c. insecticides
Organophosphate + Carbamates use
a. air freshener
b. fuel
c. insecticides
d. household cleaning agent
c. malathion
Organophosphate insecticide
a. physostigmine
b. edrophonium
c. malathion
d. atropine
a. parathion
Organophosphate insecticide
a. parathion
b. edrophonium
c. physostigmine
d. atropine
c. physostigmine
Carbamate
a. parathion
b. malathion
c. physostigmine
d. pralidoxime
d. edrophonium
Carbamate
a. parathion
b. malathion
c. pralidoxime
d. edrophonium
b. inhibition of acetylcholinesterase
The mechanism of toxicity of organophosphates and carbamates is:
a. activation of acetylcholinesterase
b. inhibition of acetylcholinesterase
c. blockade of dopamine receptors
d. inhibition of serotonin release
b. irreversibly
Organophosphates inhibit acetylcholinesterase:
a. reversibly
b. irreversibly
a. reversibly
Carbamates inhibit acetylcholinesterase
a. reversibly
b. irreversibly
b. DUMBBELS
Increased muscarinic cholinergic activity in poisoning is remembered by:
a. MAPLE
b. DUMBBELS
c. MONA
d. ABCDE
b. muscle weakness and fasciculations
Nicotinic effects of organophosphate poisoning include:
a. constipation and urinary retention
b. muscle weakness and fasciculations
c. severe jaundice
d. bradycardia
b. tachycardia and hypertension
muscle weakness + fasciculations, adrenal medulla = ↑ epinephrine activity, tachycardia, cramping, HTN
Stimulation of the adrenal medulla in poisoning may cause:
a. decreased epinephrine activity
b. tachycardia and hypertension
c. severe hypoglycemia
d. respiratory alkalosis
b. atropine
Counteracts cholinergic effects in organophosphate poisoning
a. naloxone
b. atropine
c. methylene blue
d. flumazenil
a. pralidoxime
Reactivates acetylcholinesterase in organophosphate poisoning
a. pralidoxime
b. physostigmine
c. edrophonium
d. atropine
b. early (within 24–36 hours)
Pralidoxime is most effective when given:
a. after several weeks
b. early (within 24–36 hours)
c. only after coma develops
d. before atropine
d. reversing the bond between AChE and organophosphate
Pralidoxime works by:
a. increasing acetylcholine release
b. inducing methemoglobinemia
c. blocking nicotinic receptors permanently
d. reversing the bond between AChE and organophosphate
b. aging into a covalent bond
Pralidoxime should be given before:
a. renal excretion
b. aging into a covalent bond
c. seizure onset
d. atropine administration
b. hypertension and cardiac arrhythmia
Drugs affecting the vasculature and heart may cause:
a. hypotension only
b. hypertension and cardiac arrhythmia
c. renal failure only
d. jaundice and edema
b. cGMP
Nitroglycerin (NTG) primarily acts by increasing:
a. cAMP
b. cGMP
c. ATP
d. dopamine
b. smooth muscle relaxation
Increased cGMP results in:
a. smooth muscle contraction
b. smooth muscle relaxation
c. either systemically or locally
Toxic substances may affect the lungs:
a. only locally
b. only systemically
c. either systemically or locally
a. paraquat
Primarily affects the lungs systemically
a. paraquat
b. atropine
c. naloxone
d. methylene blue
d. aspiration
Primarily affects the lungs locally
a. methylene blue
b. atropine
c. naloxone
d. aspiration
b. carbolic acid
Phenol is also known as:
a. sulfuric acid
b. carbolic acid
c. nitric acid
d. boric acid
a. industrial paint removers
Phenol is a component of:
a. industrial paint removers
b. oral antibiotics
c. anticoagulants
d. bronchodilators
a. Joseph Lister
Phenol was once widely used as an antiseptic by:
a. Joseph Lister
b. Alexander Fleming
c. Louis Pasteur
d. Edward Jenner
d. protein denaturation
The mechanism of toxicity of phenol is:
a. acetylcholinesterase inhibition
b. methemoglobin formation
c. dopamine blockade
d. protein denaturation
a. burning sensation
Which symptom is commonly seen in phenol exposure?
a. burning sensation
b. jaundice
c. hematuria
d. bradycardia
a. tingling and numbness
Phenol exposure may also present with:
a. tingling and numbness
b. paralysis
c. hypertension
d. hyperglycemia
b. burn mark formation
A characteristic local effect of phenol exposure is:
a. cherry-red skin
b. burn mark formation
c. cyanosis
d. edema
a. dilution
Mechanism of phenol exposure treatment
a. dilution
b. neutralization
c. antagonism
d. ionization
a. castor oil
Which agent may be used to treat phenol exposure?
a. castor oil
b. naloxone
c. atropine
d. flumazenil
a. PEG &
c. mineral oil
Which of the following may be used in phenol treatment?
a. PEG
b. insulin infusion
c. mineral oil
d. sodium bicarbonate
a. acetaminophen
Which drug is a classic example of delayed liver and kidney toxicity?
a. acetaminophen
b. atropine
c. naloxone
d. lidocaine
a. heavy metals
Which substance class may cause delayed liver and kidney damage?
a. heavy metals
b. antihistamines
c. bronchodilators
d. antacids
b. liver and kidney
Delayed toxic effects commonly involve which organs?
a. lungs and skin
b. liver and kidney
c. brain and eyes
d. stomach and pancreas