GFR Estimation
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
what is GFR?
-equal to the sum of the filtration rates in all of the functioning nephrons
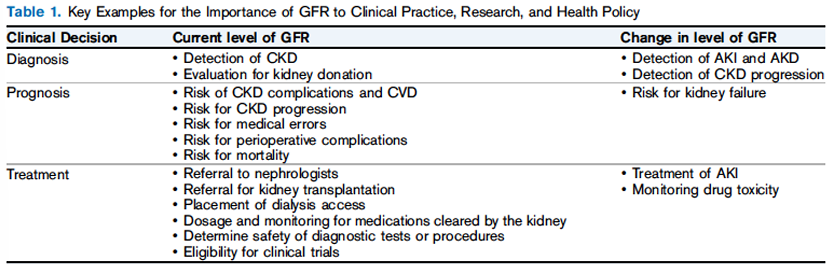
GFR assessment is essential for
-patient care, research, and public health
what is a normal GFR?
-for healthy young adults: 90-120 mL/min/1.73m²
-expected age-related decline in GFR: ~1 mL/min/1.73m² per year beginning in the third decade of life
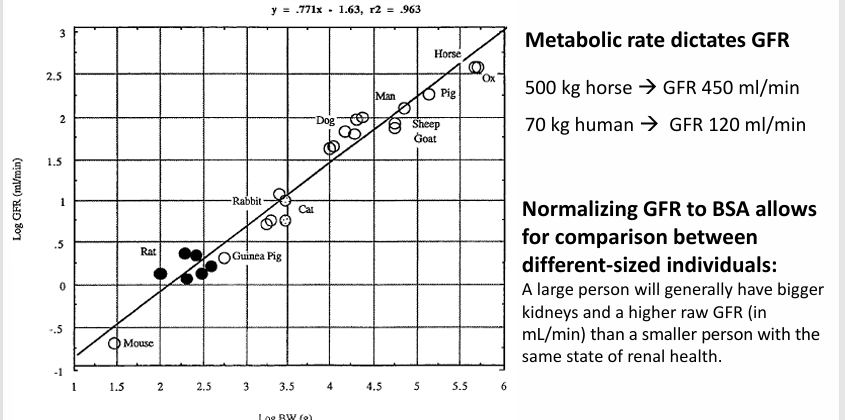
GFR is normalized to
-body surface area (BSA)
how to assess GFR
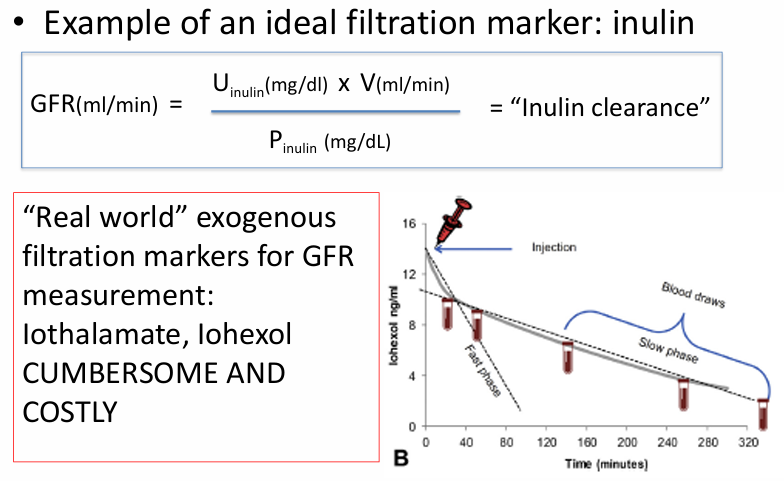
-direct measurement of GFR: EXOGENOUS filtration markers- most accurate, costly, cumbersome
-estimation of GFR: relies on ENDOGENOUS filtration markers (creatinine, cystatin C)- 24 hr urine for creatinine clearance, estimating equations
how to measure GFR
1) collect all urine entering Bowman’s space in a given time (impossible)
2) pick a substance that is freely filtered at the glomerulus BUT not reabsorbed, metabolized, or secreted (“ideal filtration marker”), measure its clearance form the blood or urine
measuring GFR
creatinine
-an endogenous, very good (non-ideal) filtration marker
-creatinine = waste product formed by normal breakdown of muscle
-released into circulation at relatively constant state
-freely filtered at the glomerulus
-not reabsorbed or metabolized by the kidney
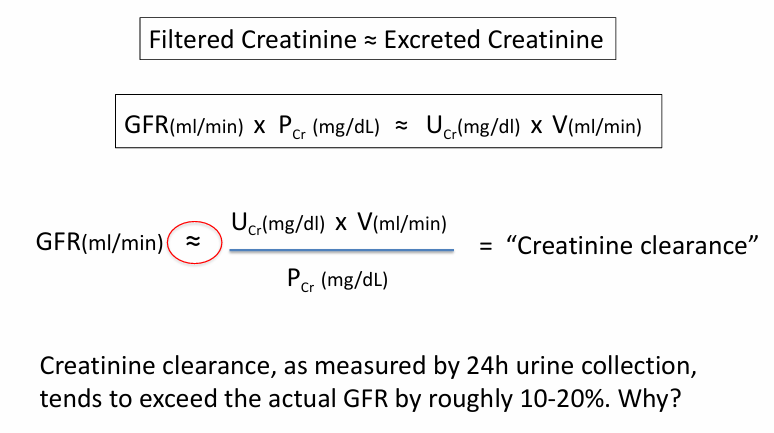
-*there IS secretion by the proximal tubule
24hr urinary clearance of creatinine as estimate for GFR
relationship of GFR and plasma [Cr]
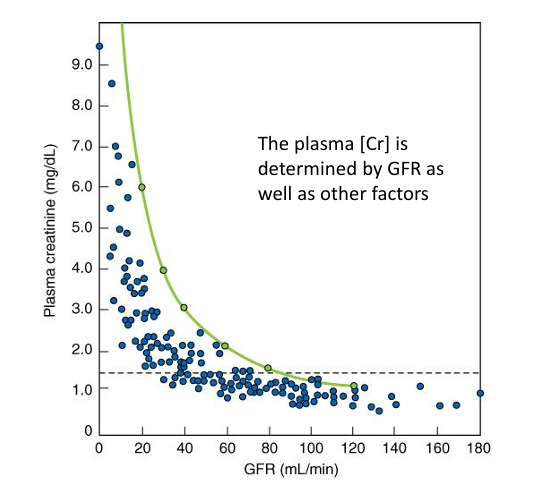
relationship of plasma [Cr] to GFR
GFR estimating equations
-for each patient in a large cohort: collect an abundance of clinical and demographic data and measure their GFRs
-apply stepwise multiple regression to find the fewest number of variables that most effectively predict the measured GFR
the MDRD eGFR equation
-1628 patients with measured GFR (iothalamate)
-mean age 50, 60% men, 80% white, mean GFR 40 ml/min/1.73²
-stepwise multiple regression to predict GFR
-clinical variables: weight, height, gender, race, age, diabetes, MAP, serum- creatinine/urea nitrogen/albumin/phos/calcium, urine- creatinine/urea nitrogen/protein/phos
the 4-variable MDRD eGFR equation
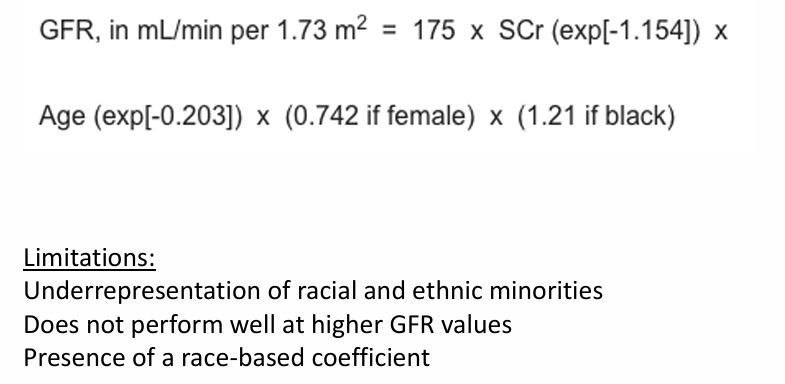
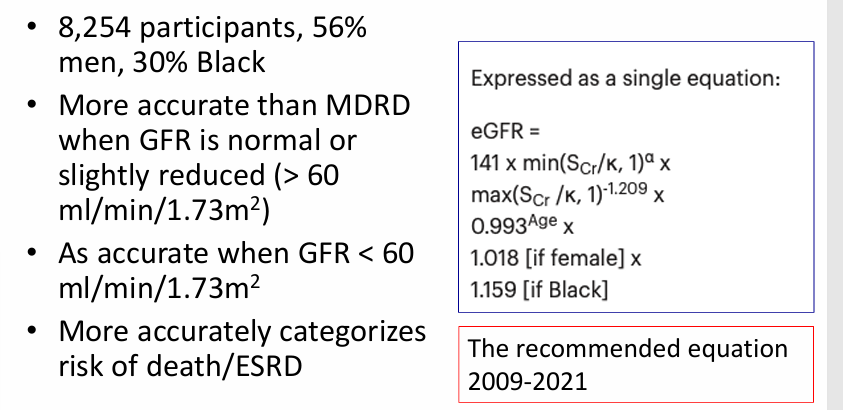
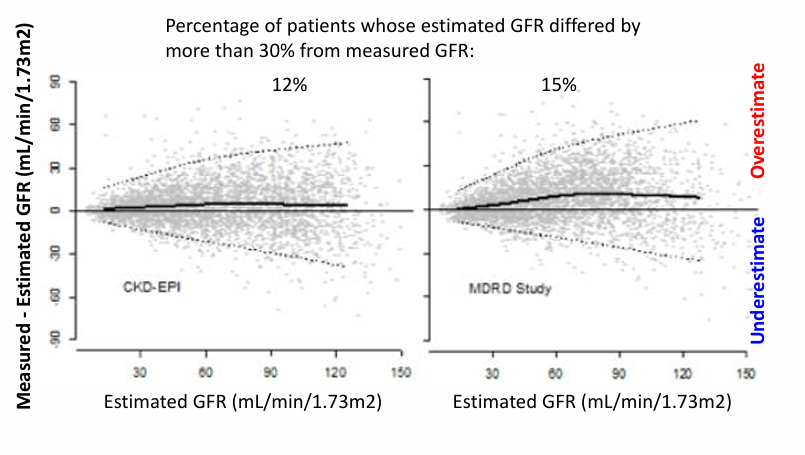
the 2009 CKD-EPI equation
problems with including race in GFR reporting
-race is a social construct, not a biologic determinant:
-the genetic variation found in the human species is not grouped into discrete, genetically distinct units scientists can identify as races
-race is an unreliable proxy for social determinants of health
-may normalize or perpetuate harmful beliefs about race and biology
-dichotomization of race is inappropriate
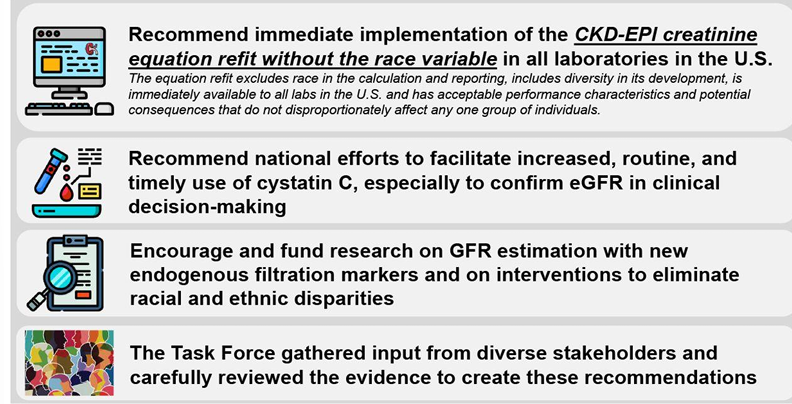
unifying approach for GFR estimation- recommendations of the NKF-ASN task force on reassessing the inclusion of race in diagnosing kidney disease
important caveats about Cr-based GFR estimating equations
-stable serum Cr is required (steady state!)
-eGFR: emphasis on the “estimate”
-equations will be less accurate in people with extremes of: muscle mass, animal protein intake
-equations will be less accurate in situations where tubular secretion of Cr is affected
eGFR- emphasis on “estimate”
limitations of SCr-based estimation equations- examples
-extremes of body composition: bodybuilder, lower extremity amputee
-dietary extremes of animal protein intake: high animal protein intake/creatinine supplements
-variability in tubular secretion: trimethoprim/sulfamethoxazole, cimetidine (inhibit tubular secretion of Cr)
-AKI with rapidly rising serum Cr
sometimes ____ is needed to better characterize GFR
-confirmatory testing
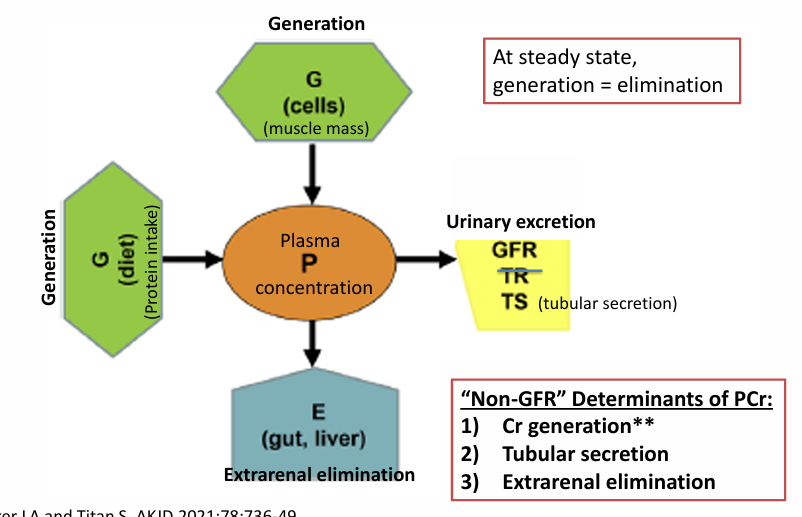
-when non-GFR determinants of PCr are prominent
-when the estimated GFR lies close to an inflection point that could change management (kidney donation, chemotherapy, clinical trial inclusion)
what tests can you order for confirmatory testing?
-cystatin C
-24h urine collection for creatinine clearance
-measured GFR with injectable filtration marker (ie iothalamate)
cystatin C
-endogenous filtration marker
-protein produced in all nucleated cells
-freely filtered at glomerulus
-catabolized and reabsorbed by tubular epithelial cells
-less affected by muscle mass and diet than serum Cr
-inflammation, smoking, thyroid abnormalities, and obesity may affect
eGFR equations that use cystatin C
-2012: CKD-EPI cystatin C (no race)
-2021: CKD-EPI creatinine-cystatin C (no race)
-equations that use BOTH Cr and cystatin C tend to be more accurate than either one alone
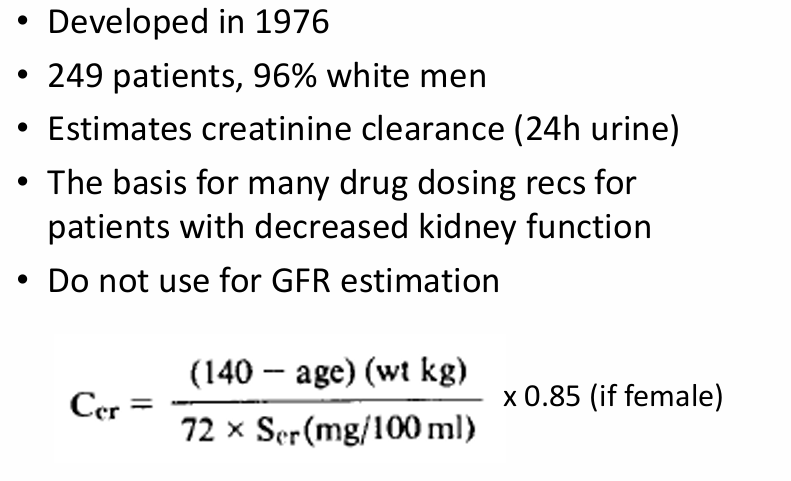
Cockcroft-Gault equation