MRI MEGA QUIZ
1/308
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
309 Terms
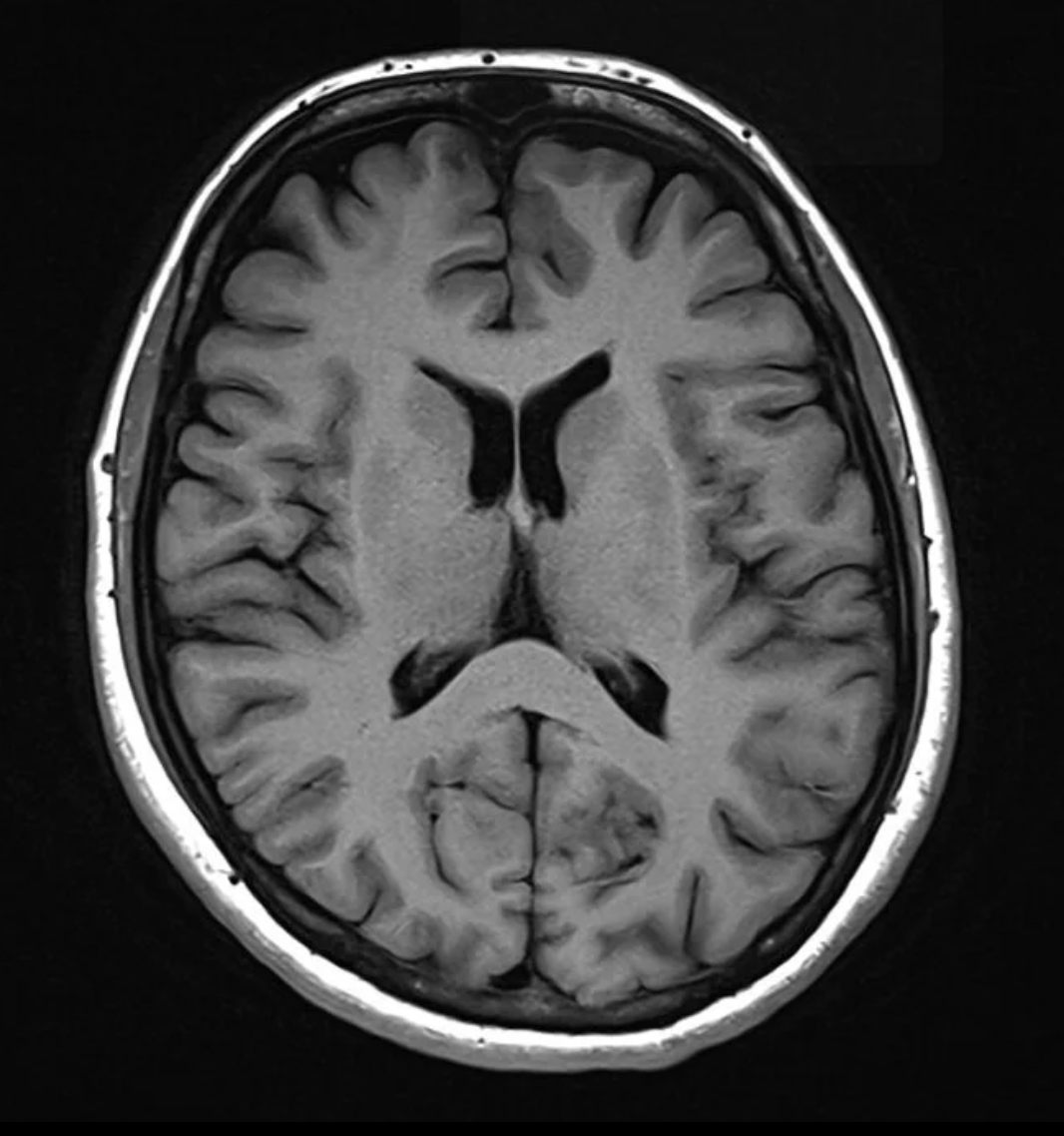
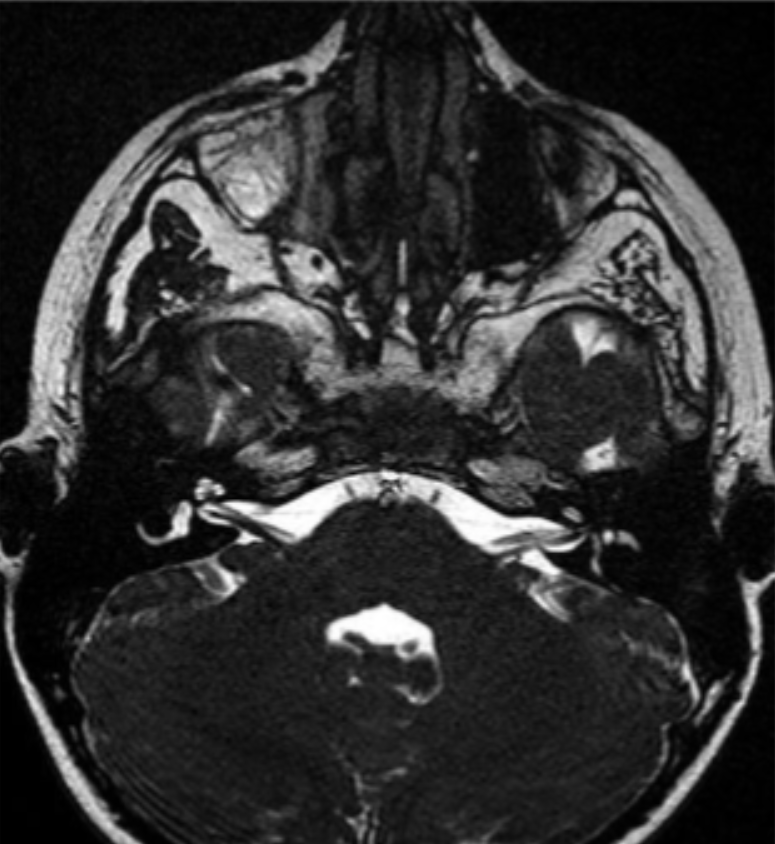
What weighting and plane is this image in?
T1 axial
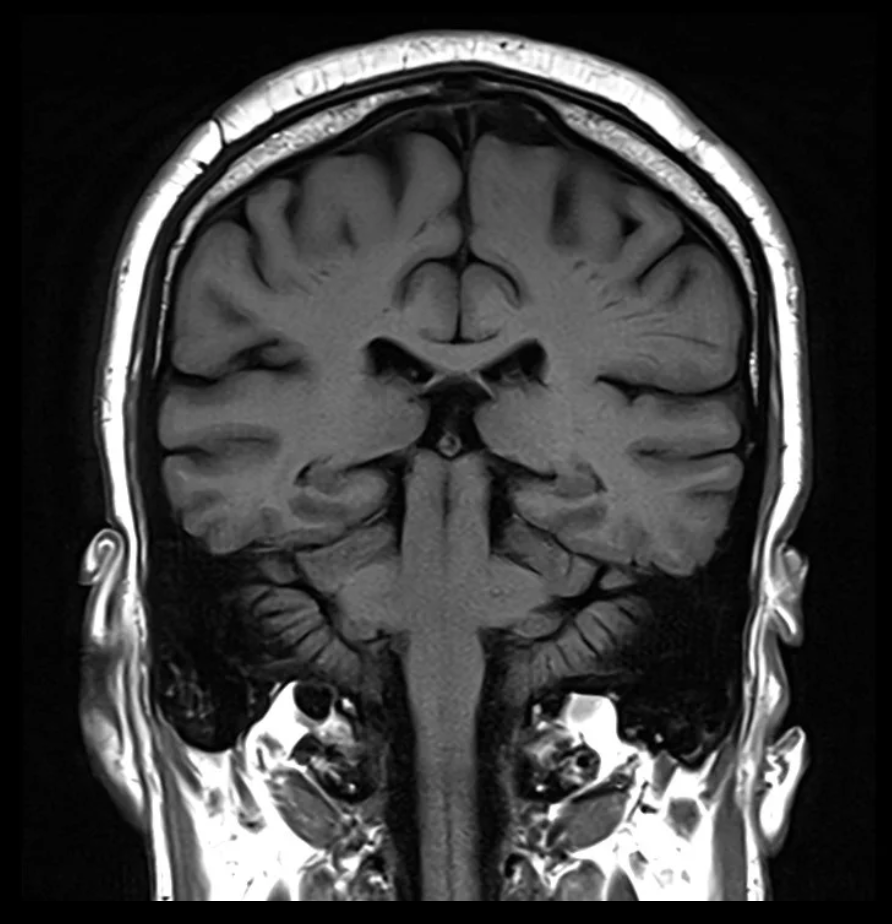
What weighting and plane is this image in?
T1 coronal
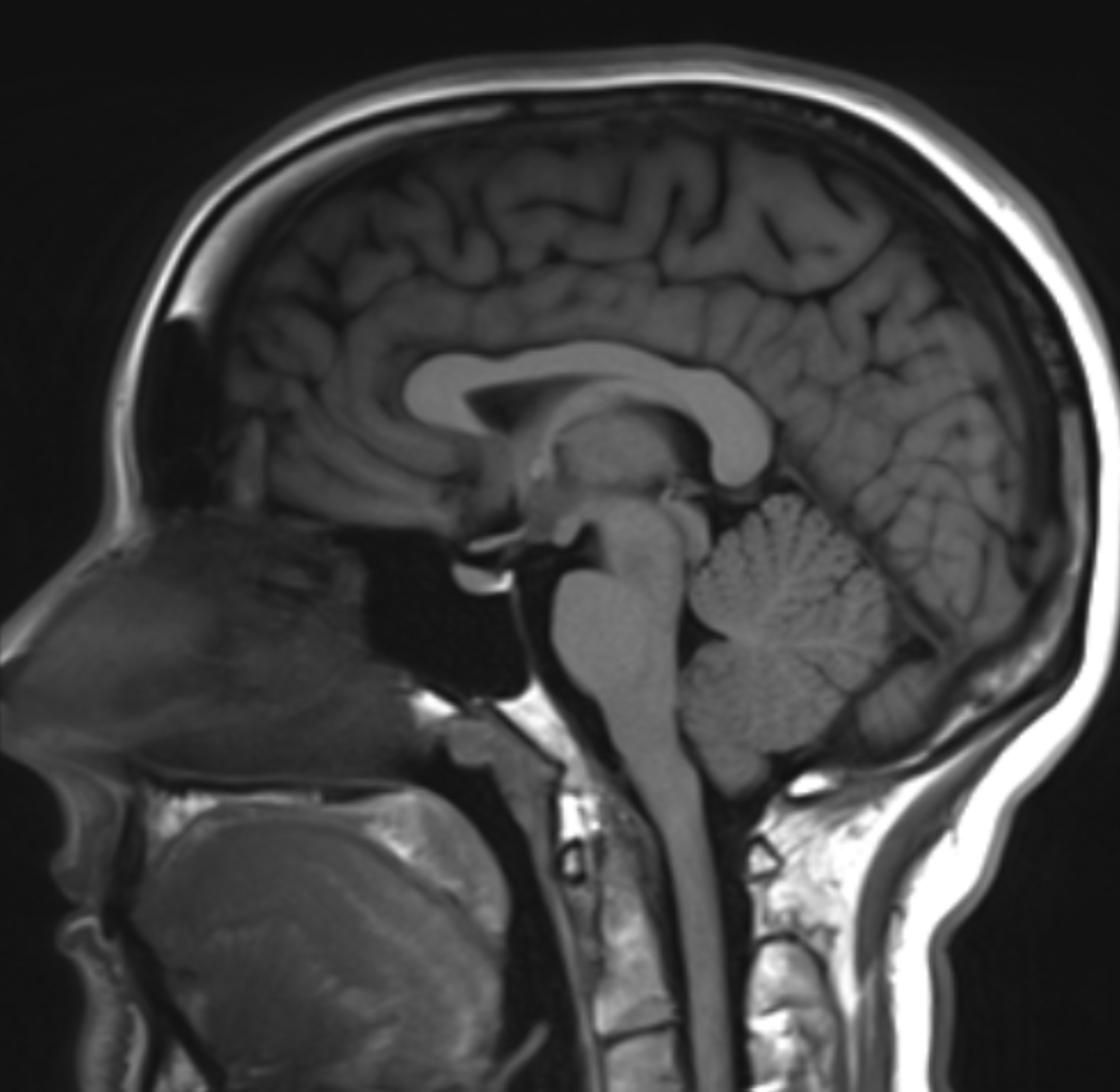
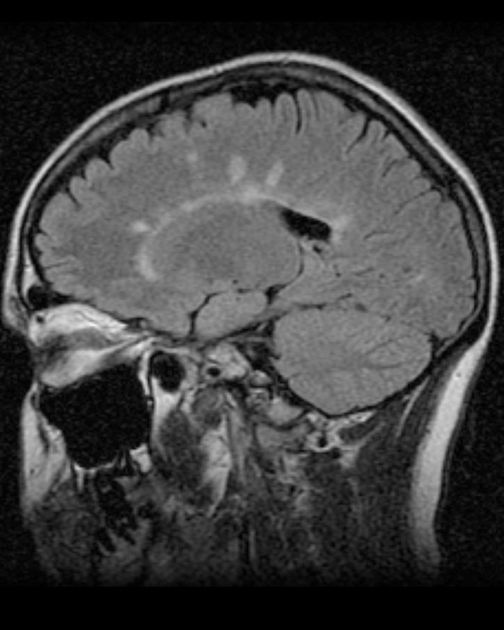
What weighting and plane is this image in?
T1 sagittal
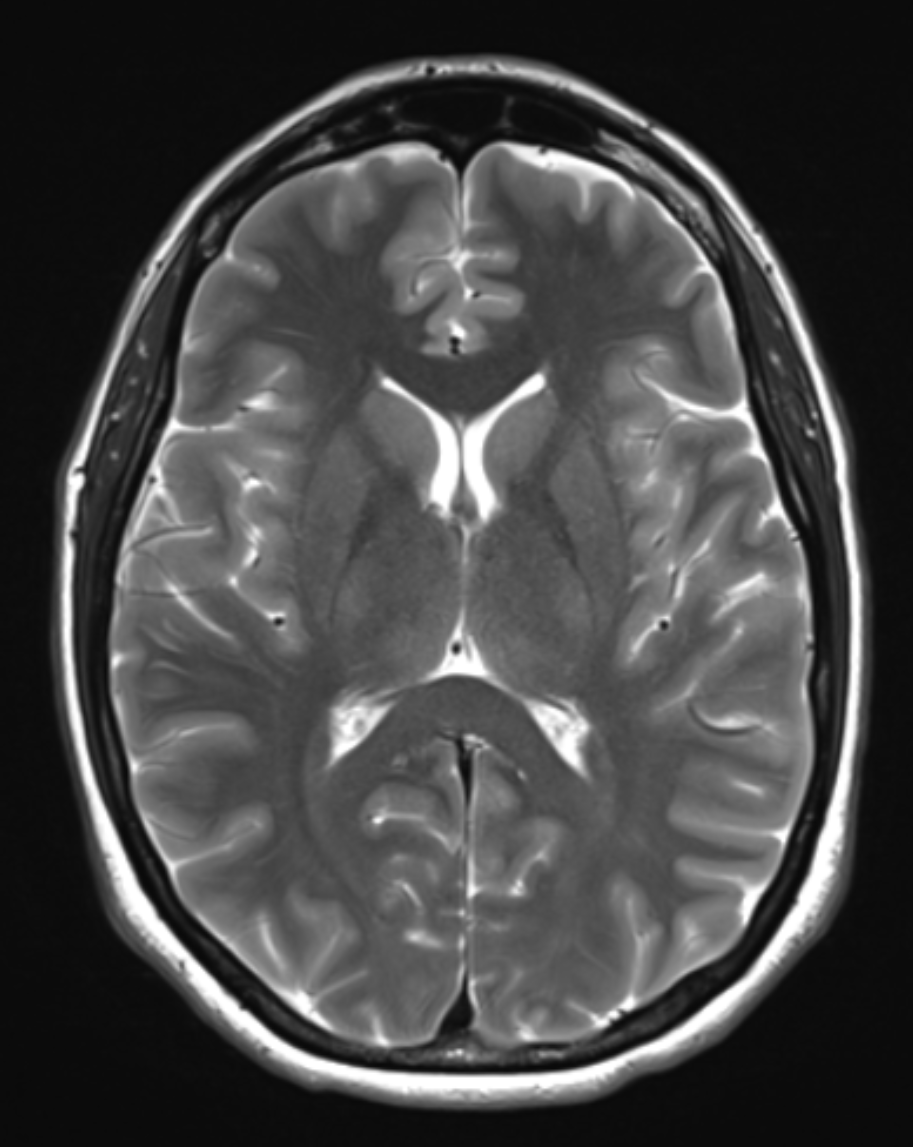
What weighting and plane is this image in?
T2 axial
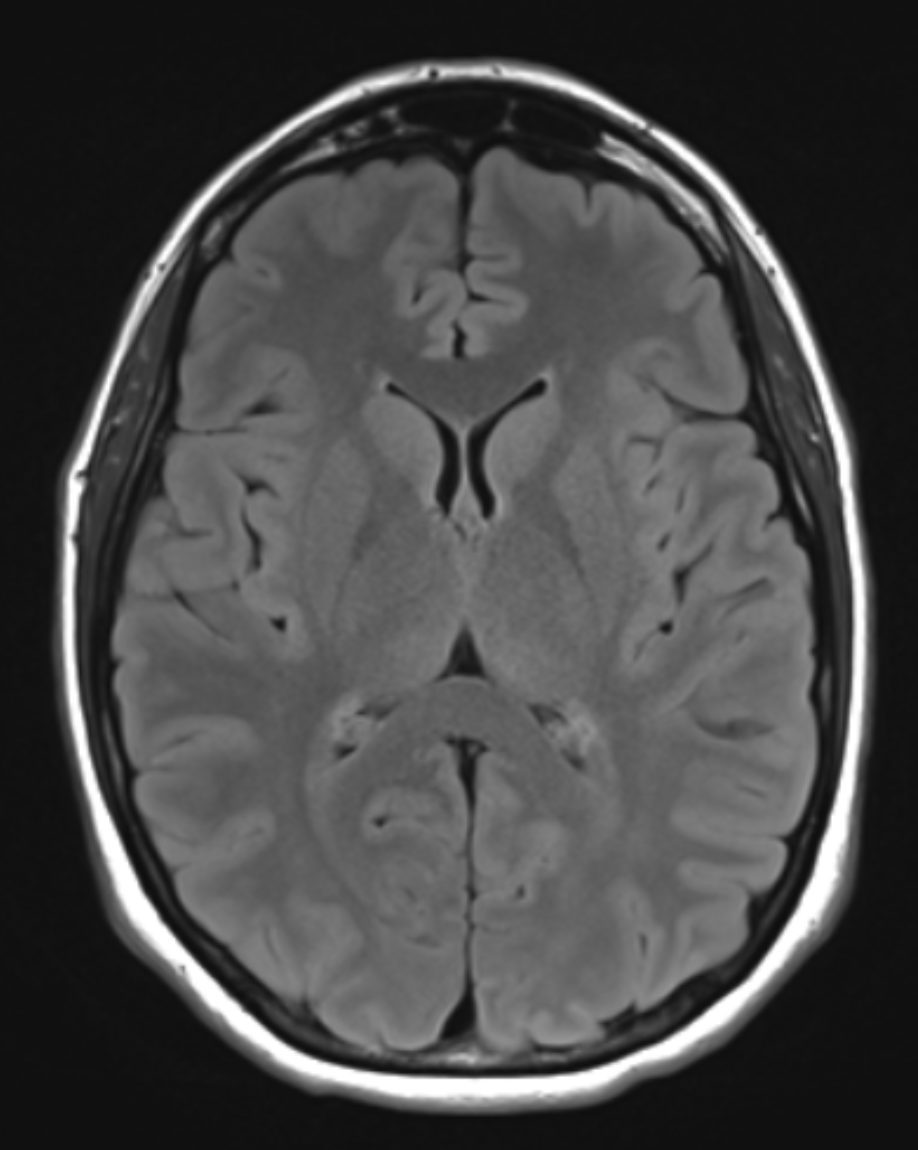
What weighting and plane is this image in?
FLAIR axial
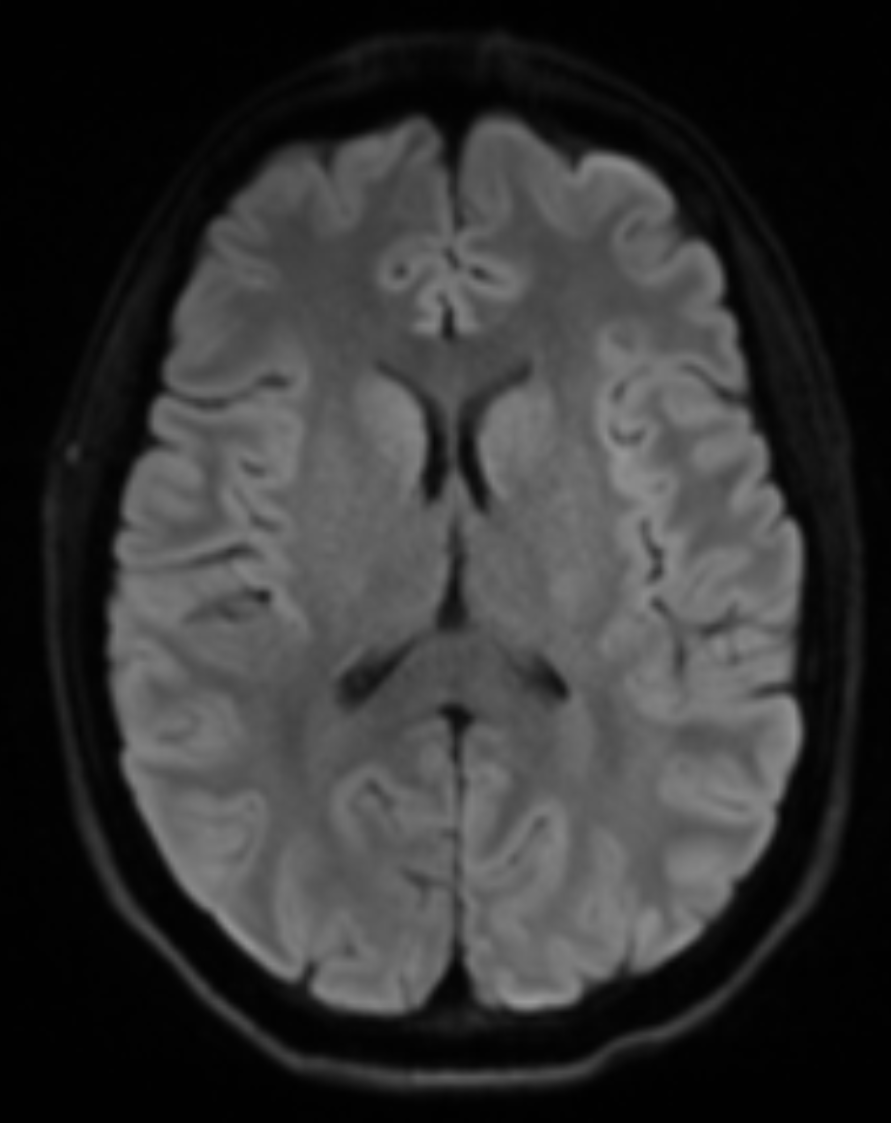
What weighting and plane is this image in?
DWI axial
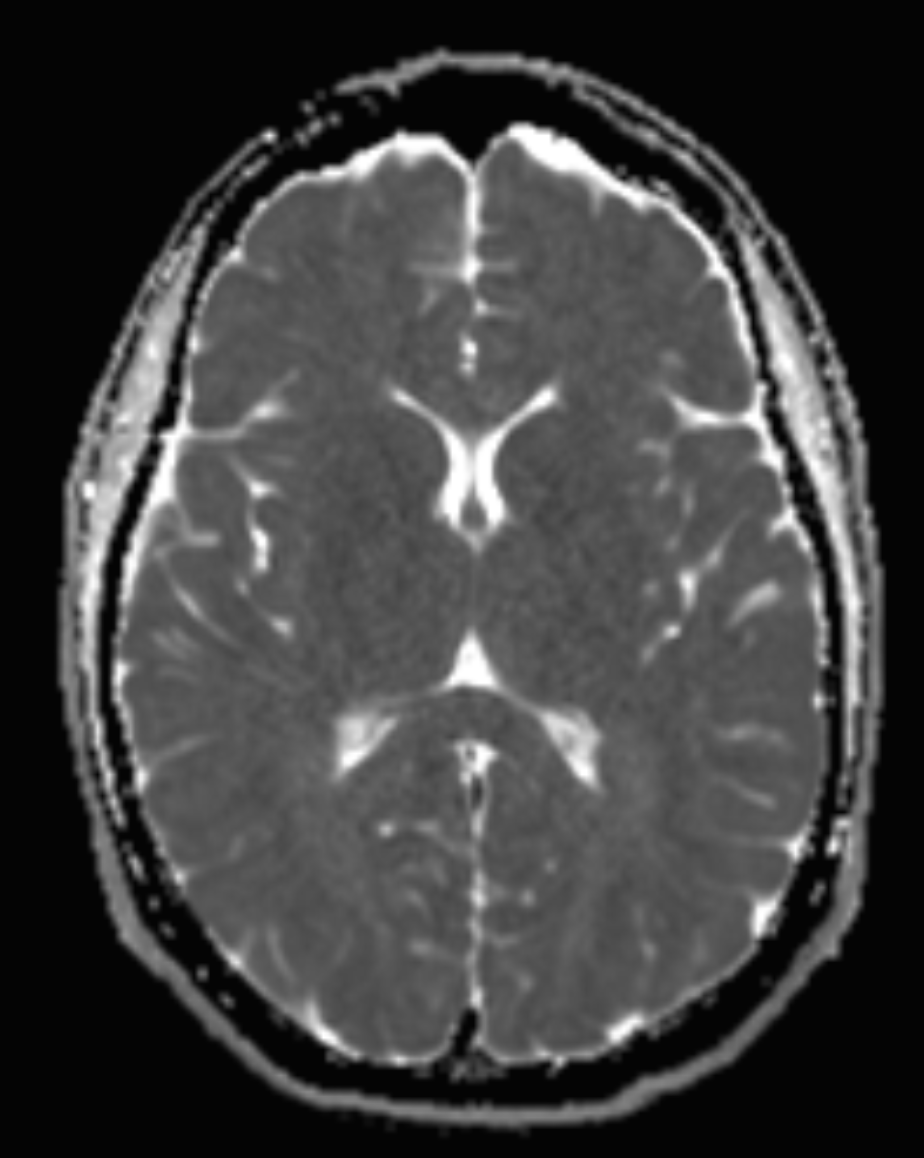
What weighting and plane is this image in?
ADC axial
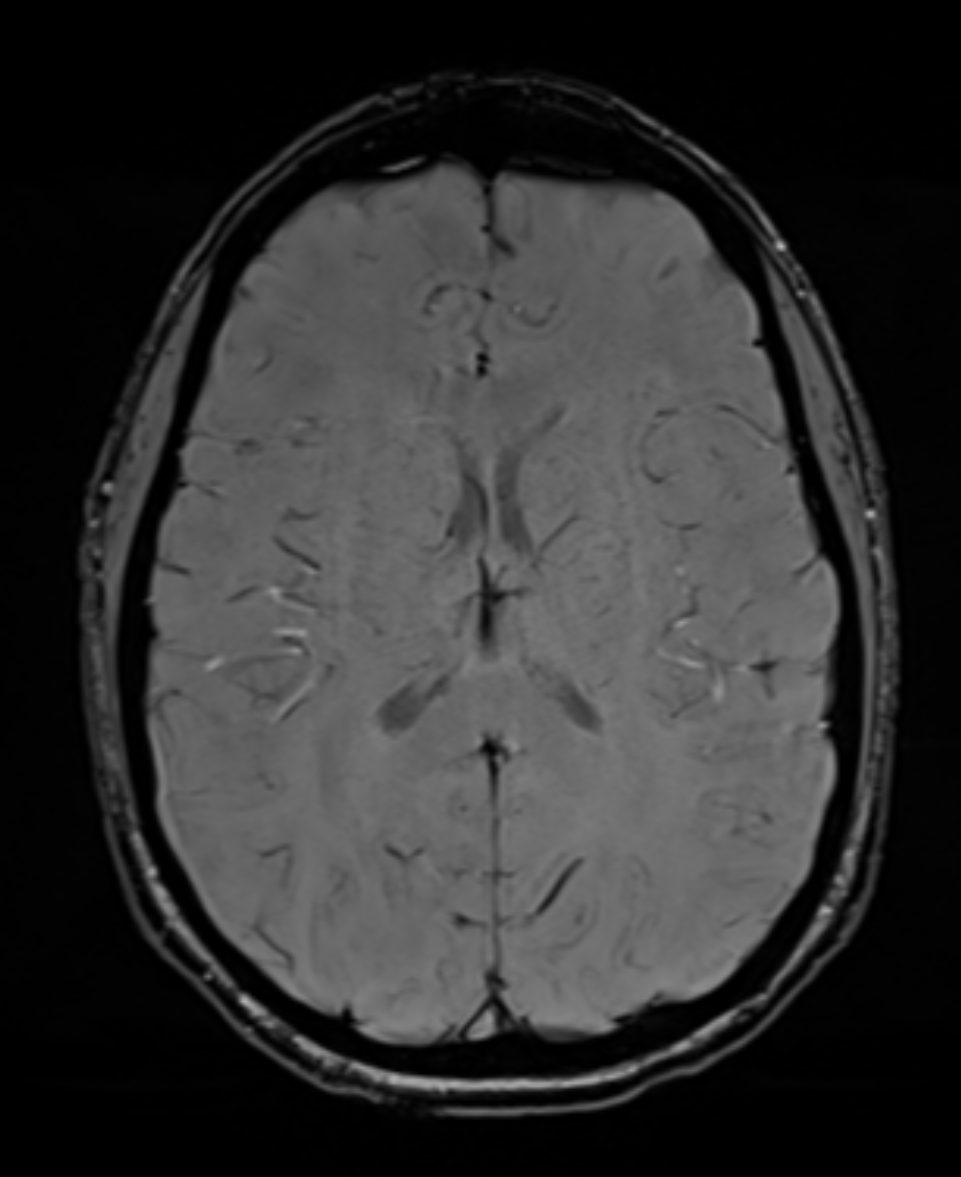
What weighting and plane is this image in?
SWI axial
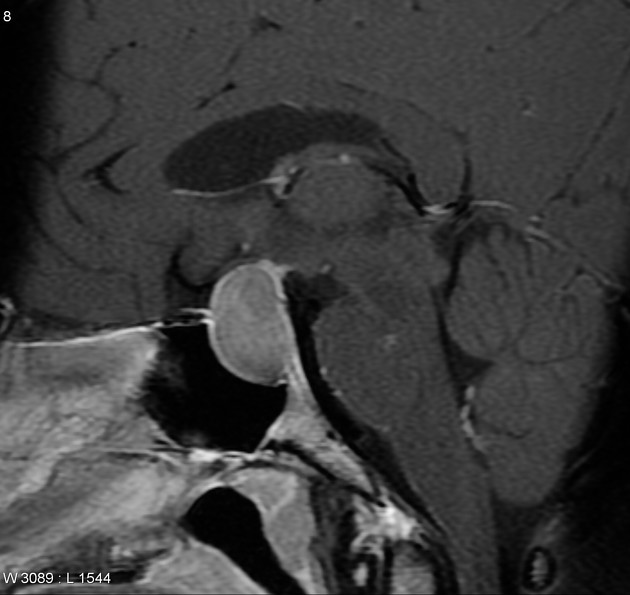
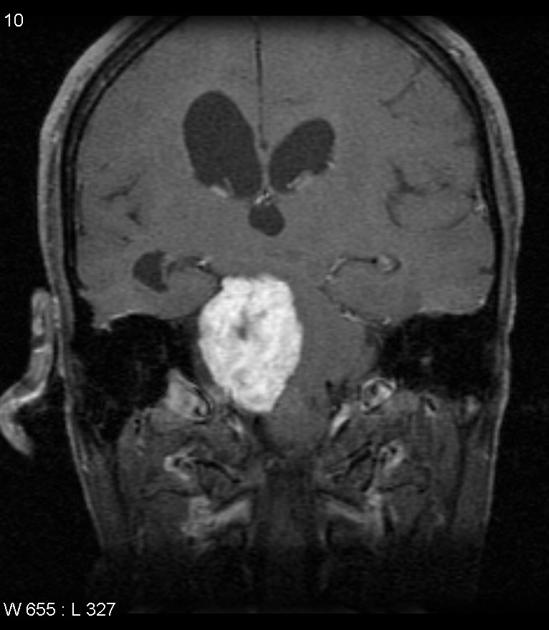
Name this pathology (Sag T1 C+)
Macroadenoma of the pituitary gland
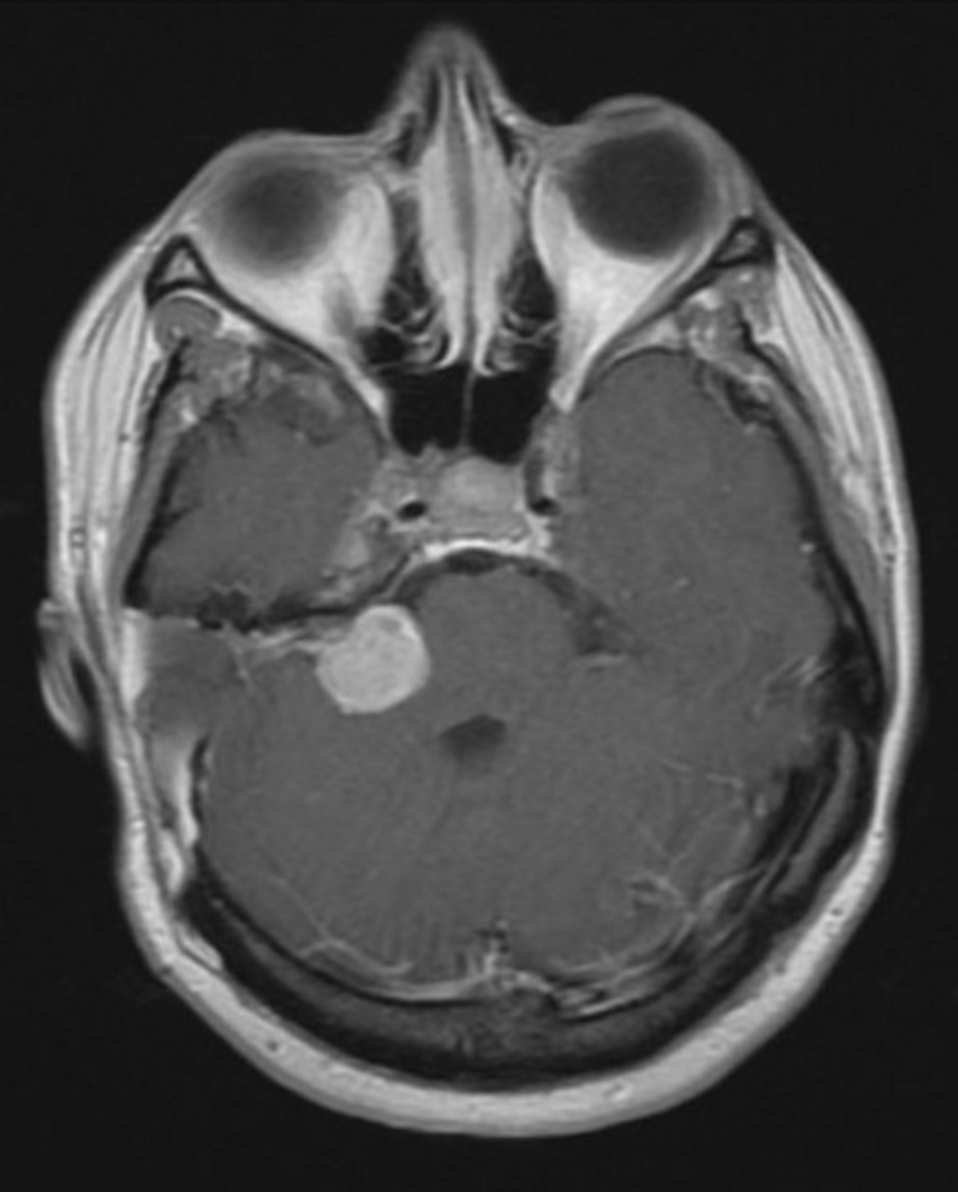
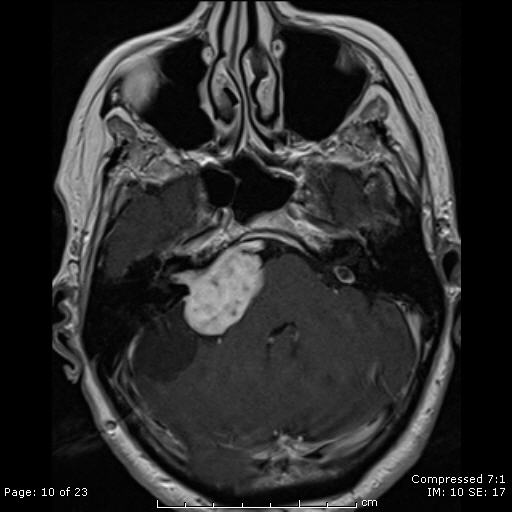
Name this pathology (Axial T1 C+)
Right-sided acoustic/vestibular Schwannoma

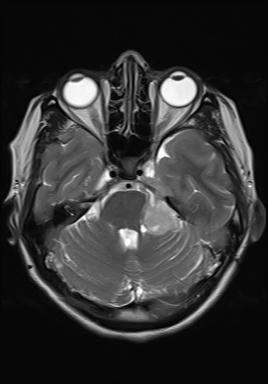
Name this pathology (Axial T2)
Intra-axial tumour with adjacent oedema (medulloblastoma)
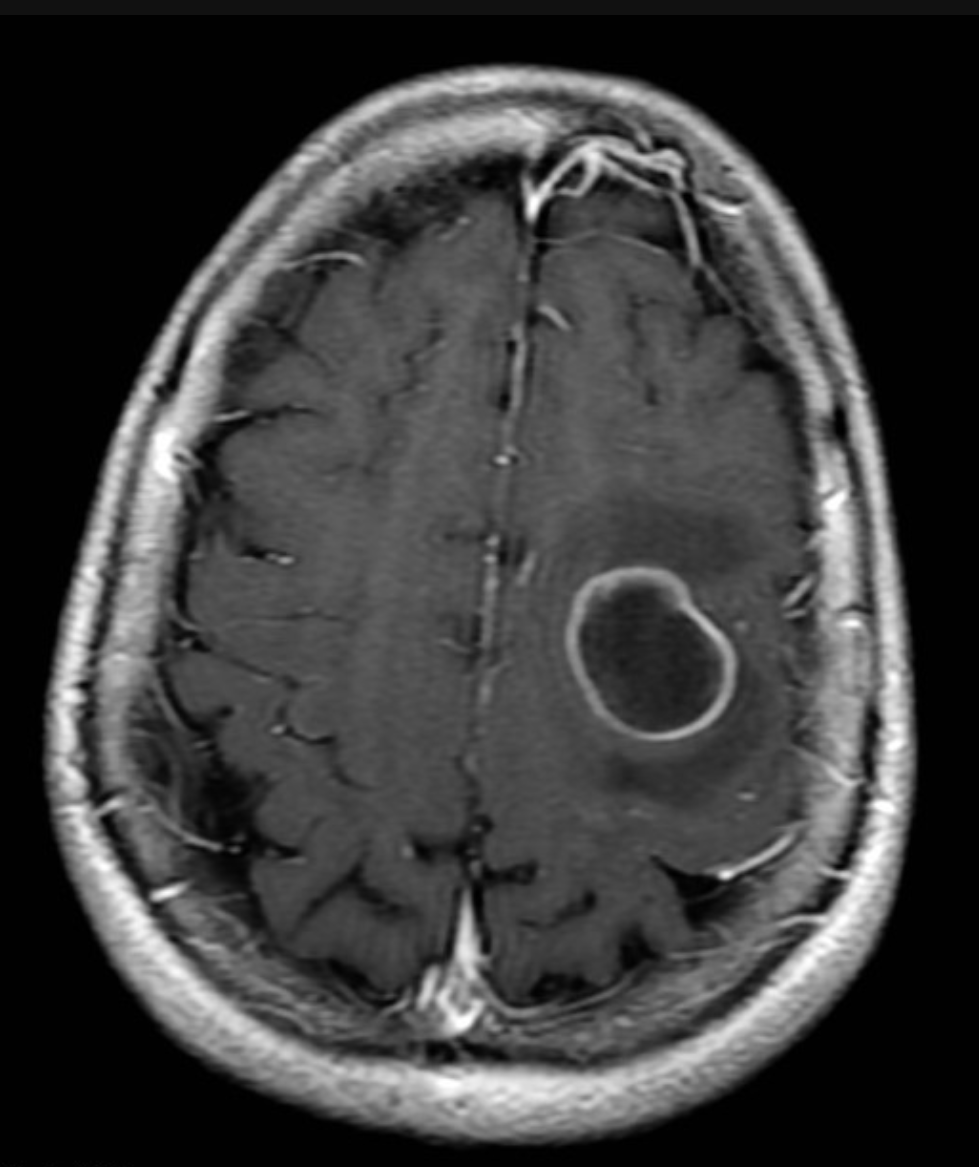
Name this pathology (Axial T1 C+)
Intra-axial ring-enhancing tumour in the left frontal lobe with small amount of oedema (cerebral metastasis)
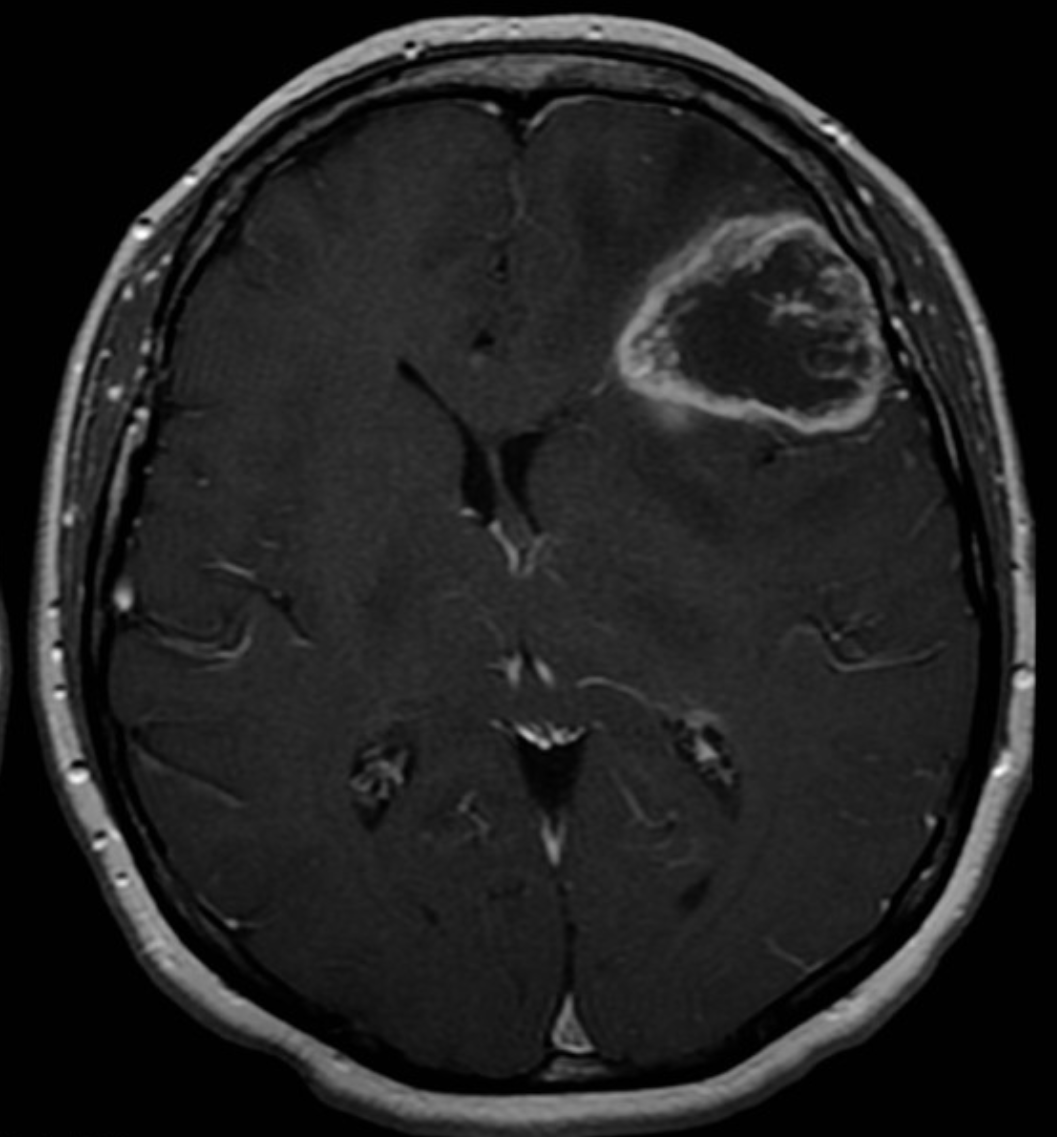
Name this pathology (Axial T1 C+)
Intra-axial, ring-enhancing tumour in the left frontal lobe with positive mass effect (GBM)

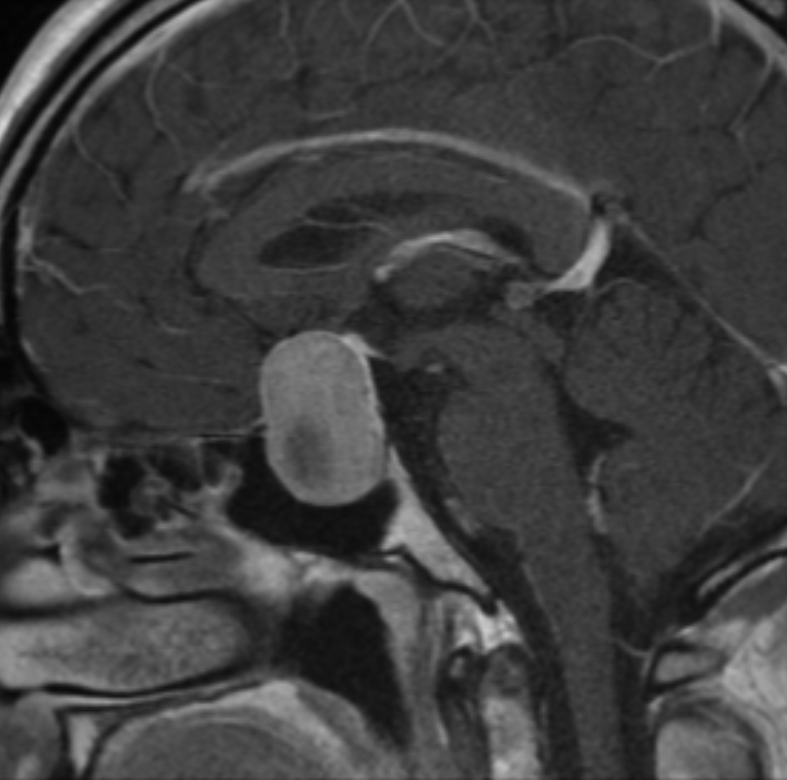
Name this pathology (Sagittal T1 C+)
Extra-axial tumour in the posterior fossa, demonstrating homogenous enhancement with a dural tail (meningioma)
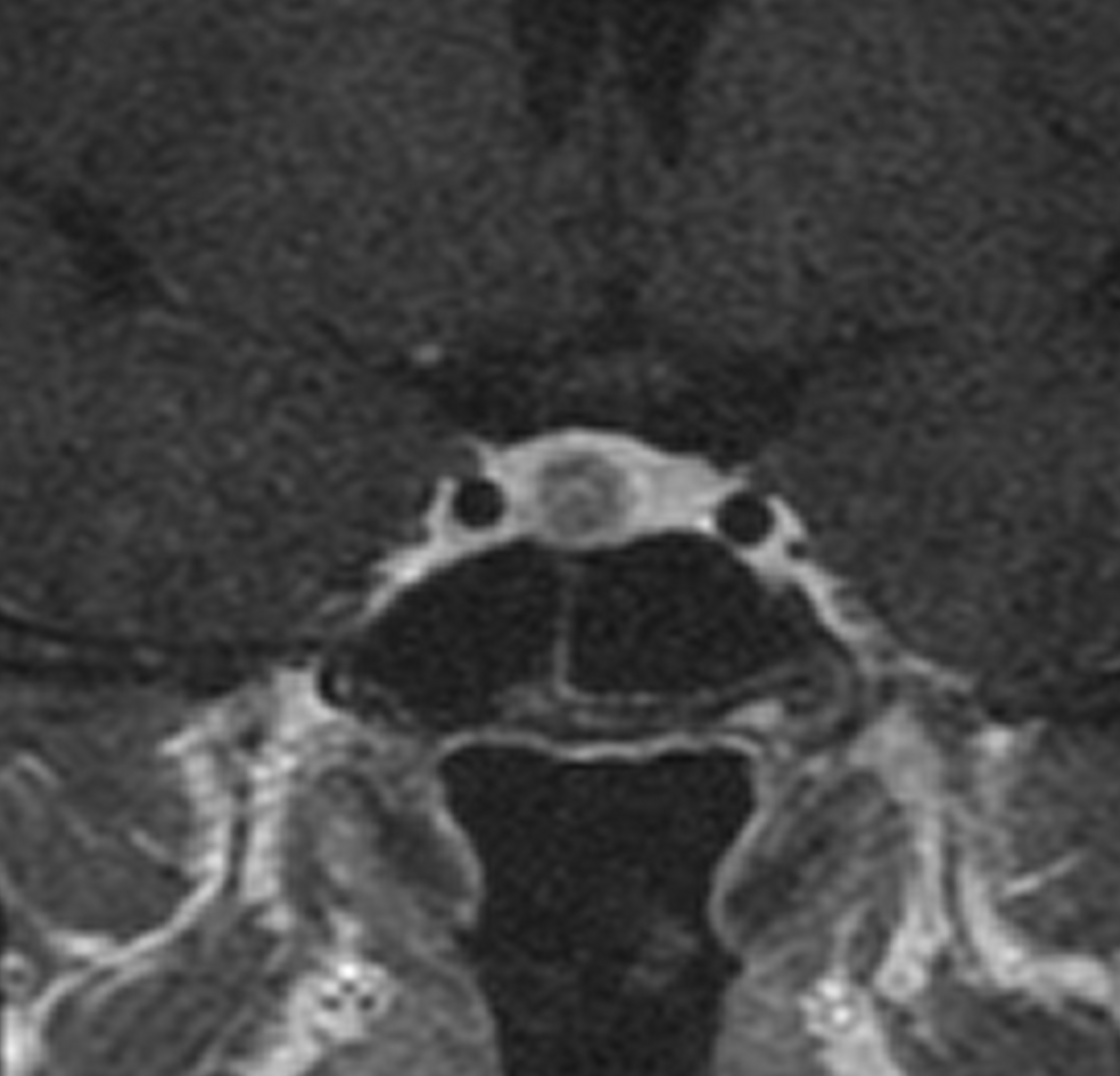
Name this pathology (Coronal dynamic T1 C+)
Microadenoma of pituitary gland
Name this pathology (Coronal T1 C+)
Microadenoma in right aspect pituitary gland
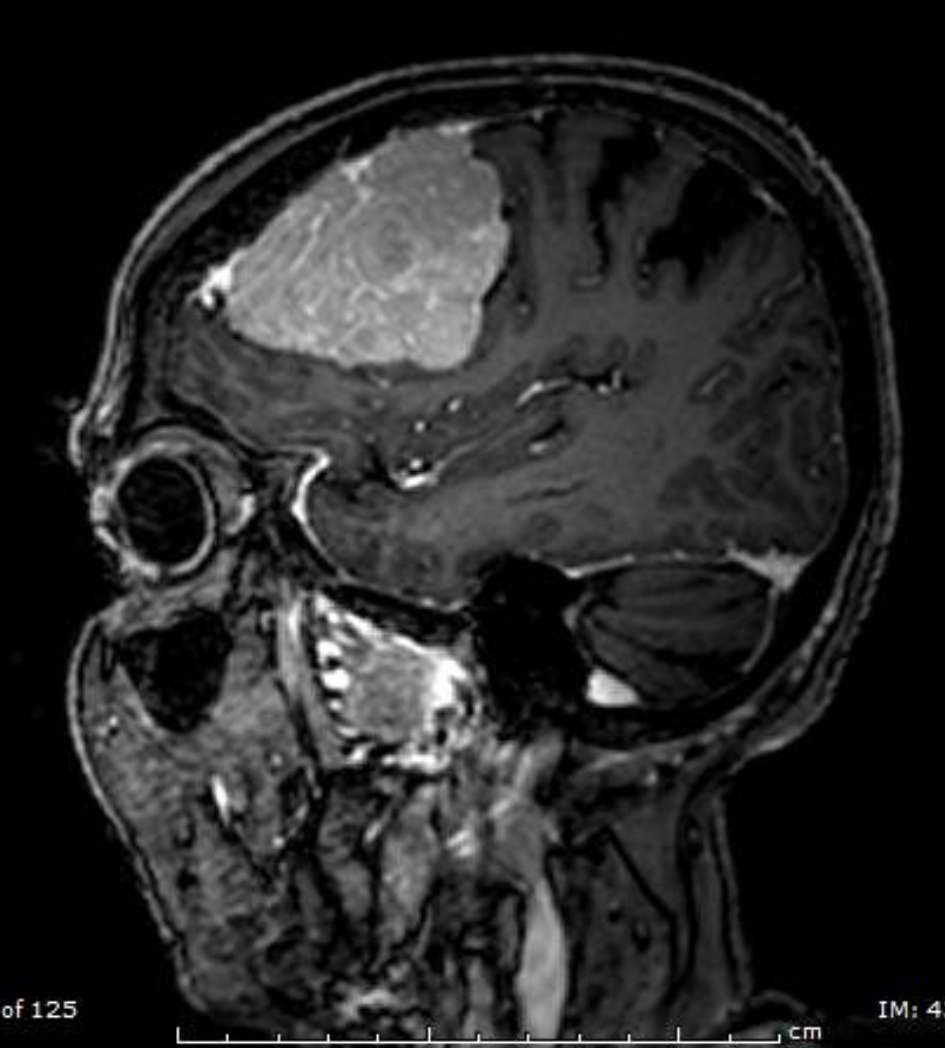
Name this pathology (Sagittal T1 FS C+)
Extra-axial tumour in the (left) frontal lobe, with fairly homogenous enhancement, enhancing dural tails (and mass effect) - meningioma
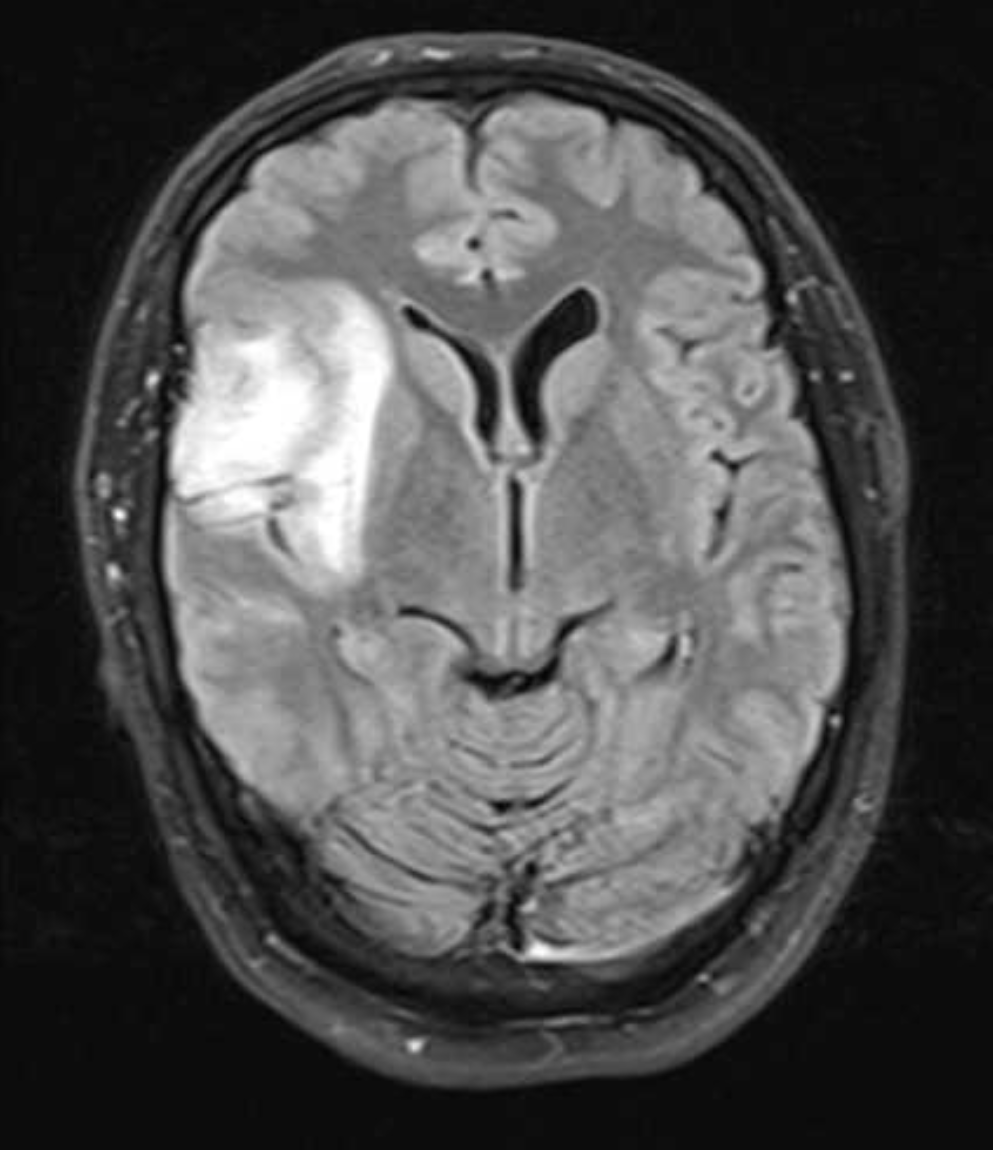
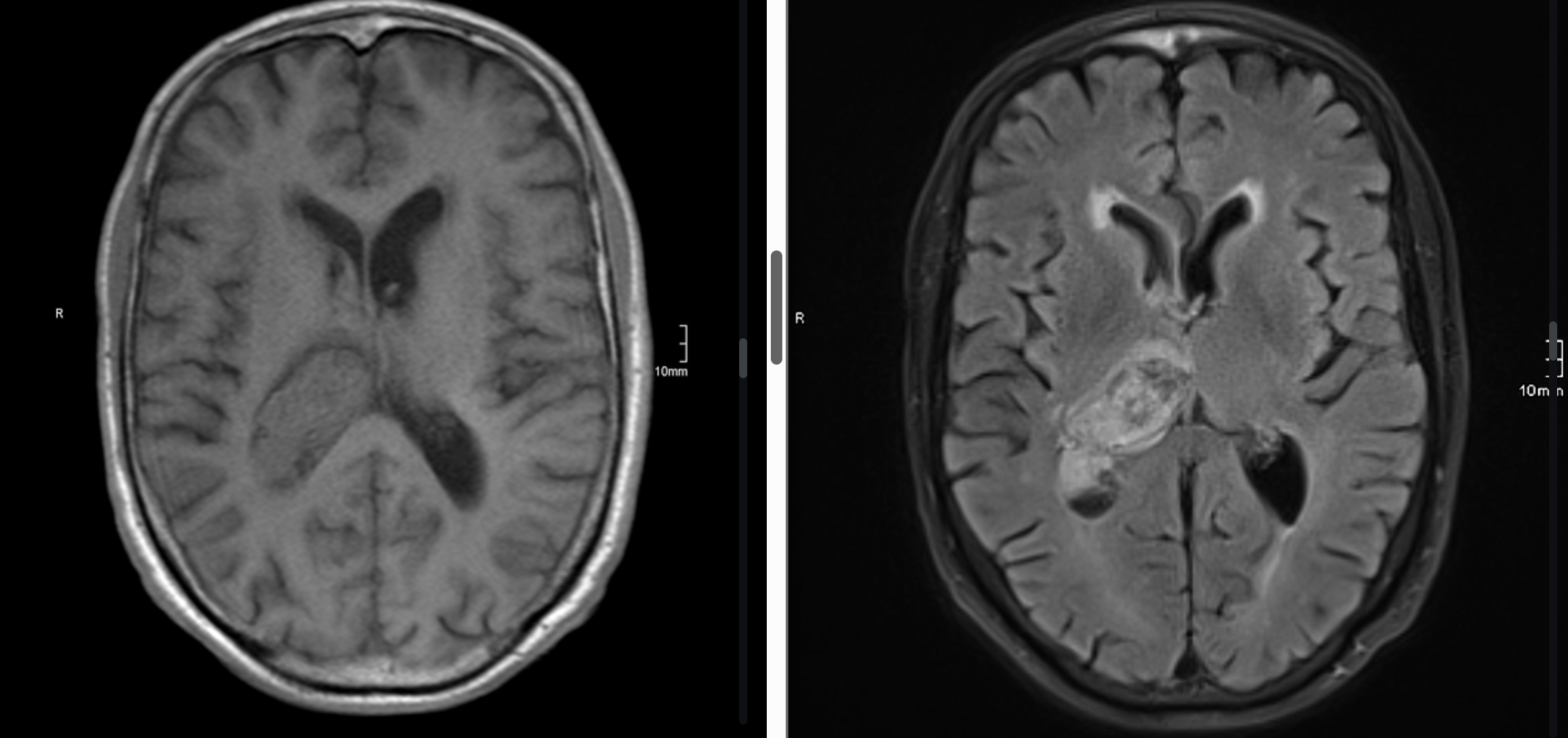
Name this pathology (Axial FLAIR, low signal on T1)
Intra-axial tumour in the right frontal lobe (astrocytoma)
Name these sequences and pathology demonstrated.
Lesion in the posterior right lateral ventricle (and right thalamus)
T1 - isointense
T2 FLAIR - iso/hyperintense
Therefore, hyperacute intracranial haemorrhage
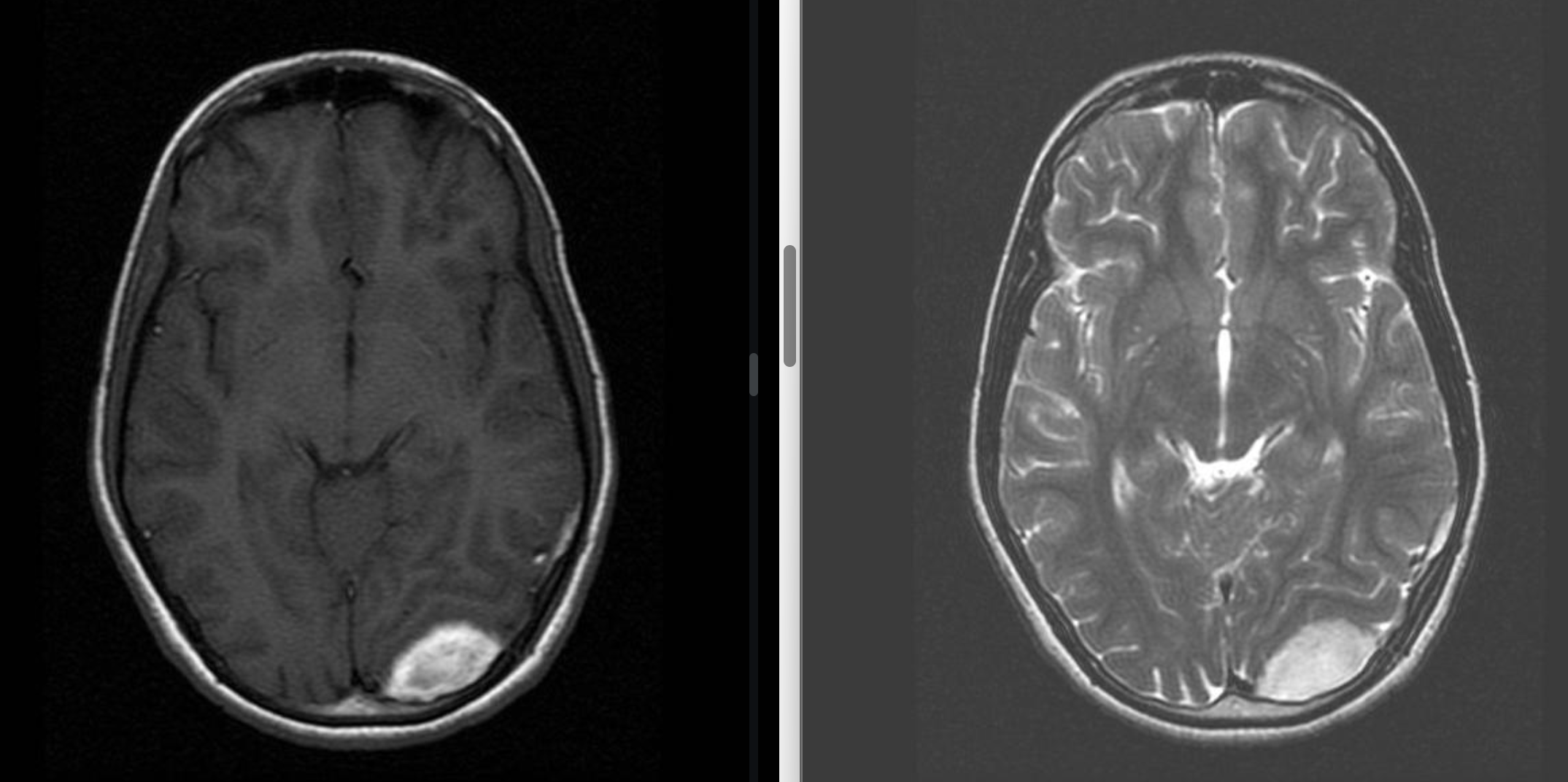
Name these sequences and pathology demonstrated.
Extra-axial lesion in the posterior left occipital lobe
T1 - hyperintense
T2 - hyperintense
Therefore, late subacute extracranial haemorrhage
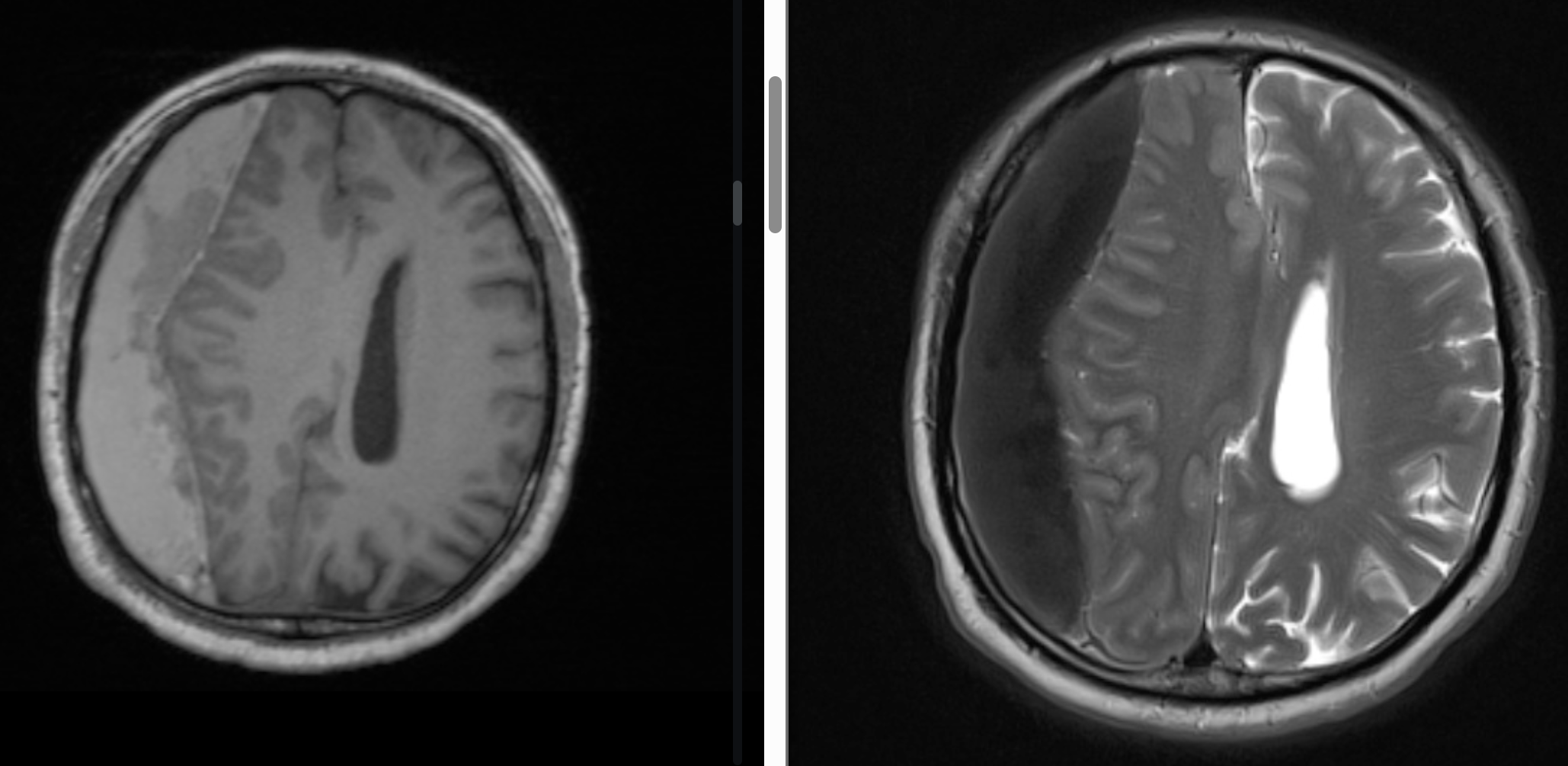
Name these sequences and pathology demonstrated.
Subdural lesion in the right frontal lobe with midline shift
T1 - hyperintense
T2 - hypointense
Therefore, early subacute extracranial haemorrhage
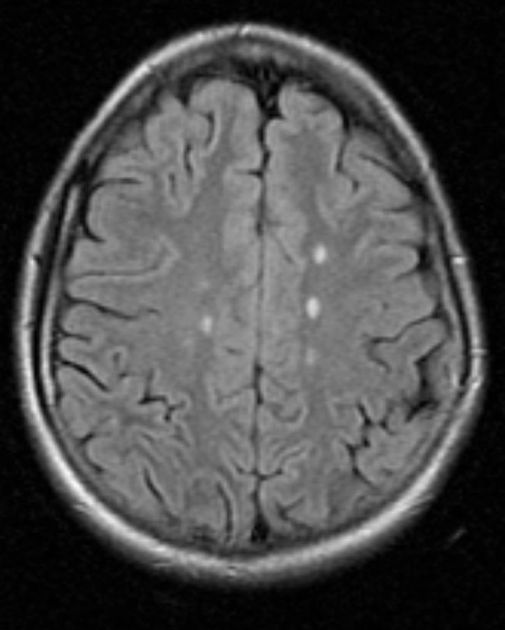
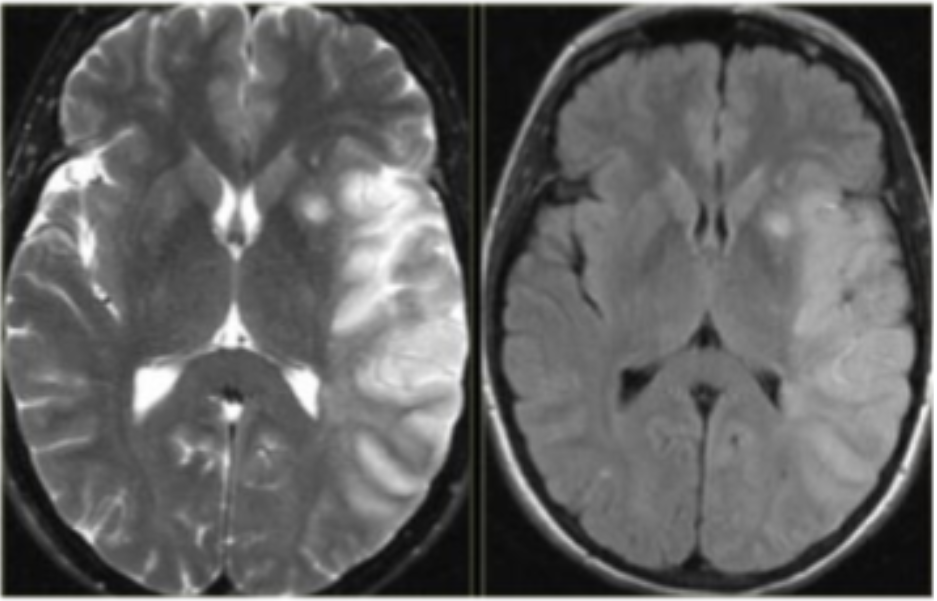
Name this sequence and the pathology demonstrated.
FLAIR Ax - bilateral hyperintense foci superior to lateral ventricles likely Dawson’s fingers (better seen on sagittal) indicating multiple sclerosis
Name this sequence and the pathology demonstrated.
FLAIR Sag - hyperintense Dawson’s fingers extending from the corpus callosum, indicating multiple sclerosis
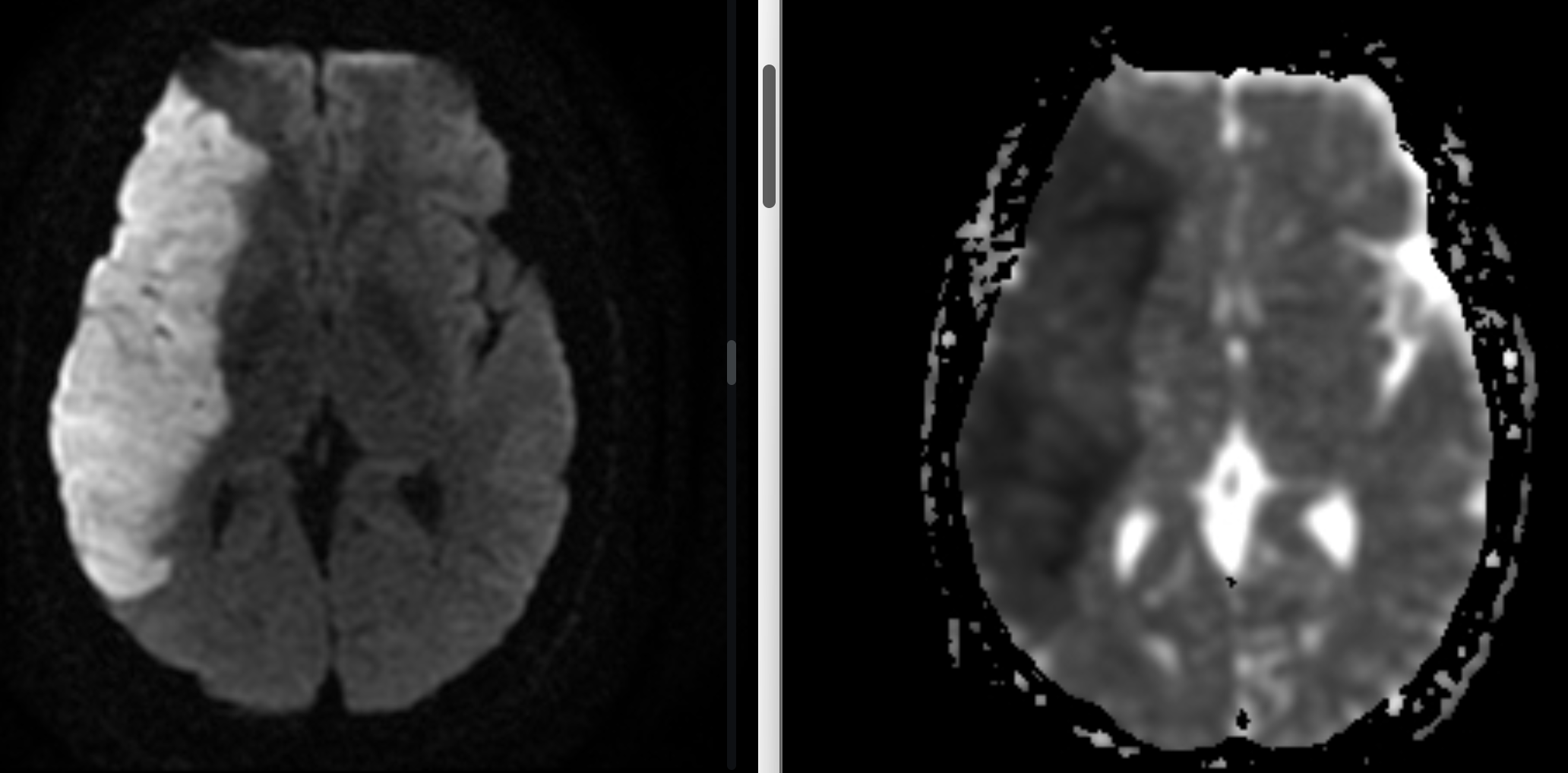
Name these sequence and the pathology demonstrated.
Large right fronto-temporo(-parietal) lesion
DWI - hyperintense
ADC - hypointense
Therefore, restricted diffuse, likely stroke
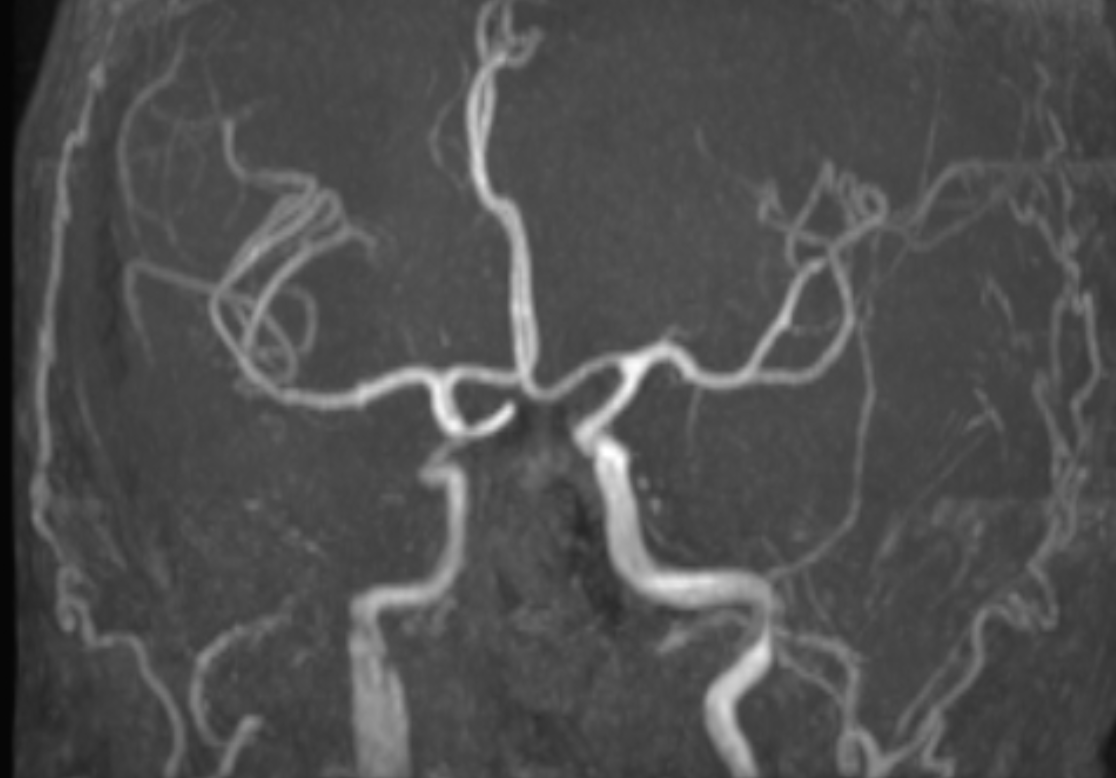
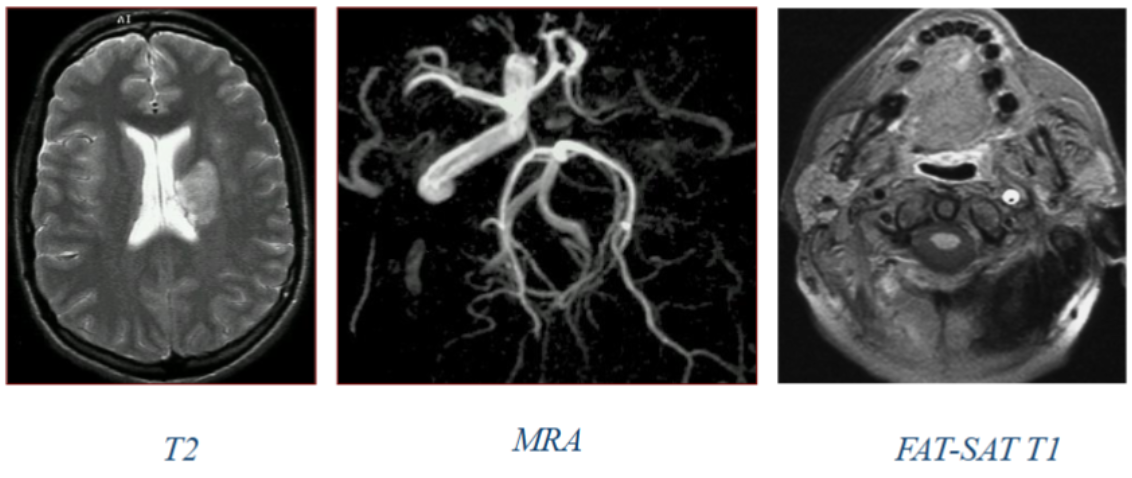
Name this sequence and the pathology demonstrated.
TOF MIP - dissection of the (right) internal carotid artery (cervical segment)

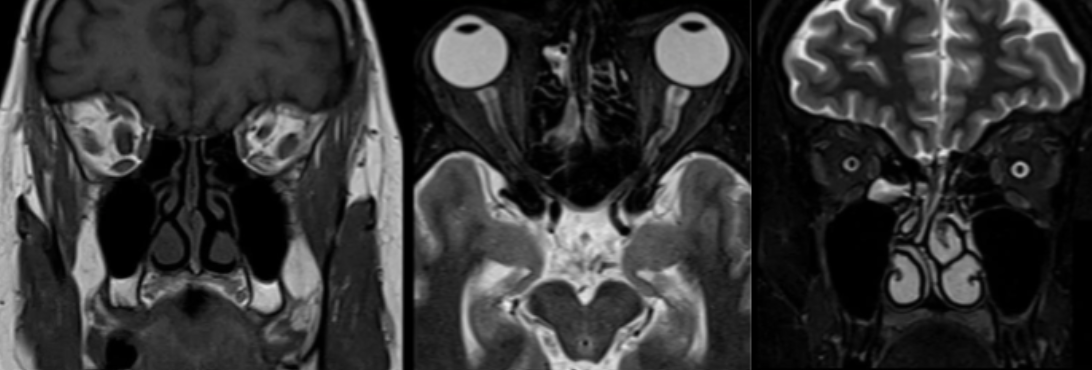
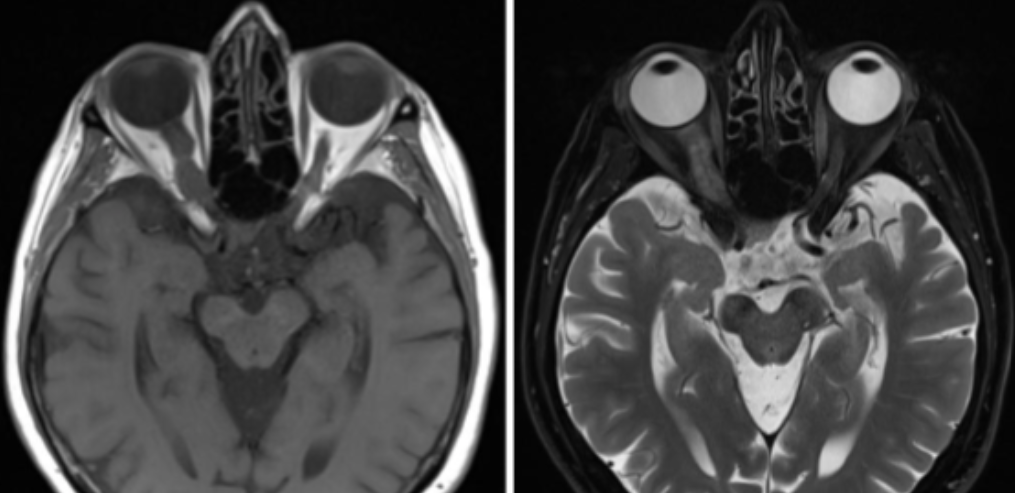
Name this sequence and the pathology demonstrated.
T2, hyperintense fluid surrounding the right optic nerve (optic neuritis)
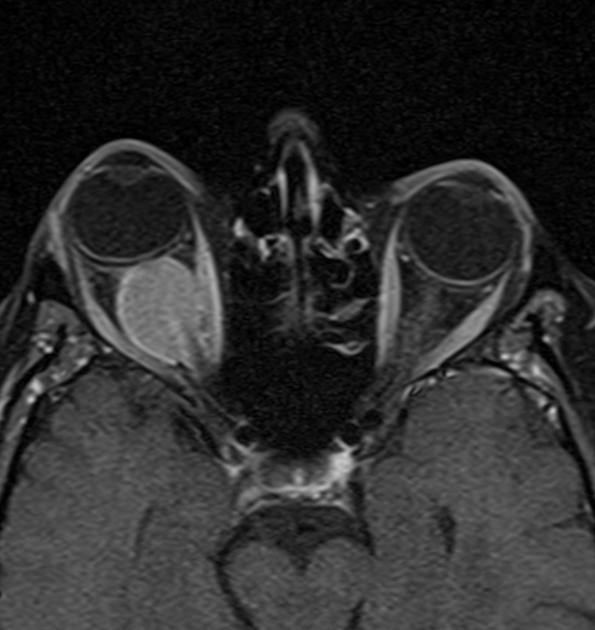
Name this pathology (T1 FS C+).
Enhancing orbital mass involving the right optic nerve
Name this pathology (T1 C+).
Diffusely enhancing mass in the right internal auditory canal with mass effect, likely a vestibular schwannoma
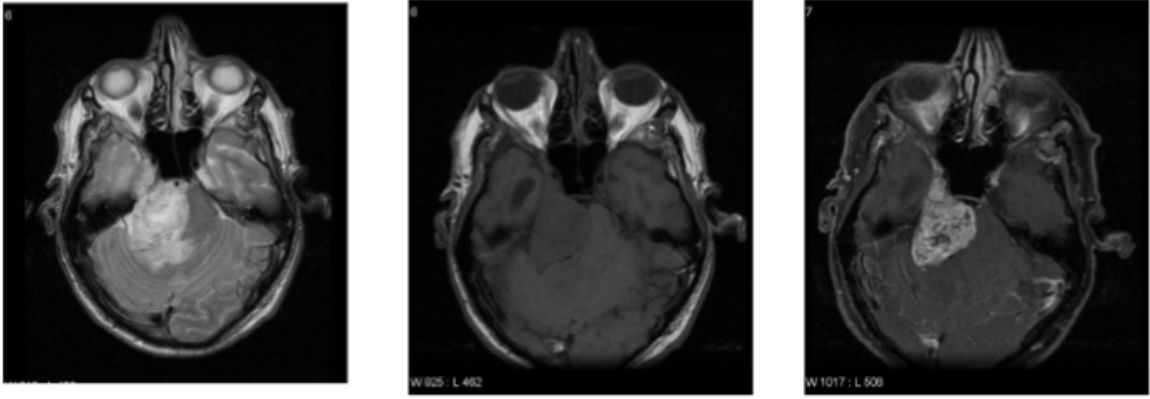
Name this pathology (T1 C+).
Hetergeneously-enhancing lesion involving the cerebellopontine region (and Meckel’s cave) with mass effect (trigeminal tumour)
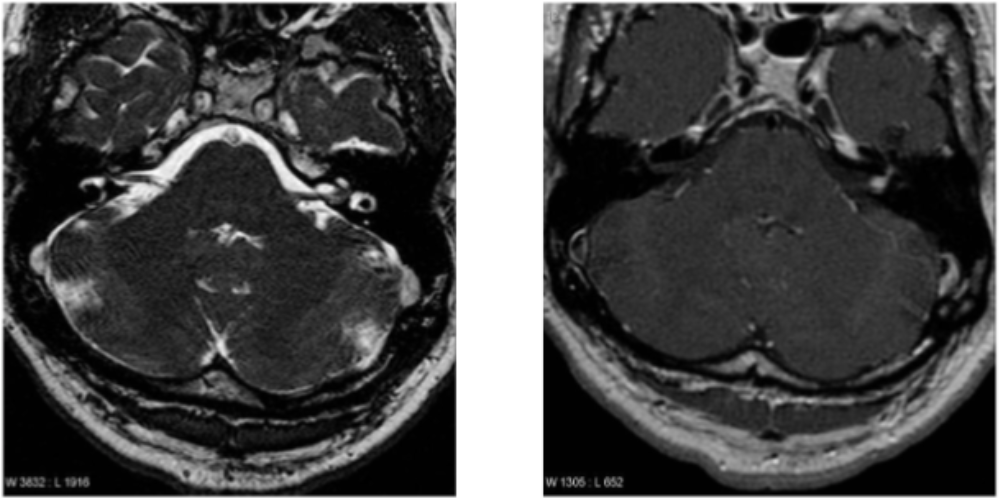
Name this pathology (T2)
Hyperintense lesion in the left cerebello-pontine angle cistern (+ left Meckel’s cave and left cavernous sinus) —> affecting the trigeminal nerve?
What structures must be aligned to correctly angle the transverse scan plane of the head?
Anterior commissure and posterior commissure
How should the slices be angled in a coronal scan plane of the head?
Along the long axis of the brainstem
What is the appearance of a hyperacute cerebral haemorrhage on T1 and T2?
Isointense on T1 and hyperintense on T2
What is the appearance of an acute cerebral haemorrhage on T1 and T2?
Hypointense/Isointense on T1 and hypointense on T2
What is the appearance of an early subacute cerebral haemorrhage on T1 and T2?
Hyperintense on T1 and hypointense on T2
What is the appearance of a late subacute cerebral haemorrhage on T1 and T2?
Hyperintense on T1 and hyperintense on T2
What is the appearance of a chronic cerebral haemorrhage on T1 and T2?
Hypointense on T1 and hypointense on T2
What sequence is important in multiple sclerosis imaging and why?
Sagittal 3D FLAIR - allows any demyelinating plaques to appear hyperintense and stand out
Why are saturation bands used in pituitary imaging?
To eliminate flow artefacts
What pathology resembles a ‘snowman’ coming from the sella turcica?
Macroadenoma
What pathologies involve the hippocampus and are investigated as part of a temporal lobe study?
Temporal lobe epilepsy
Alzheimer’s disease
Cysts or atrophy
When imaging the optic nerve, track from the ___ to the _______.
Globe, optic chiasm
What sequences optimises visualisation of the optic nerve and why?
T1/T2 FS techniques, to use the peri-orbital fat to highlight the nerve
What brain pathology looks like a snowcone?
Vestibular schwannoma in the acoustic meatus
Which cranial nerve passess through the cavernous sinus?
Trigeminal nerve
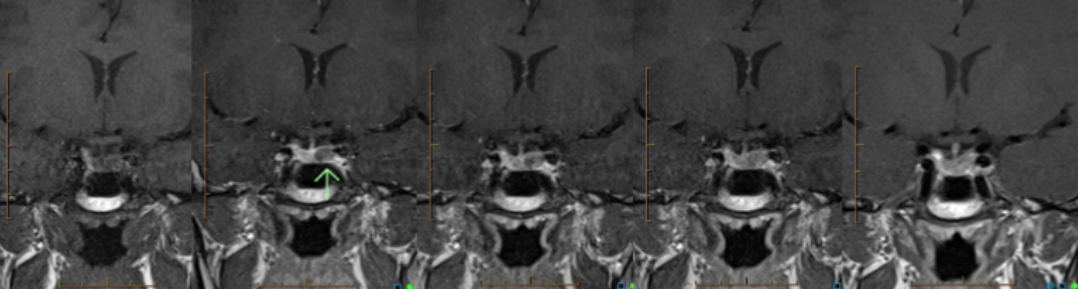
What is the pathology demonstrated? What is this imaging series called and why would it be performed?
Microadenoma of the pituitary gland demonstrated on a dynamic series to demonstrate contrast enhancement of the pituitary gland around the microadenoma
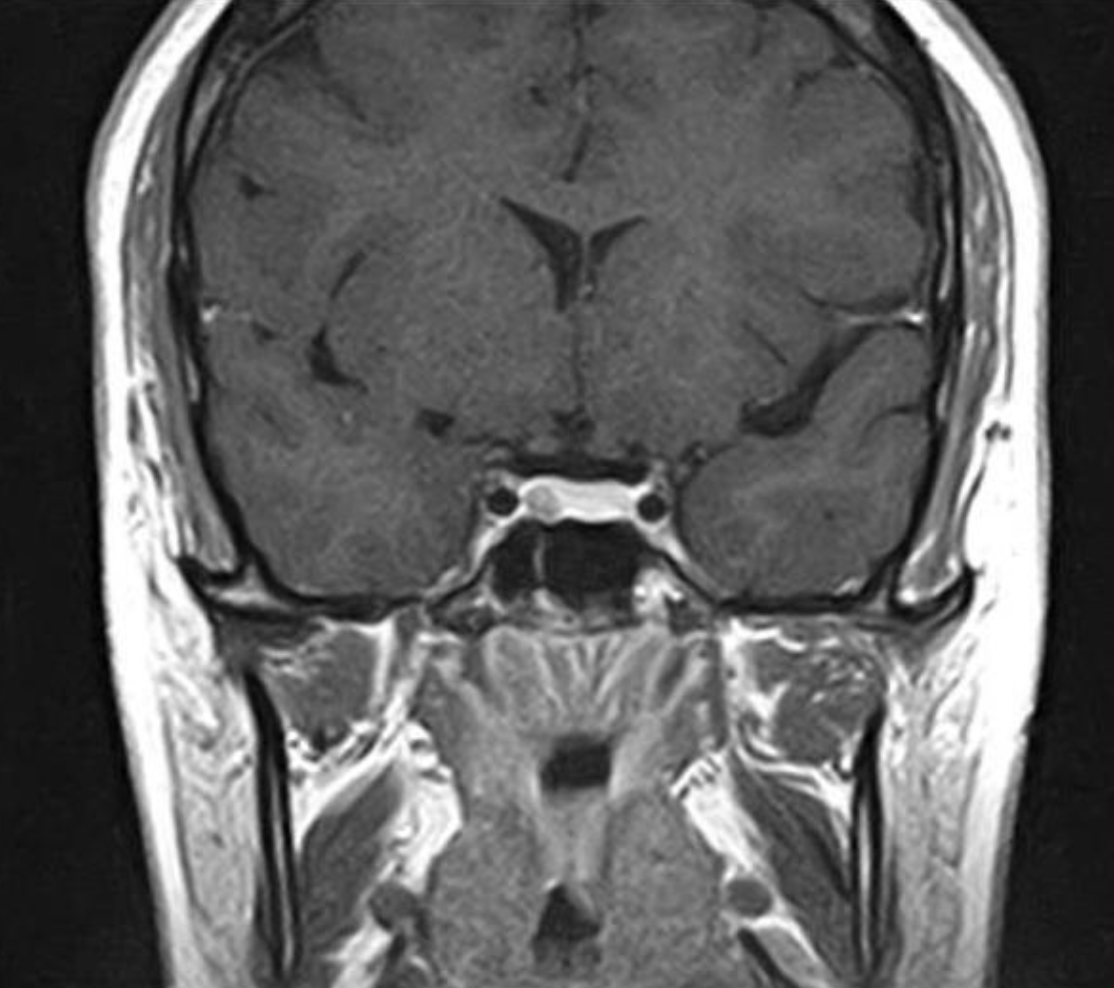
Describe this pathology.
Macroadenoma of the pituitary gland with homogeneous contrast enhancement
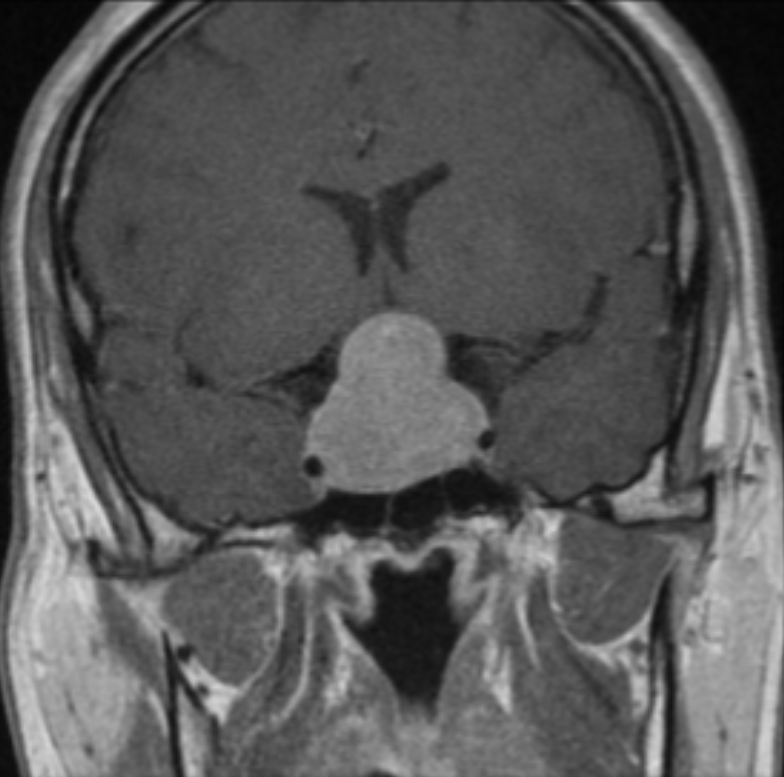
Describe this pathology. What is the appearance of the pituitary gland called?
Macroadenoma of the pituitary gland, ‘snowman’ sign
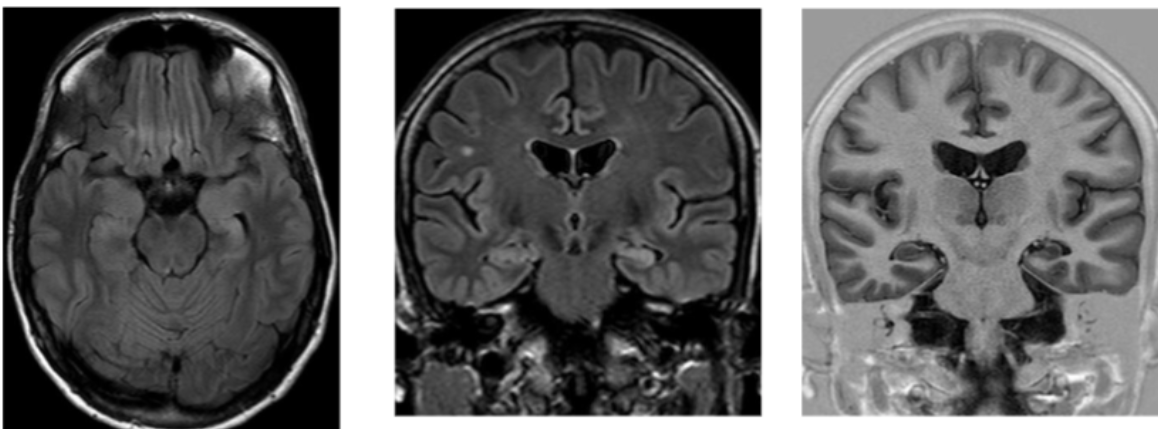
What are the ideal imaging planes for the temporal lobe?
Axial brain
T1 3D sagittal
Oblique coronal FLAIR (angled to temporal lobe)
Which part of the brain is primarily assessed in temporal lobe imaging? What are some pathologies that can be seen?
Hippocampus, to see temporal lobe epilepsy and Alzheimer’s disease (atrophy of the hippocampus)
This is a heavily T1-weighted 3D gradient-echo. Why is it important in temporal lobe imaging?
To acquire a 3D volume in the shortest plane for reconstruction
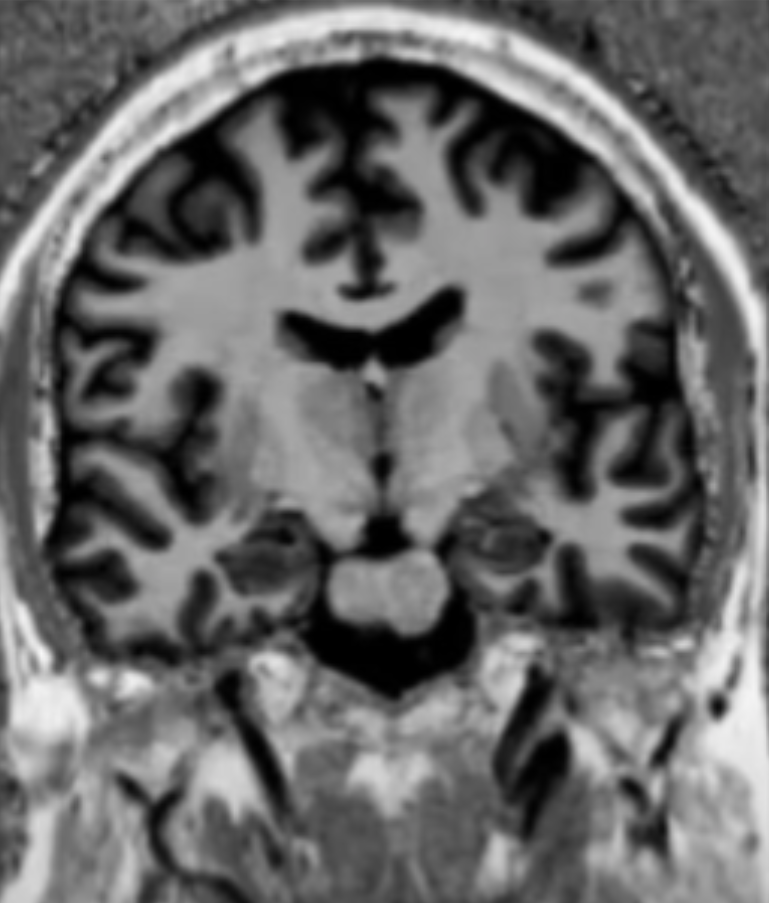
What is this temporal lobe pathology?
Mesial temporal sclerosis
What are some general imaging requirements for cranial nerve imaging?
Thin slices for high resolution
Post-contrast images in two planes
Which cranial nerve is the focus of these images?
Optic nerve
Describe the pathology demonstrated.
Enlargment of the right optic nerve —> right optic nerve meningioma
Which cranial nerves sit within the inner ear complex? Which sits superior to the other
Facial nerve (CNVII) and vestibulocochlear nerve (CNVIII), facial nerve sits more superior to the vestibulocochlear nerve
What is a vestibular schwannoma?
A slow-growing, benign tumour that develops on the vestibulocochlear nerve (CNVIII) which may cause oedema, expansion of the inner auditory canal and deformation of the adjacent brain tissue
Which cranial nerve is shown here?
Facial nerve (CNVII)
Which cranial nerve is shown here?
Facial nerve (CNVII)
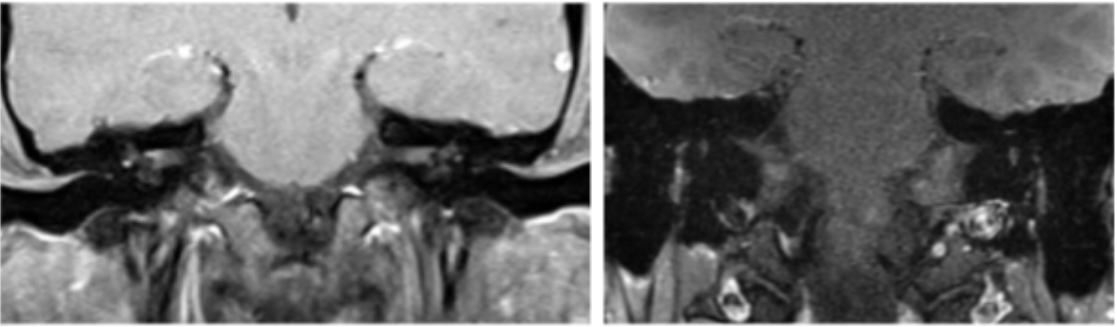
Which cranial nerve pathology is shown here?
Left facial nerve neuritis (enlargement?)
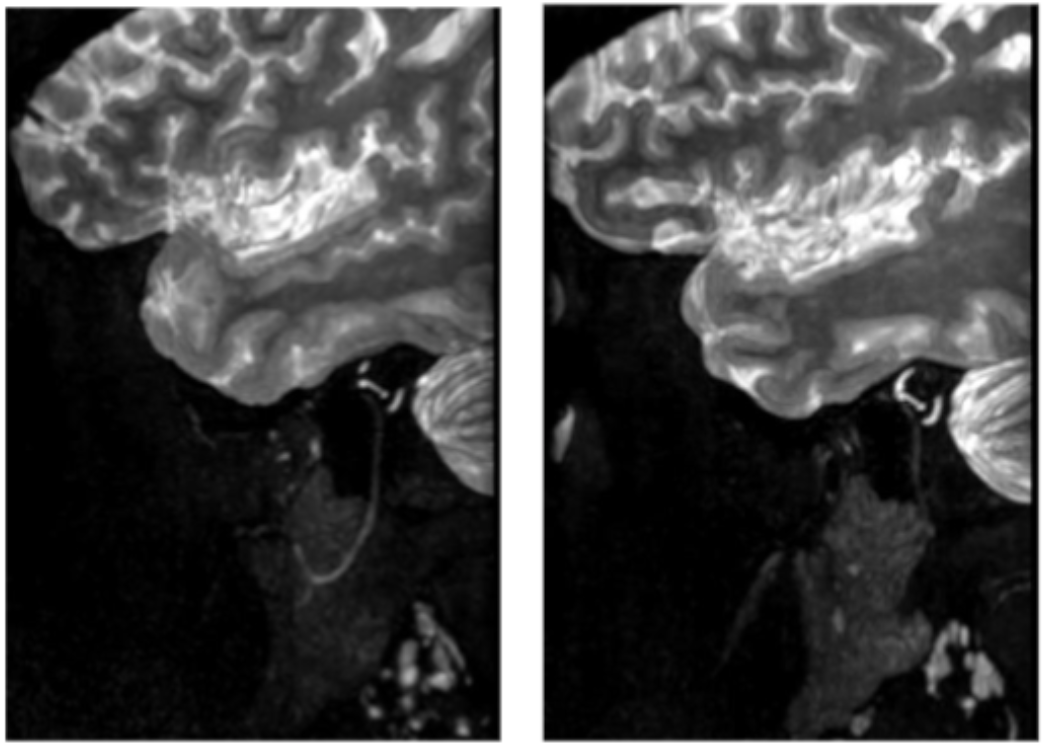
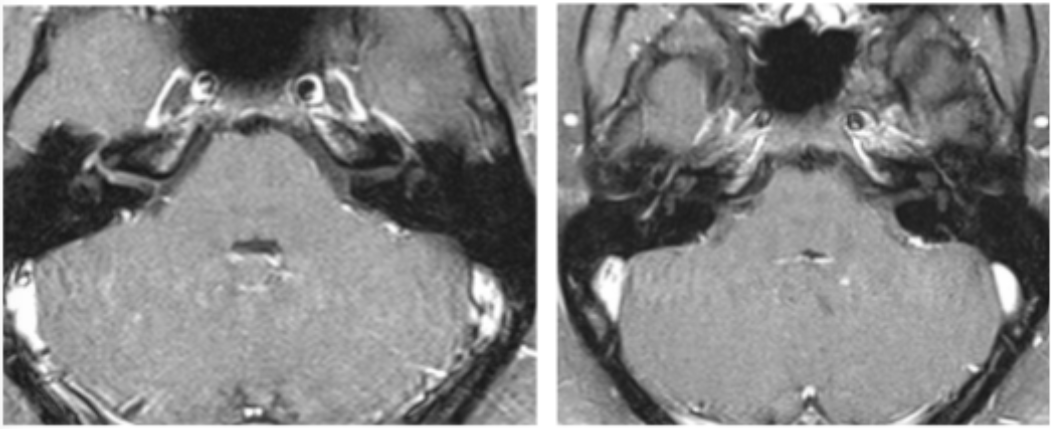
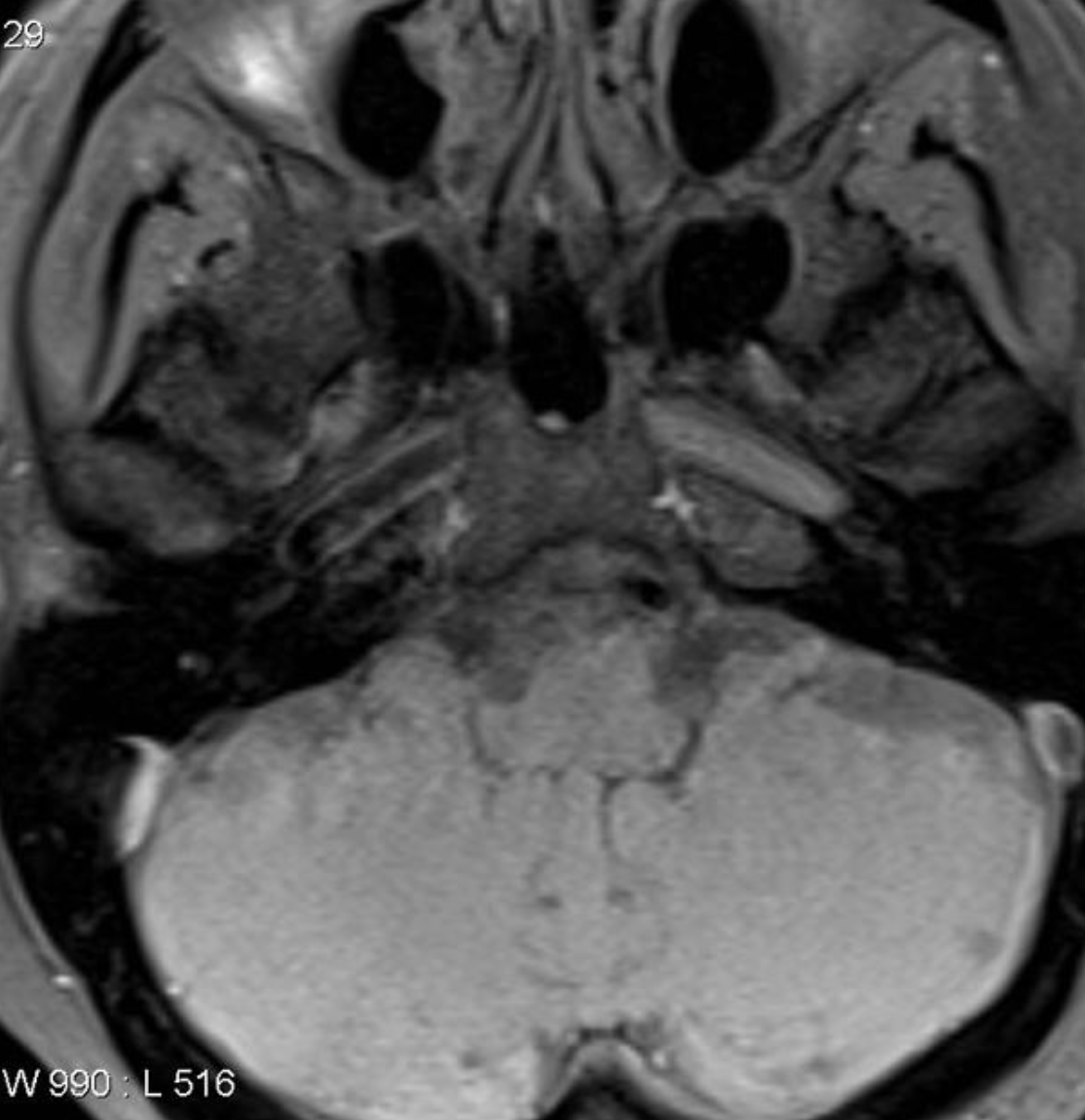
What cranial nerve pathology is demonstrated in the right image? (The left image is normal)
Facial nerve neuritis (thickening and increased intensity)
What is the cranial nerve pathology demonstrated?
Facial nerve schwannoma
What cranial nerve pathology is shown?
Trigeminal schwannoma
What is the hyperintensity in the left cerebral hemisphere? What is it commonly attributed to?
Cytotoxic oedema, occurs after a cerebral vascular event (e.g. stroke)
When is the window of potential reversibility of a stroke?
Hyperacute phase, the first 3-6 hours
After how many hours is the area of ischaemia irreversibly damaged?
24 hours
What part of the stroke is salvageable tissue?
Ischaemic penumbra
What MRI technique is used to show greater sensitivity to diffusion abnormalities (e.g. for stroke imaging)? What physics principle does this use?
Diffusion tensor, using Brownian motion
Why do ischaemic areas look bright on diffusion sequences?
Cells undergo cytotoxic reaction to ischaemia, swelling and reducing free diffusion of extra-cellular fluid, thus this extra-cellular fluid is less affected by the diffusion gradients (appearing bright)
What do B-values mean? What B-value is used for brain imaging?
Describe the sensitivity of the pulse to diffusion, brain imaging uses B=1000
What does an ADC map show? Do ischaemic areas appear hyperintense or hypointense on an ADC map?
The molecular diffusion independent of other MRI signal influences (e.g. T2 shine-through effect). Ischaemic areas appear dark on ADC.
What are some causes of arterial dissection infarction?
Spontaneous
Trauma
Arteritis (from fibromuscular dysplasia)
What is the importance of detecting arterial dissection as early as possible?
So prophylactic anti-coagulation can be administered ASAP
What image weighting is necessary in assessing arterial dissection and why?
T1 FS to demonstrate vessel patency
What is the pathology demonstrated?
Left internal carotid artery dissection
What is the pathology demonstrated?
Right internal carotid artery dissection
What is spectroscopy?
Uses gradients to selectively excite a small volume of tissue and produces a spectrum from that voxel, with metabolites plotted according to their precessional frequencies and resultant ‘chemical shift’ from their local environment
In spectroscopy, what does myoinositol indicate? Why would this peak be higher than normal?
Sugar alcohol, higher in Alzheimer’s and malignancies
In spectroscopy, what does choline indicate? Why would this peak be higher than normal?
Membrane activity, higher in malignancies
In spectroscopy, what does creatine indicate?
Used as a reference level
In spectroscopy, what does N-acetyl-aspartate indicate? Why would this peak be lower than normal?
Neuronal integrity and viability, lower in tumours
In spectroscopy, what does lactate indicate? What would its presence on a spectrum mean?
Cell death and tissue necrosis, presence indicates tumour or infarct
What does Hunter’s angle indicate on spectroscopy?
Normal metabolite peaks, involving NAA, creatine, choline, and myoinositol
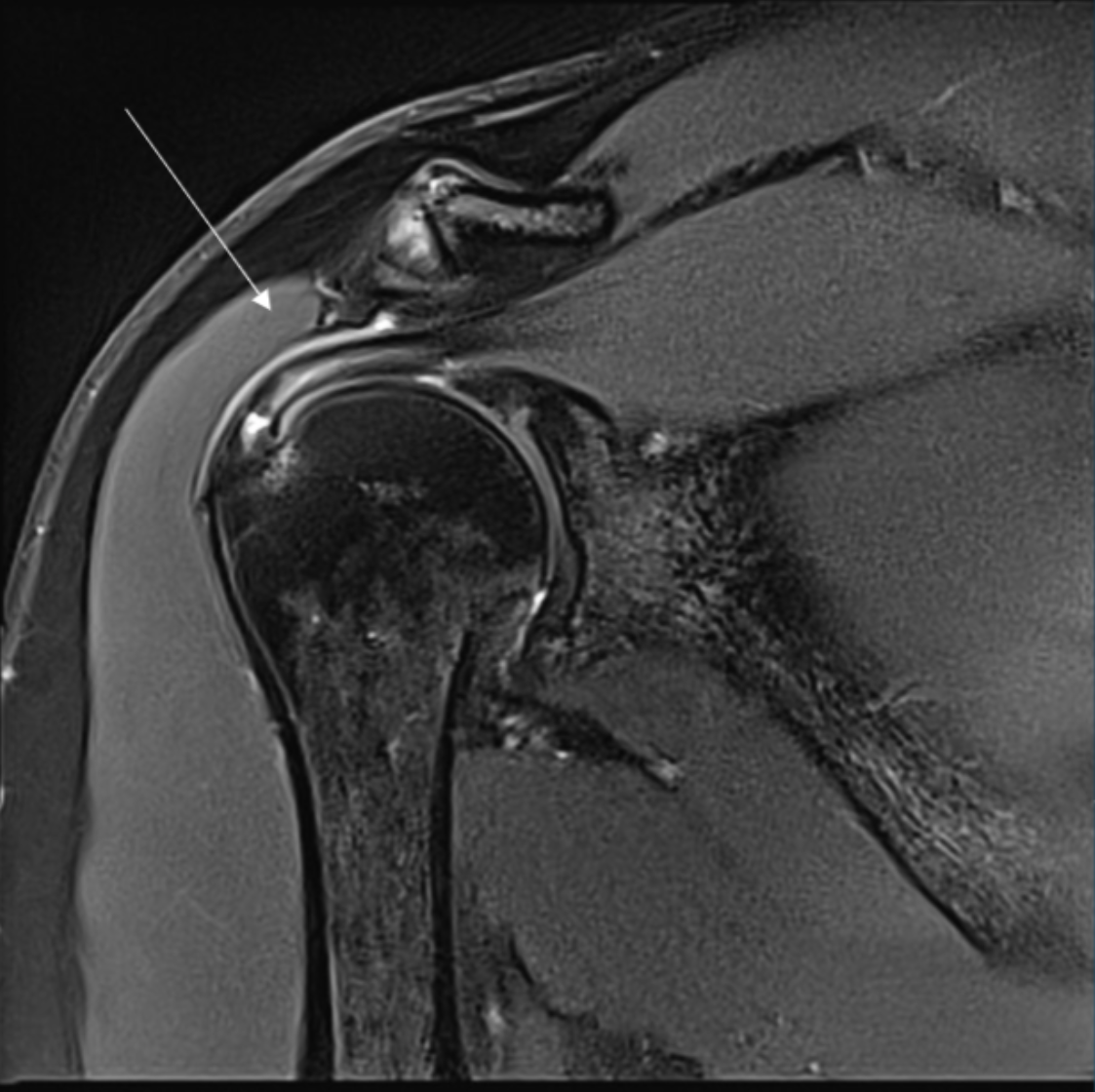
Describe the pathology indicated by the arrow (Cor T2 FS).
Supraspinatus tendon tear
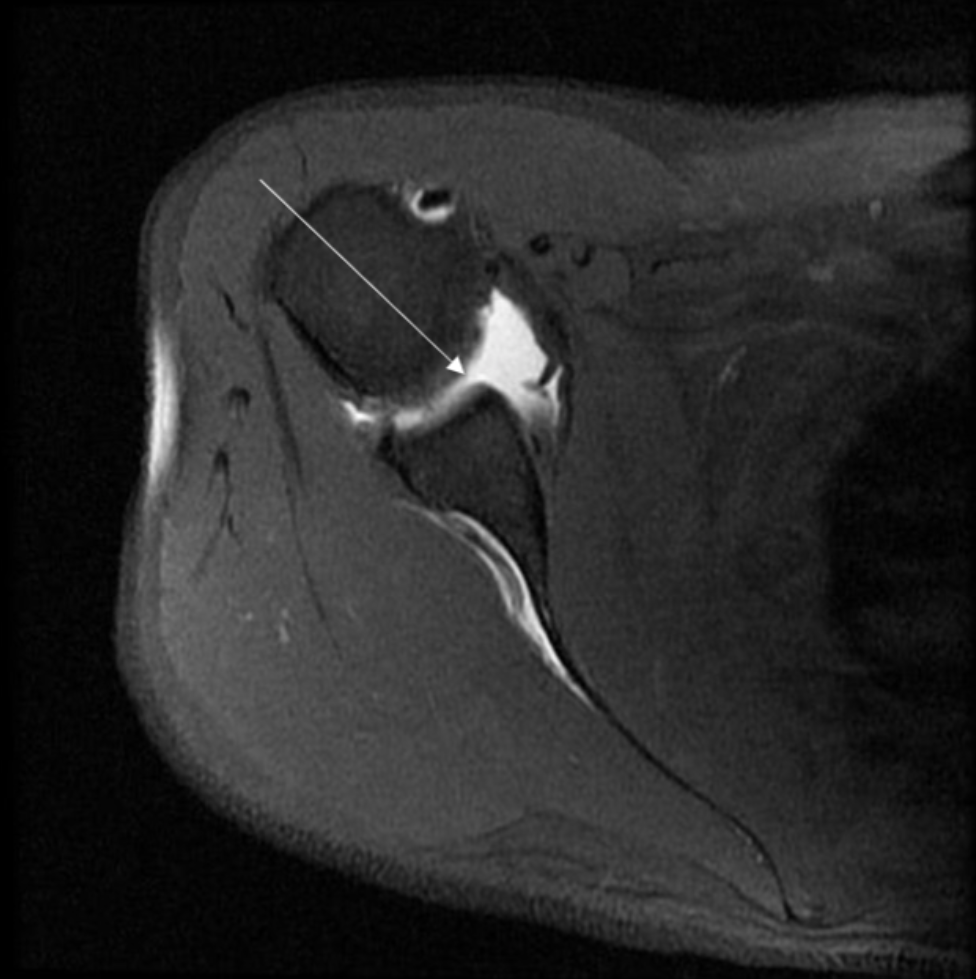
Describe the pathology indicated by the arrow (Ax T1 FS - arthrogram).
SLAP tear

Describe the pathology indicated by the arrow (Ax T1).
Bankart lesion
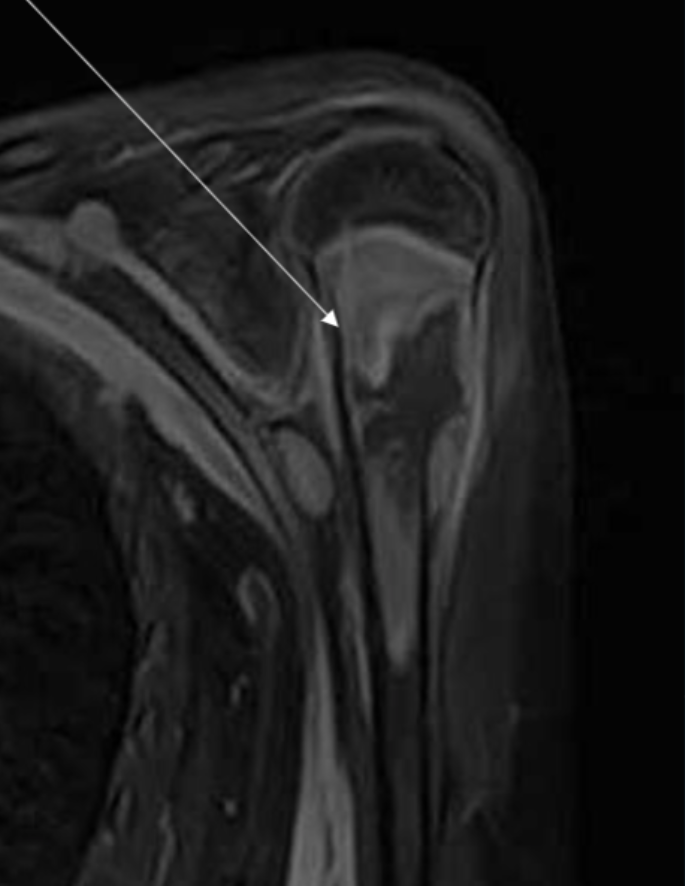
Describe the pathology indicated by the arrow (Cor T1 FS +C).
Osteosarcoma
In an axial shoulder, how should the slices be angled?
Perpendicular to the glenoid surface
In an axial shoulder, what is the scan range?
Above ACJ to below GHJ capsule
In a coronal shoulder, how should the slices be angled?
Parallel to the supraspintus tendon
In a coronal shoulder, what is the scan range?
Coracoid process (anteriorly) to acromion (posteriorly)
In a sagittal shoulder, what is the scan range?
Greater tuberosity (laterally) to past glenoid (medially)
Coracoid process (anteriorly) to acromion (posteriorly)
In a sagittal shoulder, how should the slices be angled?
Parallel to the glenoid surface
In an axial elbow, what is the scan range?
Humeral metaphysis to radial tuberosity
In an axial elbow, how should the slices be angled?
Perpendicular to humeral shaft
In a coronal elbow, how should the slices be angled?
Parallel to the medial and lateral epicondyles
In a sagittal elbow, what is the scan range?
Humeral metaphysis to radial tuberosity
In a sagittal elbow, how should the slices be angled?
Perpendicular to the coronal plane (which is parallel to the medial and lateral epicondyles)
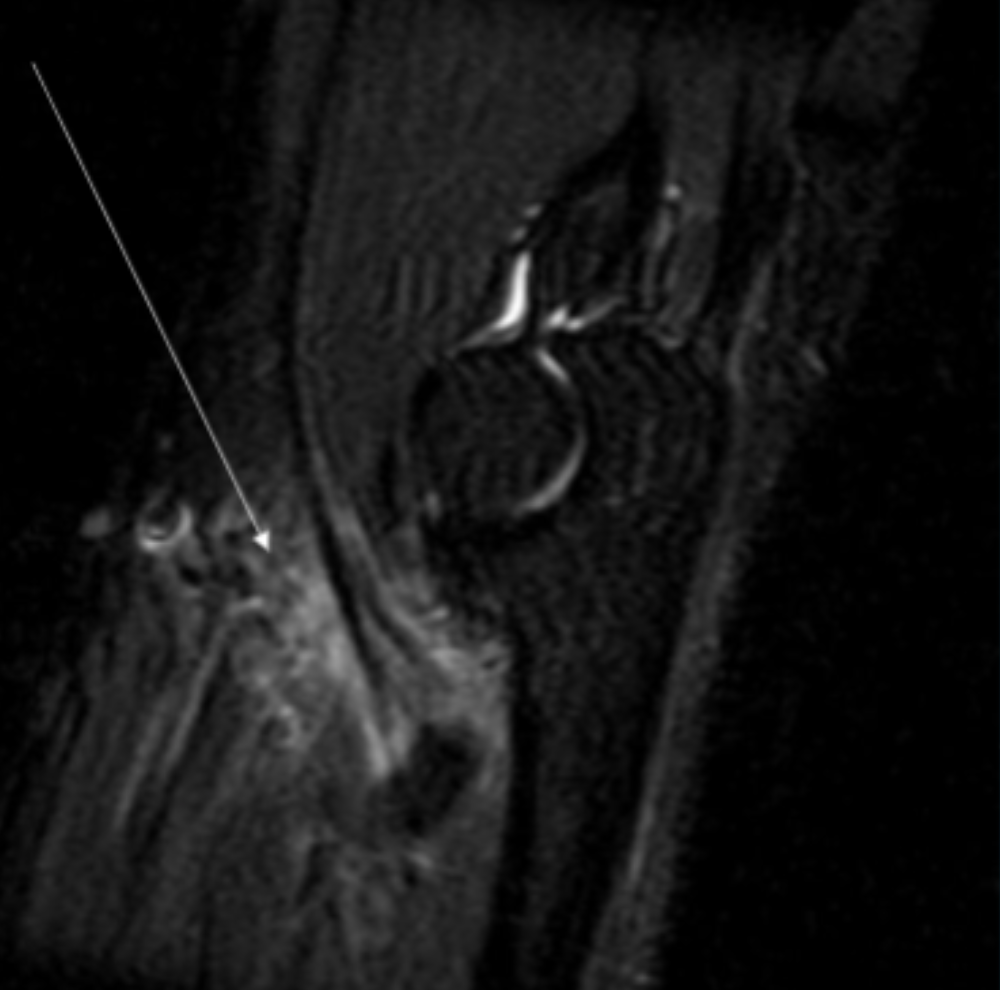
Describe the pathology indicated by the arrow (Sag T2 FS).
Biceps tendonitis
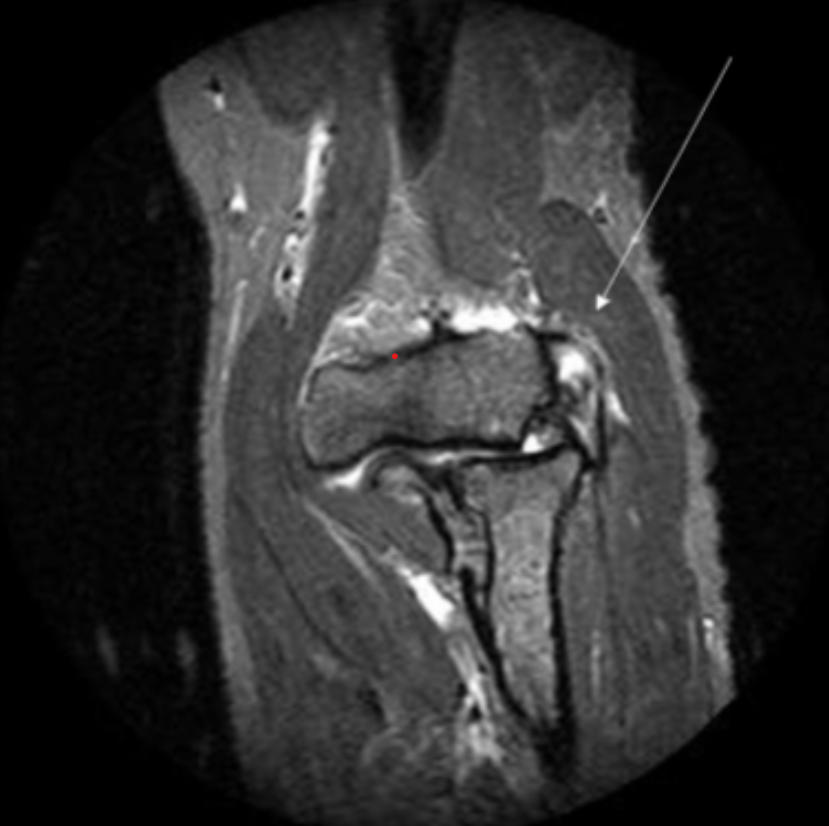
Describe the pathology indicated by the arrow (Cor T2 FS).
Lateral epicondylitis