5: Lower respiratory tract infection, Viral Adaptations
1/129
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
130 Terms
A 37 year old woman attends her GP with a history of 3 weeks of pain in her forehead following a flu-like illness. She also complains of symptoms of a postnasal drip. She takes lansoprazole 15mg daily (maintenance dose) for dyspepsia but is otherwise well. Her GP percusses her frontal sinus which is found to be painful on the left side. She is allergic to penicillin so her GP prescribes a 5 day course of ciprofloxacin 250mg bd. i. What is the likely initial URTI diagnosis?
acute frontal sinusitis but can lead to secondary bacterial infection
dyspepsia
indigestion
what organisms cause acute frontal sinusitus
95% viral origin (rhinoviruses, coronaviruses, influenza viruses, adenoviruses, human parainfluenza viruses, human respiratory syncytial viruses, other enteroviruses, metapneumovirus)
what organisms can cause secondary infection of sinusitis
3 causative bacteria:
1. streptococcus pneumoniae
2. haemophilus influenzae
3. moraxella catarrhalis
others include:
staphylococcus aureus, other streptococci species. anaerobic bacteria and less commonly g-ve bacteria
affect of HiB
haemophilus influenzae was most common bacterial agents to cause sinus infections. introduction of H.influenzae type B (HiB) vaccine dramatically decreased H.influenzae type B infections.
You are a medical student in the Emergency Department when a 34 year man presents following several seizures. He has severe cerebral palsy and epilepsy. He lives in a nursing home with 24 hour care. His vital signs are Temperature 37.8˚C, Pulse 110/min, Blood Pressure 135/70, Respiratory Rate 35/min, Oxygen Saturation 96% on 15L. On examination of his chest he has coarse crepitations over the right lung. You think he may have aspirated.
Why is this patient at risk of aspiration?
altered level of consciousness during siezures, loss of gag reflex and inability to maintain an airway
You are a medical student in the Emergency Department when a 34 year man presents following several seizures. He has severe cerebral palsy and epilepsy. He lives in a nursing home with 24 hour care. His vital signs are Temperature 37.8˚C, Pulse 110/min, Blood Pressure 135/70, Respiratory Rate 35/min, Oxygen Saturation 96% on 15L. On examination of his chest he has coarse crepitations over the right lung. You think he may have aspirated.
what SIRS criteria are present
heart rate >90/min; resp rate >20/min
conditions associated with aspiration
1)altered or reduced consciousness: alcoholism, drug overdrug overdose, stroke, headtrauma
2) oesophageal conditions: dysphalgia, strictures, neoplasm, diverticula
3) neurologic conditions: MS, dementia, parkinson's disease, pseudobulbar palsy
mechanical conditions: nasogastric tube, intubation, GI endoscope, bronchoscopy
what airway mechanisms prevent/remove material from lower airways
gag reflex, coughing, ciliary movement and immune mechanisms, phagocytotic efficiency
aspiration pneumonia- microorganisms responsible
likely organisms anaerobic alone or in combination with aerobic organisms. in anaerobic the pathogenesis, is related to large volume of aspirated anaerobes (poor dentition or poor oral care)
how can aspiration pneumonia be acquired
pathogens involved include hospital acquired (long term resident in a nursing home) flora through oropharyngeal colonisation (enteric g-ve bacteria, staphylococci). bacterial superinfection may occur after initial chemical injury- chemical pneumonitis (aspiration pneumonitis or Mandelson syndrome) is due to parenchymal inflammatory reaction caused by gastric contents independent of infection.
severe sepsis blood culture
raised WBC, neutrophilia, raised CRP, raised lactate, low K. lactate >mmol/l
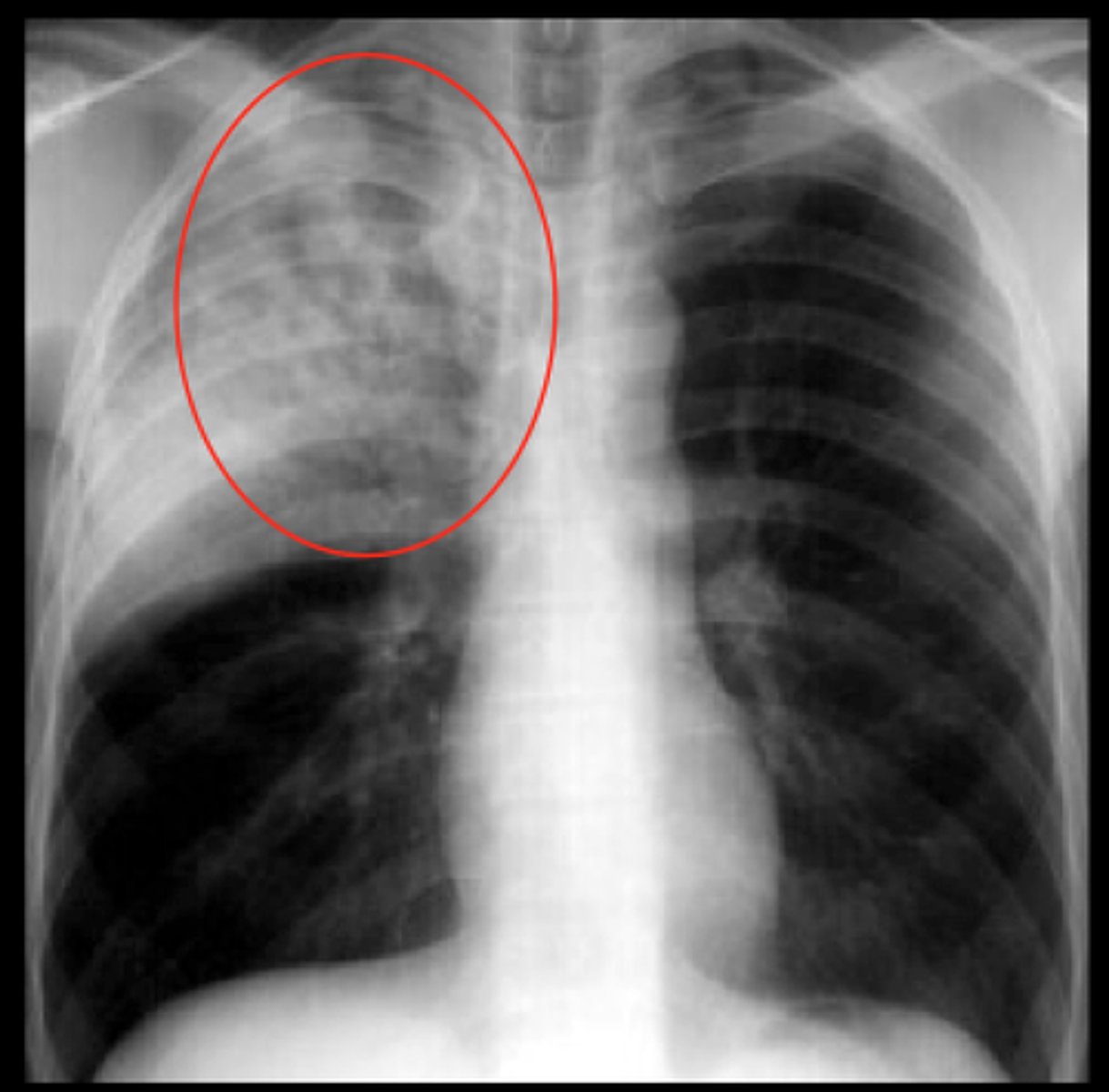
Consolidation xray
Solid white area
Pneumonia/pleural effusion
34 year man presents following several seizures. He has severe cerebral palsy and epilepsy. He lives in a nursing home with 24 hour care. His vital signs are Temperature 37.8˚C, Pulse 110/min, Blood Pressure 135/70, Respiratory Rate 35/min, Oxygen Saturation 96% on 15L. On examination of his chest he has coarse crepitations over the right lung. You think he may have aspirated.
outline managment
admit, O2 (sat >94%), investigation (bloods, blood culture, sputum, mcs, cxr)
iv antibiotics (piperacillin/tazobactam 4.5g TDS trated as hospital acquired long term NH)
IV fluids and K.
EWS chart. monitor progress with bloods CRP and WBC. check blood culture result. chest physiotherapy.
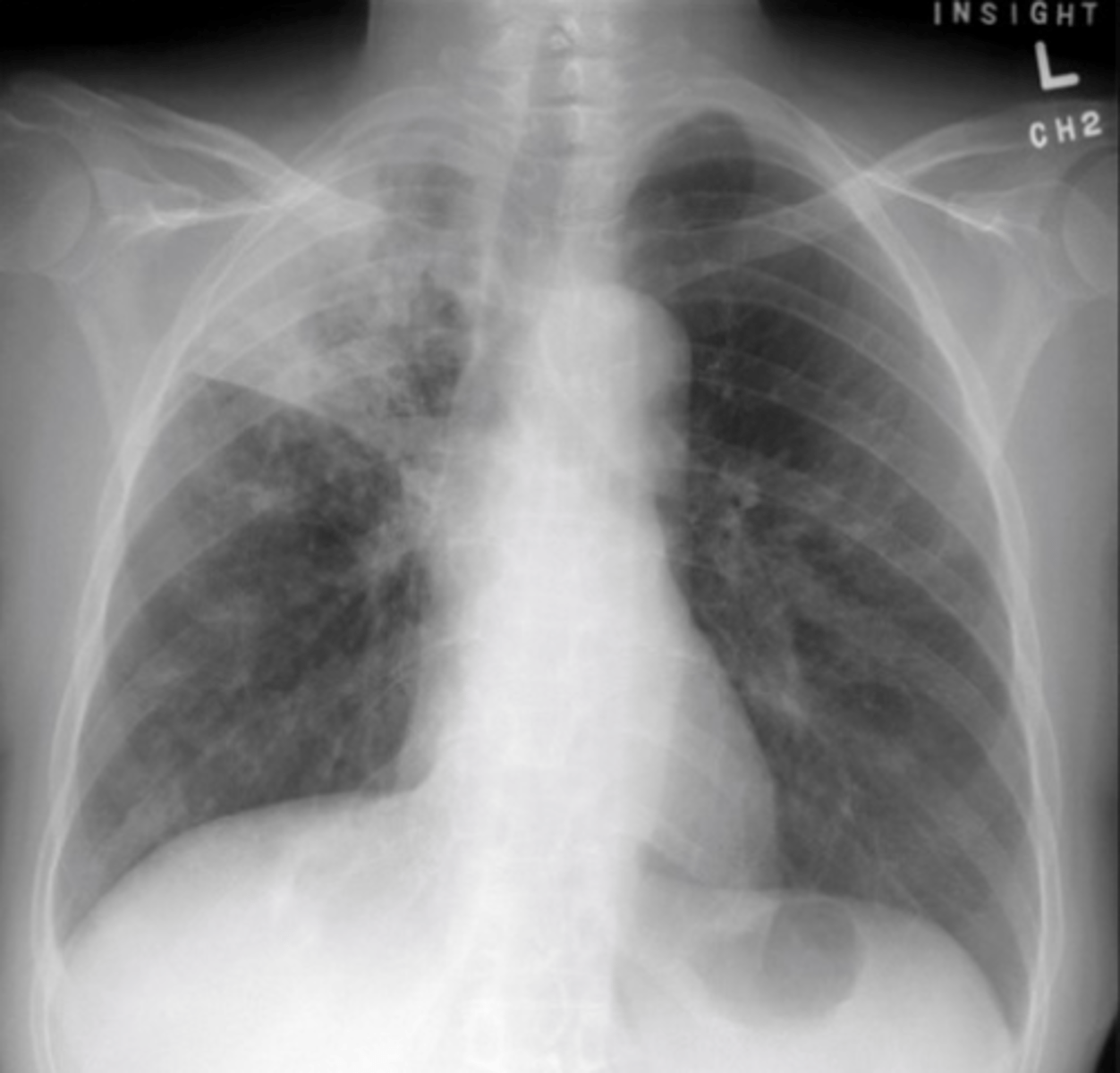
A 75 year old man was admitted to hospital with a fever and a productive cough. He is confused on admission, and has a respiratory rate of 32. On examination he has crackles at the right base. A chest x-ray is requested for him.
expectation of xray?
lobar consolidation, consolidation at right base
A 75 year old man was admitted to hospital with a fever and a productive cough. He is confused on admission, and has a respiratory rate of 32. On examination he has crackles at the right base. A chest x-ray is requested for him.
cause?
pneumonia
A 75 year old man was admitted to hospital with a fever and a productive cough. He is confused on admission, and has a respiratory rate of 32. On examination he has crackles at the right base. A chest x-ray is requested for him.
organism responsible? how do we culture?
Streptococcus pneumoniae (pneumococcus)
-blood culture
-sputum culture
sputum culture
Sputum is collected and placed on a growth medium to analyze the type of microorganisms that may be prevented.
A 75 year old man was admitted to hospital with a fever and a productive cough. He is confused on admission, and has a respiratory rate of 32. On examination he has crackles at the right base. A chest x-ray is requested for him.
how do you decide what antibiotics to give this pt?
1)hospital guidelines
2) broad spectrum antibiotics
3) tailor treatment based on sensitivities from cultures
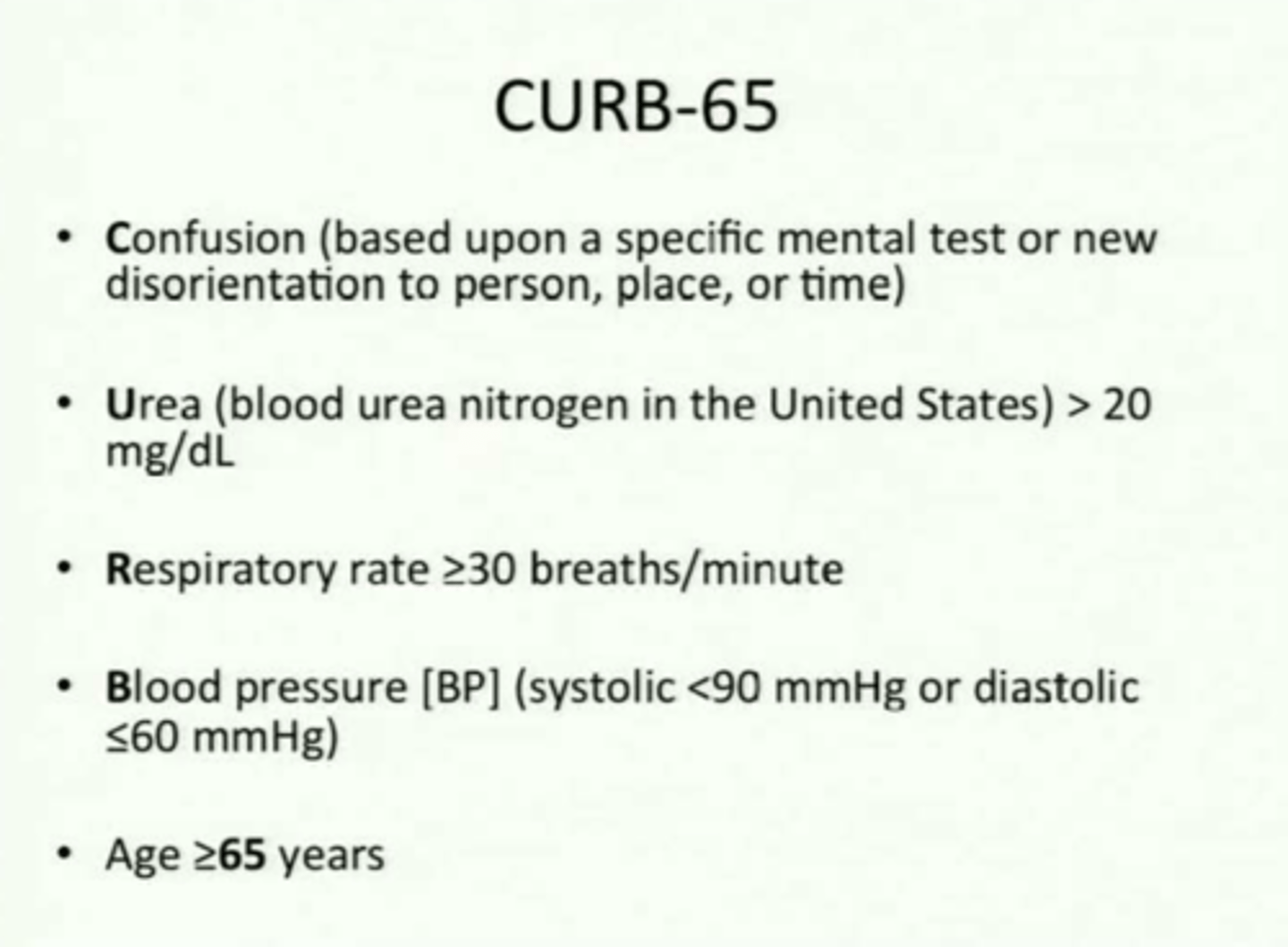
CURB-65 criteria
confusion, urea >7mmol/l, resp >30, SBP <90 or DBP <60, age >65
A 75 year old man was admitted to hospital with a fever and a productive cough. He is confused on admission, and has a respiratory rate of 32. On examination he has crackles at the right base. A chest x-ray is requested for him.
what further information do you need to calculate CURB-65 score?
urea from blood tests and blood pressure
A 44 year old woman presents acutely unwell with an 8 day history of fever, shortness of breath and productive cough. The patient returned from a 2 week holiday in Majorca, Spain 11 days ago. She had consulted her GP 4 days ago who prescribed amoxicillin but her condition had worsened. On examination she was confused and breathless (respiratory rate 40/min) with oxygen saturation 85% on air, temperature 39.8oC. Blood pressure was 112/64 and heart rate 96 bpm. On auscultation of the chest bibasal crepitation were heard.
what additional questions would you ask in history?
travel history
occupation (eg farmers wife)
pregnant (severity issues eg influenza)
anyone else in the family unwell
previous medical history
smoker
A 44 year old woman presents acutely unwell with an 8 day history of fever, shortness of breath and productive cough. The patient returned from a 2 week holiday in Majorca, Spain 11 days ago. She had consulted her GP 4 days ago who prescribed amoxicillin but her condition had worsened. On examination she was confused and breathless (respiratory rate 40/min) with oxygen saturation 85% on air, temperature 39.8oC. Blood pressure was 112/64 and heart rate 96 bpm. On auscultation of the chest bibasal crepitation were heard.
urgent investigations?
full blood count with urea and electrolytes, CRP, blood cultures, CXR,
A 44 year old woman presents acutely unwell with an 8 day history of fever, shortness of breath and productive cough. The patient returned from a 2 week holiday in Majorca, Spain 11 days ago. She had consulted her GP 4 days ago who prescribed amoxicillin but her condition had worsened. On examination she was confused and breathless (respiratory rate 40/min) with oxygen saturation 85% on air, temperature 39.8oC. Blood pressure was 112/64 and heart rate 96 bpm. On auscultation of the chest bibasal crepitation were heard.
What is your working diagnosis and how may the severity of this condition be assessed?
community acquired pneumonia. severe case. CURB-65 score 3. confusion, raised urea and tachyponoea
innate immune system are displayed to prevent RI from developng
ciliated epithelium moves particles towards pharynx and therefore down DT away from resp system. goblet cells secrete mucus which creates a physical barrier to infections but also contains lysozymes and IgA antibodies which attacks invading pathogens. normal resp flora provide competition for arriving pathogenic microorganisms. cough reflex expels harmful substances. rich vasculature of respS results means high levels of neutrophils and alveolar macrophages are available in the lungs to battle invading bacteria,
A 44 year old woman presents acutely unwell with an 8 day history of fever, shortness of breath and productive cough. The patient returned from a 2 week holiday in Majorca, Spain 11 days ago. She had consulted her GP 4 days ago who prescribed amoxicillin but her condition had worsened. On examination she was confused and breathless (respiratory rate 40/min) with oxygen saturation 85% on air, temperature 39.8oC. Blood pressure was 112/64 and heart rate 96 bpm. On auscultation of the chest bibasal crepitation were heard.
managment:
two antibiotics to cover potential pathogens since you are still guessing exact cause. co-amoxiclav and clarithromycin or doxycycline. co-amoxiclav is directed against some common or typical pathogens like pneumococci. clarithromycin directed against atypical pathogens
the 44yo woman condition deteriorates rapidly after admission and the patient is transferred to ITU for ventilation. In view of the more detailed history further microbiology investigations are requested.
what investigations happen to a sample in a microbiology lab?
microscopy
culture (sputum, endotracheal secretions, broncho-alveolar lavage, blood culture)
antigen detection
antibody detection
molecular techniques eg PCR
Legionnaire's disease
Legionella pneumophila serogroup 1. pneumonia. g-ve. faculative intracellular parasite. aerobic. normally within environmental protozoa and amebae within soil and water systems. spread by aerosols which are inhaled. human to human transmission does not occur.
legionella pneumophila uses which feature of the innate immunity to aid its replication
bacteria phagocytosed by macrophages but prevent phagosome fusing with lysosome so evades destruction by macrophage and instead uses macrophage as a site to replicate and spread
once diagnosis is reached, how should the following managment plan be amended:
two antibiotics to cover potential pathogens since you are still guessing exact cause. co-amoxiclav and clarithromycin or doxycycline. co-amoxiclav is directed against some common or typical pathogens like pneumococci. clarithromycin directed against atypical pathogens
amend emperic treatment to specific treatment. usually quinolone class antibiotic eg levofloxacin
Legionnaire's disease is a notifiable disease. does the pt need to be cared for in a side room
no case to case spread so no requirement for isolation
what is the role of the local health protection unit of public health england?
-to collect information on possible source. detailed travel history uk/abroad, other risk factors etc.
-establish whether other travellers at risk eg contact travel companies travel companies if required
-co-ordinate action to reduce the risk contact public health authorities overseas (European database of cases) investigate hotels etc. and plan environmental investigations as appropriate.
A 16 year old girl with a diagnosis of cystic fibrosis sees you in clinic complaining of worsening cough and fevers. Previous sputum cultures have grown pseudomonas aeruginosa, and her last admission with a chest infection was only 2 months ago.
What do this patient's previous sputum cultures indicate?
What do this patient's previous sputum cultures indicate?
chronic infection with pseudomonas
pseudomonas
facultative anaerobe
apart from airways where is another common site to find pseudomonas infection
urinary tract/catheters
describe how biofilm may be produced in CF patient.
mucus collects in airways and provides rich environment for bacteria. bacteria colonise this mucus forming biofilm (micro-environments)
why is it difficult to treat CF with biofilms?
biofilms difficult to infiltrate by both immune cells and antibiotics. in chronic infections, antibiotic resistance may occur due to previous courses
A 50 year old man with bronchiectasis presents at his GP with a history of an increasingly productive cough and episodes of sweating. He has a CXR done and it shows consolidation in the right lung base with air Bronchogram. He has some haemoptysis.
What are the commonest bacteria likely to be causing the pneumoniain this patient?
!!!
classification by site
by kumar and clark. classification by site:
lobar pneumonia localised with the whole of one or more lobes affected or bronchopneumonia diffuse primarily affects lobes of lung and often association with bronchi and bronchioles
classification by aetiology. atypical pneumonia
3/4 pts aetiological factor discovered. 'atypical pneumonia': caused by agents such as mycoplasma, legionella, chlamydia, coxiella bernetii. clinical features may differ from pneumococcal disease, there is a considerable overlap in clinical presentation and these agents count for 1/5 of pneumonia.
classification by aetiology
-atypical,
-chemical causes (aspiration of vomit, radiotherapy, allergic mechanisms.
-mycobacterium tubercolosis considered seperately as mode of presentation and treatment is completely different.
community acquired pneumonia
- (tends to be lobar pneumonia
- streppneumoniae (elderly, co-morbidity,acute onset, high fever, pleuritic pain),
-H influenzae (COPD),
-Kleb pneumoniae (throbocytopenia, leucopenia), -moraxella cattarhalis.
hospital acquired
tends to be bronchopneumonia. g-ve enteric bacteria, pseudomonas. staph aureus and MRSA
A 50 year old man with bronchiectasis presents at his GP with a history of an increasingly productive cough and episodes of sweating. He has a CXR done and it shows consolidation in the right lung base with air Bronchogram. He has some haemoptysis.
what would you prescribe?
term3,lecture8,
Rx amoxicillin for mild to moderate, augmentin for severe.
A 50 year old man with bronchiectasis presents at his GP with a history of an increasingly productive cough and episodes of sweating. He has a CXR done and it shows consolidation in the right lung base with air Bronchogram. He has some haemoptysis.
main infective consequences if he fails to improve?
lung abscess, bronchiectasis, empyema
main viruses that cause 10%
influenza, parainfluenza, respiratory syncytial virus, adenovirus
What is an air bronchogram?
alveoli are filled with pus making the bronchi visible as an air bronchogram. dark lines through area of white.
what sort of pt must you consider aspiration pneumonia and what microorganisms would be a consideration
aspiration of exogenous material or endogenous secretions into the RT is common in pts with strokes (neurological dysohagia), epilepsy, alcholics, drowning, nursing home residents, drug overdose. mixed infection viridians streptococci and anaerobes
useful markers for infections
WCC >20 or <4 indicates severe disease. CRP useful assesing response to treatment. radiology reliable and rarely radiological signs can lag behind clinical characteristics (24-48hrs)
A 50 year old man with bronchiectasis presents at his GP with a history of an increasingly productive cough and episodes of sweating. He has a CXR done and it shows consolidation in the right lung base with air Bronchogram. He has some haemoptysis
consider preventative measures?
physiotherapy exercises done by pt, pneumococcal vaccination, influenza vaccination, possible long term once a day antibiotics
hearing crackles in lung
fluid in alveoli or interstitial spaces.
normal o2 saturation levels
>96
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
is it reasonable to consider malaria?
yes as malaria is found in SA and can cause resp symptoms
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
differential diagnosis not malaria
RTI:
-bacterial (H.influenzae, S.pneumoniae, atypicals including C. pneumoniae, M.pneumoniae, L. pneumophilia
-Viral (including influenza, parainfluenza, rhinovirus, adenovirus.
-pulmony embolism. less likely in view of fever, systemic illness and onset of symptoms prior to fight at home
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
what initial investigations would you request?
bloods:
-malaria film x3, blood cultures, FBC, urea and electrolytes, LFT, CRP, HIV test (opportunistic screening)
-CXR
-ECG
-arterial blood gas
-nose/throat swabs for resp virus PCR
-pregnancy test (certain resp infections including influenza can be more severe in pregnancy)
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
should she be nursed in a side room?
all fibrile travellers should be nursed in isolation until either a diagnosis has been made or they have recovered. esp for travellers with resp ilnesses returning from areas known to have MERS-coV. not for this pt.
MERS-coV
novel coronavirus that can cause severe resp illness. jordan, qatar, saudi, uae, tunisia, uk. linked to travel to ME
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
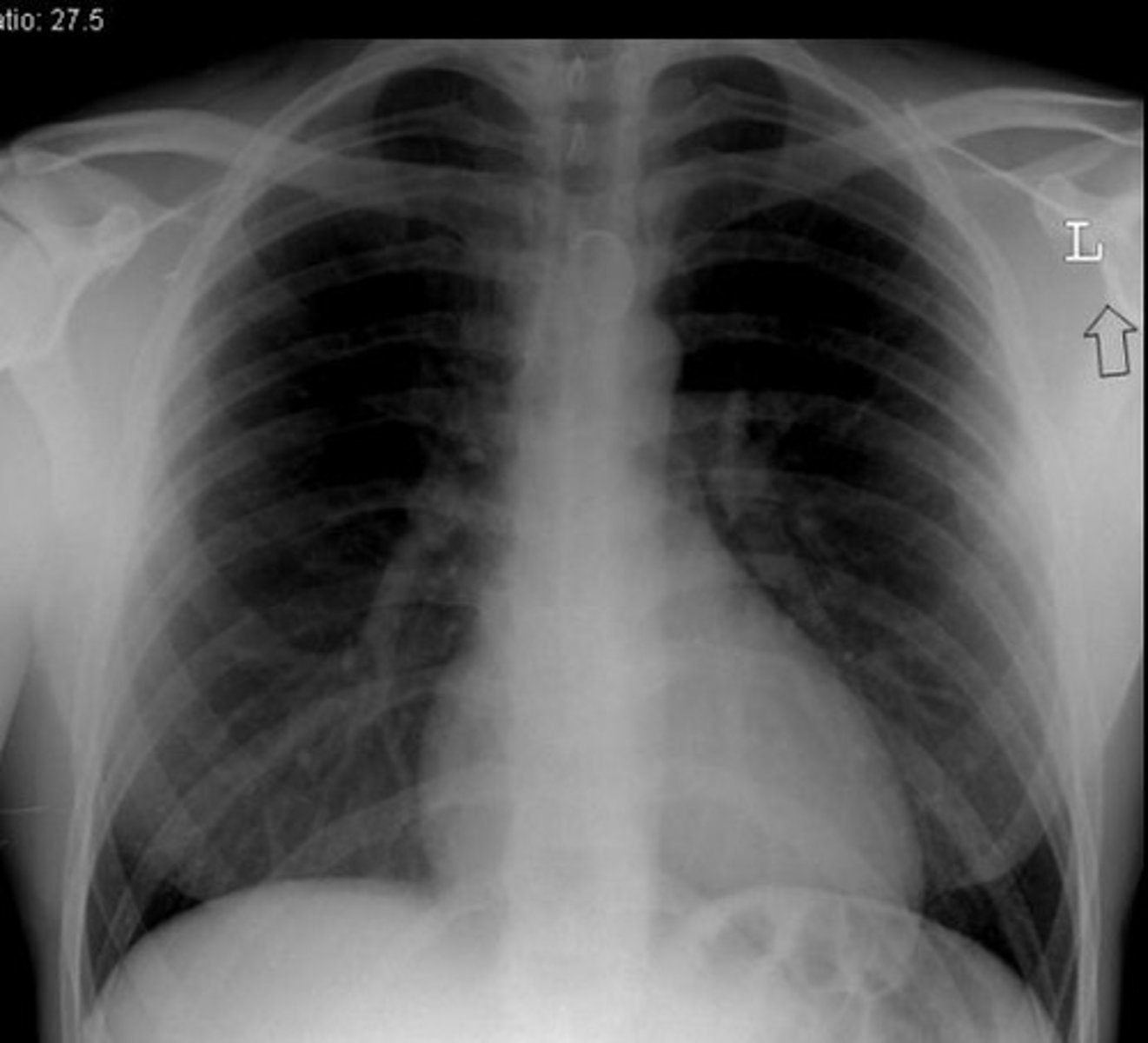
discuss her xray
normal x ray. more suggestive of viral aetiology.
what type of micro organism is influenza A
virus. spherical. enveloped rna
how is influenza A transmitted
via respiratory droplets. importance of isolation
Influenza A can be subtyped depending on the antigen associated with its outer viral proteins. What are the names of these outer viral proteins?
-hemagglutinin (H)
-Neuraminidase (N)
-16H and 9N.
how are subtypes of influenza produced
antigens on influenza viruses can vary via antigenic drift and shift
antigenic drift
influenza virus enters host cell. mutation in antigen genes occur during replication within host cell. influenza virus 1 different to virus 1. minor changes in H&N prts by random mutations in viral RNA. does NOT change subtype
antigenic shift
influenza viruses 1 and 2 enter host cell. genes and antigens from both viruses incorporated into new virions. influenza virus 3 different from the first two.
one cell infected with two different subtypes of influenza virus. reassortment of viral RNA from both subtypes leads to the creation of new subtypes of the virus. estimated to happen every 10-20 years.
A 19 year old student returned 3 days ago from a 2 week holiday in South Africa. Just prior to returning home she began to feel unwell and has felt progressively more unwell since then. She describes fevers, generalised 'aches & pains' and a non-productive cough. She has no past medical history and is not taking any medication. She is a non-smoker and travelled with her boyfriend who is well. On examination her temperature is 38.1, she is flushed and appears breathless at rest. Her Blood Pressure is 129/72, her Heart Rate is 110 bpm and her Respiratory Rate is 36/min. Her O2 saturation levels are 94% on room air. On auscultation of her chest you hear bilateral fine inspiratory crackles at both bases.
positive on PCR for Influenza A.
In light of her diagnosis what management steps would you recommend?
-isolation in side room
-oxygen >98%
-oseltamivir (neuraminidase inhibitor used in treatment of influenza)
Name the cell type in the respiratory system that is infected by the influenza virus AND describe the features of that cell type
main targets of influenza virus are columnar epithelial cells of respiratory tract. simple columnar epithelial cells are longer than they are wide. nuclei are found at base of the cell. connected by tight junctions. may be other cell junctions eg adherens and desmosomes. receive nutrients through basement membrane, separates cell from capillary basal layer. key in production
In order for the virion to attach to the cell surface, structures on the virion surface must interact with receptors on the cell surface. Name the molecules involved.
-every virus has a specific cell membrane receptor it attaches to.
-influenza viral spike that attaches to cell receptor is HA prt (hemagglutinin)
-cell receptor is sialic acid (small sugar attached to many different proteins on cell surface)
Infected cells have begun to produce IFN-α and IFN-β. Describe how this effects the neighbouring cells.
stimulate production of molecules that inhibit viral replication both within themselves and in neighbouring uninfected cells as well as stimulating NK cells to seek and kill virally infected cells
Name and describe the mechanisms that cause Seasonal influenza epidemics
every year small changes in the structure of the envelope protein of influenza virus occur that can reduce effectiveness of existing T and B memory cells in human population by genetic drift. occasionally, wholesale changes in the structure of viral envelope protein can occur bc of genetic recombination which introduces entirely new types of envelope prt, usually avian virus origin, human pop has no immunological memory. genetic shift- INLFLUENZA pandemic.
exception 1918 strain on influenza pandemic
analysis shows that that virus was not a recombinant virus but an avian virus that infected people through mutation.
Every successful infectious microorganism must undertake certain obligatory steps in its interaction with the host. Influenza virus carries a protein called neuraminidase in its envelope By what mechanism does inhibition of neuraminidase activity with oseltamivir (Tamiflu) prevents the spread of influenza
neuraminidase essential for shedding of influenza virus from cells.
Why are infections due to sneeze transmission more likely to be upper rather than lower respiratory?
most sneezes generate an aerosol mucus droplets containing micro-organisms
What is a cytokine storm (cytokine cascade or hypercytokinemia)
-pathogens attack immune system. cytokines signal T cells and macrophages to travel to site of infection
-cytokines activate these immune cells, stimulate them to produce more cytokines. +ve feedback loop. attracts more Tcells and macrophages to join.
-sometimes body is unable to control the loop. excessive feedback loop, excessive level of cytokines in the body.
-usually happens in healthy immune system. leads to release of various cellular mediators (cytokines, oxygen free radicals, coagulation factors)
-both pro-inflammatory cytokines (eg interleukin-1, tumour necrosis factor alpha etc) AND anti inflammatory cytokines (eg IL-10 and IL-1 RECEPTOR ANTAGONIST) involved
famous examples of cytokine storm
-1918 influenza pandemic
-2003 SARS
-affected disproportionate high numbers of healthy young adults.
Define lower respiratory tract infection
acute illness usually with cough as main symptoms and at least one other lower resp infection symptom eg fever, wheeze, chest discomfort
pneumonia
infection of lungs causing alveoli to fill with fluid and pus as a result of disrupting and overwhelming the protective systems
pneumococcal pneumonia
caused by streptococcus pneumoniae
secreted factors to protect airways
IgA, surfactant proteins, defensins
alveolar pneumonia
purulent exudate fill lumen
lobular pneumonia
S. pneuma, H.flu
bronchopneumonia
patchy distribution. result of aspiration, intubation. staph, enteric, pseudomonas
interstitial pneumonia
alveolar walls and connective tissue, lymphocytes, macrophages and plasma cells interfere with gas exchange at alveoli level
atypical pneumonia
diffuse infiltrate w/ perihilar concentration
Different bacteria/viral causes:
-Legionella pneumophila, Mycoplasma pneumoniae, and Chlamydophila pneumoniae
-Respiratory viruses, e.g. influenza
how is pneumonia spread
spread person-person by coughing out droplets. some pathogens can live in nose and throat without causing disease. when inhaled into the lungs can cause pneumonia.
at risk groups of pneumonia
babies and young children, people over 65, people with long term heart and kidney diseases, diabetes, smokers.
how can cough reflex be impaired
anaesthesia, neuromuscular disorder, coma
how can the mucociliary escalator become impaired
cigarrette smoke, corrosive gases.
phagocytic action of alveolar macrophages impairment
alcohol, tobacco
secretion clearance impairment
cystic fibrosis
typical community acquired parenchyma
severe, acute presentation. infectious agent identifiable and responsive to cell wall active antibiotics
Atypical community acquired pneumonia
sub acute presentation, causative pathogens are difficult to culture or identify by standard methods. not responsive to penecillins
four stages of classical lobular pneumonia
local capillaries become engored with neutrophils causing acute congestion. red blood cells flow into alveolar spaces causing red hepatisation. large numbers of dead neutrophils and degeneratic RBC form grey hepatisation. resolution when adaptive immune response produces antibiodies
hospital acquired nosocomial pneumonia
pneumonia more than 48 hours after admission excludes infection that is incubating at the time of admission. malaise, fever, chills. MRSA. g-ve bascilli and S.aureus.
ventillator associated pneumonia
nosocomial pneumonia in pt who has been mechanically ventilated by endotracheal tube or tracheostomy for at least 48 hours at time of diagnosis. g-ve bascilli and S.aureus.
example of acute community acquired pneumonia
S.pneumoniae, H.influenzae
community acquired pneumonia atypical
mycoplasma, chlamidya
example of nosocomial pneumonia
enterobacteriae, pseudomonas
aspirated pneumonia
anaerobic oral flora and aerobic bacteria
chronic pneumonia cause
nocardia actinomyces and granulomatous