AOS 2 - Psychology
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
75 Terms
The Human Brain
The body’s ‘control centre’, coordinating everything we think, feel and do.
Most complex organ in the human body
A single organ made up of different areas, each with specific functions.
Psychology definition:
Psychology is the study of human mental states and behaviours.
Brain Versus Heart Debate - Theory
There was a historical debate over whether the heart or the brain was responsible for mental processes such as thoughts, feelings & behaviours.
Ancient Egyptians believed that the heart was the source of all human psychology, wisdom, the mind and the soul. It was believed that personality, logic and emotion originated in the heart, this is why they were preserved.
Ancient Greek Philosophers believed that the brain alone was responsible for mental functions such as personality and logic.
The Mind-Body Problem - Theory
The Mind-Body Problem - a complex philosophical question as to whether our mind is separate and distinguishable from our body or one integrated entity.
The Mind-Body Problem (Theory) - Opposing debates
Dualism - believe that the human mind and body are separate from one another. They can be distinguished between their function and substance, the mind is not physical, the body is.
Monism - believe that the human body and mind are one complete entity. Although our minds are not tangible they complete physical processes. Physiological processes occur when mind processes are used.
Pseudoscience definition:
A pseudoscience is a theory or method that appears to be based on science, but is actually not.
Phrenology - Theory
Phrenology is the study of the shape and size of the human skull to determine personality and mental function.
Established in 1796 by Franz Gal
Phrenologists believed that the amount an area of brain was used would relate to the size of the area.
27 ‘mind organs’ which have their own distinct location and mental function.
Discredited as a science post the 1900’s
*Proved specific localised areas of the brain
List the First Brain Experiments:
Ablation
Brain lesioning
Split-brain research
By the end of the 19th century, such techniques enabled scientists to assign functions to specific brain regions.
Brain Experiments: Ablation
Pierre Flourens (1794–1867)
Brain ablation involves the surgical removal, disabling or destroying a selected region of brain tissue. Irreversible and permanent.
Used historically to treat neurological /psychological disorders.
SCIENTISTS STUDIED BEHAVIOUR OF PATENTS, MAKING INFERENCES ABOUT LOCALISED FUNCTIONING.
*Methods still used to remove brain tumors or on animals.
Brain Experiments: Brain Lesioning
The practice of inducing and/or studying the effects of damage to a particular area of the brain.
Damage could have been caused by:
A researcher studying the effects of brain damage
brain damage caused by illness (eg: stroke) or head trauma
HELPS RESEARCHERS UNDERSTAND LOCALISED BRAIN FUNCTIONING - OBSERVING HOW PATIENTS ARE AFFECTED AFTER DAMAGE IS INDUCED
Hemispheric Specialisation.
Hemispheric specialisation refers to the difference in functioning between the left and the right hemispheres of the brain. (Cerebral hemispheres)
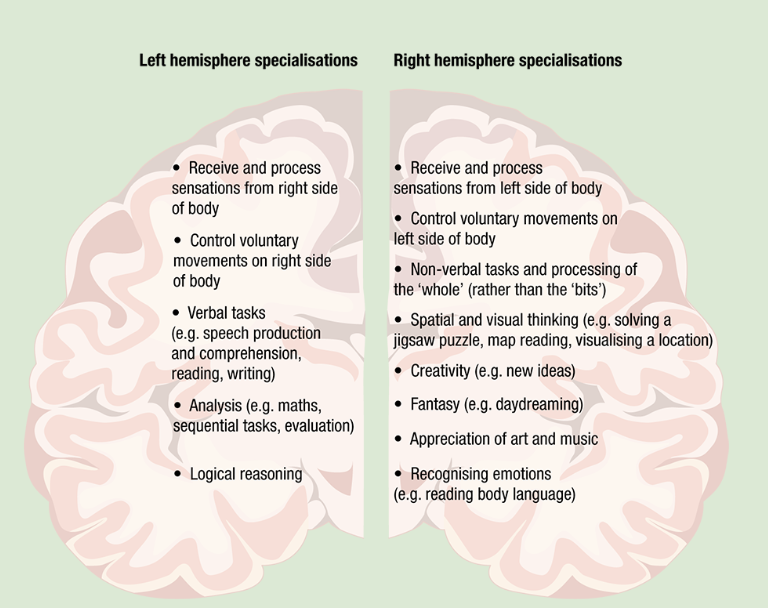
Define the Specialisation of each hemisphere:
Left hemisphere specialises in verbal and analytical functions.
Right hemisphere specialises in non-verbal functions.
Brain experiments: Split-Brain Experiments Background
Roger Sperry (1913 - 1994)
Observed individuals who had undergone split-brain surgery (epilepsy treatment): cutting the corpus callosum, tissue connecting the two hemispheres
Medical reports of split-brain patients indicated no loss or impairment to brain functions - SPERRY PROVED OTHERWISE.
Split Brain Experiments - Method
Participants were tested one at a time:
Seated behind a screen.
The screen is would flash a word or picture for a second while the participant focuses on a black dot in the middle of the screen.
The word or picture is flashed either to the left or right of the black dot.
In response to the images flashed in the right visual field (sent to the left hemisphere), patients named the objects.
Images flashed in the left visual field (sent to the right hemisphere), patients could not name the objects they saw. BUT they could draw or select object with their left hand only.
Right image = name objects (LEFT BRAIN)
Left image = draw or select object (RIGHT BRAIN)
Split Brain Experiments - Conclusions
Visual information sent to the right hemisphere cannot cross back to the left hemisphere , then the person is unable to say what they saw.
Confirmed theory of hemispheric specialisation.
Confirmed theory of contralateral control:
Left hemisphere controls right side of body
Right hemisphere controls left side of body.
Brain lateralisation:
The difference in functioning between the left and the right hemispheres of the brain when we perform a specific behaviour or task.
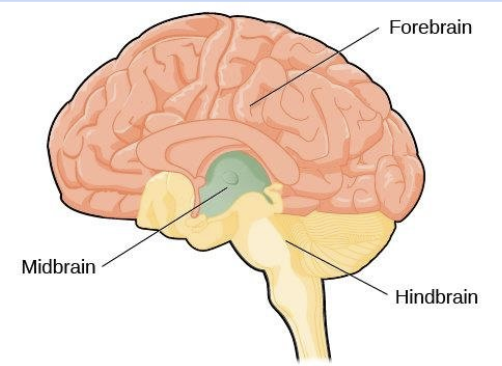
Three main regions of the brain:
Hindbrain
Midbrain
Forebrain.
Each area is associated with identifiable mental processes and behaviour.
The more basic survival mechanisms develop earlier (hindbrain and midbrain) than the more ‘higher order’ functions (forebrain).
Hindbrain:
Located at the base of the brain.
Collection of lower level brain structures, including the cerebellum, medulla and pons.
CONTROL VARIOUS INVOLUNTARY MOTOR FUNCTIONS AND VITAL AUTOMATIC RESPONSE
Breathing, heart rate, sleep and arousal (alertness)
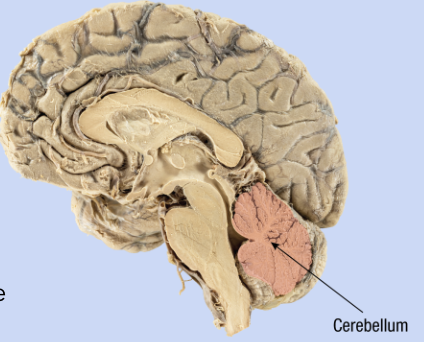
Hindbrain: Cerebellum
Cauliflower-shaped structure.
The second largest part of the brain, 10% of brain’s mass but 80% of the brain’s neurons.
Coordinates fine muscle movements (smooth and precise) (through communication to skeletal muscles)
Regulates posture and balance.
Involved in activities requiring a rapid and skilled sequence of movements (eg: riding a bike)
Damage to the cerebellum - difficult to coordinate muscle control for everyday activities, problems with balance, and difficulties with speech.
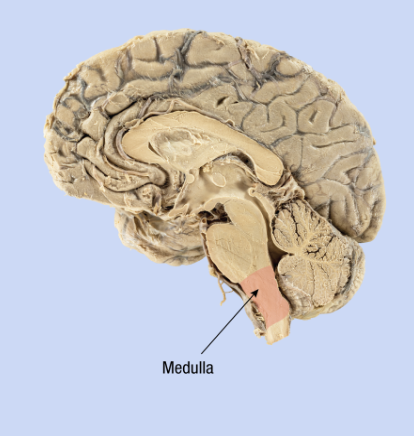
Hindbrain: Medulla
The lowest part of the brain
A mass of neurons that regulates autonomic functions
Controls vital bodily functions such as swallowing, breathing, heart rate, blood pressure, vomiting, salivating, coughing and reflex actions such as sneezing, coughing and vomiting all of which occur automatically and are essential for survival.
Connects the brain to the spinal cord creating a pathway for neural signals to be transmitted.
Injury to the medulla is often fatal.
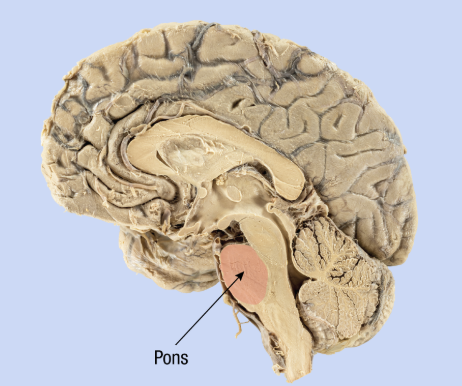
Hindbrain: Pons
Above the medulla, a small bundle of neural tissue about 2.5 cm long.
Relays information to different brain areas acting as a bridge
Involved in sleep, dreaming and arousal from sleep (‘waking’)
Helps control breathing and coordination of some muscle movements.
Involved in various involuntary behaviours such as blinking
Midbrain:
The central part of the brain.
Contains neural pathways connecting upper and lower brain areas.
A collection of structures involved with movement, processing of visual, auditory and tactile sensory information, sleep and arousal.
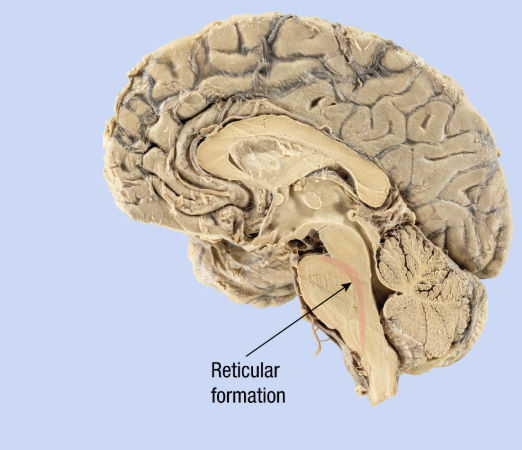
Midbrain: Reticular Formation
Helps screen incoming information so as not to overload the brain.
Alerts higher brain centres to important information
Helps maintain consciousness, and regulates arousal (such as awakening from sleep) and muscle tone (tension).
Forebrain:
Largest and most prominent part of the brain.
Neural pathways connect midbrain and hindbrain (to coordinate brain activity).
The forebrain is a collection of upper level structures that include the hypothalamus, thalamus and cerebrum.
Regulates complex cognitive processes such as thinking, learning, memory and perception, as well as various aspects of emotion and personality.
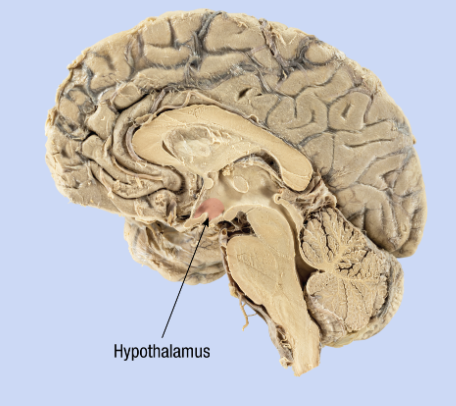
Forebrain: Hypothalamus
The size of a sultana grape.
Part of the limbic system
Helps maintain homeostasis.
Regulates the release of hormones from various glands in the body.
Influences behaviours associated with basic biological needs, such as hunger, thirst and sleep.
Involved in emotions such as anger and fear.
The Limbic System:
Contains:
Amygdala
Hippocampus
Hypothalamus
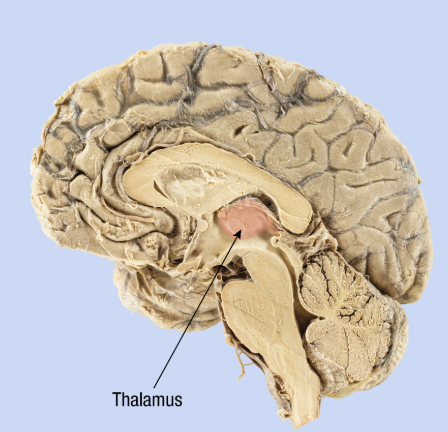
Forebrain - Thalamus
3 cm in length and comprises two parts egg shaped parts
Each one lies within a different hemisphere.
Processes almost all sensory and motor information (except smell) going to and from the cerebral cortex.
Forebrain: Cerebrum (location, structure, responsible for)
Top half of the brain, occupies most of the forebrain.
Consists of the cerebral cortex (outer surface)
Divided into two cerebral hemispheres - deep groove runs from the front to the back (longitudinal fissure).
Responsible for almost everything we consciously think, feel and do!
Hemispheres connected, by corpus callosum which enables information exchange and coordinated brain functioning.
Forebrain: Cerebral Cortex
The outer layer of the cerebrum that covers the brain.
It is approximately 2.5mm thick
Its folds, bulges and groves maximize the surface area which enables the cortex to contain around 16 billion neurons.
The cerebral cortex plays an important role in mental processes and behaviors.
Initiating voluntary movements
Processing sensory information
Mental processes such as language, sensation, perception, problem-solving, judgement and the regulation of emotions
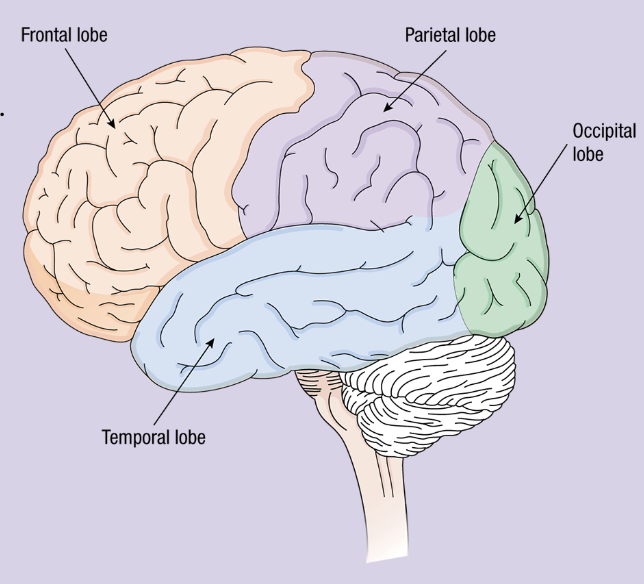
Cortical lobes of the cerebral cortex:
Cortical lobes are areas of the cerebral cortex associated with different functions.
Each cerebral hemisphere has four lobes:
frontal lobe,
parietal lobe,
occipital lobe
temporal lobe.
Frontal Lobe: (2 cortexes)
The largest of the four lobes.
It receives and combines information from throughout much of the brain to perform many complex functions.
The frontal lobe is responsible for planning and initiating voluntary bodily movements.
The prefrontal cortex plans the required motor sequence then sends the instructions to the premotor cortex.
The premotor cortex prepares the appropriate movement sequence and sends the information to the adjacent primary motor cortex.
*CONTAINS THE PREFRONTAL CORTEX
Frontal lobe - Prefrontal cortex
Sits just behind the forehead
Occupies over one-quarter of the cerebral cortex.
Involved with sophisticated mental abilities such as reasoning, planning, problem solving, decision making and symbolic thinking
attention (picking out relevant information through the senses)
regulation of emotions and expression of emotional reaction
self-awareness
aspects of personality
Has an ‘executive’ role in all our thinking, feeling and behaving.
Coordinates many of the functions of the other lobes and determines our responses.
Frontal lobe - Primary motor cortex
The primary motor cortex initiates and controls voluntary movements through its control of skeletal muscles.
Found in both lobes, controlling the opposite side of the body
The amount of cortex devoted to a particular body part corresponds to the complexity, or ‘fineness’, of its movements. Parts that we are able to move with the greatest precision (such as the fingers and tongue) take up more cortical space.
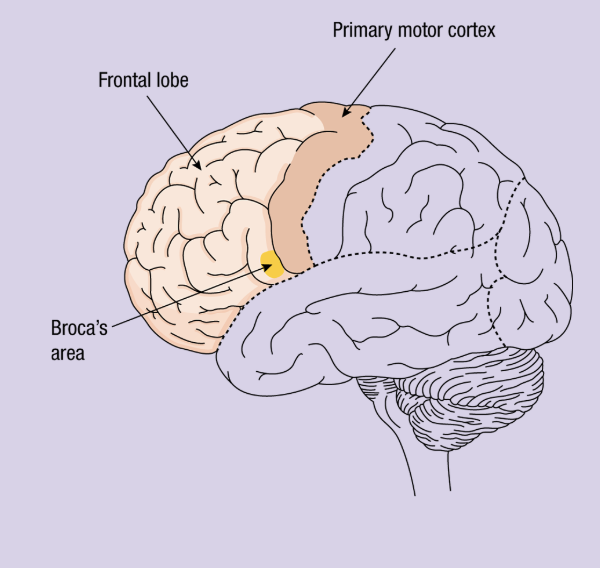
Frontal lobe - Broca’s area
Located in the frontal lobe of the left hemisphere. (next to the primary motor cortex)
It coordinates movements of speech muscles muscles+supplies this information to motor cortex.
Broca’s area has a crucial role in the production of articulate speech; that is, speech that is clear and fluent.
Damage to this area due to stroke or injury leads to Broca’s Aphasia.
Parietal lobe:
Is located behind the frontal lobe and occupies the upper back half of the brain.
Receives and processes bodily, or ‘somatosensory’, information.
Includes touch and temperature (from the skin) and information about muscle movement and the body’s position (from muscles, tendons and joints).
PARIETAL LOBE IS JUST THE SENSES + POSITION
Primary Somatosensory Cortex:
Located at the front of each parietal lobe (CONTRALATERAL CONTROL)
Receives and processes sensory information from the skin and body parts.
The amount of cortex devoted to a body part corresponds to the its sensitivity and use.
Occipital lobe:
Is located at the rearmost area of each cerebral hemisphere, at the back of your head.
Is almost exclusively devoted to the sense of vision.
Damage to the occipital lobe can cause serious visual impairments.
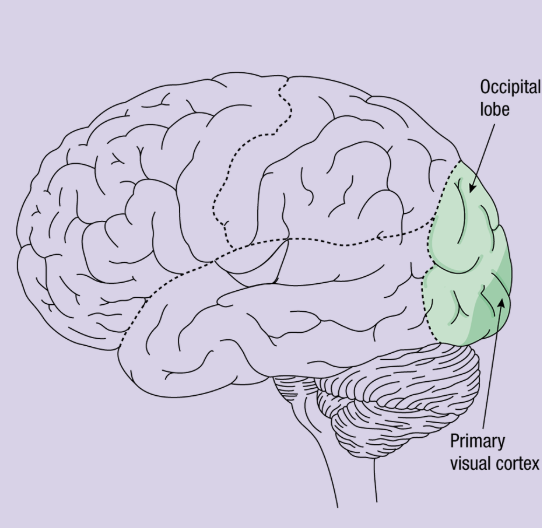
Primary visual cortex:
Located at the back of each occipital lobe and this is the major destination of visual information from the two eyes.
Information comes to the primary visual cortex from visual sensory receptors located on the retina at the back of each eye.
Temporal Lobe:
Is involved with auditory perception.
Plays an important role in memory.
Plays a part in aspects of visual perception such as our ability to identify objects and recognise faces.
Emotional responses to sensory information and memories.
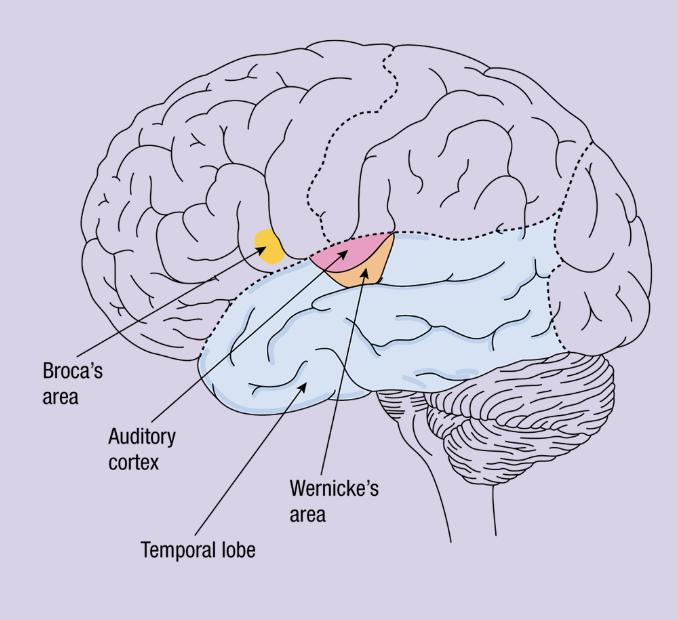
Primary Auditory Cortex:
In each temporal lobe receives and processes sounds from both ears so that we can perceive and identify different sounds.
Different areas of the auditory cortex are specialised to register and respond to different types of sound.
Wernicke’s area:
Located in the temporal lobe of the left hemisphere, connected to Broca’s area.
Involved in speech production and comprehension - interpreting the sounds of human speech.
Individuals cannot understand auditory sensations until the information has been processed by Wernicke’s area.
Damage to this area due to stroke or injury leads to Wernicke’s Aphasia.
The Neuron:
Neurons are nerve cells that receive, process and transmit neural messages. Found in the brain and nervous system.
Different parts of the neuron work together to enable the transmission and reception of neural information:
List and define the parts of a neuron: (7)
Dendrites: receive neural messages from the previous neuron (aka presynaptic neuron)
Myelin sheath/myelin: insulates the neuron and prevents disturbance from other neurons
Axon terminals/terminal buttons: sends neural messages to the next neuron (aka postsynaptic neuron)
Synapse: the region that includes the axon terminals of the presynaptic neuron, the synaptic gap, and the dendrites of the postsynaptic neuron
Synaptic gap: Microscopic space between neurons
Presynaptic neuron: the neuron that comes before the synaptic gap; sends the message to the next neuron
Postsynaptic neuron: the neuron that comes after the synaptic gap; receives the message from the previous neuron
Neuroplasticity: (relate to neurons)
Neuroplasticity: ability of the brain to change in response to experience and activity
Brain changes occur as a result of neurons communicating and creating connections with each other, and forming pathways and networks
Pathways strengthened through repeated use, or eliminated through lack of use
List the two types of Plasticity:
Two types of plasticity:
Developmental plasticity
Adaptive plasticity
Developmental plasticity:
Changes in the brain that occur in response to ageing and maturation.
Three factors influencing developmental plasticity include:
Synaptogenesis
Synaptic pruning
Myelination
Infancy and adolescence are two periods of significant neuronal change due to developmental plasticity.
Infancy the number of neuronal connections (synapses) greatly increases through synaptogenesis.
From late childhood and into adolescence, our neuronal connections are refined and reduce greatly in number through synaptic pruning.
Factors of Developmental Plasticity: Synaptogenesis:
Synaptogenesis: the formation of synapses between neurons as axon terminals and dendrites grow
When an individual learns something new, the axon terminals of neurons grow and form connections to nearby neurons.
This creates synapses to represent and retain this learning.
Most intense during infancy but continues to take place throughout the lifespan.
Factors of Developmental Plasticity: Synaptic pruning:
Synaptic pruning: elimination of underused synapses
Underused synapses are cut off or ‘pruned’ to free up space in the brain and allow for the strengthening of frequently used synapses.
Childhood toddlers and adolescence undergo intense periods of synaptic pruning, but it occurs throughout the lifespan
Factors of Developmental Plasticity: Myelination:
Myelination: the formation and development of myelin around the axon of a neuron
Myelin on axons facilitates more efficient communication of neural impulses
This is done by protecting the neuron from interference from other neurons so that as we develop and learn new skills, communication in the brain can happen quickly and smoothly.
Brain trauma: (definition and examples)
Brain trauma: damage to the brain that is caused by an external force.
Examples include:
falling and hitting your head
a head assault (e.g. experiencing a severe knock to the head)
vehicle accidents
sporting injuries to the head
Adaptive Plasticity
Adaptive plasticity: brain’s ability to restore adequate neural functioning over time after sustaining injury (affected by sprouting and rerouting)
Factors of Adaptive Plasticity: Sprouting:
Sprouting: ability of a neuron to develop new branches on the dendrites or axons
This expands the reach of a neuron, particularly when the neuron has been damaged from the trauma, enabling new neural connections to be formed in areas of the brain where the neural activity has been prevented or depleted.
Factors of Adaptive Plasticity: Rerouting:
Rerouting: a neuron’s ability to abandon connection with damaged neuron and form a new connection with another undamaged neuron
This enables new neuronal connections to be formed after trauma; therefore, cognitive functioning is re-developed.
Ways to maintain brain functioningL
Mental stimulation
Diet
Physical activity
Social support
Acquired Brain Injury: (definition, types and characteristics)
Acquired brain injury: all types of brain injuries that occur after birth
Traumatic brain injury: Damage to the brain caused by an external force
Non-traumatic brain injury: Damage to the brain caused by internal factors, such as a lack of oxygen or a tumour (e.g. stroke, aneurysm, tumor, substance abuse)
Impairments can be permanent or temporary and can cause disability.
Brain injuries vary in the rate at which they develop, their intensity, or even the consequences that they induce.
Acquired Brain Injury - Damage
Effect on individual functioning due to an acquired brain injury is directly related to the area of the brain that is damaged.
An acquired brain injury can affect your:
Biological functioning
Psychological functioning
Social functioning
Effects on Functioning - Acquired Brain Injury (3 types)
Biological functioning - observed through changes in behaviour, organ function, and cellular and neuronal function.
Eg: Seziures, movement impairment, olfactory impairment (smell)
Psychological functioning - observed though cognition, behaviour and emotion.
Eg: Memory loss, personality changes, increased likelihood of mental disorders
Social functioning - observed through relationships, interactions with the environment and interpersonal skills.
Eg: Job productivity loss, social support, anti-social behaviour
Neurological disorders
Neurological disorders: diseases characterised by any damage to or malfunctioning of the nervous system.
Any change to neural functioning that impairs the nervous system to function effectively.
Two neurological disorders we will focus on are:
Parkinson’s disease
Epilepsy
Parkinsons Disease:
Parkinson’s disease: a progressive, neurodegenerative disease of the nervous system characterised by both motor and non-motor symptoms.
Progressive → it continues to get worse, is not reversible/no cure
Neurodegenerative → characterised by the death of neurons in the brain
The part of the brain that is affected is primarily responsible for dopamine production.
Dopamine
Dopamine: neurotransmitter responsible for the coordination of voluntary movement and the experience of pleasure and pain.
Symptoms of Parkinson’s:
Progressive (continues to get worse)
Neurodegenerative (death of neurons in the brain)
Tremors
Reduced motor control
Muscle stiffness
Problems with cognition
Fatigue
Depression and anxiety
Epilepsy
Epilepsy: neurological disorder associated with abnormal electrical activity in the brain, categorised by recurrent seizures.
Seizures → brief episodes of uncontrolled and unrestricted electrical discharging of neurons in the brain.
Epileptogenesis → structural and functional changes occur in the brain creating an environment ‘supportive’ for seizures to occur.
Symptoms of Epilepsy:
Seizures (uncontrolled electrical discharge of brain neurons)
Epileptogenesis (create environment supporting seizures)
Involuntary shaking
Loss of consciousness
Loss of awareness
An aura (sensory disturbance)
Contemporary Research:
*Historically epilepsy was considered to be spirit possession of a person
*Historically parkinson’s disease was classified by symptoms, but its development not understood
Contemporary research challenged these theories, discovers new treatment:
Gut-brain axis
Machine learning
Machine Learning:
Machine learning: Artificial intelligence, creating more accurate software, predicts outcomes.
(mimickings human learning)
Uses statistics to create algorithms - accurately classify information and make predictions
Machine learning processes are often broken into two categories:
Supervised learning
Unsupervised learning
Machine Learning - Supervised Learning
Supervised learning: process involves the use of labelled data to train algorithms on how to classify data or predict outcomes.
E.G. by presenting an algorithm with hundreds of images of typical brains and Parkinson’s affected brains, labelled as such, it will eventually be able to detect the difference between the two without any human input or labelling.
Used to diagnose neurological disorders in a more efficient and accurate way
Includes the detection of stages of a disorder.
Machine Learning - Unsupervised Learning
Unsupervised learning: process involves using an algorithm to identify patterns or trends within unlabelled data that have not yet been discovered.
E.G. unsupervised machine learning may be used to analyse the demographic data of epilepsy patients to uncover trends as to which groups of people are most susceptible to the disorder.
Used to analyse the demographics of individuals with neurological disorders- identify biological markers that may have been previously overlooked.
Gut-brain Axis
Gut-brain axis (GBA): bidirectional connection between the gut and the brain through multiple parts of the nervous system
The gut and the brain are able to communicate and influence one another.
Having a ‘brain condition’, stress or a mental health issue, can lead to changes in the gut, eg: imbalance of good and bad bacteria
Having a gut related condition (e.g poor gut health, digestive problems etc) can lead to ‘brain effects’ such as low mood, being more susceptible to stress, and a more intense stress response.
Gut-Brain Axis - How?
The gut can influence the brain because of our gut microbiota.
Gut microbiota: all of the microorganisms that live in the gut.
An imbalanced gut microbiota has the potential to lead to central nervous system disease progression, such as the progression of neurological disorders
Chronic traumatic encephalopathy
Chronic traumatic encephalopathy (CTE): a progressive and fatal brain disease associated with repeated head injuries and concussions
The development of CTE is typically associated with repeated concussions - usually arising from contact sports, combat, head banging, and intimate partner violence, OR a single severe brain injury eg: car accident.
Effects of Chronic traumatic encephalopathy
CTE is considered to be an example of a neurodegenerative disease (characterised by the progressive loss of neurons in the brain)
Effects do not occur immediately after head injury/concussion.
Causes damage to neurons over time and the progressive worsening of brain functioning.
CTE can become fatal as the brain reaches a point of degeneration in which it is difficult to function and sustain life.
Chronic traumatic encephalopathy - Symptoms:
Generally appear 8 to 10 years after the experience of repetitive concussions.
Symptoms include:
Impairments in executive functions, such as reasoning and decision-making
Memory loss
Depression
Difficulties with attention and concentration
Disturbances in behaviour
Anxiety and paranoia
Mood impairments, such as increased aggression and emotional outbursts
Chronic traumatic encephalopathy - DIAGNOSIS
Brain scans do not have the capacity to detect CTE (brain changes)
A conclusive diagnosis of CTE can only be made through a post-mortem examination.
Post-mortem examination: assessment of a dead body that occurs to determine the cause of death
Chronic traumatic encephalopathy - Protein + Prevention
CTE is associated with the widespread build up of a particular protein (p-tau) substance in certain brain regions - detected in a post-mortem examination.
The accumulation of the protein tau forms neurofibrillary tangles.
Currently no cure.
Education and behavioural therapies have been effective in preventing/ treating post-concussion symptoms.
Sporting regulations (e.g. using helmets and implementing concussion protocols) can protect athletes.
Neurofibrillary tangles - CTE
Neurofibrillary tangles: tangles within neurons, inhibiting the transportation of essential substances - eventually kill the neuron entirely.