Eye Movements: Clinical Disorders
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
What are the two ways in which eye movements can provide insights into clinical disorders?
Characteristics of the eye movements themselves (fixation lengths, movement from stimuli, etc)
The locations people look
Can be applied by inclusion in diagnostic criteria or treatment protocols
Different disorders have different characteristics
Think: People with ASD less likely to fixate on faces (diagnostic) VS attentional control training to correct attentional biases in GAD (treatment)?
What are the benefits of using eye movement tracking in clinical research?
Affords benefits such as:
Easy to use
Affordable
Accessible
Quick
Non-invasive
Saccades
Overt, ballistic eye movements aimed at bringing a target into foveal vision
Can be internally or externally guided
Remember the fovea is a tiny spot int he centre of visual fields
Saccadic eye movements work by capturing a broad range of visual information to be able to understand the whole environment and stimuli, rather than just fixating on that tiny proportion of the visual field
Think: Like when you can send a message or photo on text with that effect where you rub out the blurry overlay to see the whole thing underneath. In this case, your finger is working as a saccadic eye movement
External Saccades
Saccades that are guided by an instruction, task or salient cue
E.g. Participants are instructed to look at a visual stimulus as soon as it appears OR a red flashing light captures attention
Think: I have been summoned
Internal Saccades
Saccades that are executed in the absence of a visual stimulus/target or instruction
Top down processes direct the saccades
YOU are directing your eye movements to a spot
Think: I am searching for visual information because I want it
Pursuit
Eye movements that tracking stimuli that move relatively slowly and smoothly
Smooth, non-ballistic movements
Match the velocity of gaze to the velocity of the target
Purpose is to keep a target in foveal vision
System can be divided into initiation and maintenance phases
Think: Watching a plane fly across the sky
What does the ‘integrity of pursuit’ refer to?
The ease at which a pursuit eye movement matched the velocity of a moving target
Essentially the mean velocity of eye movement divided by the mean target velocity
Low gain scores indicate difficulty matching gaze velocity to target velocity (because it would suggest the target was much faster than the eye)
Think: If they can stay on track with the moving target, that is, keeping it in foveal vision, then the pursuit has a high integrity
Gain
A ratio of the velocity of a person’s pursuit eye movements to the velocity of the target itself
Measures integrity of pursuit
Mean eye velocity / mean target velocity
1 would be a perfect score, meaning the eye movements matched their velocity to keep the target in foveal vision (high integrity)
Close to zero would mean their eye movements were much slower than the target, and they struggled to keep up (low integrity)
If gain is low, people may engage in more compensatory saccades or intrusive saccades
Compensatory Saccades
Saccadic eye movements used to catch up to moving targets when integrity of pursuit/gain is low
Intrusive Saccades
Anticipatory saccades or pares of saccades that move away from the target and then back
Think: Doing something illegal and glancing back at the door in anticipation that someone will walk in
Two divisions of the pursuit system
Initiation - picking up on the stimulus to be pursued
Maintenance - matching and maintaining the velocity of the moving object with eyes
Therefore, any issues with pursuits could be attributed to a failure or deficiency in one of these.
Either you don’t catch the object to pursue, or you catch it but can’t keep up with it
State 4 metrics of fixations
Location
Duration
Sequences of fixations
Distance between fixations
Pupillary Dilation
The diameter of the pupil varies as a function of:
Light
Task-specific recruitment of cognitive resources
General factors (arousal, stress, anxiety, etc)
The onset of stimuli responses
They are sensitive to working memory load on tasks
With each increase in working memory load, the pupil dilates linearly
How do we know that pupillary dilation is not a passive process?
They dilate to expected stimuli being absent
Think: There is something top-down and preparatory going on
How does cognition relate to pupillary dilation?
Increasing working memory load causes linear pupil dilation
Think: They trained people with locked-in syndrome to give dichotomous answers by doing mental arithmetic to dilate their pupils, as it increased working memory load.
Describe differences in eye movement behaviour for people with
Schizophrenia
Reduced smooth pursuit gain
AKA low integrity of pursuit
They struggle to keep up with tracking moving objects and matching the velocity of their eye movements to the object
The frequency of saccades during smooth pursuit is increased
Makes their ‘smooth’ pursuit less smooth (jerky eye movements rather than smooth)
Increased anti-saccade error rates and latencies
I.e. looking at certain stimuli when you’re not supposed to, and taking longer to get to the target stimulus
Increase in the frequency of catch-up saccades
Their pursuits lag behind so they often have to reposition their gaze back on the target
Changes in saccadic dynamics, rates of intrusive saccades such as anticipatory saccades, increasing the mismatch between eye position and target position
Basically speaking more to the idea that they struggle to keep their gaze on the moving target because other eye movements redirect them
Differences in fixation patterns of static scene viewing
Think: They have a hard time following the task at hand - WHAT’S COMING oh fuck I went too far WAIT WHERE DID IT GO
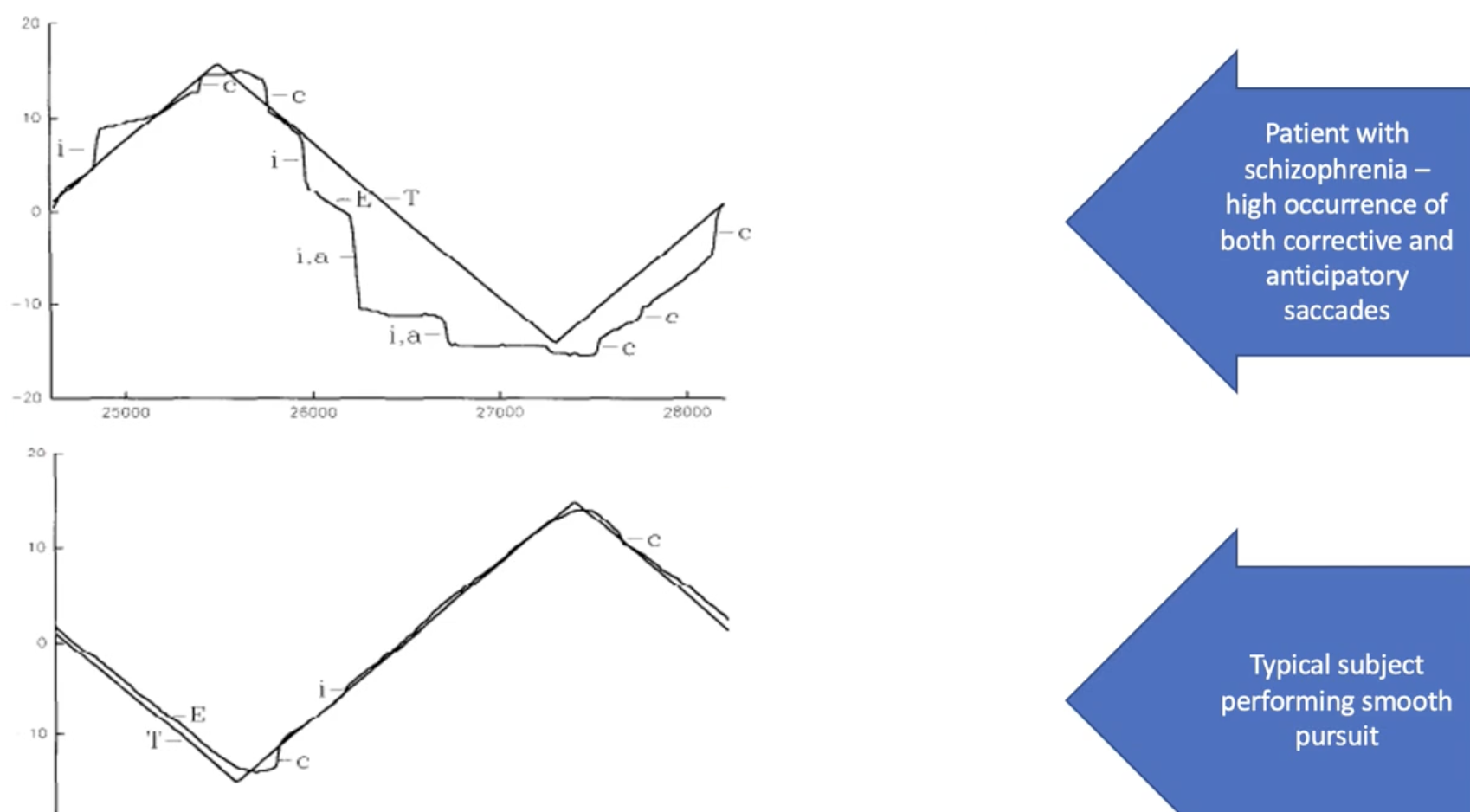
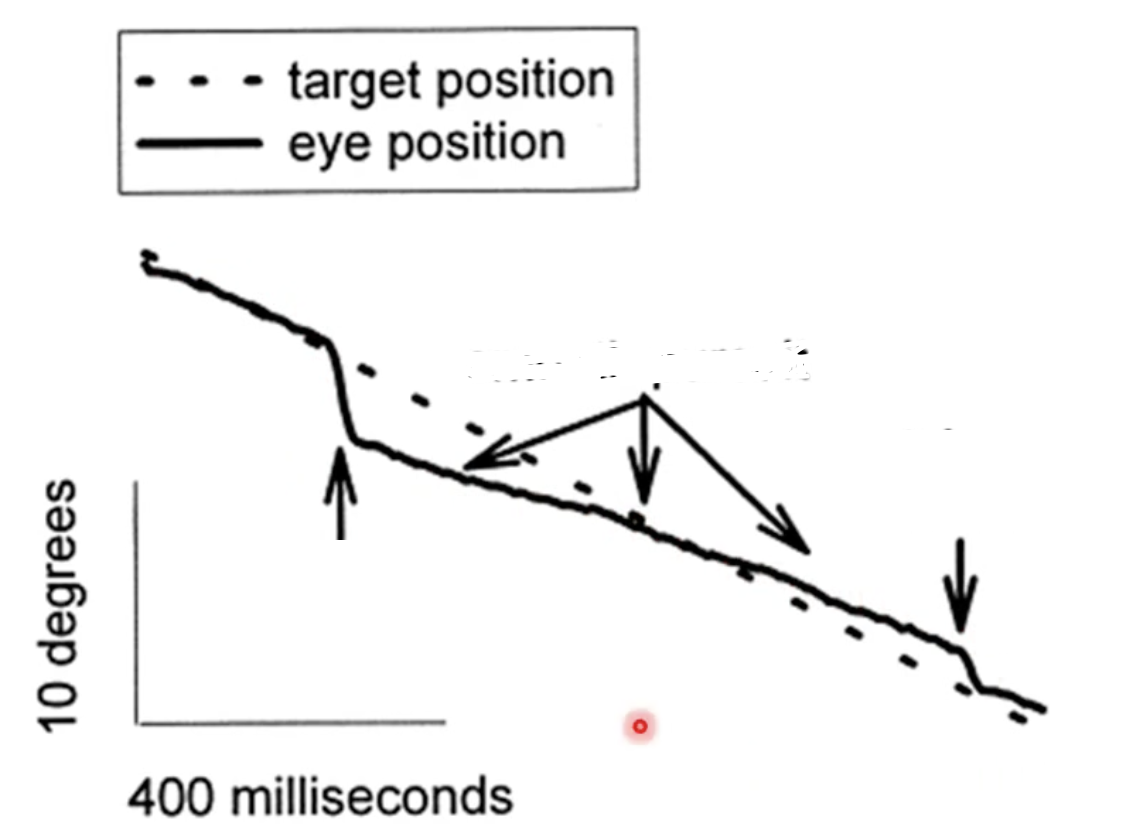
What is happening here?
This is a demonstration of a smooth pursuit of parents of a person with schizophrenia
When the eye position matches the target position, smooth pursuit is occurring
When the eye position dips below the target at the beginning, this is an anticipatory saccade (looking beyond the target)
When the eye position goes above the target and then quickly returns, this is a catch up saccade (the lagged behind and need to quickly get back)
The presence of these intrusive saccades may indicate genetic predisposition even though they don’t have schizophrenia (parents can exhibit biomarkers of schizophrenia)
Observed as an increase in the total number of eye movements because of these anticipatory and catch-up saccades
This is observed in half of children with schizophrenic parents too
Think: Anticipatory quickly moves AWAY from the target (sharp change away) whereas catch ups quickly move back (sharp change towards)
Takeaway: Eye movements can be used to identify biomarkers which can inform diagnosis and sometimes even heritability factors for clinical disorders such as schizophrenia
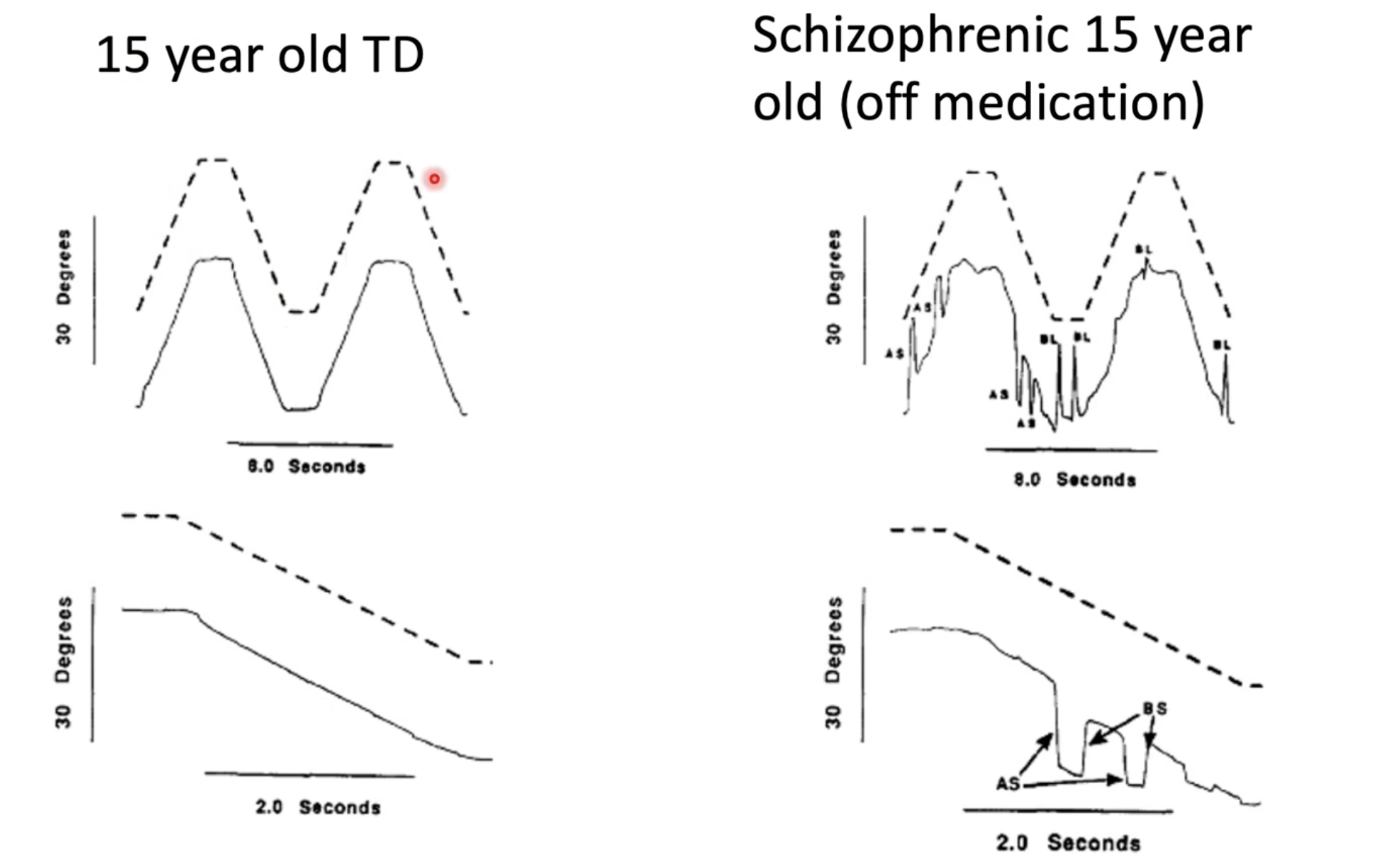
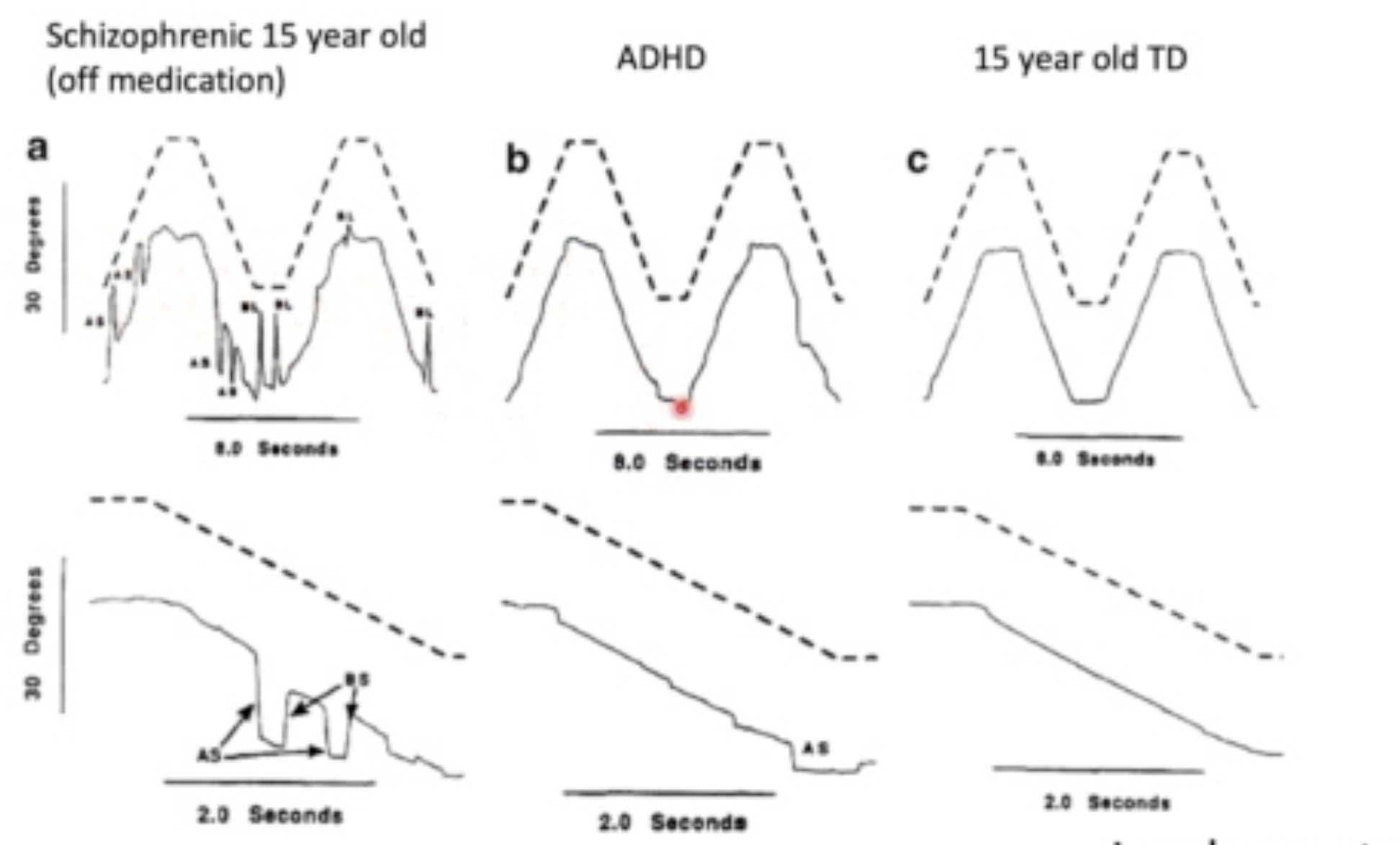
Describe the difference between eye movement and smooth pursuits of typically developed (TD) 15 year olds VS schizophrenic 15 year olds as found by Jacobsen et al. (1996)
There are significant differences
On the left, you can see that the TD child is far more accurate in smoothly following the target. Apart from maybe a tiny catch-up saccade when the target first changed direction, it is largely smooth
On the right, the eye movements of the schizophrenic child is sporadic and they spend less time fixated on the target. There are significantly more intrusive saccades (anticipatory and catchup). They really can’t smoothly track the target.
Findings from this study contributed to existing support that there is significant continuity between adult and childhood onset forms of schizophrenia
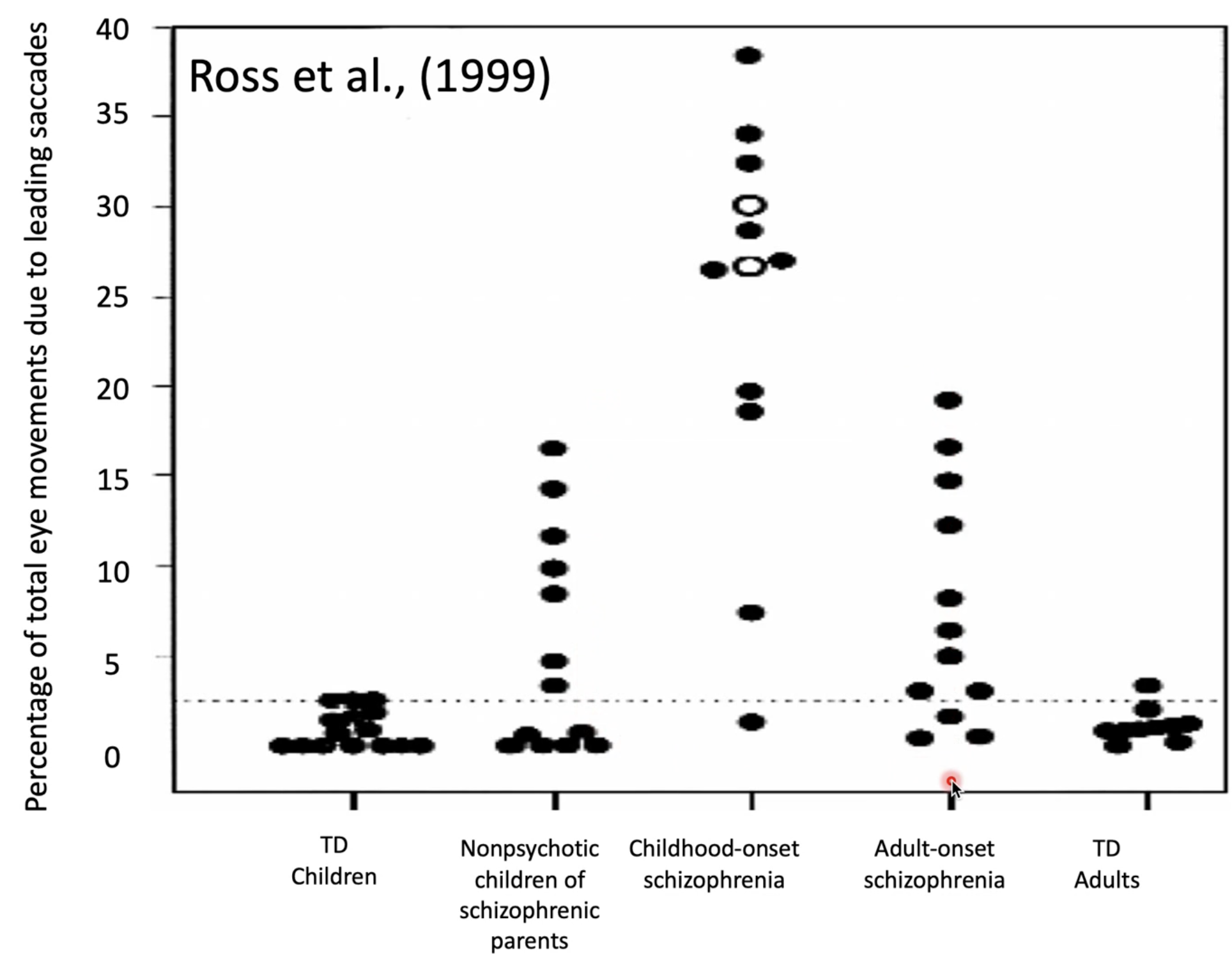
Interpret this graph by Ross
Lower number of saccades = better
typically developing (TD) children exhibit the lowest number of saccadic eye movements, which closely resembles TD adults
Demonstrates continuity (i.e. if eye movements are typical in childhood, it is likely they will be TD adults)
Childhood onset schizophrenics display the highest number of saccadic eye movements
The most important part of this graph is the resemblance between non-psychotic children of schizophrenic parents (Think: they have genetic predisposition and remember the diathesis stress hypothesis!) and adult-onset schizophrenics
Again, continuity → predisposed children’s eye movements may be biomarkers for schizophrenia that will onset later in life!
Means we need to keep an eye on children who are predisposed and are exhibiting these eye movement patterns, and perhaps put some extra supports and measures in place because they are showing the risk signs of developing later-onset schizophrenia!
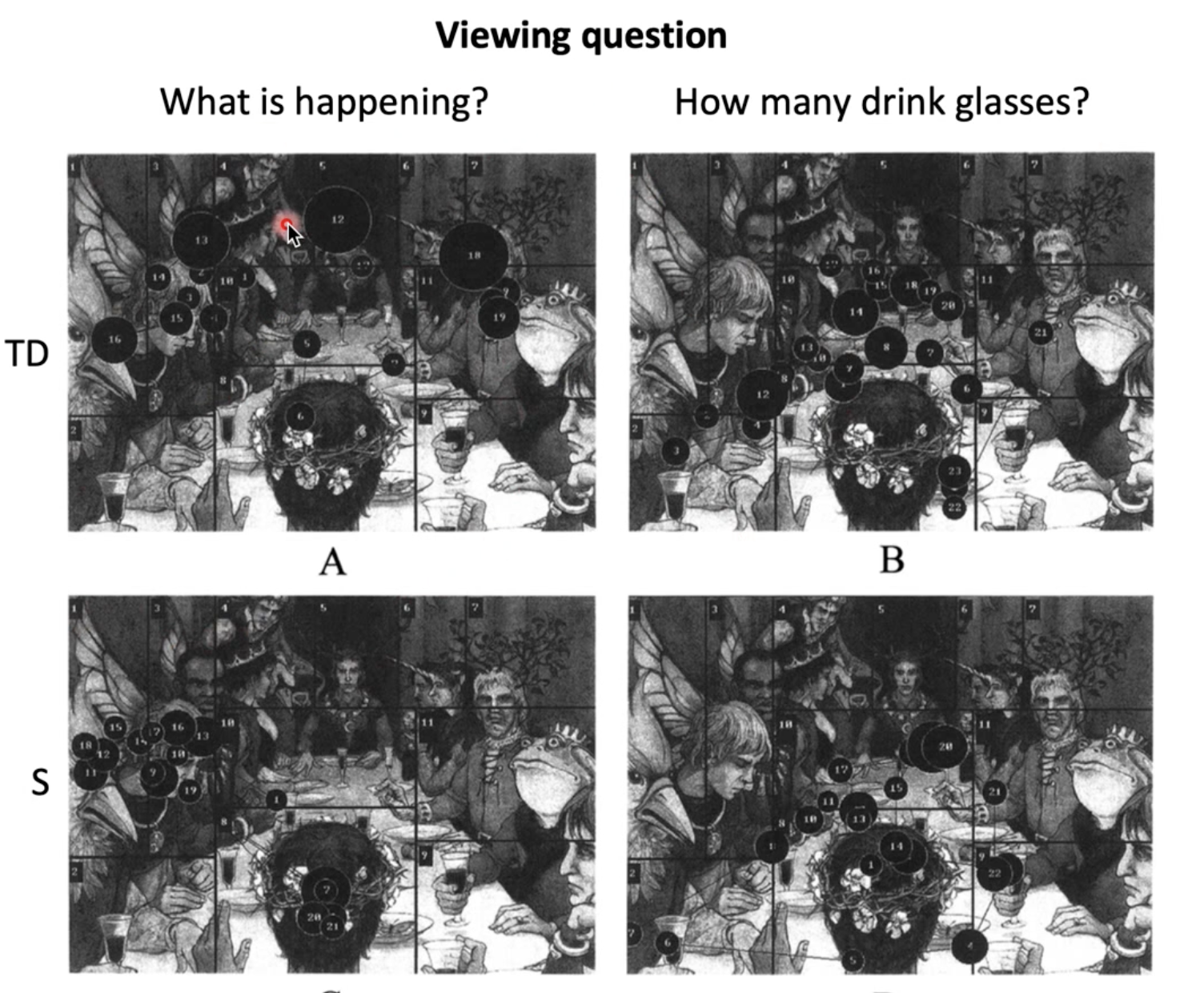
Describe this study by Karatekin and Asarnow (1999)
They compared eye movements between schizophrenic children and typically developing children when asked to view a scene
They were given:
global questions (i.e. what is happening in the picture?)
This required them to integrate all information given in the scene
Focal questions (I.e. how old do you think each person is?)
This required information from 2-3 places
Counting question (i.e. count the number of cups on the table)
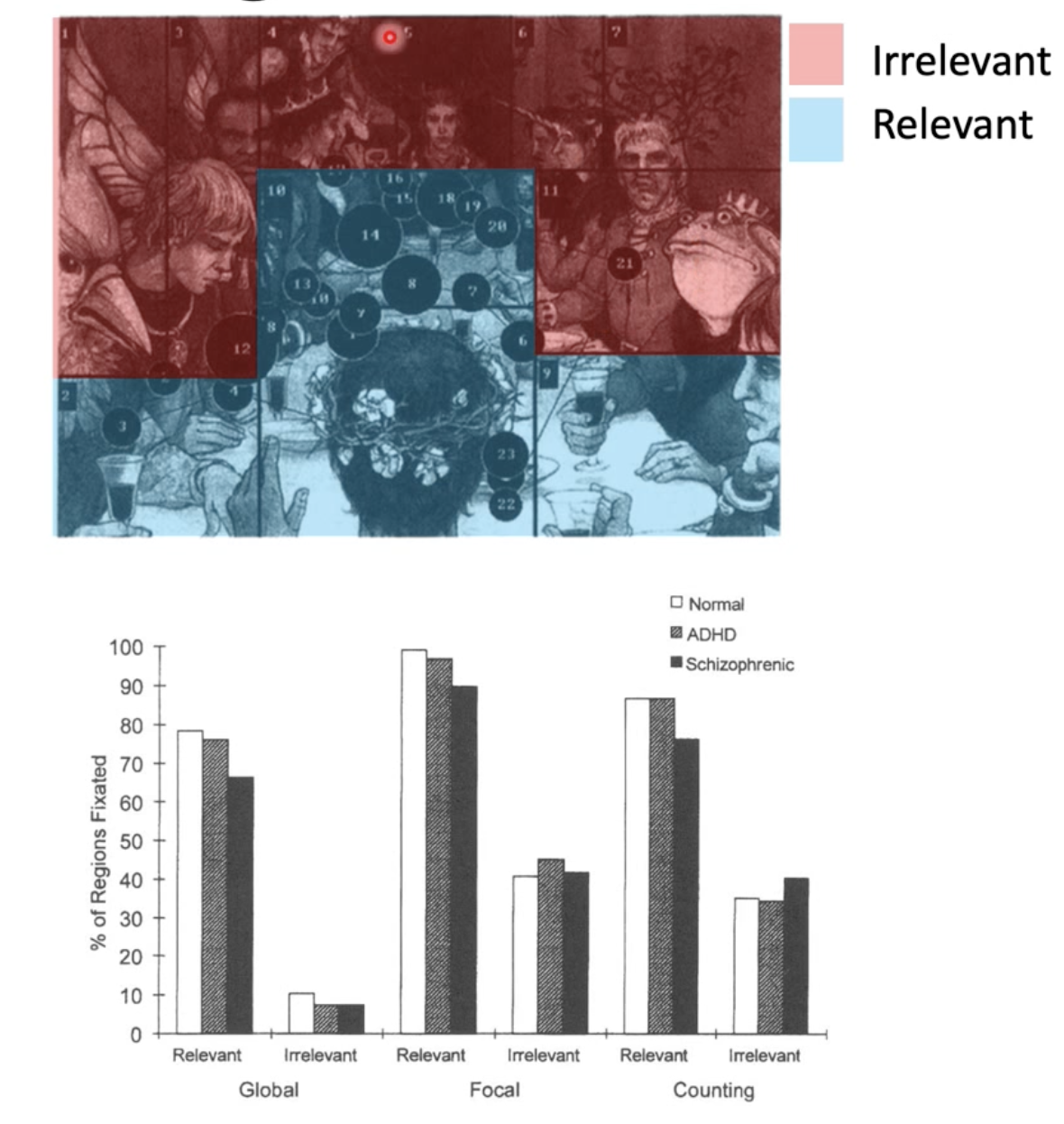
The identified spatial areas of the pictures that were either relevant or irrelevant based on the task (ie. looking at the heads would be irrelevant when asked to count cups)
They then examined the % of regions (relevant or irrelevant) that were fixated on in each question
They did this because they hypothesised that the intrusive eye movements as seen in smooth pursuits may influence scene viewing in schizophrenics too
There were no elevated looks to irrelevant locations in any task in schizophrenics compared to TD children.
Therefore, whilst saccadic behaviours are affected by schizophrenia in smooth pursuits, scene viewing is unaffected
A child with schizophrenia is asked to describe what is happening in a picture. They are then asked to follow a moving target on a screen.
Describe what we can expect their performance to be like in each task, providing evidence as to why
Children with schizophrenia experience a greater number of intrusive saccadic eye movements, but this is only apparent in certain contexts. People with schizophrenia have difficulties specifically with smooth pursuits, which is a smooth and continuous eye movement used to track moving objects. Studies comparing TD children and schizophrenic children have demonstrated that whilst TD children can closely match the direction and velocity of targets, schizophrenic children exhibit a greater number of anticipatory and catch-up saccades and spend less time fixated on the object (Jacobsen et al., 1996; Ross et al., 1999). Therefore, their performance in the target tracking task would likely be poor.
However, these intrusive saccades do not appear to influence scene viewing. Karatekin and Asarnow (1999) compared eye movements and fixations between TD children and children with schizophrenia when asked to derive specific information from a visual scene. They found that schizophrenics did not look at task irrelevant information significantly longer than TD children, refuting their hypothesis that intrusive saccades may affect their performance. Therefore, schizophrenia does not appear to influence performance in scene viewing and they would be able to complete this task.
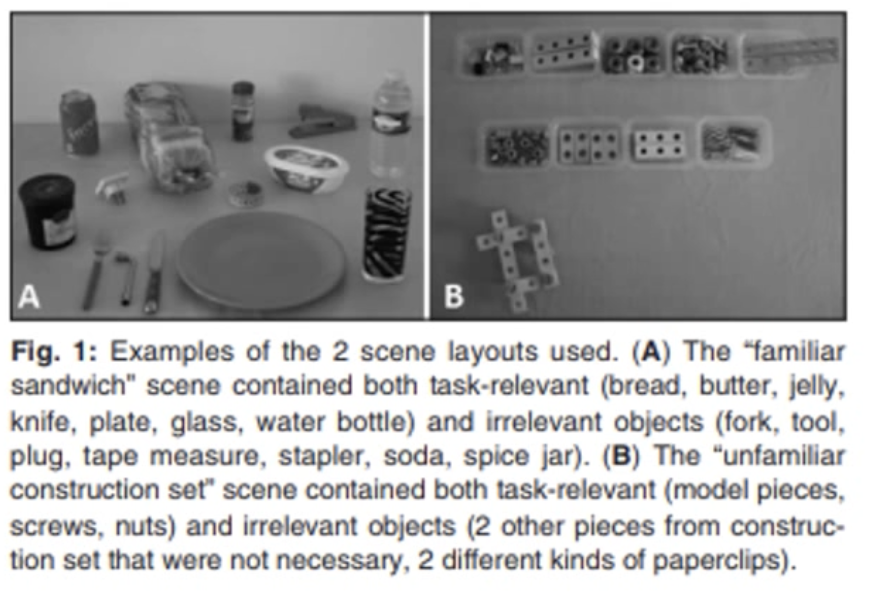
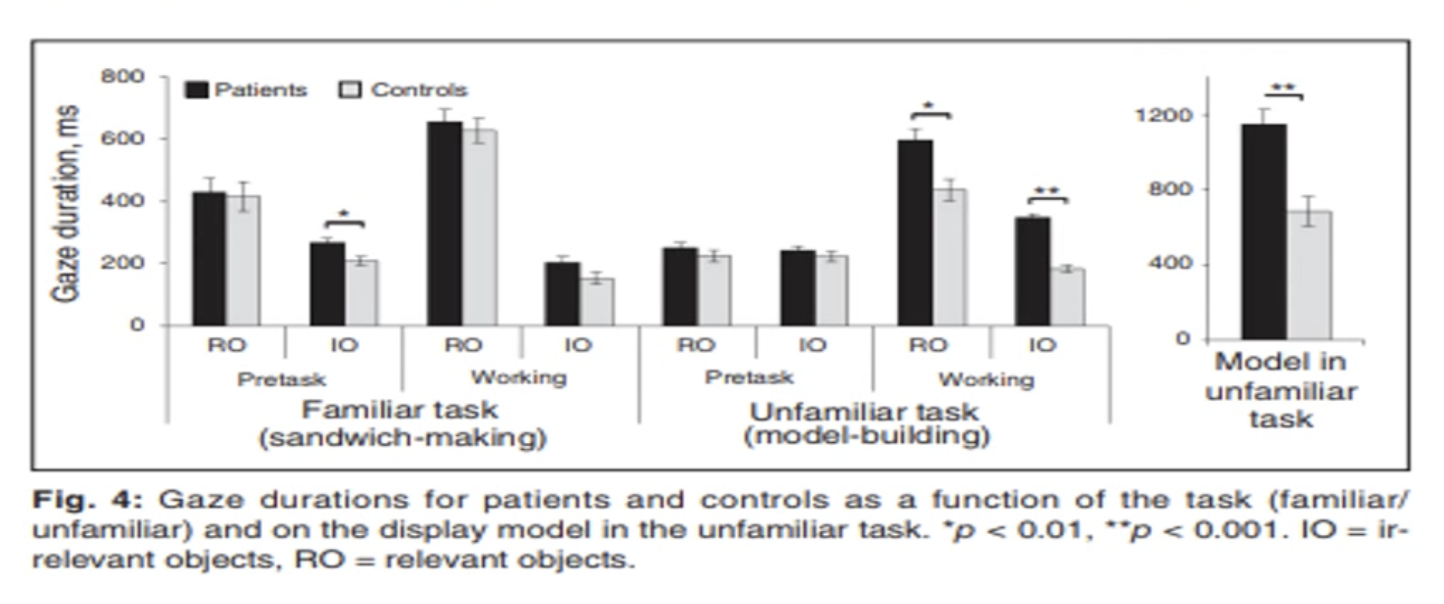
Describe Delerue et al.’s (2013) study
They conducted a sandwich making task with individuals with schizophrenia and healthy controls to see if there were any differences in gaze and fixation patterns in free viewing (looking at a kitchen bench with task relevant and irrelevant objects) vs active viewing (making the sandwich in that scene) in familiar VS unfamiliar tasks
People with schizophrenia looked (fixations and gazes) at both task relevant and irrelevant objects significantly longer than healthy controls ONLY IN THE FREE VIEWING CONDITION FOR THE FAMILIAR TASK (sandwich making)
Think: They be staring at it all for ages when there is no task demand, but when they start doing the task, they don’t give a fuck about irrelevant objects anymore
This was inverted when the task was unfamiliar: in the active viewing task, they fixated and gazed upon both relevant and irrelevant objects significantly more than healthy controls
May be because they were making less look-ahead fixations (cannot plan unfamiliar tasks)
There were no differences in fixations between HC and schizophrenics in free viewing unfamiliar tasks.
Takeaway: Schizophrenics be fixating. When the task is familiar they just want to take it all in when they’re sitting back and doing nothing, but when they do the task they lock in. When it is unfamiliar, they need to know EVERYTHING even if its irrelevant to the task which makes everything longer; even motor initiation of the task.
They be freaking out in unfamiliar tasks, which is proposed to be due to a planning deficit
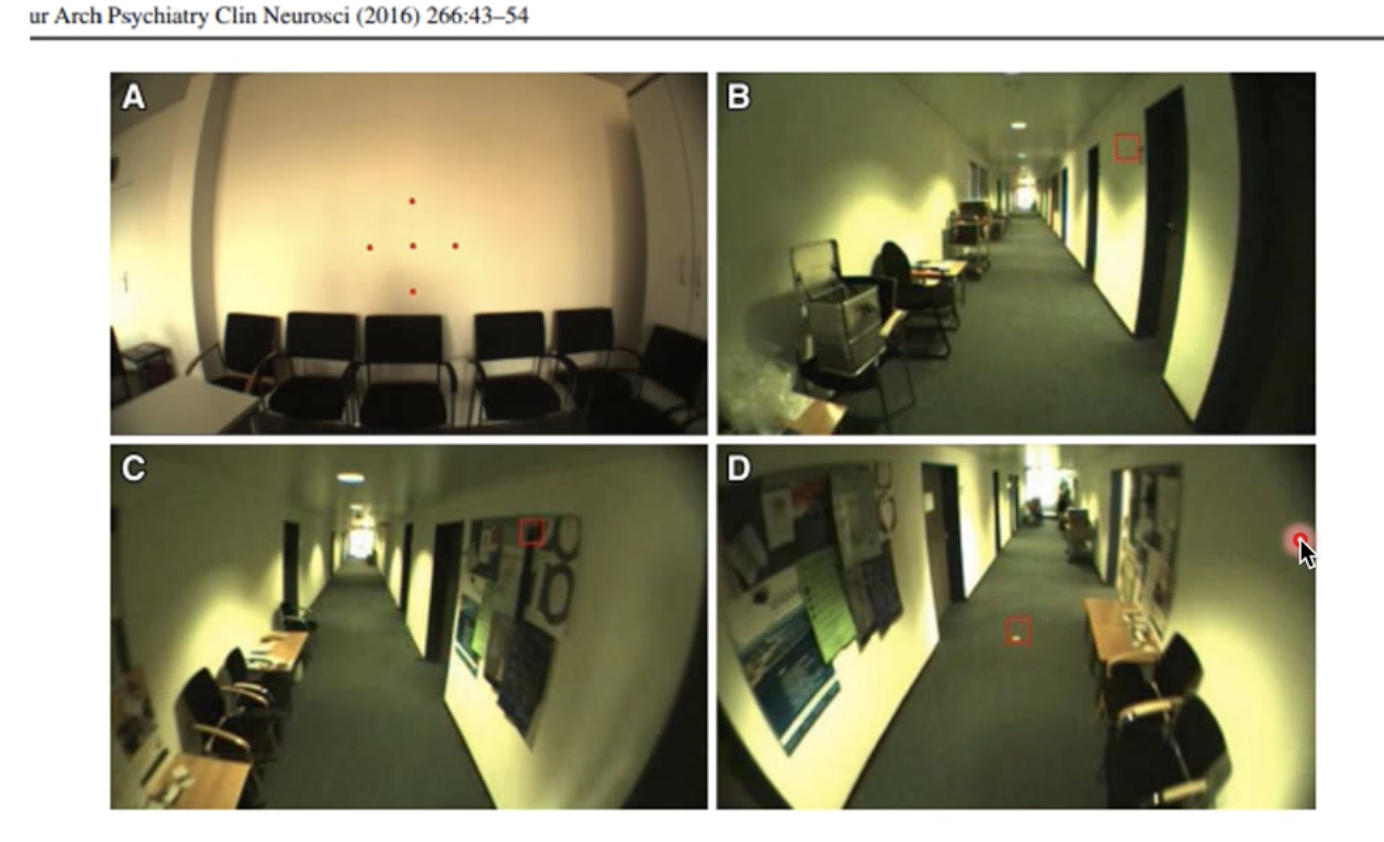
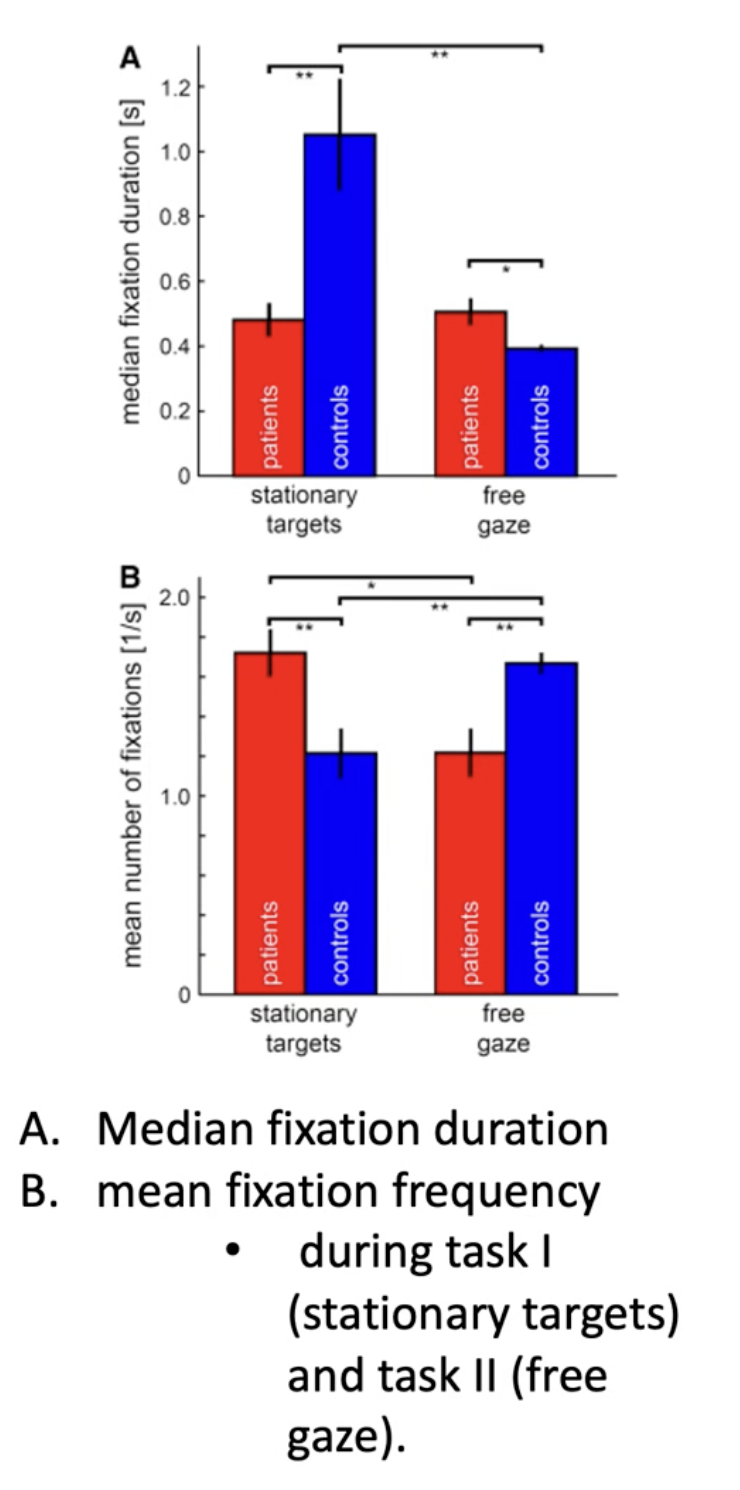
Describe Dowiasch et al.’s (2016) Study
Compared eye movements of schizophrenics VS healthy controls in 4 natural tasks using a mobile eye tracker:
Fixating on stationary objects in a waiting room
Sitting in a hallway with free gaze
Walking down the hallway
Visually tracking targets on the floor while walking straight ahead
Results:
When they had to fixate on predefined targets in a freely chosen, random order, the patient’s fixations were significantly shorter in duration, but occurred more frequently than healthy controls (think: that gif where she’s eating chips and looking side to side)
During free gaze (i.e. sitting aimlessly in a hallway), this was inverse and they fixated for LONGER, but less frequently than HCs.
However, the median fixation duration did not differ between the two groups
Takeaway: There are significant differences in fundamental oculomotor parameters between schizophrenic patients and HCs during NATURAL behaviour in a REAL environment
Not just in lab settings!
Also shows they might have some compensatory strategies in natural settings to overcome deficits observed in lab studies, but little is known about how
Meaning, the bleak results from previous lab studies probably don’t translate into the real world (good news)
Describe differences in eye movements for people with ADHD
Context: There are fronto-striatal deficits that make it difficult for these individuals to inhibit reflexive responses, leading to hypotheses that people with ADHD may have some more crazy eye movements going on - not really the case!
The Jacobsen et al. (1996) study showed that whilst there are differences between ADHD and HC, the differences are not as significant as schizophrenics.
Can do smooth pursuits fine (image)
Struggles with saccadic inhibition (Munoz et al., 2003)
Think: They just can’t stop themselves from looking!
Who would do better in smooth pursuit tasks?
ADHD or schizophrenics
ADHD
Describe Munoz et al.’s (2003) study

Tested performance for people with ADHD in oculomotor tasks that require suppression of reflective or unwanted saccadic eye movements
Measured eye movements for ADHD and HCs in pro- and anti-saccade tasks in 9-59yos
Pro saccade: they look at a central fixation point and instructed to look at a target to the side when it pops up (reflexive)
Think: Look at it!!! Woooo!!!!
Anti-saccade: they must suppress the saccade and look to the opposite side of the fixation point away from the target.
Think: MIND YOUR BUSINESS
Found that people with ADHD make significantly more errors than HCs in this task with more intrusive saccades (rate of saccades/sec)

Describe the results of Munoz et al.’s (2003) study
Pro-saccade task:
People with ADHD had:
Long reaction times
Greater intra-subject variance
Saccades has reduced peak velocities and increased durations
Summary: When ADHDs were allowed and encouraged to look at the target, they were much slower with their eye movements and reactions, and their individual performance was inconsistence
Anti-saccade task:
People with ADHD had:
Greater difficulty suppressing reflexive pro-saccades toward the target
Increased reaction times for correct anti-saccades
Greater intra-subject variance in a third task requiring prolonged fixation
Summary: It took them more effort and time to suppress the reflex to look at the target than HCs (they struggled to inhibit basically)
In general:
ADHD had more intrusive saccades during periods they should have been fixating on the central area (naughty)
Takeaway: ADHD Px have reduced ability to suppress unwanted saccades and control their fixation behaviour voluntarily. This is consistent with a fronto-striatal pathophysiology
Think: It is not that they can’t do it, it's more that its harder to voluntarily control
William’s Syndrome
Genetic disorder characterised by:
Disassociation of higher cognitive functions
Distinct social phenotype
Drive toward social behaviour, often labeled as ‘hyper-sociability’ or ‘pro-social compulsion’
They demonstrate
Desire to interact regardless of familiarity
Hold prolonged face gaze during interactions
Atypical interpretations of facial cues for emotion and identity
Prevalence is 1 in 20 000 people
Think: Anti-autism
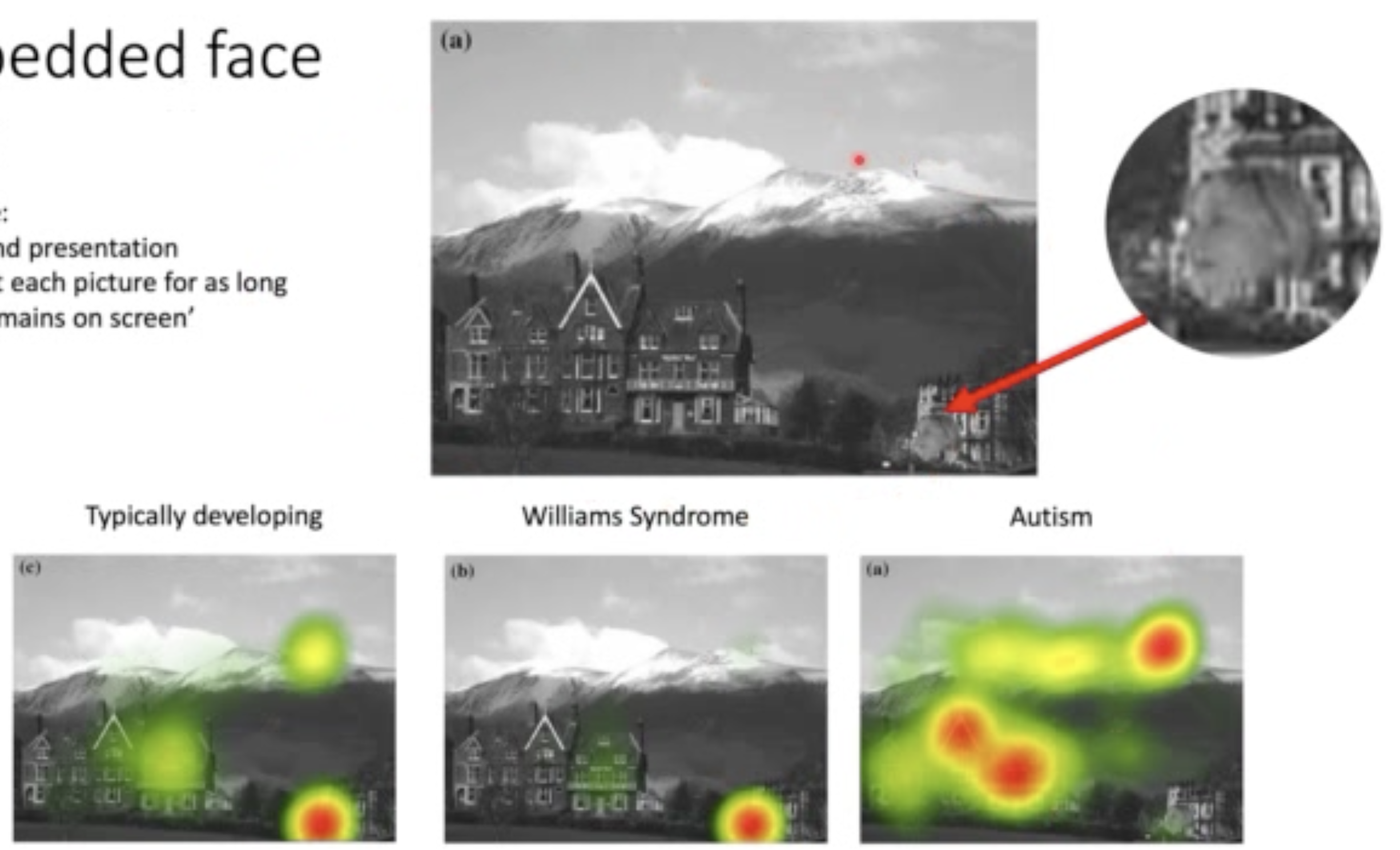
Describe Ruby & Hancock’s (2009) study (was a reading)
Compared how faces capture the attention of people with autism vs William’s syndrome
Used an embedded face task (basically hide a face in a scene)
Scenes were presented for 5 seconds and they were instructed to look at each picture for as long as they were on the screen
Also used a scrambled picture task (same thing but a picture was broken into tiles and components of the picture were scrambled, with one containing a face)
Results:
Embedded Face Task:
There was no difference between William’s and TD in how long it took them to detect the face
However, Willliam’s kids fixated on the face for significantly longer and TD
ADD kids took significantly longer to detect the face
When they did detect it, they spent less time fixating on it (didn’t care)
Scrambled Picture Task:
TD and William’s took the same amount of time to locate the face, but William’s fixated significantly longer
ADD did not fixate on faces for long at all
When a fixation was made, it took significantly longer to get there than other groups
Summary: Individuals with ADD showed dramatically less face gaze with shorter face fixations (don’t want to look at them, and when they do, make it short)
Individuals with William’s syndrome exhibit prolonged face fixations and face gaze.
What tasks can be used to assess facial attention?
Embedded face task
Scrambled picture task
Both ‘hide’ faces in scenes that don’t make much sense and track eye fixations
Evaluate this statement:
People with autism cannot process facial information
Evidence suggests that it may not be a reflection of ability, but rather that they are just not looking.
Ruby & Hancock (2009) found that in a face scramble and embedded face task, individuals with ADD took significantly longer to locate the face in the image, and when they did fixate, the fixations were significantly shorter than people with William’s syndrome and TD individuals.
There may still be deficits in facial processing, but this observation likely has something to do with those lack of fixations to actually detect the information in the first place.
What is the general pattern of fixations and eye movements for autistic people in regard to faces?
They show significantly less face gaze (less likely to fixate on faces) and when they do, the fixation duration is much shorter (Ruby & Hancock, 2009)
What is the general pattern of fixations and eye movements for William’s syndrome in regard to faces?
They have prolonged durations of face fixation and gaze
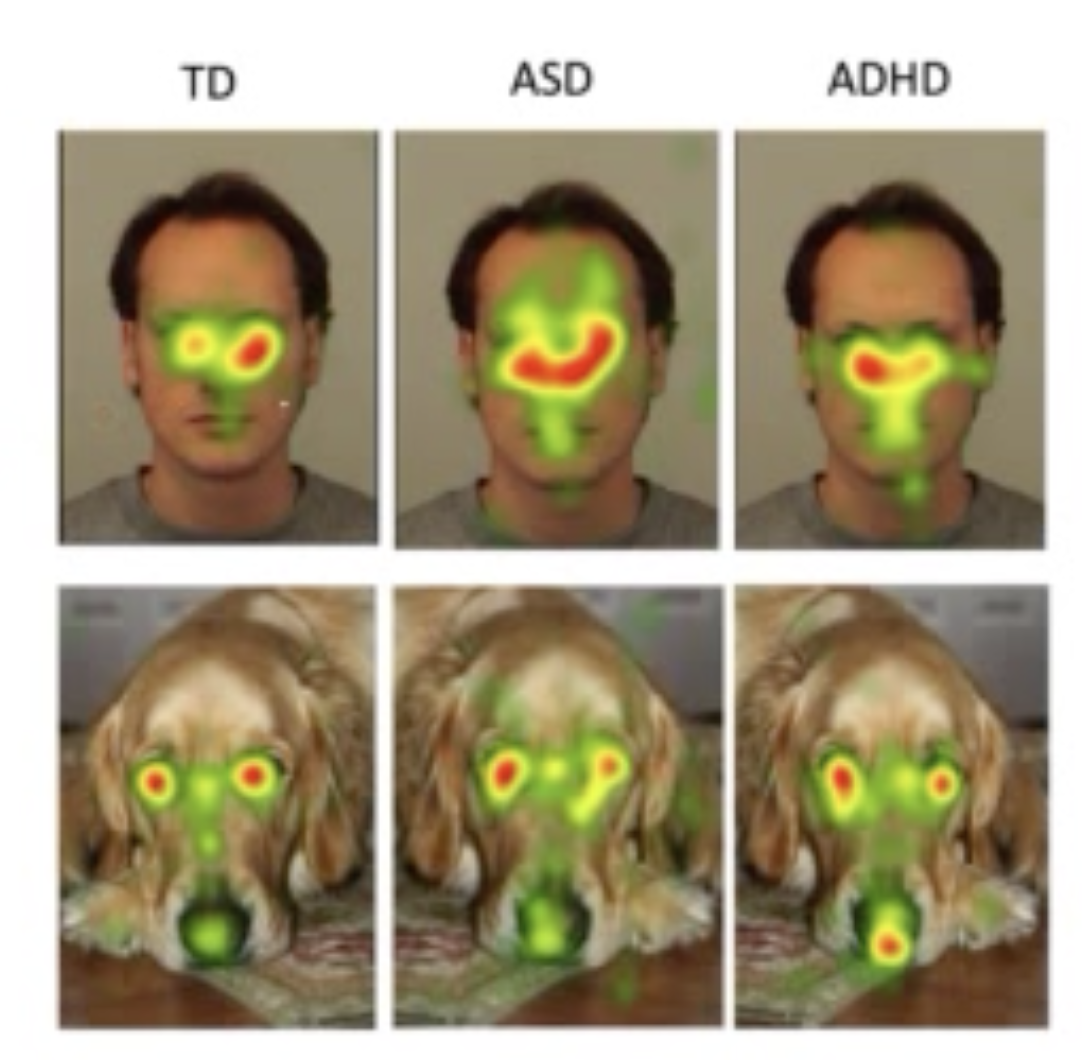
Describe Muszcat et al's (2015) study
They compared face scanning between people with ADHD, ADD or TD when looking at dogs or humans
Found that:
ADD and ADHD kids spent less time viewing the eye region than other regions of the face
Supports that difficulties in processing social cues may be shared by both conditions
People with ADHD had higher intellectual and adaptive functioning than people with ADD, but it didn’t impact the amount of time or region of interest
Takeaway: People with ADD and ADHD are less likely to look people in the eye
Limitation: Lab based - is this generalisable?
What did Pelc et al. observe?
In a face recognition task, children with ADHD had more difficulties with anger and sadness faces than other emotions
Problems in emotion recognition were also identified in boys at risk for ADHD
Describe Fletcher-Watson et al.’s Study
Naturalistic study where they tracked eye movements of people with ASD to investigate attention to social information
Presented ASD and TD adults/kids with a complex social scene (left), alongside a non-social scene (right)
Px were to free view the scenes
Results:
The people in the ADD group appeared to have a normal attentional preference for social information
People in the TD group were more inclined to look at the object being looked at by the person in the scene than the ASD group.
Takeaway: Social attention deficits in ADD may not be because they don’t attend to social information per say, but they don’t attend in the same way TD people (i.e. staring at the person instead of the object the person is looking at) which may produce serious difficulties in real-life scenarios
This study was good because it was in a naturalistic setting, not lab

Body Dysmorphic Disorder
A preoccupation with an imagined defect in one’s appearance
Distress causes functional impairment
Characterised by some of the following behaviours:
Excessive mirror gazing (or avoidance)
Comparison of self to others
Excessive camouflage
Skin picking
Reassurance seeking
Avoidance of social situations
Intimacy avoidance
Increased use of alcohol or illegal substances
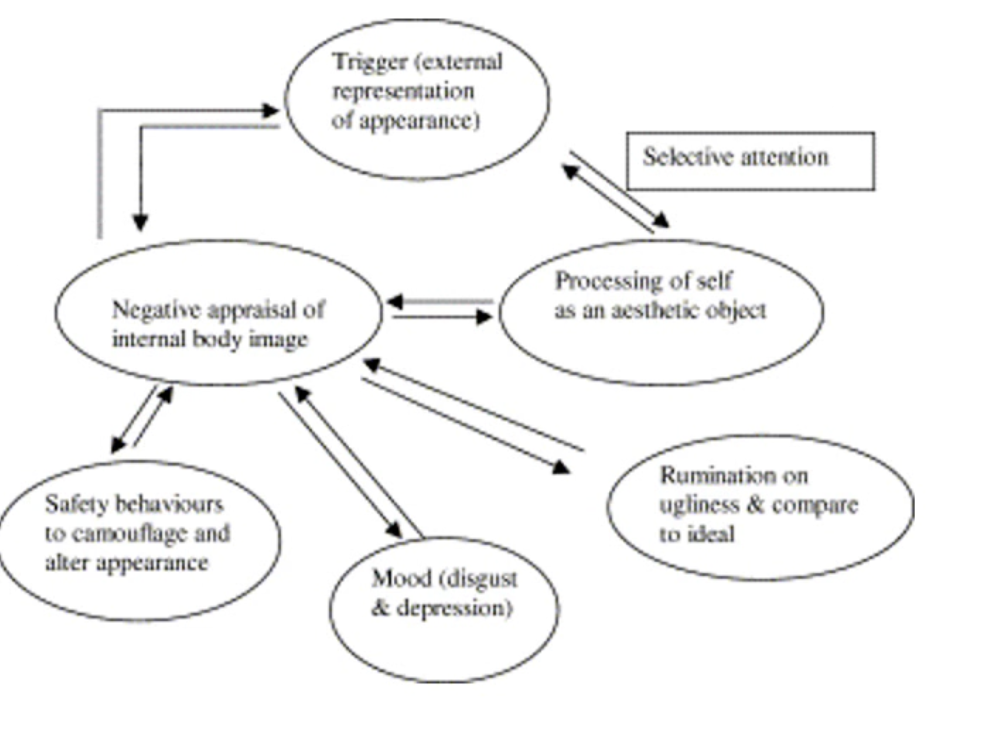
Describe how looking in a mirror can act as a trigger for BDD symptoms according to Veale’s model
Cyclic in nature and the process perpetuates its own existence
They look in the mirror and selective attention to negative stimulus (ie. stomach) triggers a negative evaluation of self, but also promotes the processing of self as an aesthetic object
These all bidirectionally perpetuate each other
The negative appraisal leads to
Safety behaviours like camouflaging or avoidance
Negative moods (disgust and depression)
Rumination on ugliness and comparisons to ideal
Describe Greenberg et al.’s Study
They studied how HC groups vs people with BDD viewed pictures of themselves and others, and compared them
Individuals with BDD fixated for longer on their own features they perceived as unattractive
This could be due to an existing attentional bias that maintains the symptoms, but it could simultaneously contribute/reinforce the bias itself
BDD also allocated more visual attention to the attractive features of others, which perpetuates upwards comparisons
HCs had a more holistic view of themselves, indicating a more positive attentional process
Takeaway: there appears to be a cyclic process involving an attentional bias with people with BDD where they fixate on ‘unattractive’ parts of themselves, but ‘attractive’ parts of others, which perpetuates upwards comparisons
Describe the cognitive and attentional patterns associated with anorexia nervosa and bulimia nervosa
Repeated checking of shape and weight as well as comparison of self to other’s body weight
Cognitive bias is perpetuated by an attentional bias towards perceived flaws with self compared to aspirations to others
Over-evaluation of body shape and weight
Takeaway: Suggests that individuals with these disorders may allocate different visual attention to different features which is perpetuated by the cognitive bias but simultaneously maintains it
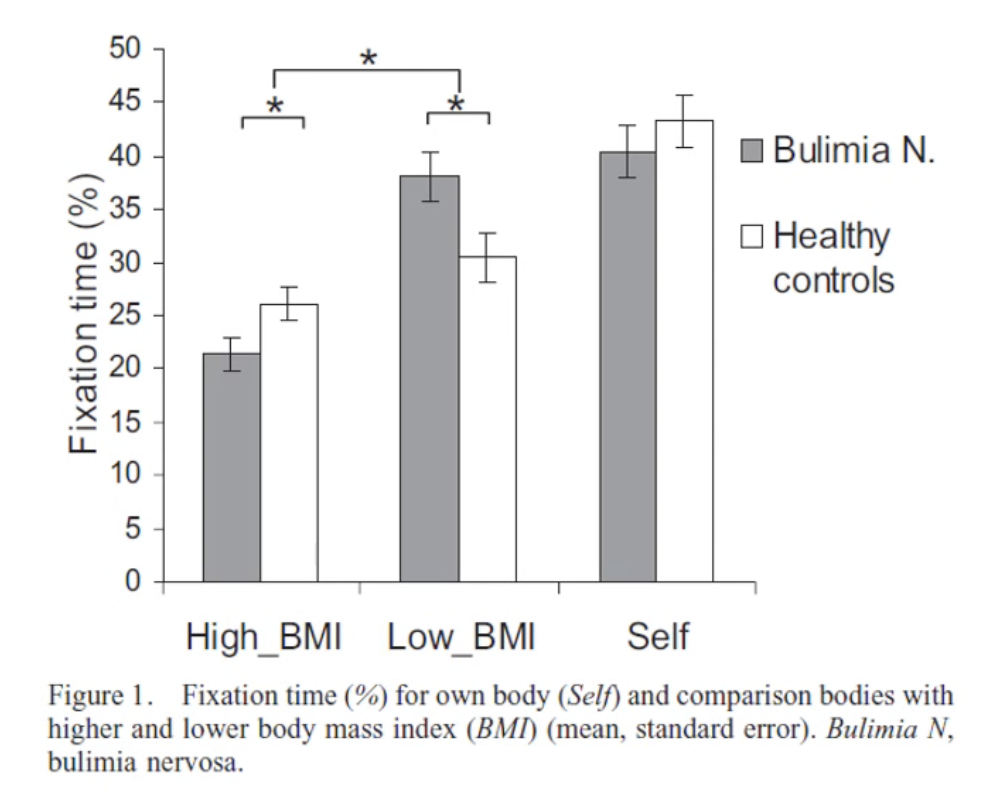
Describe Blechert et al.’s (2009) Study
Investigated whether individuals with bulimia nervosa preferentially fixate on images of others with low BMI
Results: Yes, it appears so
BN Px had longer fixations on individuals with low BMIs compared to HCs
They spent significantly less time fixating on individuals with high BMI
There was no difference between the amount of time spent fixating on their OWN image between the BN and HC groups
Takeaway: Disadvantageous social comparison strategies might be related to body dissatisfaction and maintenance of BN symptoms
Further support for the notion that upward comparisons play a huge role for EDs
Describe Horndasch et al’s (2021) Study
Compared visual attention of adolescent ED patients and HCs when looking at images of women wearing bathing suits or underwear
3 picture conditions; underweight, average and overweight
Results:
All Px directed their visual attention to the abdomen, buttocks, hips and upper legs (no differences between ED and HC)
Think: No one is safe! This is why social media can be harmful
HOWEVER, ED Px fixated on unclothed body parts for longer than HCs
Takeaway: People with EDs appear to have an attentional bias towards parts of bodies often deemed unattractive gives rise to potential attentional training interventions to reduce bias and prevent harm from idealised media images.
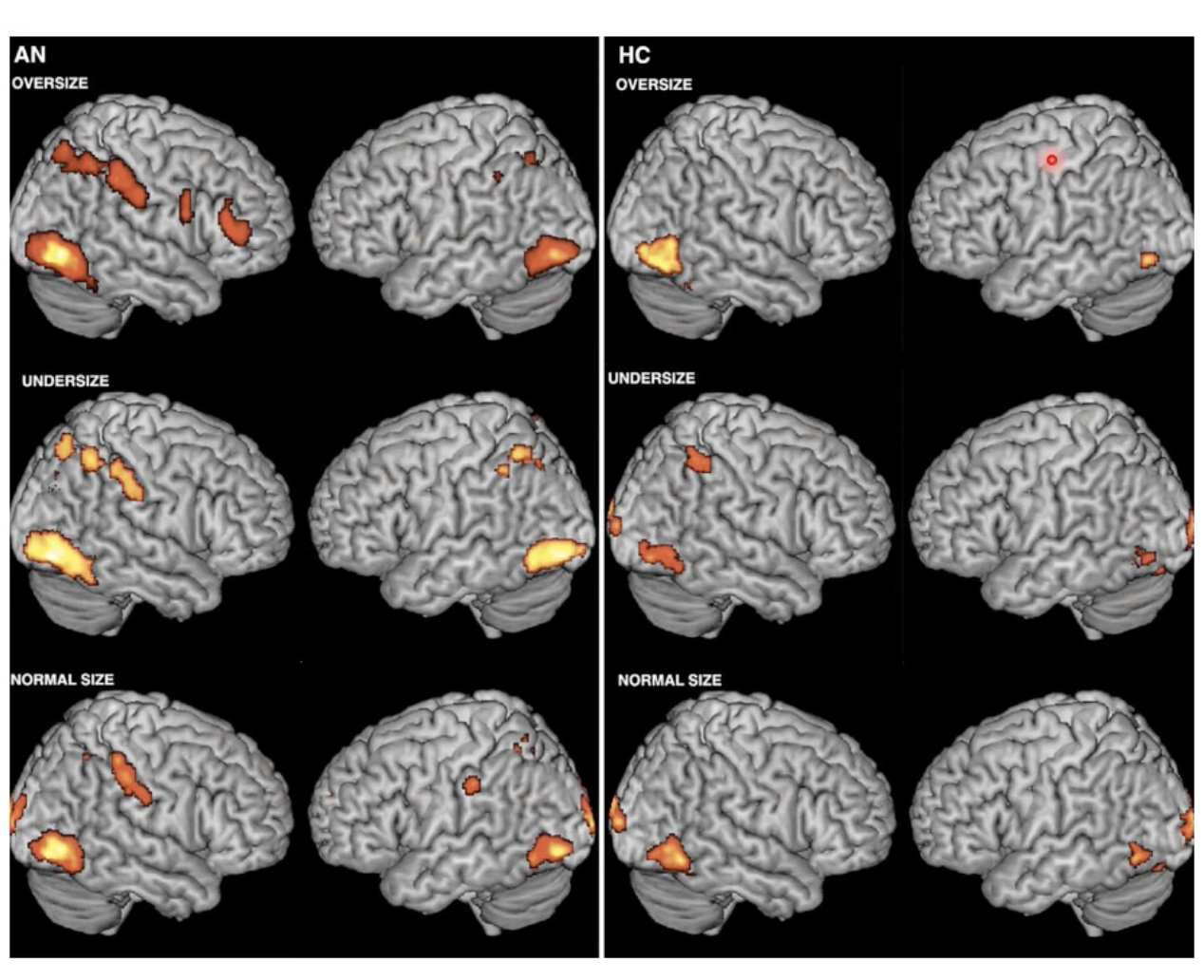
Describe Castellini et al.’s (2012) Study
Compared fMRI images been people with anorexia and HCs when viewing altered images of themselves with different body weights
There was an elevated neural response in attentive, executive and self-evaluation networks in the brain for people with AN
ESPECIALLY when they viewed themself in the overweight condition
Everyone seemed to follow the same pattern of escalation with increase in body weight, but AN Px were stronger
Takeaway: A pathological neural response exists for people with AN which contributes to distorted body image through visual processing
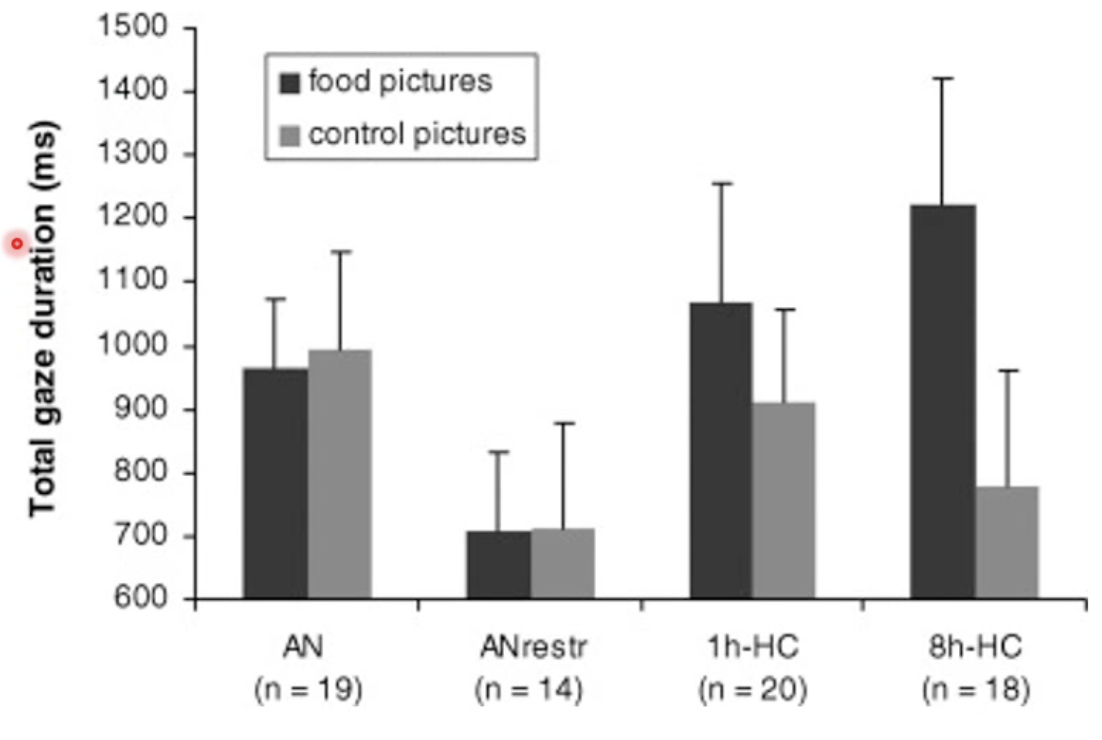
Describe Giel et al.’s (2001) study.
Assessed attentional processing of food pictures in patients with anorexia and HCs who had fasted for 8 hours or hadn’t.
Tracked eye movements for food and non-food control images
AN Px showed more attentional disengagement to food pictures compared with control (think: cognitive avoidance strategy?)
Takeaway: AN people appear to disengage attention from food related stimuli
Describe attentional biases for individuals with alcohol related disorders
Increased dwell times for alcohol related stimuli
Reduced inhibitory control on saccadic movements
Increased pupillary reactivity to visual stimuli regardless of emotional content
Limited visual attention to prevention messages (!)
Takeaway: There appears to be this pattern of ‘I shouldn’t do that’ so it makes them want to look at it….?
Think: Trying to cognitively engage with the substance rather than ingesting it because it is more acceptable and discrete