9.9 - Osmoregulation & thermoregulation
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
What is thermoregulation?
A homeostatic mechanism that enables organisms to control their internal body temperature within set limits
What are endotherms?
Animals that warm their bodies through metabolic processes & usually have a body temperature higher than the external, environmental temperature (e.g. mammals & birds)
What are ectotherms?
Animals that are largely dependent on the external environment for their body temperature (e.g. reptiles)
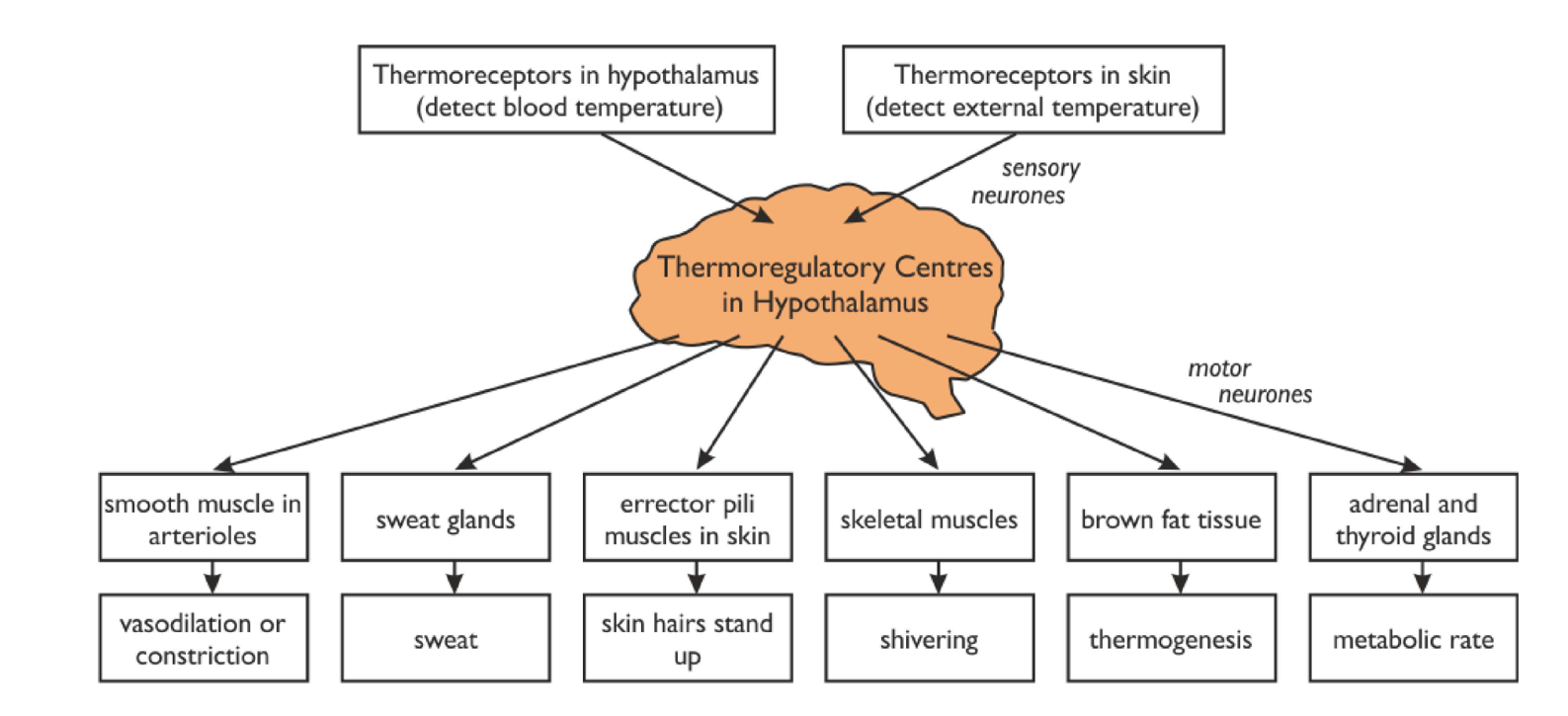
In humans, what is thermoregulation controlled by?
Two thermoregulatory centres in the hypothalamus, which receive input from two sets of thermoreceptors:
receptors in the hypothalamus itself → monitor temperature of blood flowing through the brain (core temperature)
peripheral receptors (receptors in the skin) → monitor external, environmental temperature
What are the two thermoregulatory centres?
Heat loss centre (activated by a rise in blood temperature):
impulses are sent down the parasympathetic nervous system to trigger responses in the skin, hair erector muscles & sweat glands to lower blood temperature
Heat gain centre (activated by a decrease in blood temperature):
impulses are sent down the sympathetic nervous system to trigger responses in the skin, hair erector muscles & sweat glands to raise blood temperature
How does the body respond to an increase in body temperature?
Sweating increases:
releases lots of heat energy to enable water from sweat to evaporate from the skin’s surface
Erector pili muscles relax:
causes hairs to lie flat against the skin
reduces the thickness of the layer of insulating air, allowing more heat to be lost by radiation
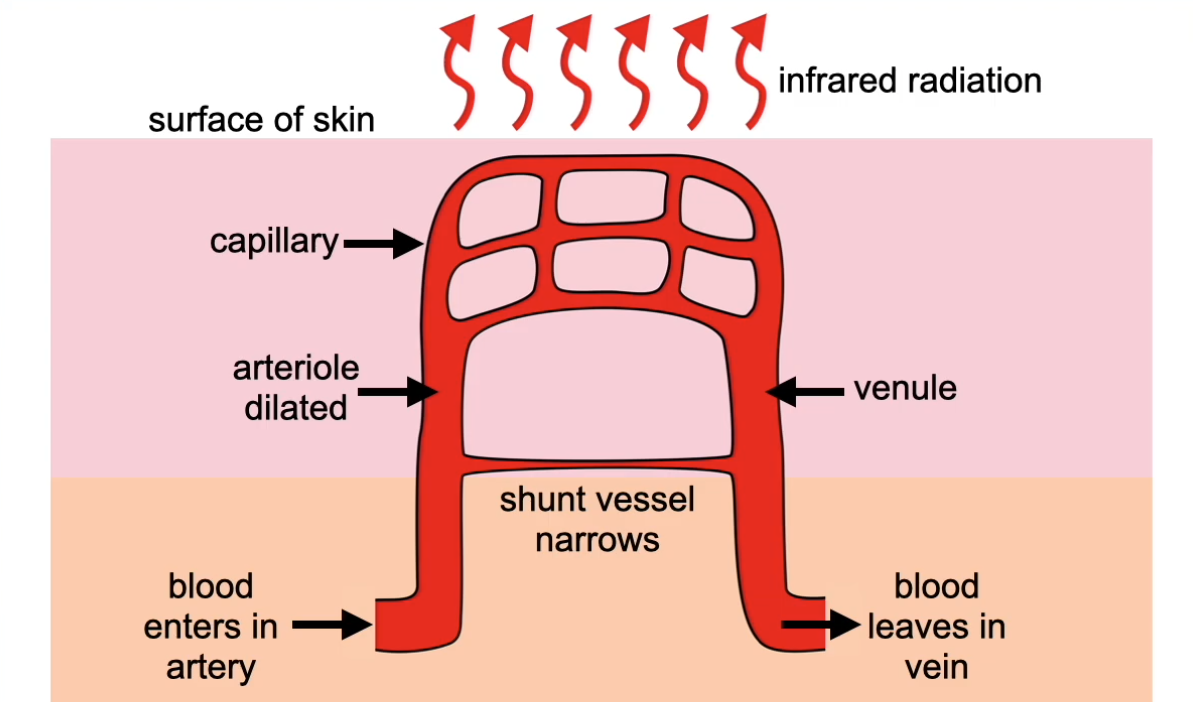
Vasodilation occurs:
sphincter muscles surrounding the arterioles relax
more blood flows into the capillaries near the skin’s surface & less blood flows through the arteriovenous shunt vessels
increased cooling, as more heat is lost by radiation
Reduced metabolic/respiration rate:
reduced secretion of adrenaline & thyroxine from the adrenal & thyroid glands
reduced metabolic heat generation
How does the body respond to a decrease in body temperature?
Shivering occurs:
rapid contraction & relaxation of muscles
increases respiration in muscle cells, releasing more heat energy
Erector pili muscles contract:
causes hairs to stand upright
increases the thickness of the layer of insulating air, reducing heat loss by radiation
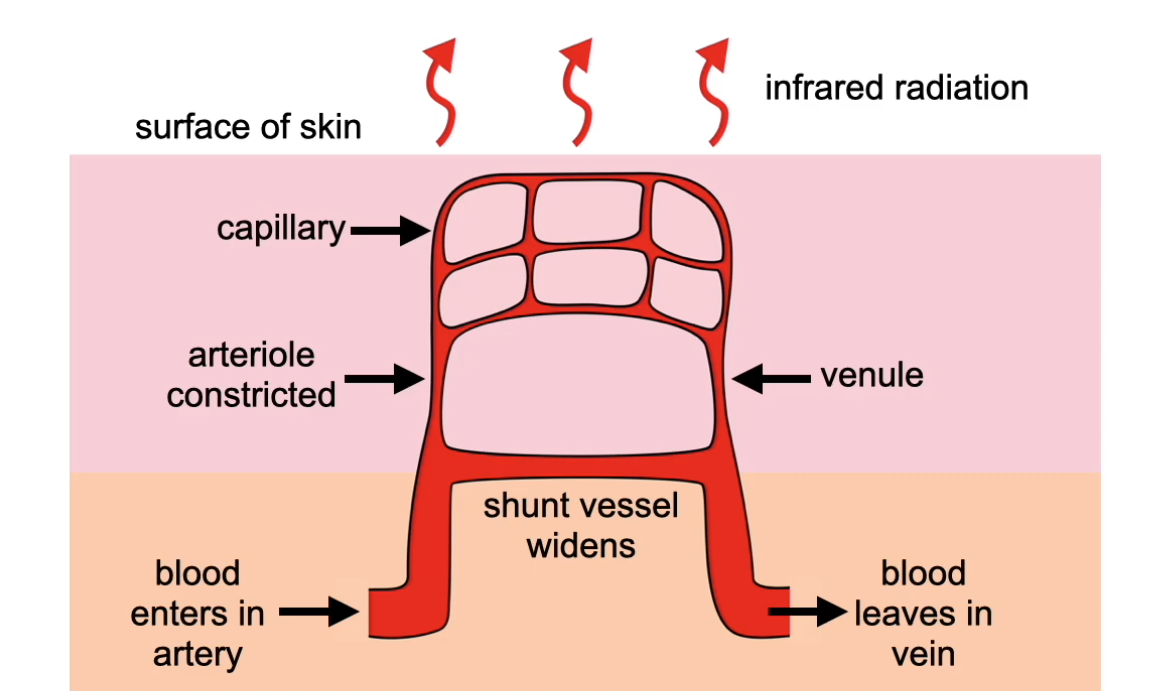
Vasoconstriction occurs:
sphincter muscles surrounding the arterioles constrict & arteriovenous shunt vessel widens
less blood flows into the capillaries near skin’s surface & more blood flows through the arteriovenous shunt vessels
reduced cooling, as less heat is lost by radiation
Increased metabolic/respiration rate:
increased secretion of adrenaline & thyroxine from the adrenal & thyroid glands
increased metabolic heat generation
How do ectotherms regulate their body temperature?
Thermoregulatory behaviour:
iguanas start everyday by basking on rocks in the sun until their metabolic rate is fast enough to become active
lizards lie down on warm ground to gain heat & raise themselves if they get too hot
at night, lizards shelter in burrows, which provide insulation to reduce heat loss
What are the kidneys in humans & other mammals?
A pair of dark reddish-brown organs attached to the back of the abdominal cavity
They are part of the urinary system & are surrounded by a thick layer of fat to protect them from mechanical damage

What are the two important functions of the kidneys?
Osmoregulation: regulate the water content of the blood (vital for maintaining blood pressure)
Excretion: remove the toxic waste products of metabolism (e.g. urea) & substances in excess of requirements (e.g. salts) from the body
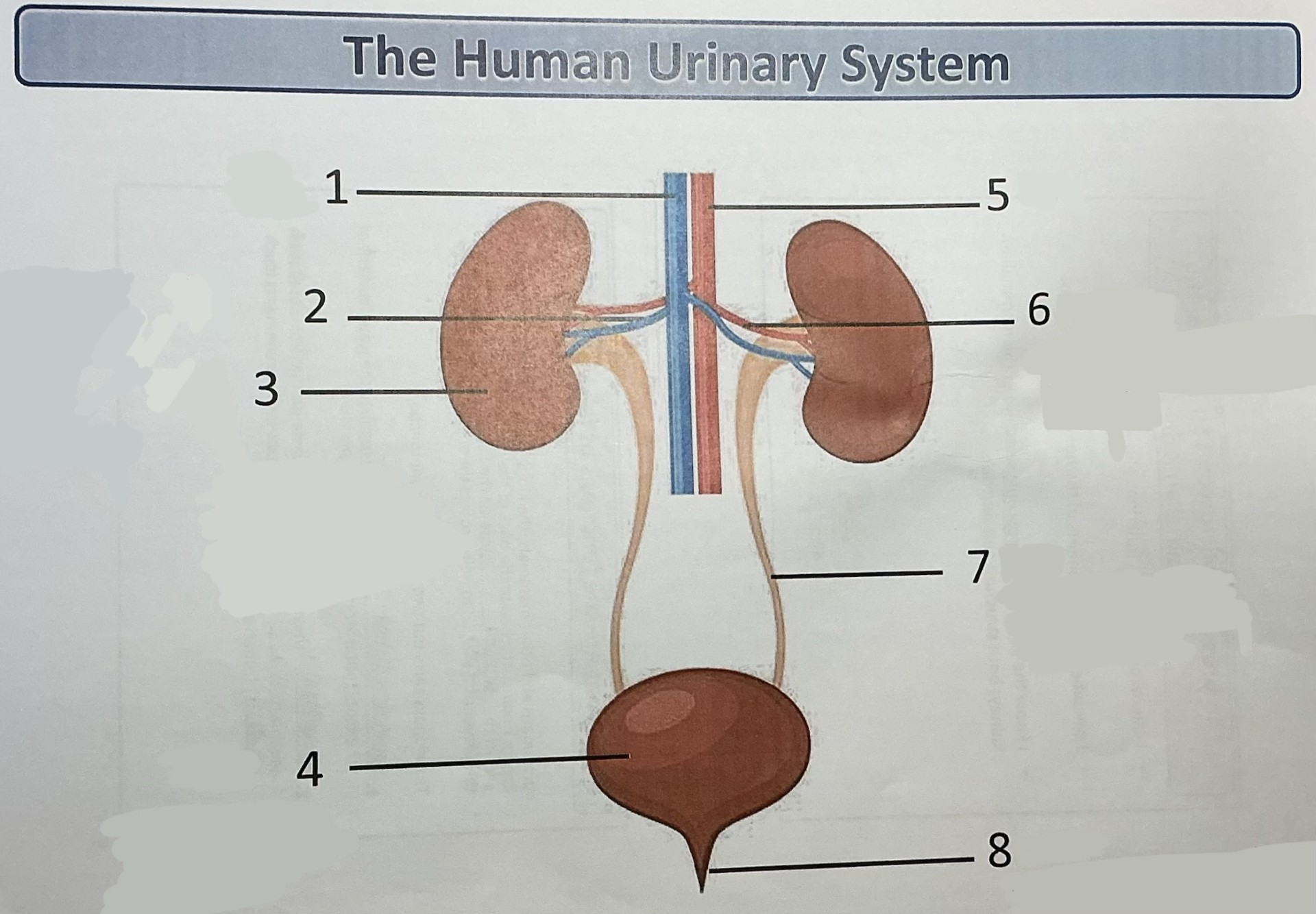
Label this diagram of the human urinary system
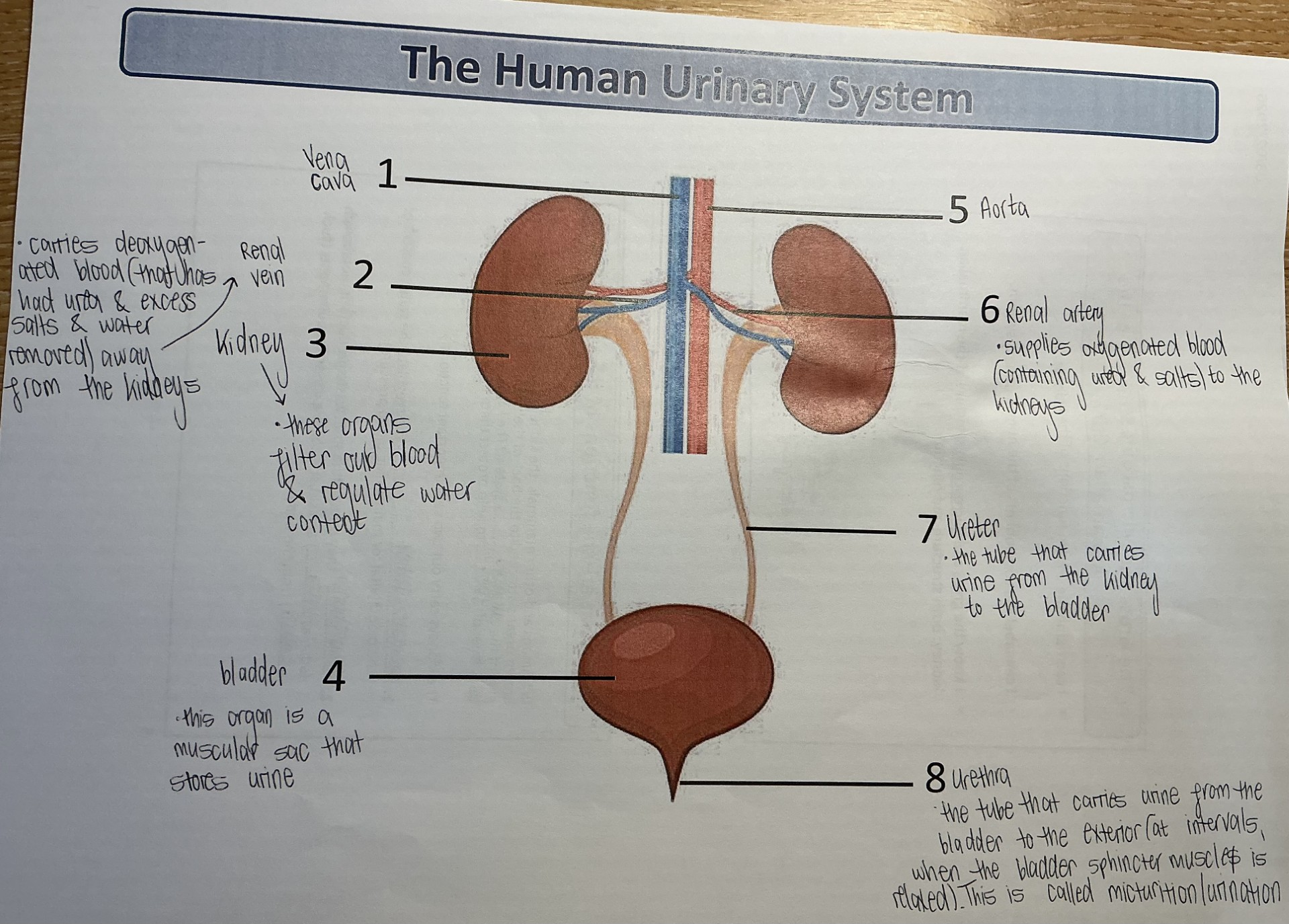
What is the function of the renal vein?
Carries deoxygenated blood (urea, excess salts & water removed) away from the kidneys to the heart
What is the function of the bladder?
This organ is a muscular sac that stores urine
What is the function of the renal artery?
Carries oxygenated blood (containing urea & salts) away from the heart to the kidneys
What is the function of the ureter?
The tube that carries urine from the kidney to the bladder
What is the function of the urethra?
The tube that carries urine from the bladder to the exterior, at intervals when the bladder sphincter muscle is relaxed (urination)
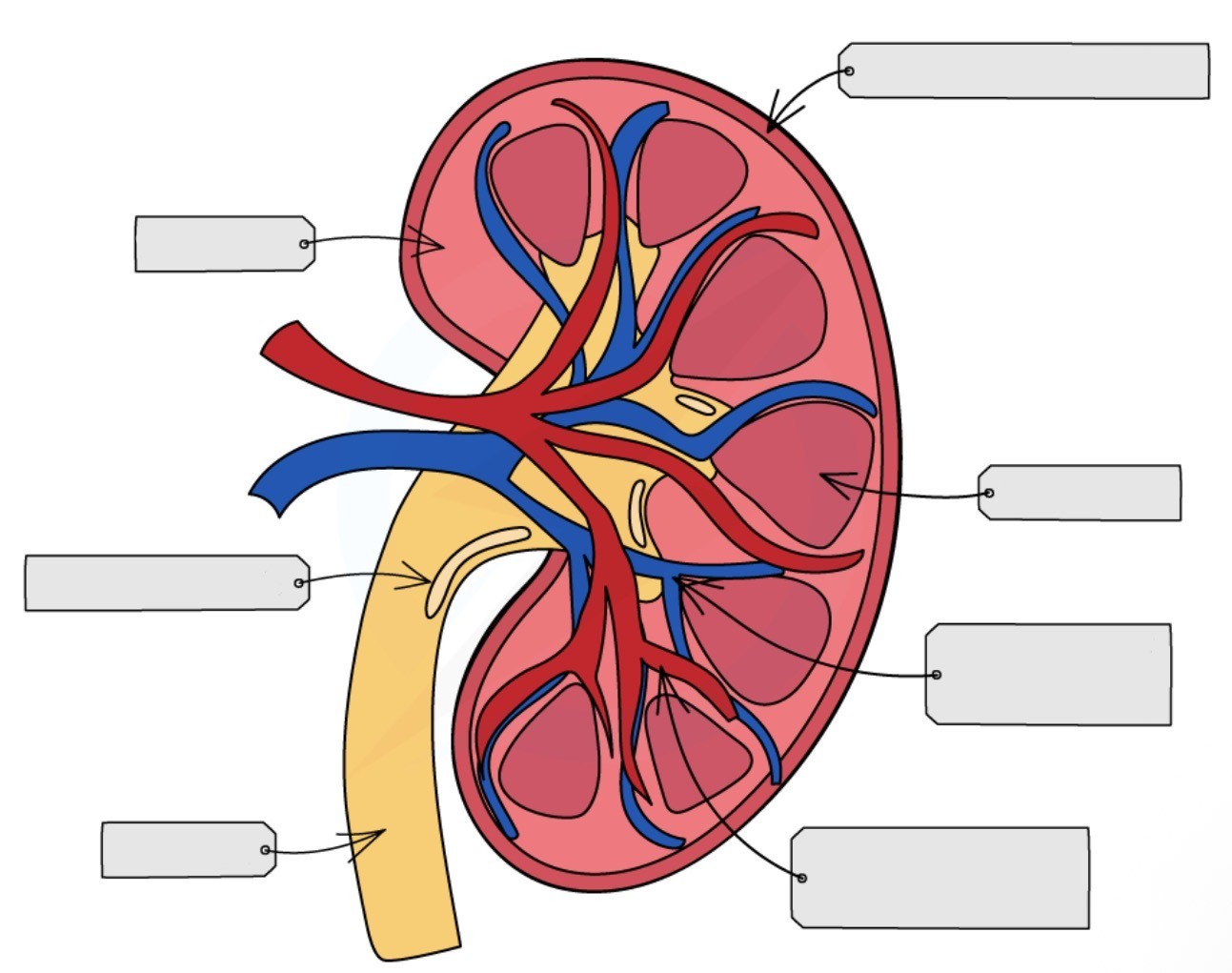
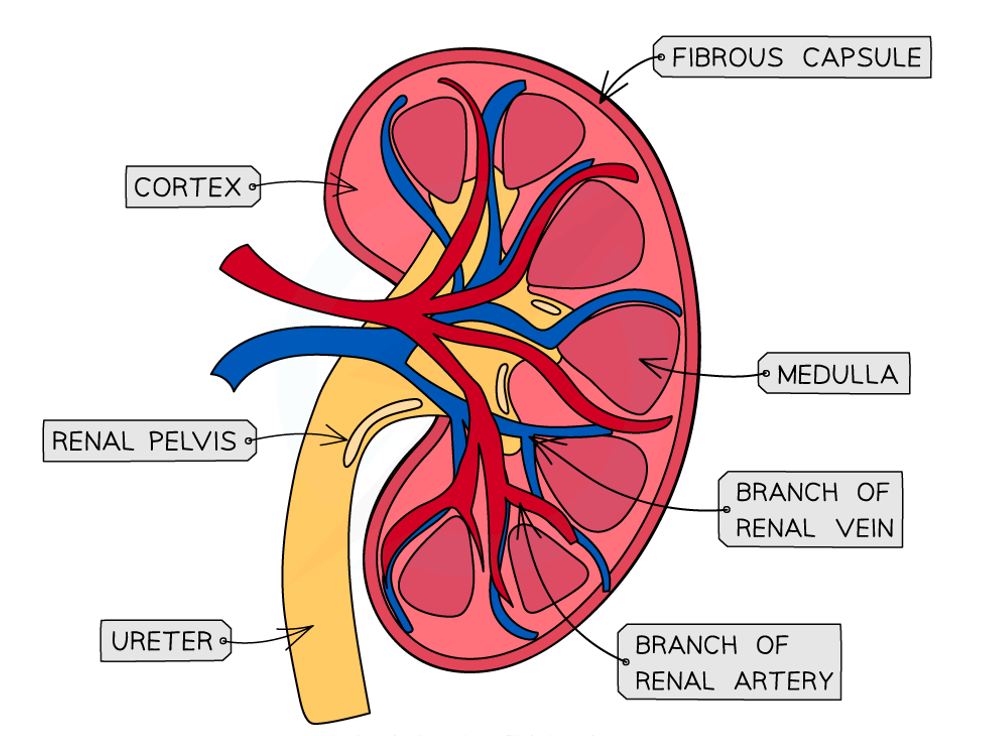
Label this diagram of a cross-section of a kidney
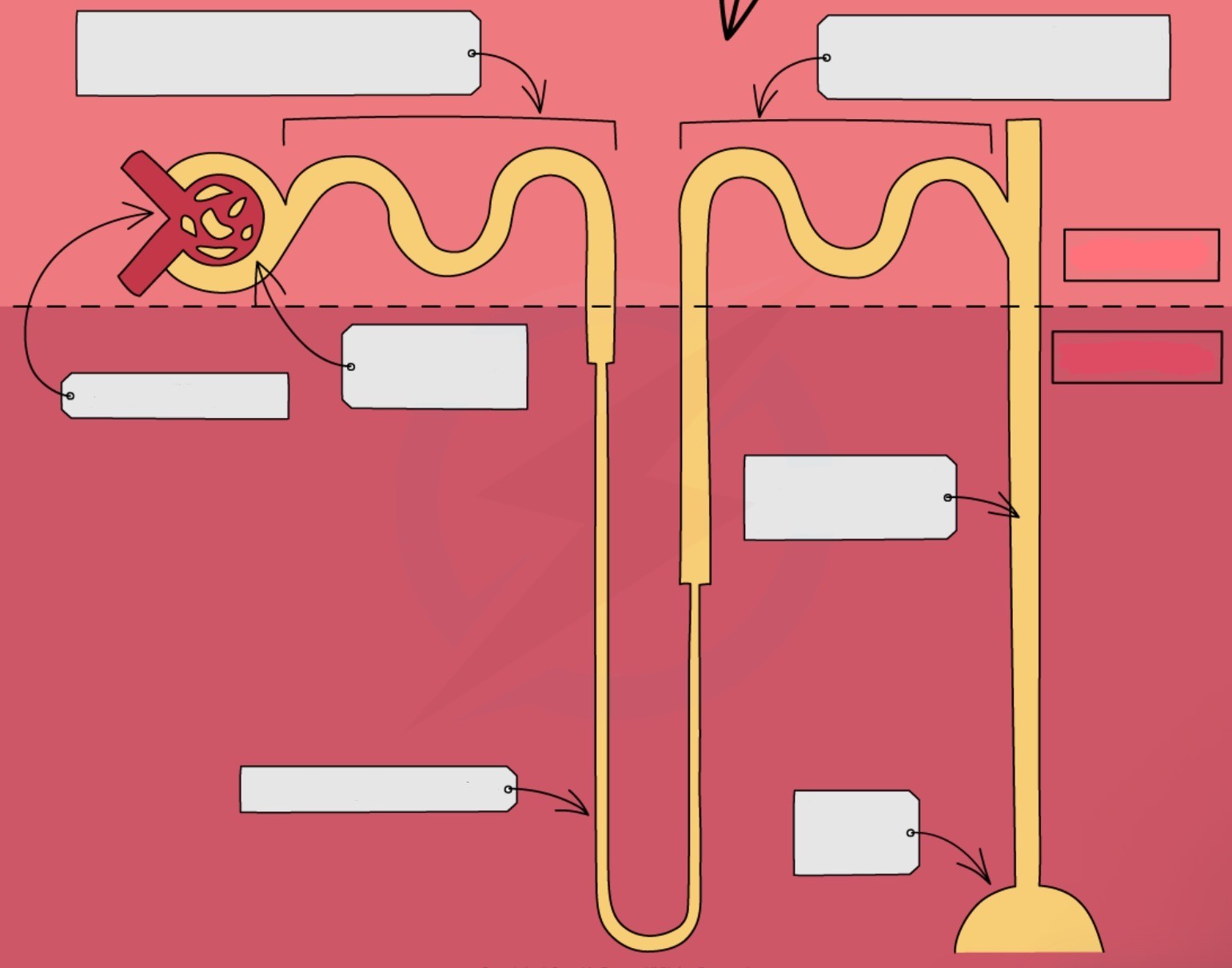
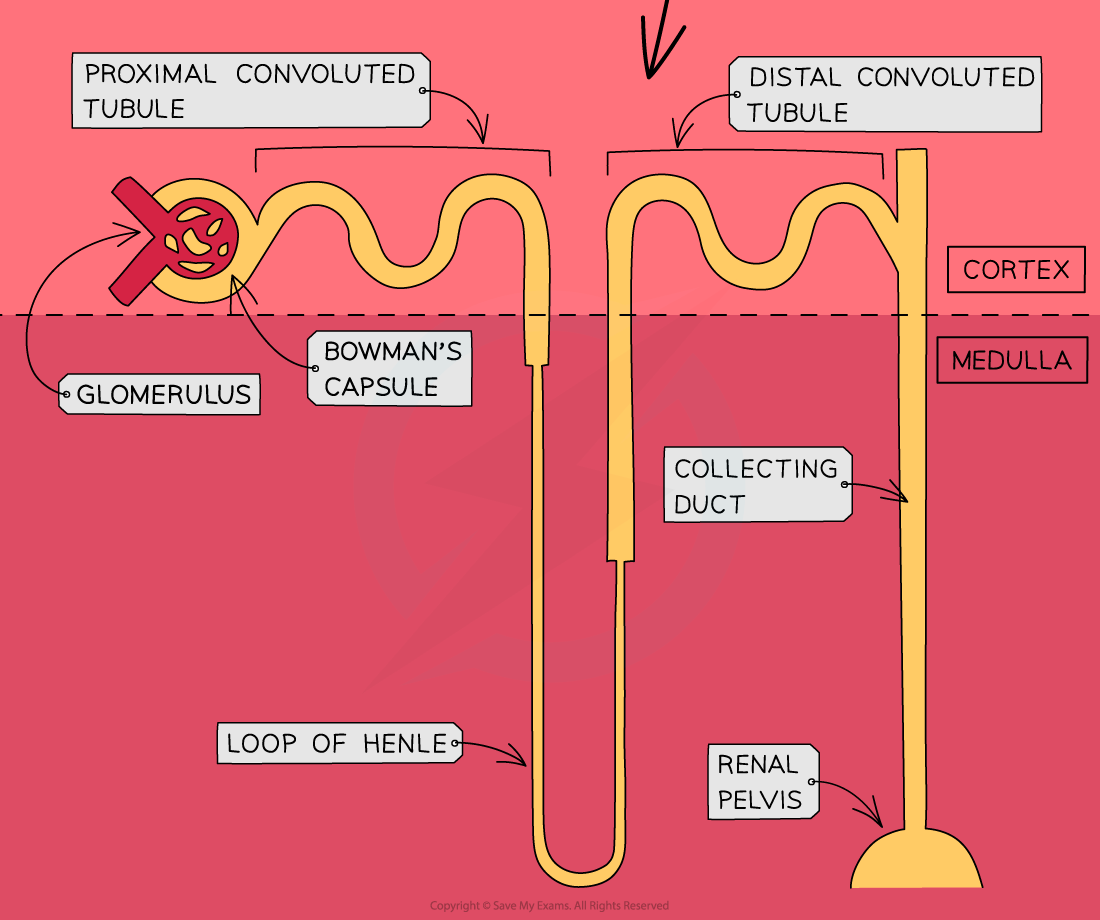
Label this diagram of the location & structure of a nephron
What are the two stages of urine formation in the kidneys?
Ultrafiltration:
small molecules are filtered out of the blood, into the Bowman’s capsule of the kidney nephron, forming glomerular filtrate
Selective reabsorption:
useful molecules are reabsorbed from the filtrate back into to the blood
after reabsorption is complete, the remaining filtrate forms the urine, which then flows out of the kidneys, along the ureters & into the bladder, where it is temporarily stored
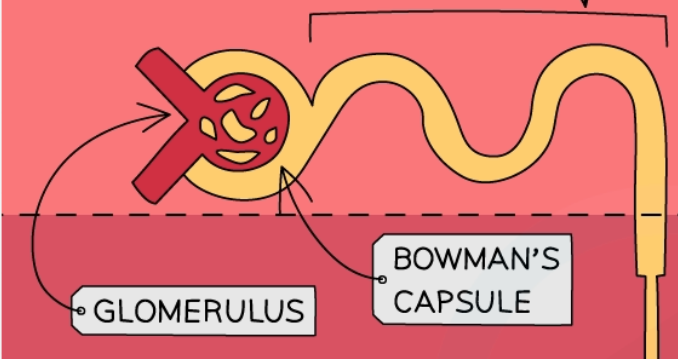
Where does ultrafiltration take place?
In the glomerulus & Bowman’s capsule
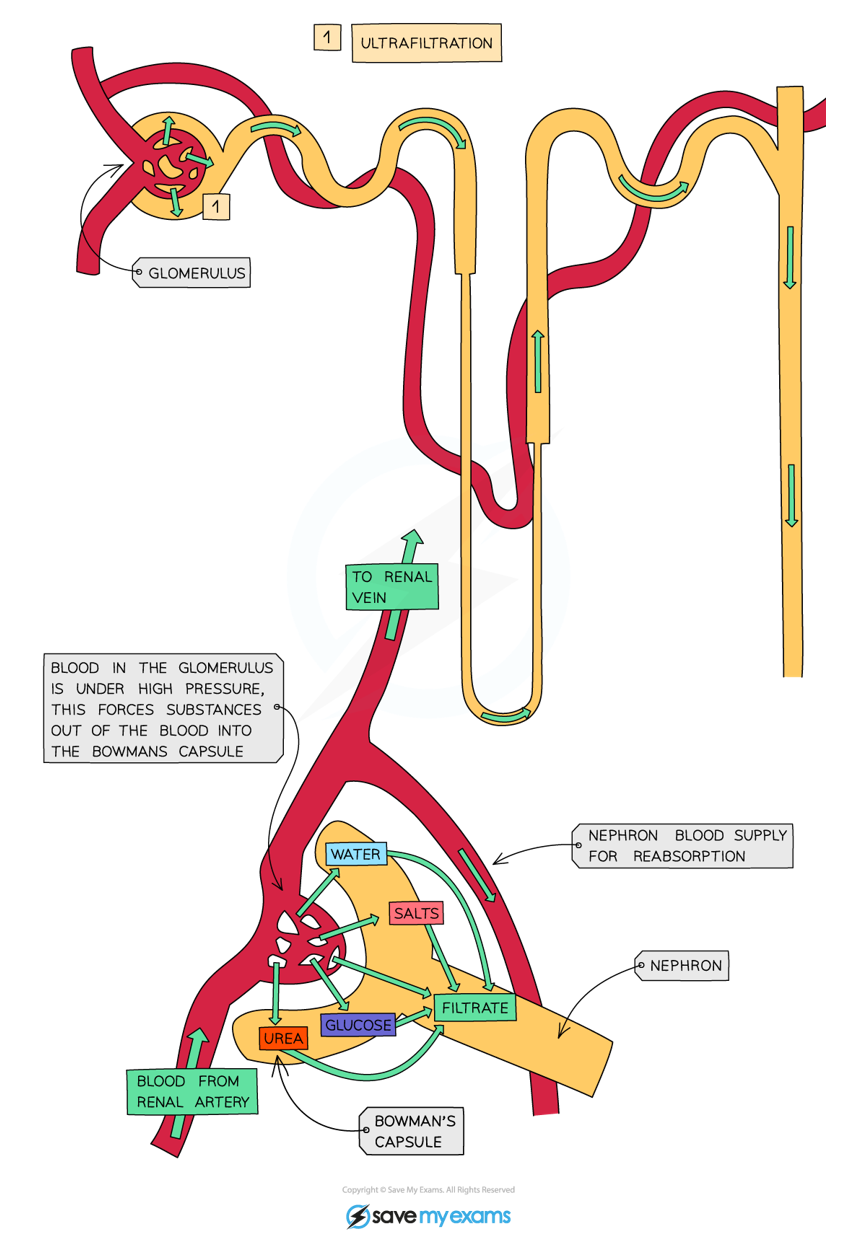
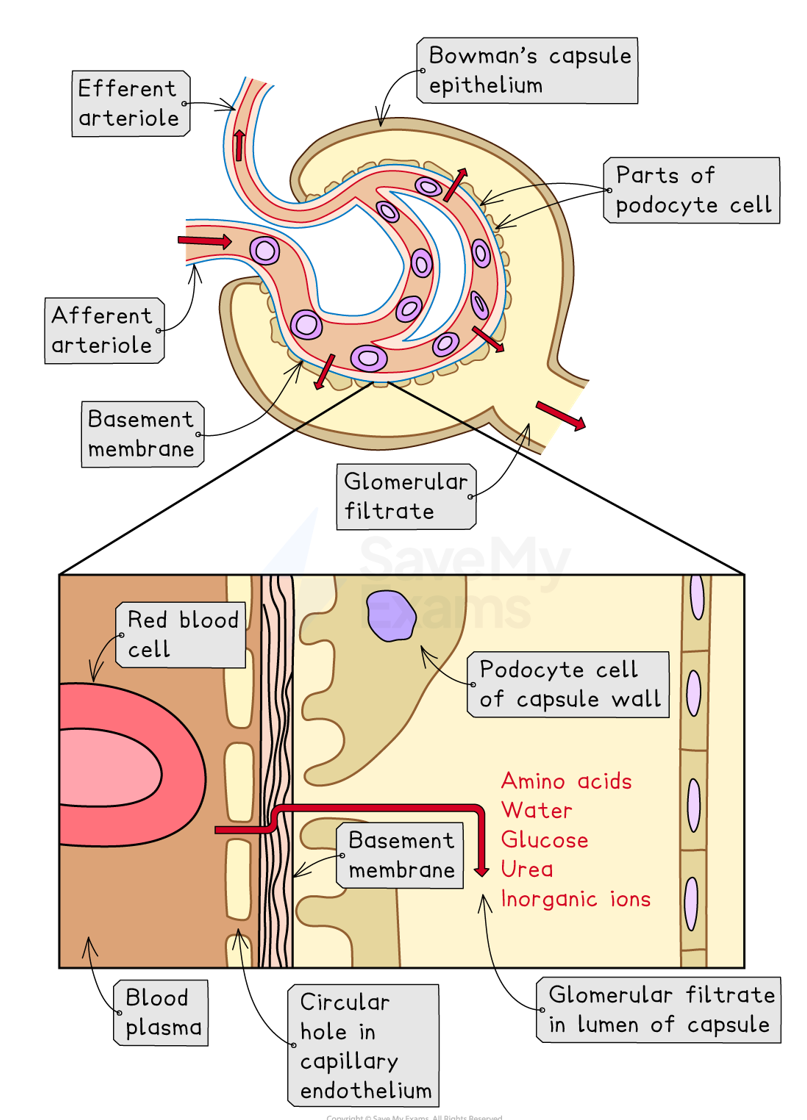
Outline the process of ultrafiltration
Arterioles branch off the renal artery & lead to each nephron, where they form the glomerulus, which sits inside the Bowman’s capsule
Blood is filtered at the glomerulus under high hydrostatic pressure from the renal artery (afferent arteriole is wider in diameter than efferent arteriole)
This causes small molecules carried in the blood to be forced out of the capillaries of the glomerulus & into the Bowman’s capsule, forming glomerular filtrate (e.g. amino acids, water, glucose, urea, ions)
Red/white blood cells & large proteins remain in the blood, as they are too big to be filtered through the capillaries
Small molecules must pass through fenestrations between endothelial cells of the capillary wall, the basement membrane & then gaps between podocytes to enter the Bowman’s capsule
What are the features that aid ultrafiltration?
The blood in the glomerular capillaries is separated from the lumen of the Bowman’s capsule by two cell layers & a basement membrane:
capillary endothelium → fenestrations between the endothelial cells allow small molecules to pass through
basement membrane → mesh of collagen & glycoproteins allows passage of small molecules
Bowman’s capsule endothelium → many podocytes (finger-like projections) between which there are gaps for small molecules to pass through
What is selective reabsorption?
The process whereby useful substances from the glomerular filtrate are taken back from the kidney tubules & put back into the blood
What substances are partially, completely & not at all reabsorbed during selective reabsorption?
Partially reabsorbed: water & mineral ions (salts)
Completely reabsorbed: glucose & amino acids
Not at all reabsorbed: urea
Where does selective reabsorption occur?
In the proximal convoluted tubule
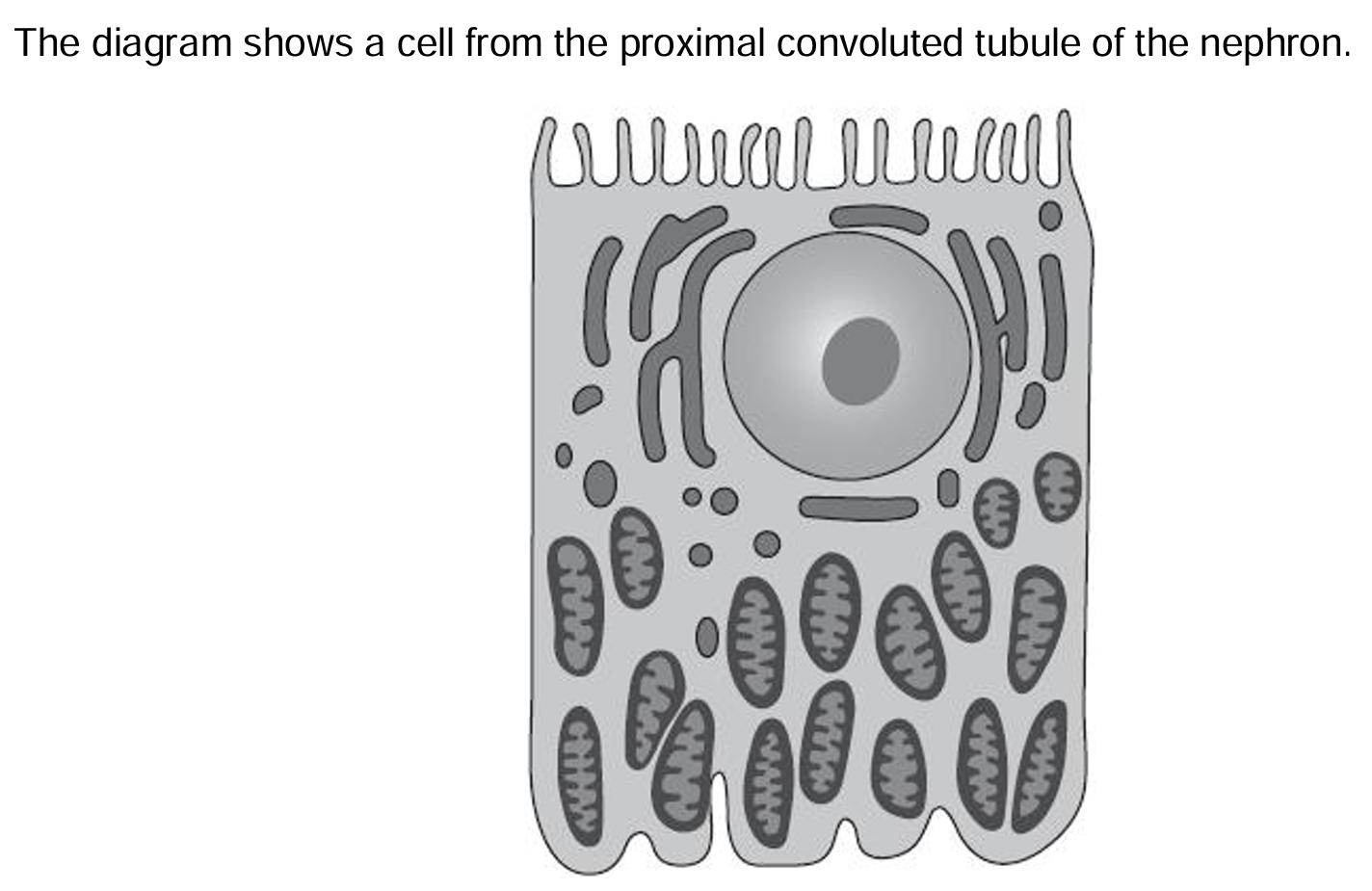
Explain how the features shown in the diagram enable this cell to carry out its function
Large numbers of mitochondria to provide ATP for active uptake of glucose, salts & amino acids
Microvilli provide a large surface area for many carrier proteins for glucose, salts & amino acids
Outline the mechanism for selective reabsorption
Na+ ions are actively transported out of the epithelial cells lining the proximal convoluted tubule into the capillaries which carry them away, using a Na+/K+ pump
This lowers the Na+ ion concentration inside the epithelial cells, creating a concentration gradient between the proximal convoluted tubule lumen & the epithelial cell
Na+ ions now diffuse down their concentration gradient from the lumen of the proximal convoluted tubule into the epithelial cells through carrier proteins by facilitated diffusion
As they do so, they bring a molecule of glucose/amino acid with it (co-transport)
Glucose/amino acid then diffuses from the epithelial cells into the blood by facilitated diffusion, through a carrier protein
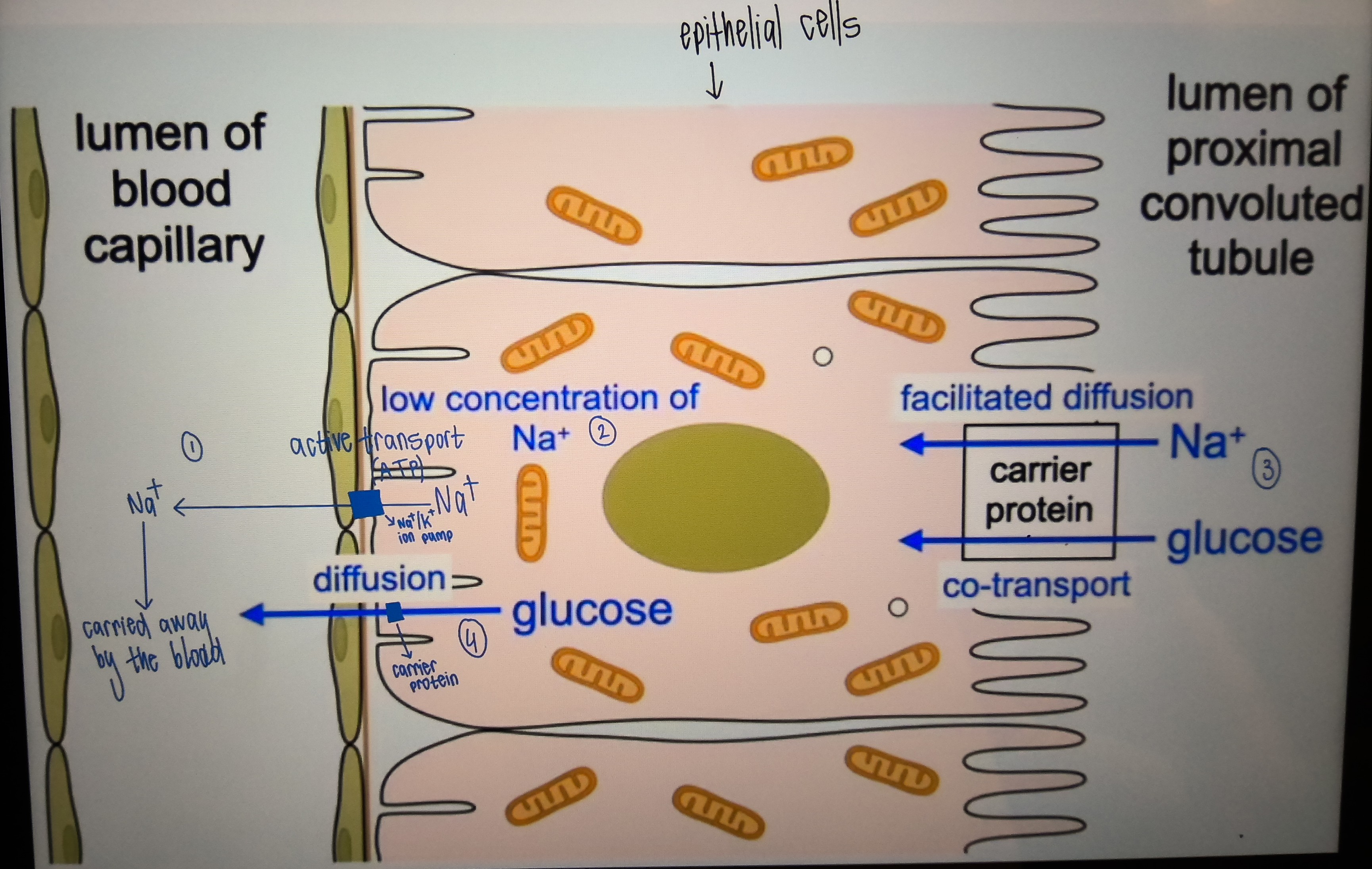
What type of active transport does glucose use to go into the capillaries?
Indirect active transport: glucose uses the concentration gradient of Na+ ions to get into the blood, instead of ATP
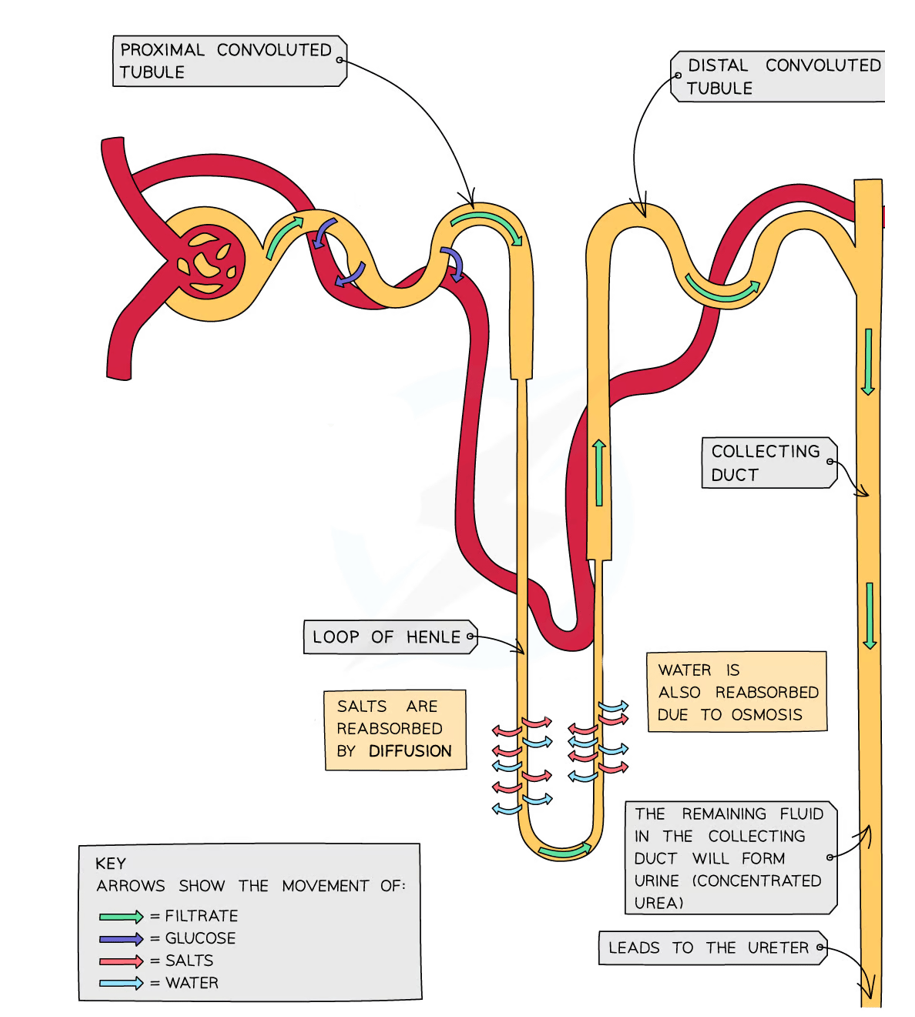
What is the job of the loop of Henle & how does it do this?
Concentrate the urine by lowering the water potential in the medulla:
makes the medulla a ‘salt bath’ using a counter-current multiplier
fluid is moving in opposite directions in the limbs & the efficiency of ion transfer out of fluid in the ascending limb is amplified by the transfer of water out of the fluid in the descending limb
as the fluid moves down the collecting duct, water moves from the fluid into the medulla by osmosis, which is then reabsorbed back into the blood
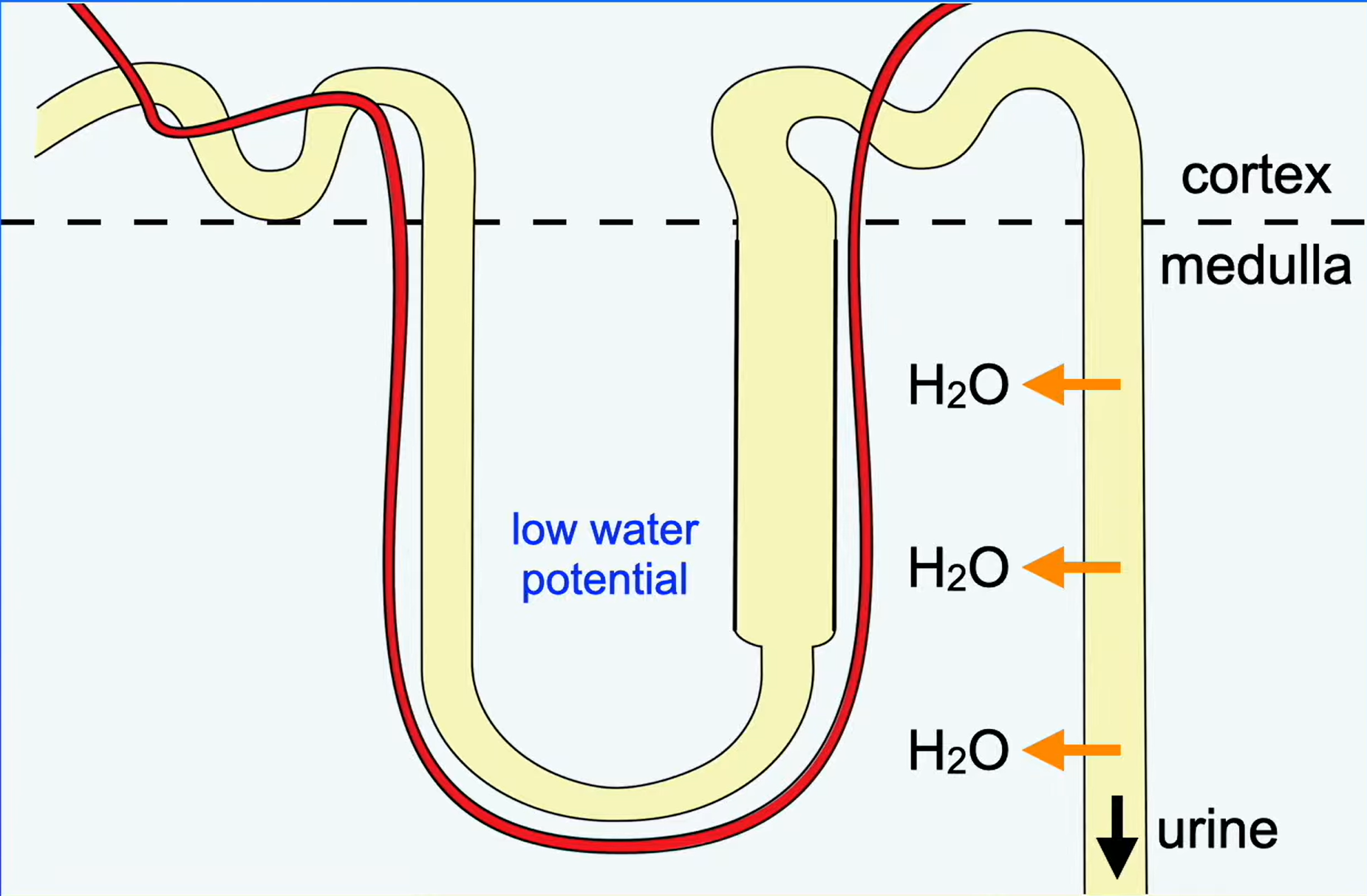
What issue is there involving the fluid at the end of the proximal convoluted tubule?
It has the same water potential as the blood:
if this fluid was released as urine, we would produce large volumes of dilute urine, which is lethal
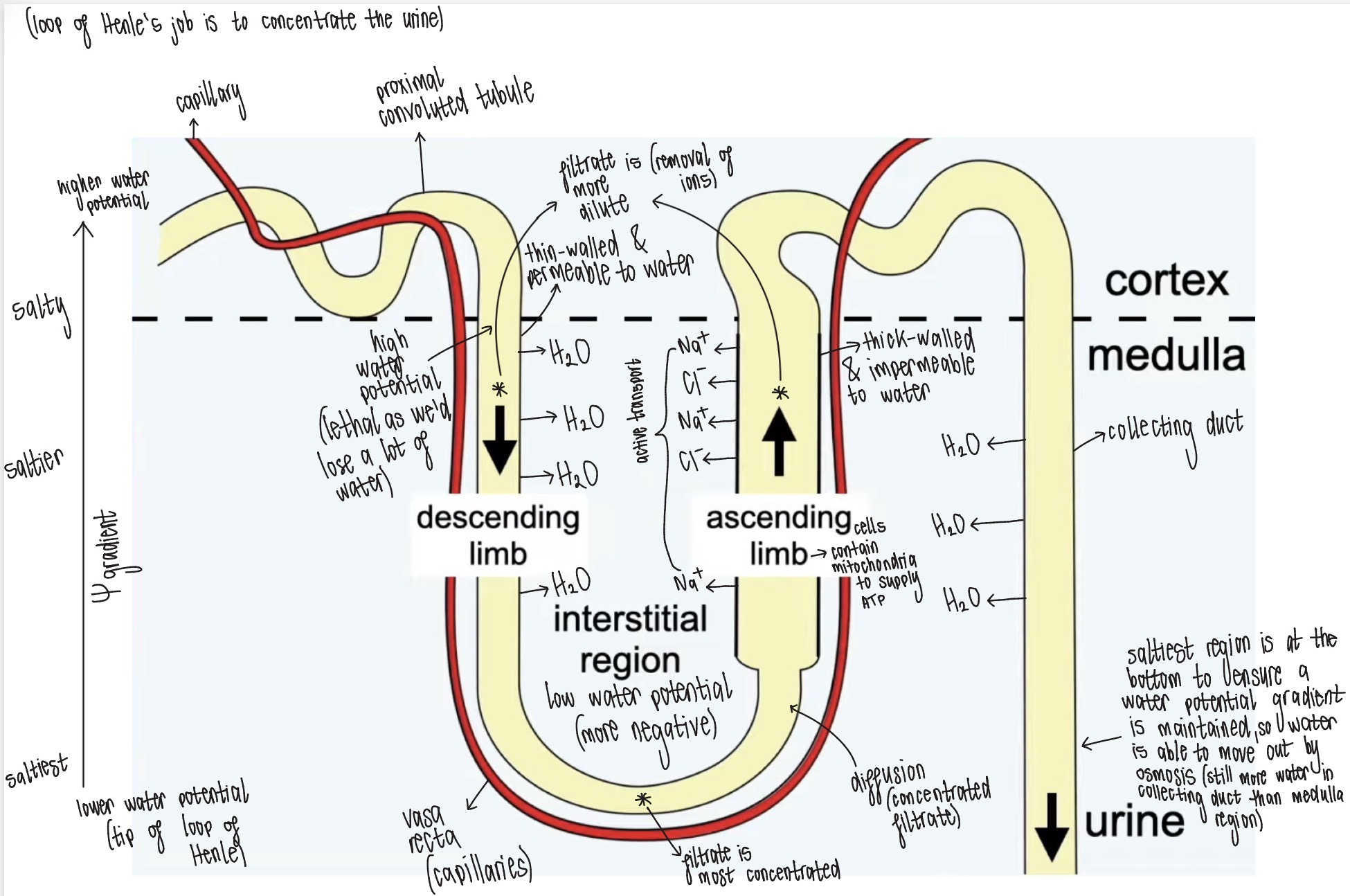
Outline the mechanism for the reabsorption of water
(loop of Henle acts as a counter-current multiplier)
As the fluid moves up the ascending limb, Na+ & Cl- ions are actively transported into the interstitial region (ATP for energy is provided by mitochondria in ascending limb cells)
The walls of the ascending limb are impermeable to water but permeable to ions, so water cannot leave the fluid in the ascending limb
There is now a high concentration of Na+ & Cl- ions in the interstitial region, meaning the medulla has a very low water potential
Fluid at the start of the proximal convoluted tubule has the same water potential as the blood. However, the descending limb walls are permeable to water but impermeable to ions
As the descending limb passes down into the medulla with a decreasing water potential gradient, water moves out of the fluid, into the medulla by osmosis
Water then moves by osmosis into the blood by the vasa recta (capillaries) & is carried away
As fluid moves down descending limb, it loses water & becomes progressively more concentrated, due to a decreasing water potential gradient
When this concentrated fluid starts moving up the ascending limb, the concentration is so high, that Na+ & Cl- ions move out of the fluid by diffusion
Further up the ascending limb, active transport takes over, pumping Na+ & Cl- ions out of the fluid
What is osmoregulation?
The homeostatic control of the water potential of body fluids (kept within narrow limits by controlling the water & salt concentrations)
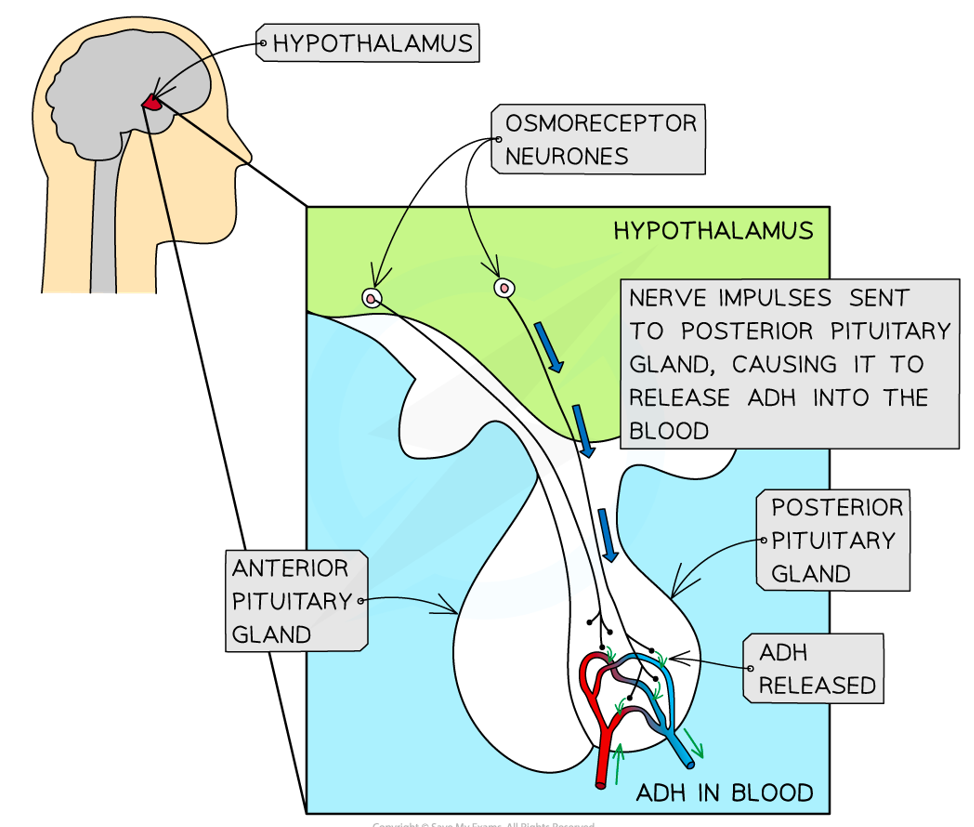
The concentration of urine is the most important in osmoregulation. What is this controlled by?
A negative feedback mechanism involving ADH (antidiuretic hormone → ‘anti-wee’):
produced in the hypothalamus & stored in the posterior lobe of the pituitary gland before being released
increases the permeability of the distal convoluted tubule & collecting duct → more water is reabsorbed from kidney tubules into the blood
Outline the negative feedback mechanism involving ADH when there is too much water in blood
Normal water potential of the blood
The blood becomes more dilute, meaning a higher water potential
This change is detected by osmoreceptors in the hypothalamus
The posterior pituitary gland releases less ADH
The distal convoluted tubule & collecting duct become less permeable to water, due to fewer aquaporins
Less water is reabsorbed & large volumes of dilute urine is produced
Outline the negative feedback mechanism involving ADH when there is too little water in the blood
Normal water potential of the blood
The blood becomes more concentrated (lower water potential)
This change is detected by the osmoreceptors in the hypothalamus
The posterior lobe of the pituitary gland releases more ADH
The distal convoluted tubule & collecting duct become more permeable to water, due to more aquaporins
More water is reabsorbed & small volumes of concentrated urine is produced
Outline the mechanism of ADH action
ADH travels through the bloodstream & binds to specific complementary receptor proteins on the surface of the cells of the distal convoluted tubule & collecting duct
This activates a signalling cascade that results in the production of cAMP as a second messenger
cAMP triggers vesicles within the cells to move to & fuse with the luminal membranes
The vesicles contain many aquaporins (water-permeable channels), which are inserted into the luminal membranes, increasing the permeability of the cells to water
Water molecules can then move by osmosis into the medulla & be carried away in the bloodstream
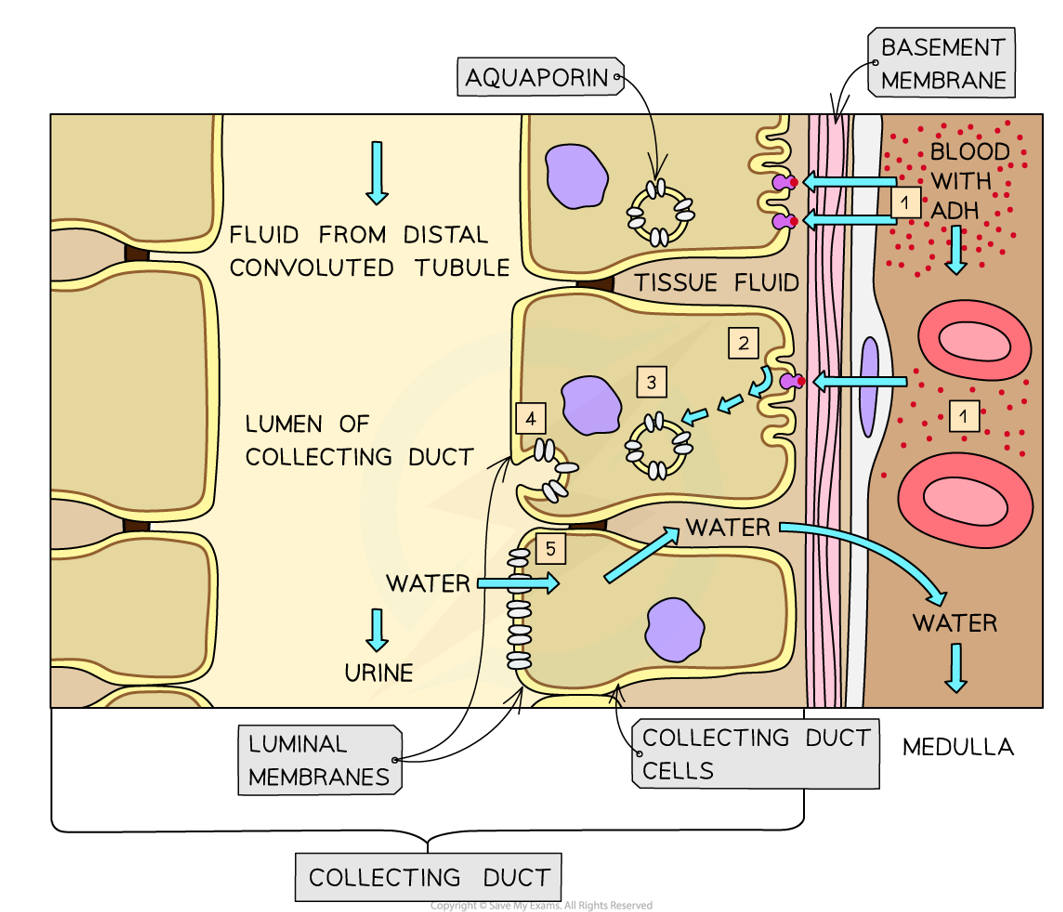
What happens when ADH & cAMP levels fall?
The aquaporins are withdrawn from the membranes & re-packaged into vesicles (stored ready for re-use when needed)
How is the release of ADH also stimulated or inhibited by changes in blood pressure?
More water in the blood means a higher blood pressure, which is detected by the baroreceptors in the aorta & carotid arteries
The release of ADH is inhibited, meaning less water is reabsorbed & more urine is released
What are the adaptations of a kangaroo rat for life in a dry environment?
They live in cool, stable burrows underground
They obtain 90% of water from metabolic, condensation reactions & 10% from food (e.g. seeds)
They forage at night to reduce water loss & avoid predators
They lack sweat glands& don’t pant
They produce highly concentrated urine, due to long loops of Henle
Their kidney tubule cells have many microvilli for increased reabsorption (larger surface area)
Their kidney cells contain many mitochondria to provide ATP for active transport

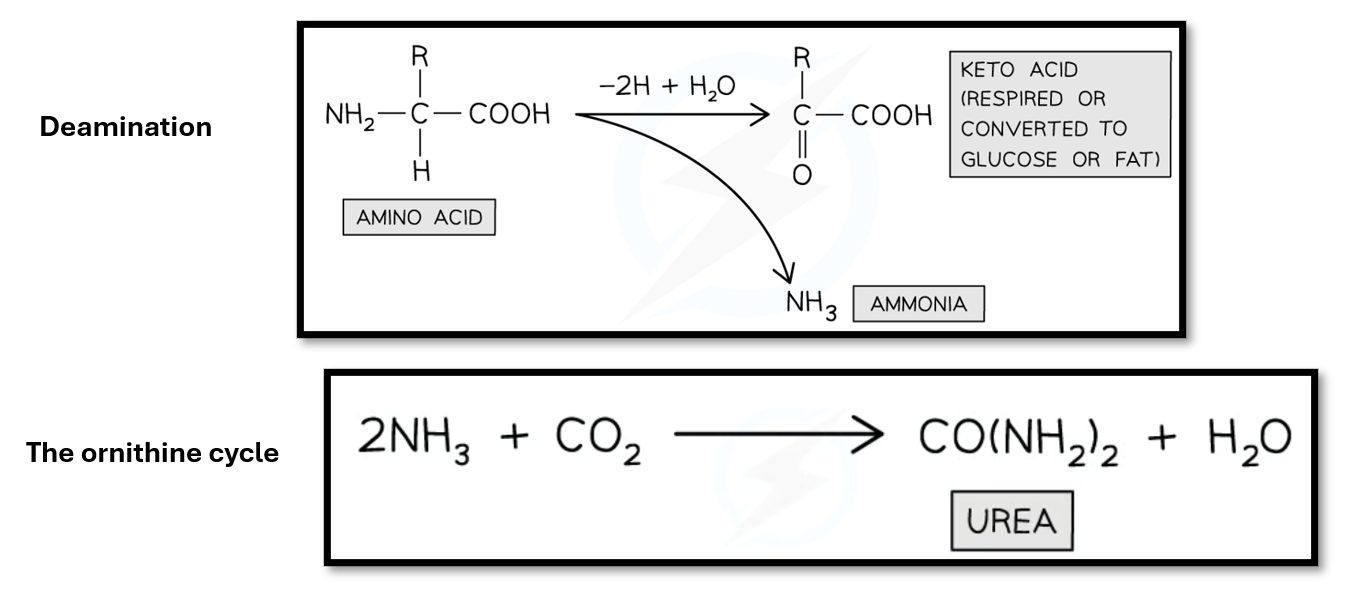
Outline how urea is produced in mammals
Ammonia is produced when amino acids undergo deamination in the liver, which removes the amino group
Ammonia is harmful & needs to be converted into a less toxic form, so it combines with carbon dioxide in the ornithine cycle to form urea
Urea is transported in the blood to the kidneys, where it is excreted in urine