Lecture 5 - Extraocular Muscles
1/47
Earn XP
Description and Tags
Ocular Anatomy
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
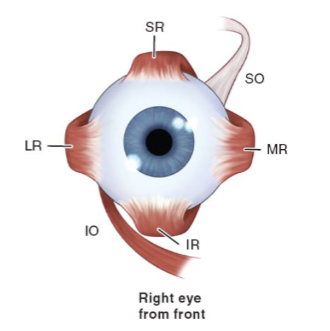
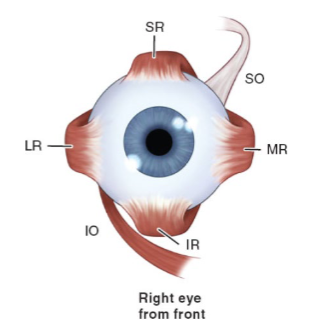
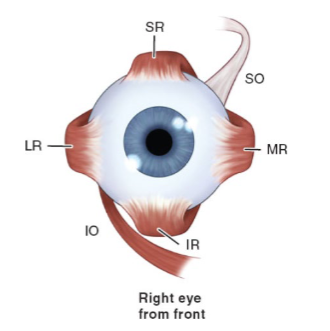
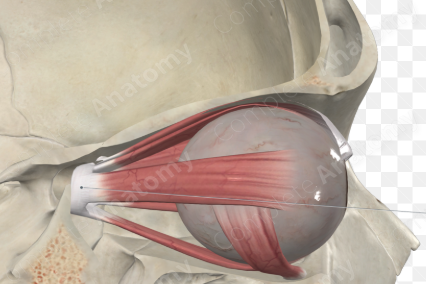
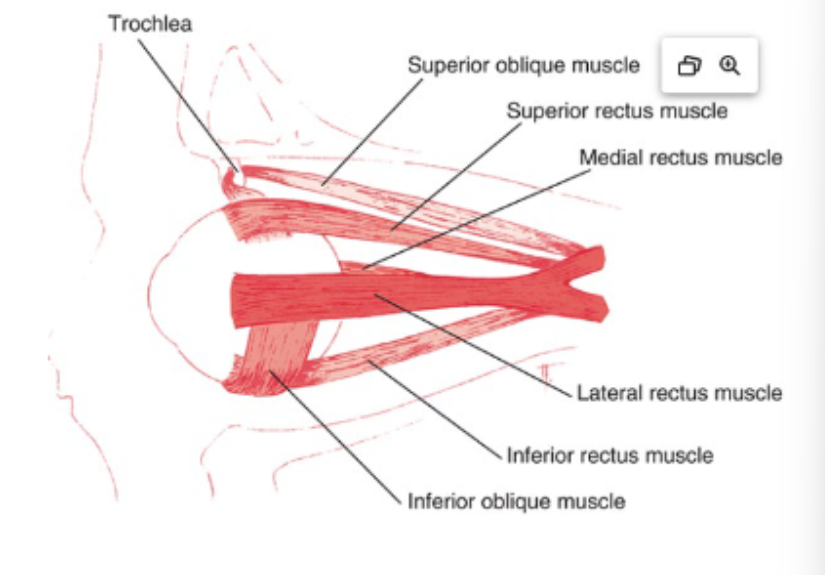
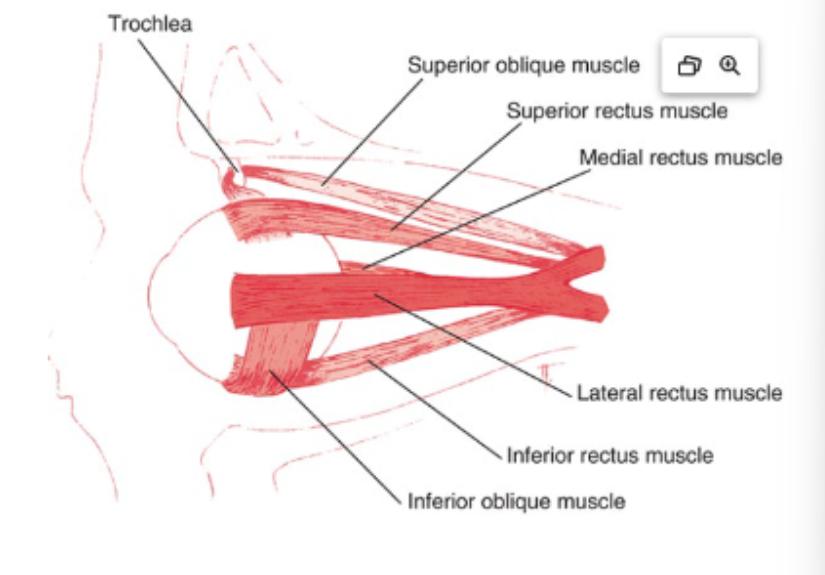
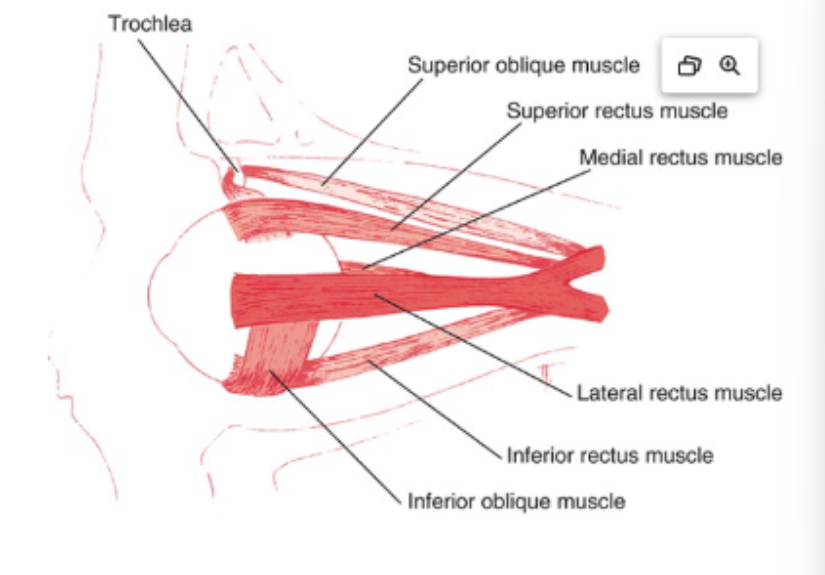
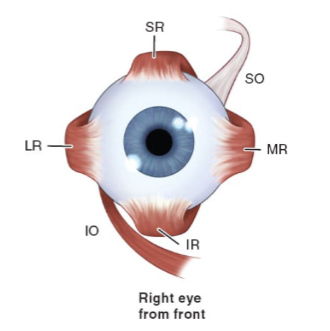
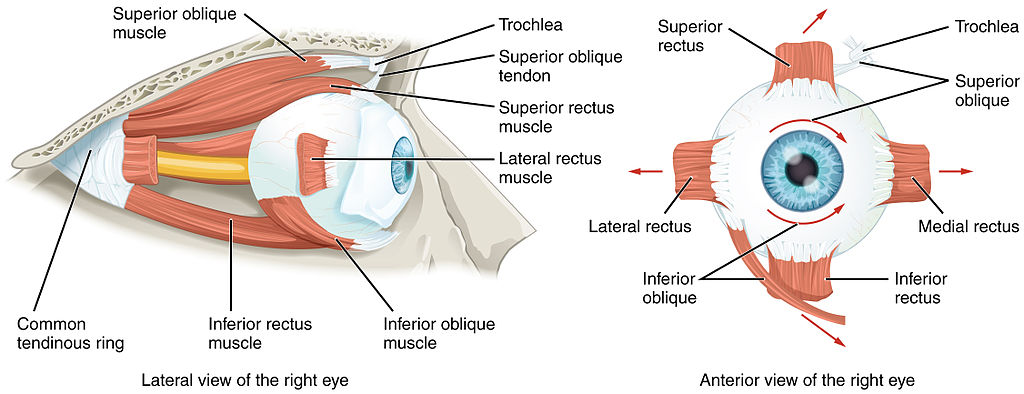
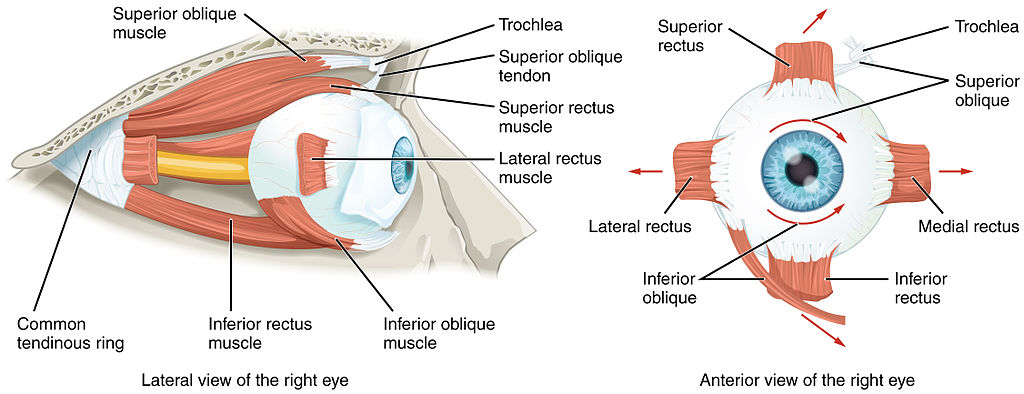
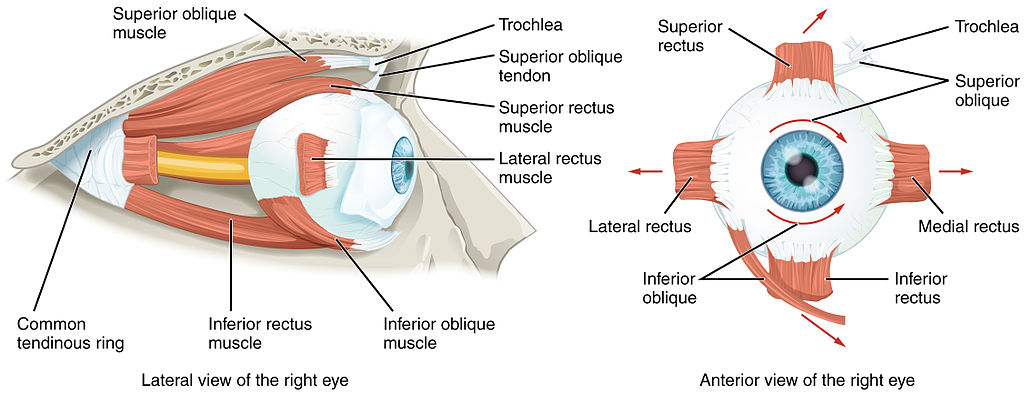
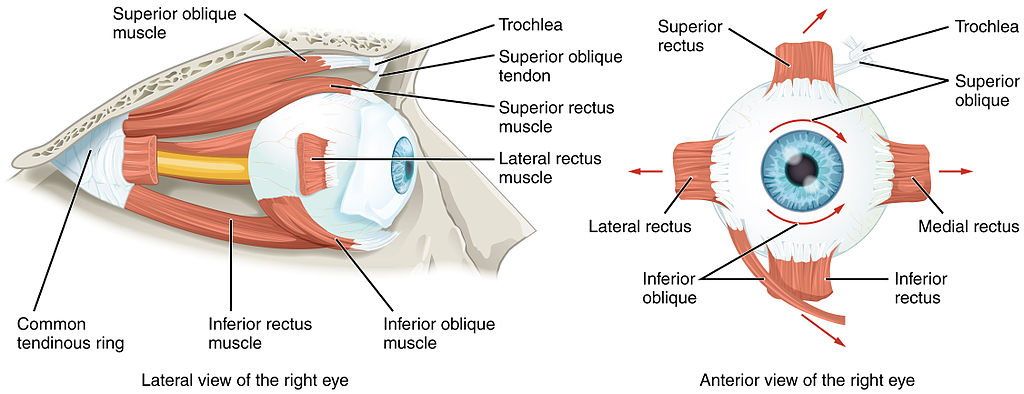
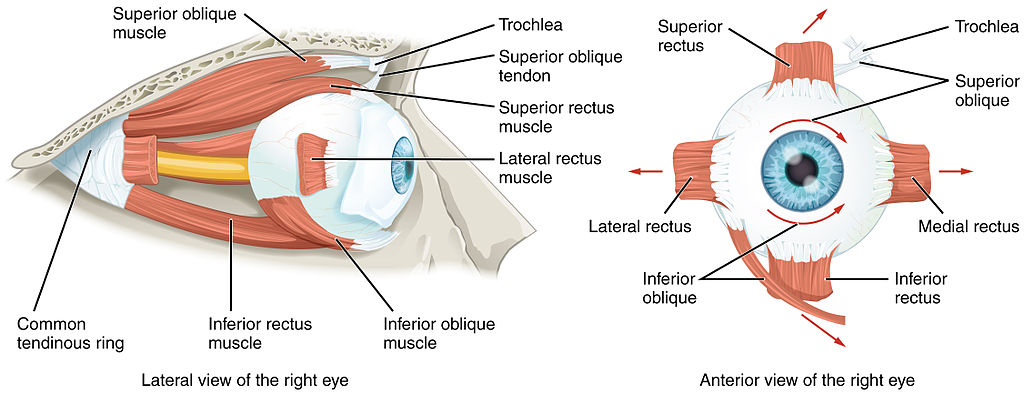
How many extraocular muscles are there, and what are they?
Six: superior rectus, inferior rectus, medial rectus, lateral rectus, superior oblique, inferior oblique.
What do EOMs attach to and control?
They attach to the sclera and control globe movement.
What are the rectus muscles from longest to shortest?
Superior → medial → lateral → inferior.
“SMeLI”
What structural features make EOMs unique compared to other skeletal muscle?
Dense blood supply
Delicate connective tissue sheaths rich in elastic fibers
Dense innervation for precise fine motor control
Among fastest and most fatigue-resistant striated muscle
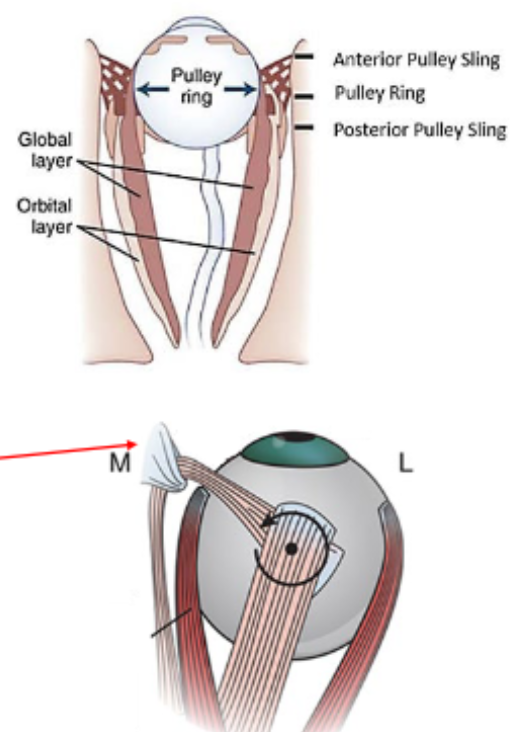
What are EOM pulleys and their function?
Rings of dense collagen (2 mm in length) with smooth muscle-connective tissue struts that anchor to periorbita.
They act as functional origins, refining coordination of binocular movements and redirecting muscle pull.
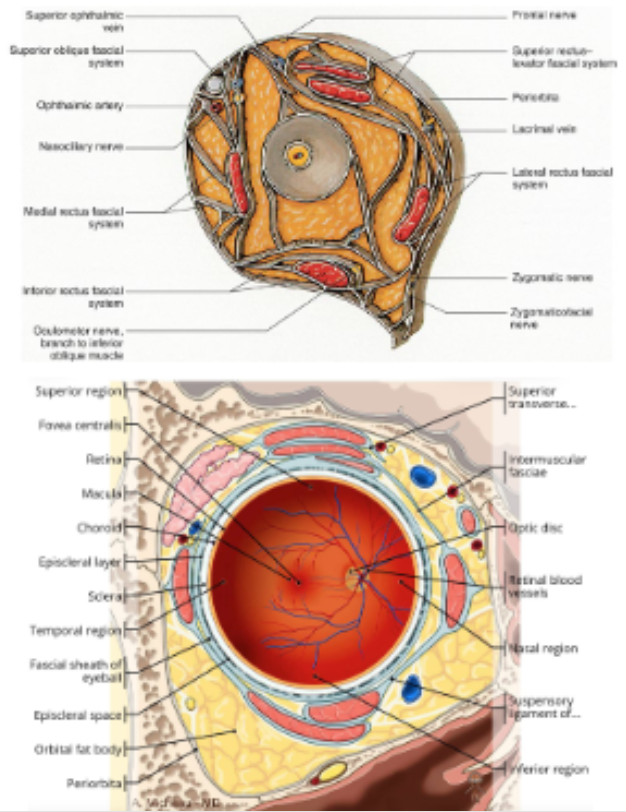
What does orbital connective tissue provide?
A dense supportive framework, stabilizing muscle paths and limiting eye movement.
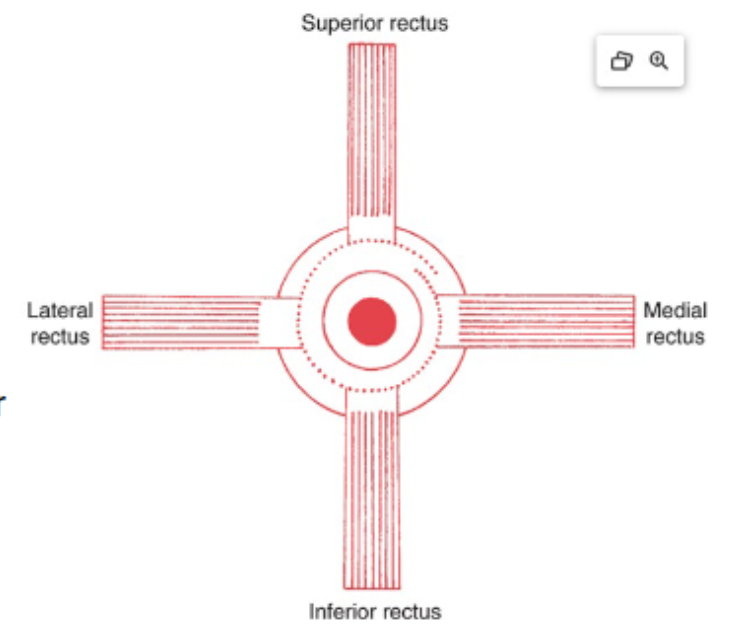
What is the common origin of the rectus muscles?
The common tendinous ring (annulus of Zinn) at the orbital apex, continuous with periorbita.
Which rectus muscles originate from both upper & lower parts of the ring?
Medial rectus and lateral rectus.
Which muscles originate from the upper limb only?
Superior rectus.
Which muscles originate from the lower limb only?
Inferior rectus.
Which recti are also attached to the dural sheath of the optic nerve?
Medial rectus and superior rectus.
Where do the four rectus muscles insert relative to the equator of the globe?
Anterior to the equator.
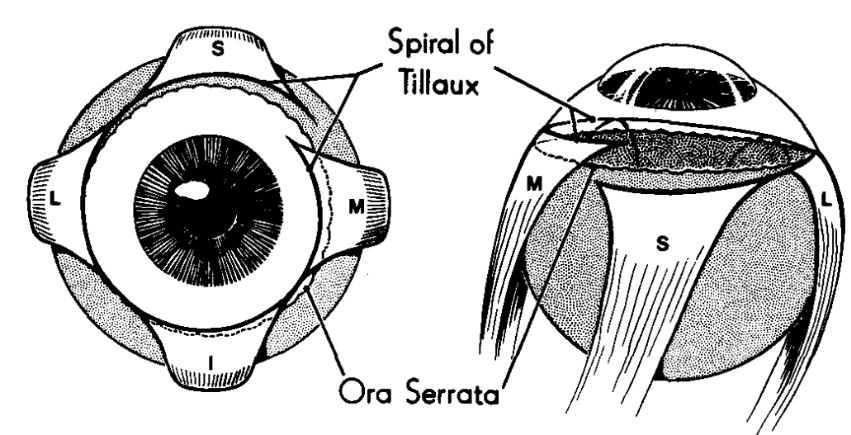
What line connects the rectus muscle insertions?
Spiral of Tillaux.
Order of recti insertions from closest to furthest from limbus?
Medial (5.5 mm) → Inferior (6.5 mm) → Lateral (6.6 mm) → Superior (7.7 mm).
Mnemonic: MILS.
Medial Rectus (MR):
Largest EOM
Origin: Upper & lower parts of tendinous ring + optic nerve sheath
Insertion: ~5.5 mm from limbus
Innervation: Inferior division of CN III
Lateral Rectus (LR):
Origin: Upper & lower tendinous ring + spina recti lateralis (sphenoid)
Insertion: ~6.6 mm from limbus
Innervation: CN VI (abducens)
Superior Rectus (SR):
Origin: Upper tendinous ring + optic nerve sheath
Connections with levator sheath coordinate eyelid & globe movement
Innervation: Superior division of CN III
Inferior Rectus (IR):
Origin: Lower tendinous ring
Connections with lower lid (tarsal plate) → lid lowering with down gaze
Innervation: Inferior division of CN III
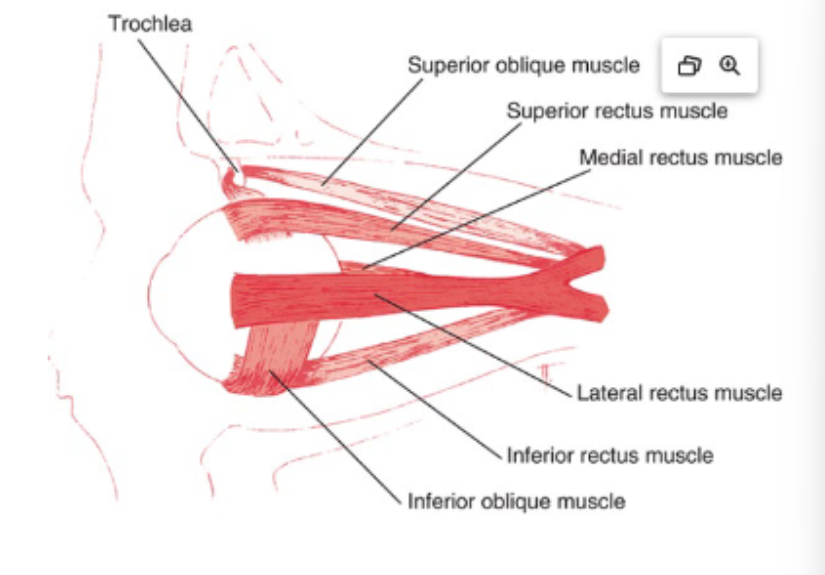
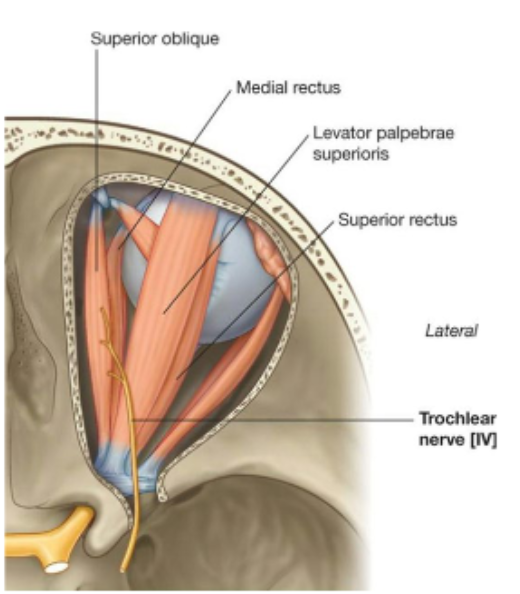
Superior Oblique (SO):
Longest & thinnest EOM
Origin: Lesser wing of sphenoid → passes through trochlea (pulley)
Trochlea = functional origin
Innervation: CN IV (trochlear)
Inferior Oblique (IO):
Only EOM with anterior orbital origin (maxillary bone)
Runs parallel to SO
Innervation: Inferior division of CN III
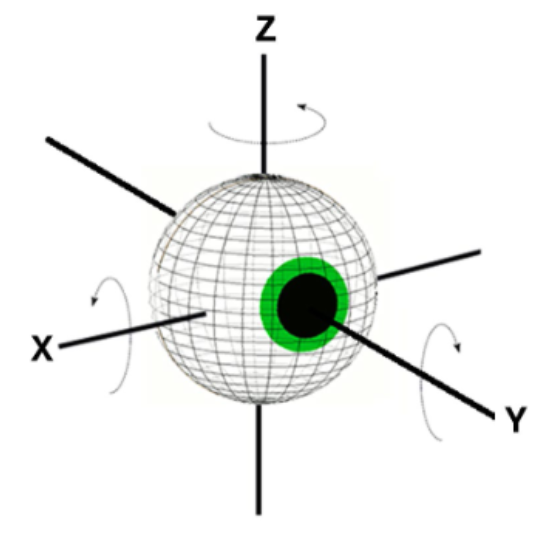
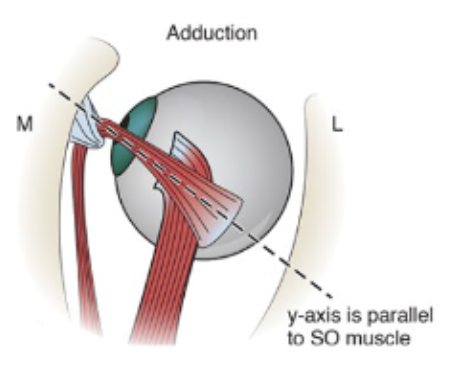
What are Fick’s Axes for eye movement?
X-axis (horizontal): center of cornea moves up/down
Runs nasal to temporal
(supraduction, infraduction)
Y-axis (sagittal): torsion (intorsion, extorsion)
Z-axis (vertical): cornea moves left/right (adduction, abduction
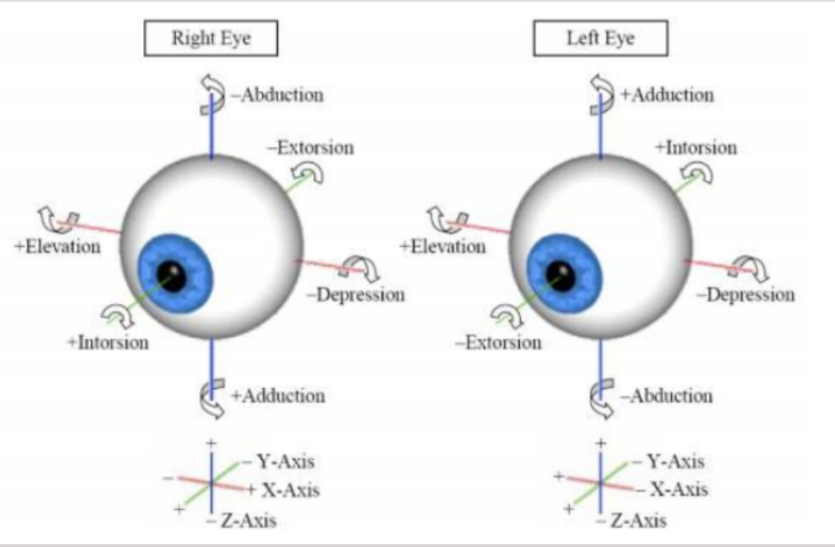
What are the types of eye movements?
Ductions (one eye): adduction, abduction, elevation, depression, intorsion, extorsion
Vergences (both eyes opposite): convergence (adduct), divergence (abduct)
Versions (both eyes same): conjugate movements
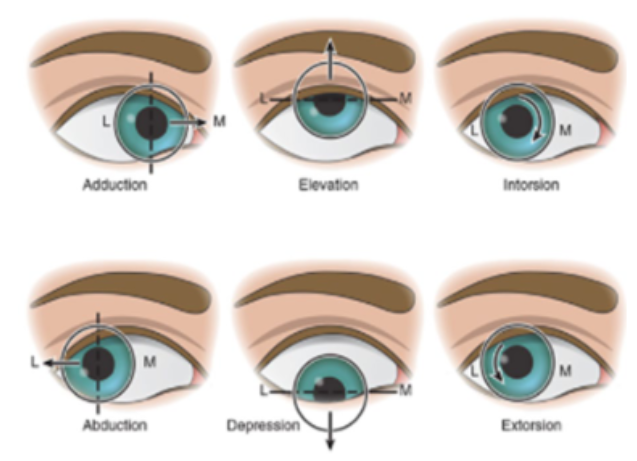
What are the duction movements?
Movements involving one eye
Rotation around vertical z-axis
adduction
abduction
Rotation around horizontal x-axis
supraduction
infraduction
Rotation around sagittal y-axis
intorsion
extorsion
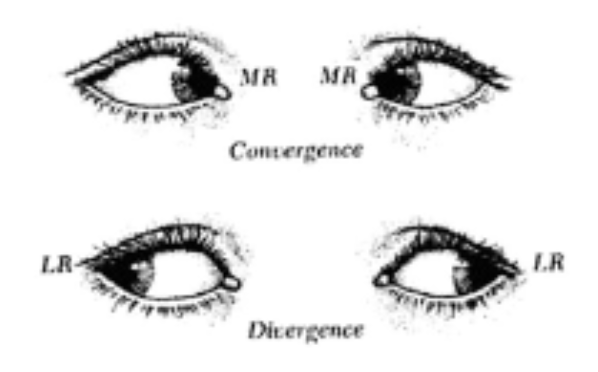
What are the vergences and versions movements?
Movements involving both eyes
Version = eyes move in same direction
Vergence = eyes move in opposite directions
Convergence = both eyes adduct
Divergence = both eyes abduct
What are the positions of gaze?
Primary = eyes straight ahead with head erect
Secondary = Rotation around vertical or horizontal axis
Eyes up/down/left/right
Tertiary = Rotations around both vertical and horizontal axes
Eyes in oblique positions
What are the primary actions of the EOMs (from primary position)?
MR: adduction
LR: abduction
SR: elevation (secondary: adduction, intorsion)
IR: depression (secondary: adduction, extorsion)
SO: intorsion (secondary: depression, abduction)
IO: extorsion (secondary: elevation, abduction)
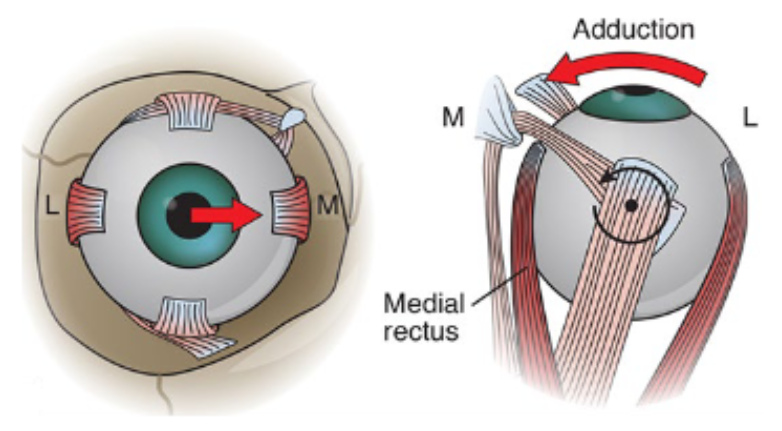
What are the movements from primary position of the medial rectus?
Adduction
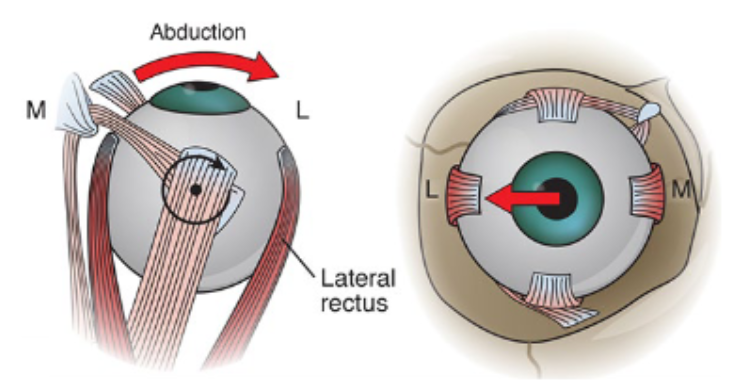
What are the movements from primary position of the lateral rectus?
Abduction
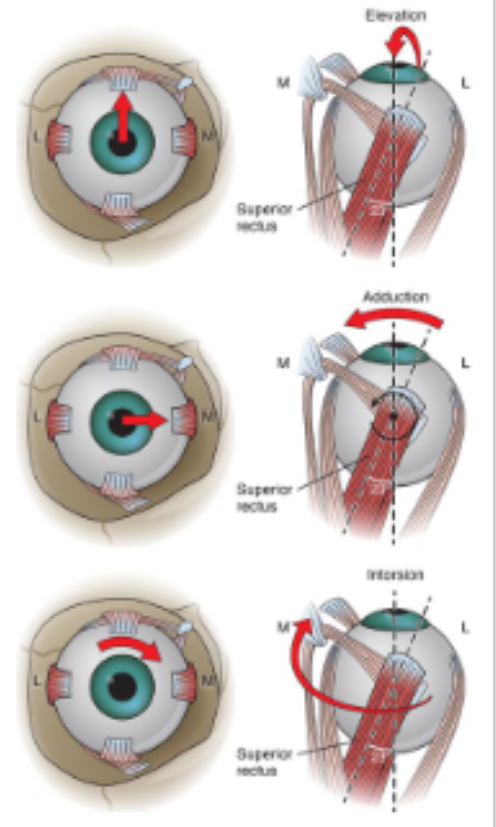
What are the movements from primary position of the superior rectus?
Primary action: elevation
Secondary actions: adduction, intorsion
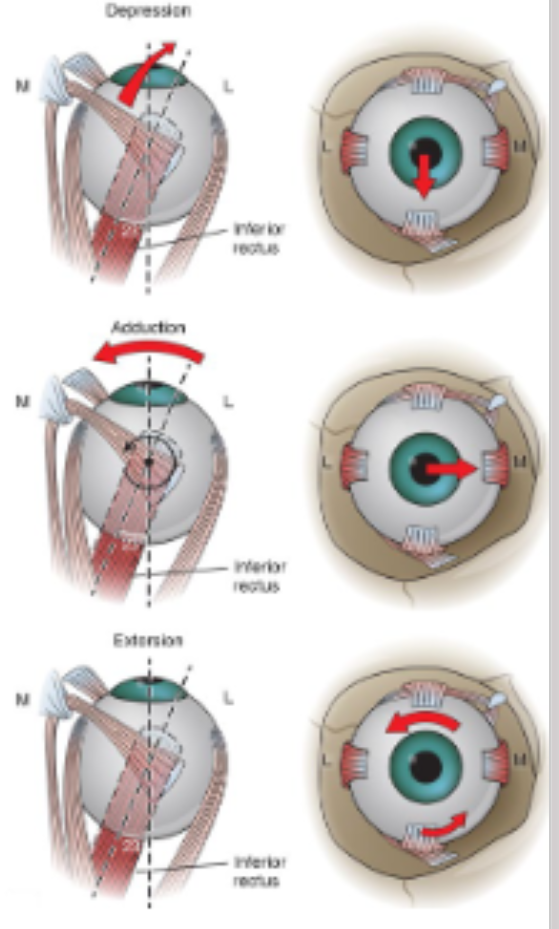
What are the movements from primary position of the inferior rectus?
Primary action: depression
Secondary actions: adduction, extorsion
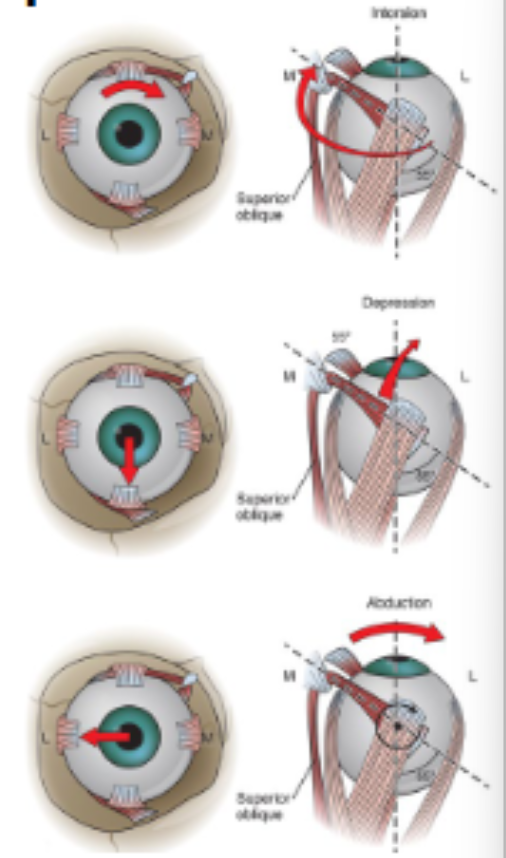
What are the movements from primary position of the superior oblique?
Primary action: Intorsion
Secondary actions: Depression, abduction
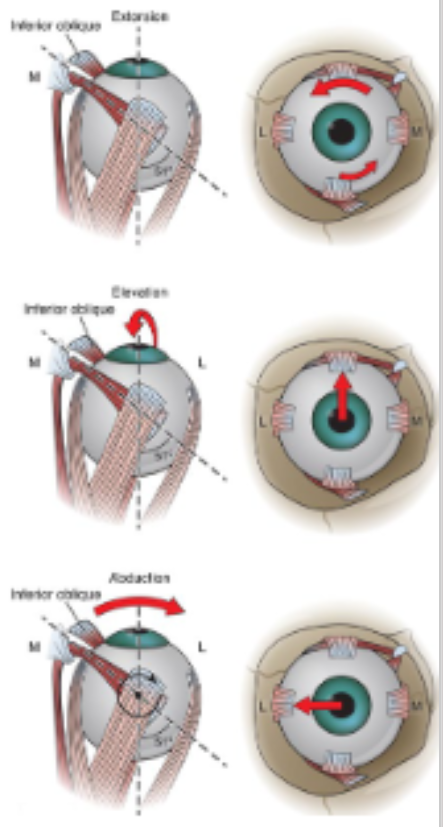
What are the movements from primary position of the inferior oblique?
Primary action: extorsion
Secondary actions: elevation, abduction
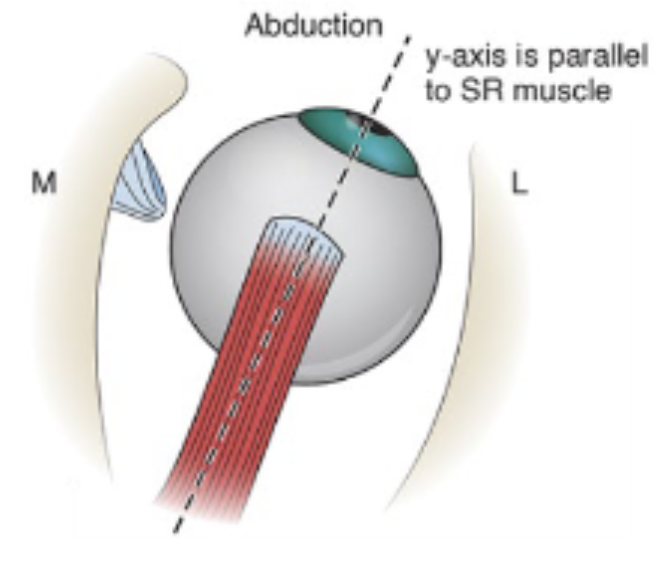
Movements from secondary position of the vertical rectus muscles — eye is abducted 23 degrees from primary position
Vertical rectus muscles parallel the y-axis
Perpendicular to x-axis
Only vertical movement occurs
Superior rectus will only elevate
Inferior rectus will only depress
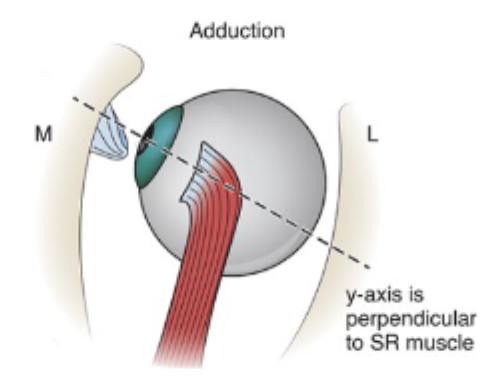
Movements from secondary position of the vertical rectus muscles — eye is abducted 67 degrees from primary position
Vertical rectus muscles parallel the x-axis
Perpendicular to y-axis
Only torsional movement occurs
Superior rectus will only intort
Inferior rectus will only extort
Movements from secondary position of the oblique muscles — eye is abducted 51-55 degrees from primary position
Oblique muscles parallel to y-axis
Perpendicular to x-axis
Only vertical movement occurs
Superior oblique will only depress
Inferior oblique will only elevate
Movements from secondary position of the oblique muscles — eye is abducted 35-39 degrees from primary position
Oblique muscles parallel to x-axis
Perpendicular to y-axis
Only vertical movement occurs
Superior oblique will only intort
Inferior oblique will only extort
What are the muscle actions in secondary positions?
Vertical recti (SR, IR):
Eye abducted 23° → pure vertical (SR elevates, IR depresses)
Eye adducted 67° → pure torsion (SR intorts, IR extorts)
Oblique muscles (SO, IO):
Eye adducted 51–55° → pure vertical (SO depresses, IO elevates)
Eye abducted 35–39° → pure torsion (SO intorts, IO extorts)
What is Sherrington’s Law?
Contraction of a muscle → proportional relaxation of antagonist
Examples:
Adduction: MR contracts, LR relaxes
Elevation: SR contracts, IR relaxes
What are the antagonist pairs?
SR/IR
MR/LR
SO/IO
What are the agonist pairs (synergists)?
Elevation = SR + IO
Depression = IR + SO
Intorsion = SR + SO
Extorsion = IR + IO
What are yoke muscles?
Muscles in opposite eyes that act together for binocular movement, receiving equal and simultaneous innervation.
Left gaze = Left LR + Right MR
Right gaze = Right LR + Left MR
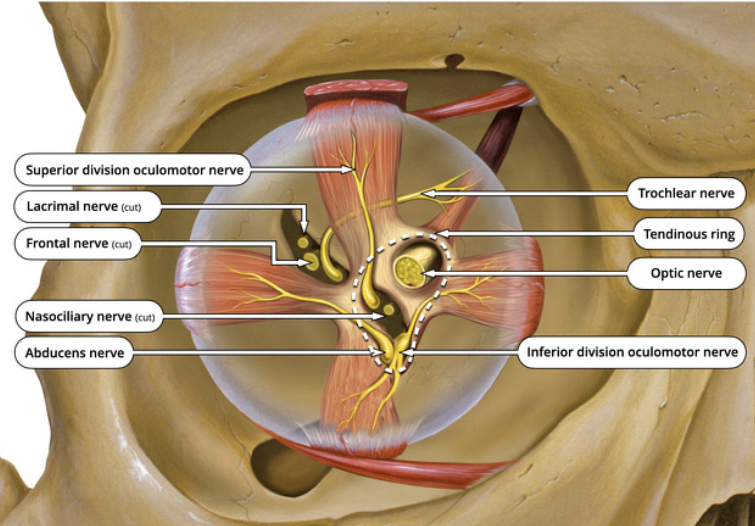
Summary of EOM innervation
CN III (oculomotor):
Superior division: SR
Inferior division: MR, IR, IO + parasympathetic to ciliary ganglion
CN IV (trochlear): SO
CN VI (abducens): LR
LR6(SO4)3
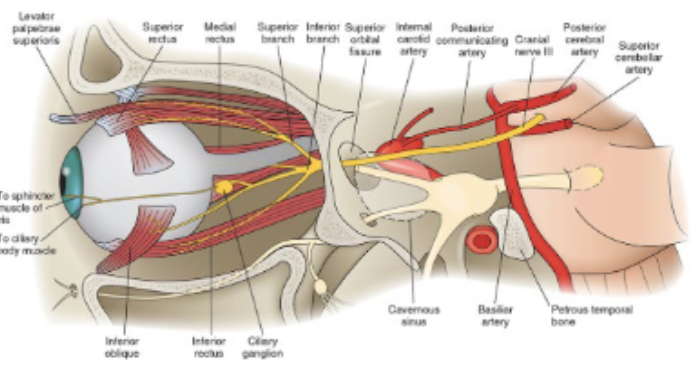
What is the pathway of CN III (Oculomotor)?
Nucleus in midbrain (motor + parasympathetic)
Fibers pass between posterior cerebral artery & superior cerebellar artery
Goes through cavernous sinus
Divides into superior & inferior branches
Superior orbital fissure (through CTR)
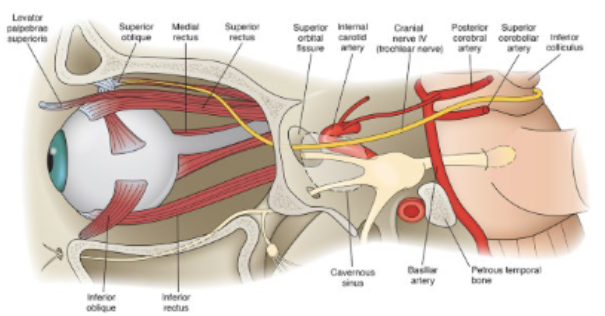
What is the pathway of CN IV (Trochlear)?
Nucleus in midbrain below CN III
Only cranial nerve exiting dorsally; decussates before orbit
Travels with frontal nerve, enters orbit above CTR → innervates SO
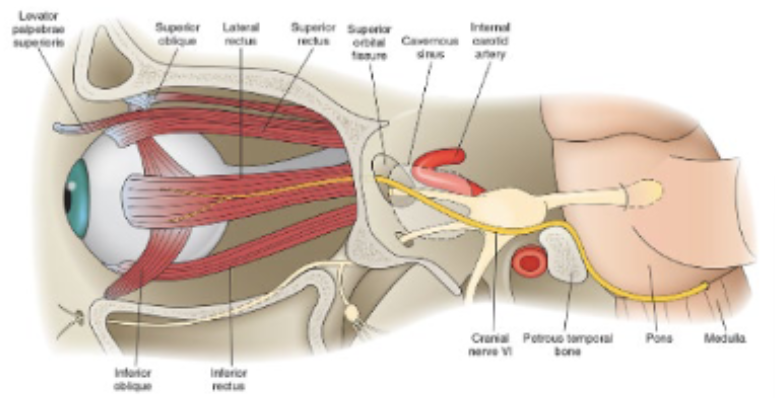
What is the pathway of CN VI (Abducens)?
Nucleus in pons
Long tortuous course: exits pontomedullary junction → over petrous ridge → cavernous sinus (next to ICA) → enters orbit via superior orbital fissure within CTR → LR
What do the branches of the ophthalmic artery supply?
Lateral muscular branch: SR, LR, SO
Medial muscular branch: IR, MR, IO
What aging changes occur with EOM?
MR & LR displaced inferiorly (MR > LR) → impaired elevation
Greater muscle fiber size variability
Increased connective tissue & fat
General degenerative changes
What is Hering’s Law?
Synergist muscles in opposite eyes will receive equal and simultanious innervation for vergence movements.
Ex: right MR and left LR work together to produce right gaze.
“Schools of herings swim together”