test 4
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
afterload
Resistance heart must overcome to eject blood.
RT: pulmonic resistance
LT: systemic resistance
preload
degree of stretch of the cardiac muscle fibers at the end of diastole
cardiac output
Volume of blood pumped by heart per minute.
4-6 L a minute
ejection fraction
percentage of blood ejected out with each beat
inotropy
force of myocardial contraction
chronotropy
heart rate
stroke volume
The amount of blood ejected from the left ventricle in one contractio, measured in mL
coronary artery disease
narrowing or obstruction of one or more coronary arteries, results from atherosclerosis
what labs are used to determine overall cardiovascular risk?
high-sensitivity C-reactive protein (hs-CRP) test results together with other screening tools such as measurements of lipid levels
fasting lipid profile should demonstrate what values?
LDL
TOTAL cholesterol
HDL
Triglycerides
LDL: <100 mg/dL
total: <200 mg/dL
HDL: males- >40mg/dL, females- >50 mg/dL
Triglycerides: <150 mg/dL
what kind of diet for CAD prevention
AHA/Mediterranean Diet: both provide similar key elements: an emphasis on plant foods (fruits, vegetables, whole-grain breads, beans, nuts, and seeds), minimally processed foods, seasonally fresh foods, inclusion of fish, and minimal intake of red meat
HMG-CoA reductase inhibitors also known as ________, examples, and what they do
Statins.
- Atorvastatin (Lipitor), Rosuvastatin (Crestor), Simvastatin (Zocor)
*works in the liver and prevents lipids from being produced
teachings, nursing interventions of statin meds
monitor serum liver enzymes, report unexplained muscular pain (myopathy) immediately (rhabdomyolysis-weakness, tea colored urine)
-administer in the evening, take as prescribed
-AVOID grapefruit juice
Fibric Acids (Fibrates)
-lipid lowering drug therapy
Gemfibrozil (Lopid)
-lowers triglycerides, increase HDLs (takes lipids AWAY from arteries)
-contraindicated in severe kidney and liver disease (monitor liver/kidney function)
-use cautiously when also taking statin med
Bile Acid Sequestrants
-lipid lowering
colestipol (colestid), cholestyramine (questran)
*They work inside your digestive system by binding to bile acids—which are made of cholesterol. This forces your body to flush the bile acids out in your stool, prompting your liver to pull more cholesterol from your blood to make new ones (decreasing hepatic cholesterol)
-effect GI and interfere with absorption of many drugs
PCSK-9 inhibitors
Alirocumab (Praluent), Evolocumab (Repatha)
-subcut every 2-4 weeks
lipid lowering drug
-destroys LDL receptors (responsible for pulling LDL out of the blood) PCSK9 inhibitors essentially block this protein, allowing more LDL receptors to remain active and remove excess cholesterol from your bloodstream
Cholesterol Absorption Inhibitor
Ezetimibe (Zetia)
Inhibits absorption of cholesterol in small intestine
depolarization
repolarization
Depolarization: contraction
Repolarization: relaxation
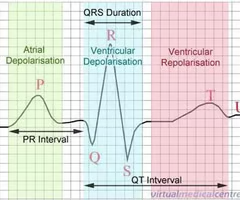
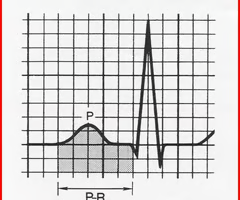
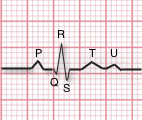
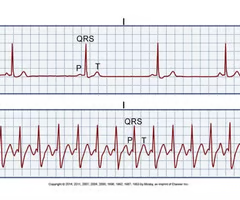
P WAVE
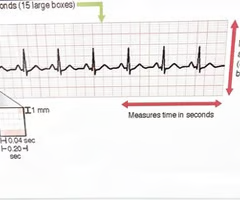
represents the electrical impulse starting in the SA node and spreading through the atria. represents atrial depolarization. It is normally 2.5 mm or less in height and 0.11 seconds or less in duration.
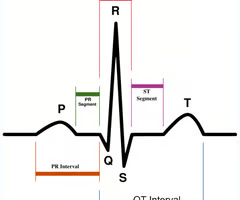
PR interval
measured from the beginning of the P wave to the beginning of the QRS complex and represents the time needed for sinus node stimulation, atrial depolarization, and conduction through the AV node before ventricular depolarization. In adults, the PR interval normally ranges from 0.12 to 0.20 seconds in duration
QRS complex
represents ventricular depolarization
0.06 to 0.12 seconds duration
QRS duration
time required for depolarization of both ventricles (0.04 TO 0.10)
ST segment
represents early ventricular repolarization, lasts from the end of the QRS complex to the beginning of the T wave
T wave
represents ventricular repolarization (when the cells regain a negative charge; also called the resting state)
U wave
thought to represent repolarization of the Purkinje fibers; although this wave is rare, it sometimes appears in patients with hypokalemia (low potassium levels), hypertension, or heart disease
QT interval
represents the total time for ventricular depolarization and repolarization, is measured from the beginning of the QRS complex to the end of the T wave
what is caused by disturbance in electrical conduction of the heart and causes can be drugs, acid base balance, electrolyte imbalance, thermal changes, disease, trauma, nicotine
arrhythmias
what assessment should you do with an arrhythmia
heart rate, apical 1 min, rhythm
with arrhythmias, patients are normally asymptomatic until what is altered and how does this present
cardiac output
-palpitations, syncope, pain, dyspnea, diaphoresis, hypotension, electrolyte imbalances
what is sinus bradycardia and how is it treated
rate of sinus node less than 60 beats per min (sinus bradycardia)
can be symptomatic or asymptomatic, can be normal in some individuals
TX: atropine (anticholinergic drug used to treat slow heart rhythms by blocking the vagus nerve's inhibitory effects on the heart. It accelerates the sinus node's pacemaking and speeds up conduction through the AV node), pacemaker, holding meds, 02, notify RN. Apply transcutaneous pacemaker pads (TCP) if atropine does NOT work
what two rhythms are the only rhythms to defibrillate
VTACH
VFIB
sinus tachycardia
rates >100 bpm
TX: depends on cause, vagal maneuver (breathing through a straw to simulate vagus nerve), valsalva maneuver (exhaling forcefully against a closed airway (pinching the nose and closing the mouth) or glottis, similar to popping your ears. This temporarily increases pressure in the chest, altering blood pressure and heart rate), adenosine, synchronized cardioversion (synched with QRS, deliver on R. if you deliver on T wave, it can cause ventricular dysrhythmia)
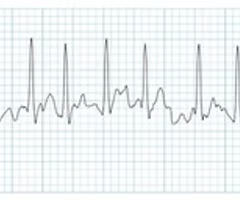
AFIB
irregularly fast or erratic heartbeat (arrhythmia) that affects the heart's upper chambers
supraventricular tachycardia (SVT) (above ventricles)
also called paroxysmal supraventricular tachycardia
-adenosine to identify underlying heart rate
most common type of supraventricular tachycardia
Atrioventricular nodal reentrant tachycardia (AVNRT)
pulse deficit
difference between apical and radial rate
apical-radial
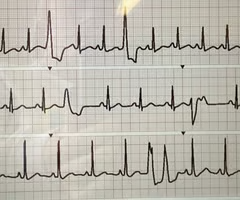
what is pacemaker close to SA node firing earlier than expected
premature atrial complex
caused by: caffeine, alcohol, nicotine, stretched atrial myocardium, hypervolemia, atria ischemia, infartion
No TX for infrequent
more than 6 per min is frequent and treat underlying cause
multiple rapid impulses from many atrial foci at a rate of 300 to 600 times per minute
atrial fibrillation
(a common heart rhythm disorder. Instead of a single electrical signal controlling the heartbeat, many "spark plugs" in the heart's upper chambers (atria) fire randomly. This causes the atria to quiver (fibrillate) chaotically rather than beating in a steady rhythm)
*highly irregular
what is causing decreased cardiac output in atrial fibrillation?
loss of atrial kick
how is atrial fibrillation classified?
paroxymal
persistent
long standing persistent
permanent
nonvalvular
paroxymal: suddent onset, lasts less or equal to 7 days. can recoccur
persistent: continuous, more than 7 days
long standing persistent: continous, more than 12 mos
permanent: decision has been made not to restore sinus rhythm
nonvalvular: absence of moderate to severe mitral stenosis (narrowing/stiffening of mitral valve)
AFIB RVR
AFIB meds
-antithrombic meds (bc risk of blood clot): warfarin, apixiban (eliquis)
-meds to control HR: beta blockers (block sympathetic system), calcium channel blockers (diltazem, cardizem)
-meds to convert heart rhythm or prevent afib: amiodarone, dofetilide
if a person is in AFIB for >48 hrs, what meds would you guve and why
adequate anticoagulants to prevent stroke from blood clots
if there is not a time to determine length of AFIB, what procedure is done to look at heart from inside
TEE- transesophageal electrocardiogram.
what is an elective procedure that must be synchronized with the QRS and patient is delivered 50-200 joules?
cardioversion
*patient is awake & frequently sedated
*consent form must be signed and EKG monitoring
*delivered on R wave
what is an emergency procedure for VTACH and AFIB and begins with 200-360 joules?
defibrillation
there is no cardiac output, patient is unconscious and requires EKG monitoring
**if its VIB, you DeFib! call a code!
difference in synch on/off with cardioversion and defibrillation
Setting Sync "On" (Synchronized Cardioversion) delivers a timed shock exactly on the heart’s R-wave to prevent triggering fatal rhythms like ventricular fibrillation. Setting Sync "Off" (Defibrillation) delivers an immediate, unsynchronized shock, which is necessary when the heart has completely stopped or shows chaotic, unorganized electrical activity
other procedures of AFIB
catheter ablation therapy: thin tubes into blood vessels and guides them to the heart, scars or destroys heart tissue thats triggering the arrhythmia
maze procedure: open heart surgery, pattern of scar tissue is made in the upper chambers forcing a normal path and sinus rhythm
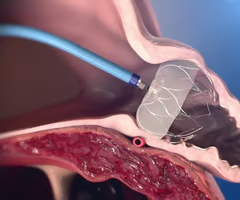
left atrial appendage occlusion: a minimally invasive procedure that permanently seals off the left atrial appendage—the heart pouch where most stroke-causing clots form in patients with atrial fibrillation, watchman device is placed that slowly grows into the endothelium preventing clots from getting out preventing strokes
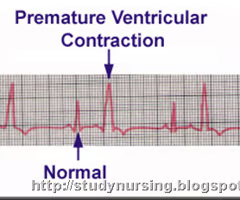
what is an impulse that starts in a ventricle and is conducted through the ventricles before the next normal sinus impulse? caused by caffeine, nictonine, alcohol, cardiac ischemia/infarction, increased workload on heart, electrolyte imbalances.
*feels like heart is skipping a beat
premature ventricular complexes
*tx usually based on cause and usual benign finding
Unifocal PVCs
bifocal PVCs
Cuplet PVCs
unifocal: extra beats look identical on ECG tracing, originate from a single, specific location
bifocal: extra beats in two distinctly different shapes or forms on the ECG, two different locations inside the ventricles
cuplet: pattern or grouping rather than shape of beat, two PVCs happen back-to-back, with no normal heartbeats between them
triplet
bigeminy PVC
trigeminy PVC
triplet: three consecutive premature ventricular contractions (extra heartbeats originating in the lower chambers) on an ECG, classfied as VTACH
bigeminy: a normal heartbeat is consistently followed by a Premature Ventricular Contraction (PVC), a pattern of two beats close together, followed by a slight pause. It often feels like a skipped beat, flip-flop, or pounding in the chest
trigeminy: a heart rhythm pattern where a premature ventricular contraction (PVC) occurs every third heartbeat, creating a repeating sequence of two normal beats followed by one early, extra beat

what is three or more PVCs in a row, repetitive firing or an irritable ventricular focus usually at greater than 100 beats/min, can be stable/unstable/pulselessness and what is treatment
ventricular tachycardia
tx: QUICKLY, id cause (H&Ts), synchonized cardioversion (WITH PULSE), antiarryhmic drugs.
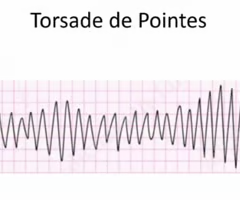
Torsades De Point
is type of VTACH
tx: magnesium sulfate
can be caused by haloperidol, CNS disease
what are the Hs of VTACH/VFIB
hypovolemia
hypoxia
acidosis
hypokalemia
hyperkalemia (tx but not cure by insulin, calcium gluconate, D50 (hypertonic solution)
hypoglycemia (d50)
Ts of vtach/vfib
hypothermia
toxins
cardiac tamponade (fluid in sac surrounding heart)
heart attack (go to cath lab)
thrombosis (PE) (heparin drip)
what is rapid, disorganized ventricular rhythms that causes ineffective quivering of the ventricles and what is the treatment
ventricular fibrillation
tx: cardiac emergency- No CO- start CPR, defibrillate (is NOT synchronized), antiarrythmic drugs within 2 mins. epinephrine every 3 mins, then amiodarone if failed

what med is used to prevent patient from remembering defibrillation
versed (midazolam)
ventricular asystole is
nonshockable
*confirmed in 2 different leads
*check monitor is still on.
*assess for h & ts
*meds: epi, atropine(stimulates sympathetic response)
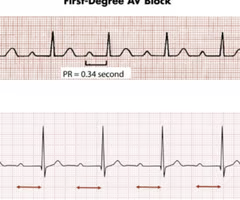
first degree atrioventricular block
when all the atrial impulses are conducted through the AV node into the ventricles at a rate slower than normal
-prolonged PR interval: greater than 0.20 seconds
-can be a precursor of higher degreees of AV block
-asymptomatic, assess cause. can cause further block
-regularly irregular
electronic device that provides electrical stimuli to heart muscles
pacemaker (cardiac resynchronization therapy)
- can be for slower than normal impulse formation, symptomatic AV or ventricular conduction disturbance
-temporary or permanent
creates an artifical block and can produce Left Bundle Branch Block (LBBB) pattern on ECG
- can be single or dual chamber

different modes of pacing in pacemakers
-synchronous
-asynchronous
-overdrive
synchronous: only if HR falls below set rate
asynchronous: fires regardless of intrinsic rate (hearts natural beating rate)
overdrive: suppress underlying rhythm so sinus node will regain control
implantable loop recorder
a tiny device placed just under the skin of your chest that continuously monitors your heart's electrical activity. It is designed for long-term use (up to 3 years) to diagnose infrequent or hidden heart rhythm issues like atrial fibrillation (AFib), palpitations, or unexplained fainting.
ACE inhibitors work on the
RAAS system
-pril
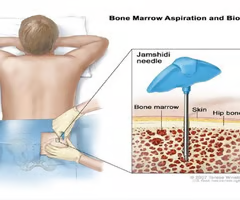
primary site for blood formation and maturation
bone marrow
-used for anemic and pancytopenia (shortage of all 3 major cells)
-aspirated in posterior superior iliac crest for biopsy. must sign consent form, physician gives.
-sharp brief pain in procedure. lidocaine is used, direct pressure after. patient can lay on that side.
what is the oxygen carrying component of an RBC and what is the lab value range
hemoglobin 12-18
lifespan of RBCs
120 days
complications of bone marrow biopsy
infection (osteomylitis), bleeding
what is reduction in oxygen-carrying capacity through either fewer RBCs or a reduction in hemoglobin
anemia
*is not a disease in itself, something else is causing it. it is a sign of an underlying disorder (decreased RBC production-nutrient deficient, decreased erythropoietin (which is how RBC are made), decreased iron), blood loss(inner, outer), increased RBC destruction (hemolysis-sickle cell, meds: methlydopa), incompatible blood, trauma
what vitamins/minerals are essential to RBC
iron, ferritin (stores iron,releases when needed), vitamin b12, folate
-transferrin which transports iron
- TIBC is the iron bonding capacity
what are some manifestiations of anemia
fatigue, weakness, pallor, jaundice, cardiac/respiratory symptoms, tongue changes, nail changes, angular cheilosis (mouth cracking), pica
measurement of RBC percentage in total blood volume, can detect blood disorders and can monitor internal bleeding post surgery
HCT
vcauses of polycthemia (too much rbc which causes blood to thicken and move more slowly)
hemoconcentration, dehydration from fluid loss, low oxygen, congenital heart diseases, pulmonary disorders which increase bone marrow stimulation, tumors, cushing syndrome (prolonged exposure to cortisol in body, usually caused by steroids)
cause of anemia
blood loss, low RBC production, high RBC destruction, malnourishment, ulcer/colon cancer, trauma, internal bleeding, menstruation, sickle cell anemia, splenomegaly, radiation/chemo
MCV
MCH
mcv: size of RCBs, think SUV (normal is 80-100 fL. <80-micocytic, >100-macrolytic
mch: color (amount of hgb) of RBCs, think C (chrome for color) 26-34 pg/cell
iorn deficiency anemia
most common in the world and most commonly caused by blood loss
I intake low or blood loss
R restless legs, strange cravings
O oxygen low (tachycardia, fatigue, pale)
N nails and structures (brittle nails, glossitis)
LOW for lab values
L low ferritin, low serum iron, low hgb/hct
O oxygen capacity high (Total Iron-Binding Capacity, or TIBC, is high)
W WBCs are fine, but RBCs are microcytic (small and pale)
*late sign of anemia
* common in premie babies
how to treat iron deficiency anemia
increase dietary iron (dark green vegetables, beets, dried beans, legumes, breads/cereals, red meat, eggs, tuna)
iron supplements: absorbed better with vitamin c. 1 hr before meals or 2 hrs after
can be given IM ztrack or IV
-educate: liquid iron stains teeth, black stool and constipation
folic acid deficiency
caused by inadequate dietary intake, malnutrition, malabsorption
onset and progression is slow
FOLATE Mnemonic:
Fatigue & Weakness: Lack of healthy red blood cells causes pale skin and low energy.
Oversized cells: increased MCV
Leafy greens: Leafy greens, fortified cereals, and citrus are top sources.
Alcoholism: Heavy alcohol use is a major cause of depletion.
Tongue swelling: Can cause a sore, red, or smooth tongue (Glossitis).
Embryo defects: Crucial for fetal spine development; deficiency causes neural tube defects like spina bifida and acromegaly (childbearing age should have 400-800 mcg daily)
*IM or PO
Vitamin b12 anemia
-inadequate source of b12 or malabsorption, can be caused by meds that decrease gatric acid, vegetarianism, veganism
PERNICIOUS Mnemonic:
P - Parietal cells in the stomach are destroyed (autoimmune).
E - Extrinsic factor (Vitamin B12 itself) can't be absorbed without the Intrinsic Factor.
R - Red blood cells become abnormally large (increased MCV)
N - Neurological symptoms (tingling, numbness, nerve damage) are the hallmark, which differentiate it from folate deficiency and can become permanent.
I - Intrinsic Factor is missing.
C - Cobalamin is the medical name for Vitamin B12.
I - Injections (intramuscular) are required for life-long treatment.
O - Originates primarily from animal products (meat, eggs, dairy, Seafood).
U - Unexplained fatigue, weakness, and pale skin occur due to low oxygen-carrying capacity.
S - Schilling test historically used to diagnose it (rarely used now)
will also have Lhermitte's Sign (flex neck, electrical shock down spine)
sickle cell disease
Genetic disorder in which red blood cells have abnormal hemoglobin molecules and take on an abnormal shape.
SICKLE Mnemonic:
S - Splenic sequestration & Strokes: Sickled cells can get trapped in the spleen (causing enlargement) and block blood vessels in the brain.
I - Infections: Because the damaged spleen cannot filter bacteria properly, patients are highly susceptible to infections. (osteomylitis)
C - Crises (Pain): Blocked blood vessels cause severe, unpredictable pain crises (vaso-occlusive crises-caused by infection, fever, dehydration, physical exertion, excessive cold exposure, hypoxia).
K - Kidney & Lung issues: Reduced blood flow damages organs, potentially leading to renal issues (jaundice bc as RBCs hemolyse, bilirubin is released) or Acute Chest Syndrome.
L - Lifespan of cells: Normal red blood cells live 90-120 days, but sickle cells only survive 10-20 days, causing severe anemia.
E - Enlarged facial bones (bone enlarging bc bone marrow is enlarging the body is compensating), Eye & Organ damage: Small vessel blockages can lead to vision issues and long-term damage to the heart, liver, and bones
-also primarily african descent
meds/treatment of sickle cell disease
hematopoetic stem cell transplant (bone marrow transplant)
hydroxyurea (PO med, reduces frequency of pain crisis, elevates hgb levels making them more flexible to prevent blockages)
folic acid (support rapid red blood cell production)
hydration
transfusion therapy
pain management
preventing infection
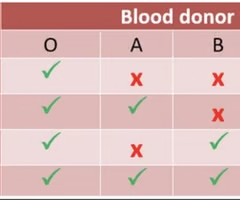
blood transfusion therapy
type and screen, consent, culture consent, IV patency- has to be started within 30 mins, VS before and every 15 mins, hang with normal saline
Factor VIII (A) (memory trick: 8 rhymes with A)
Factor 1x is (B)
HEMO Mnemonic:
H - Hemarthrosis (Bleeding into the joint spaces, causing swelling and pain) (tx RICE).
E - Easy bruising.
M - Muscle and soft tissue bleeding (hematomas).
O - Oozing (Prolonged bleeding after minor trauma or dental procedures)
*effects males, females are carriers.
*toddlers is usually dx age
*DESMOPRESSIN (Ddvap) increase plasma factor VII
*recombinant factor to replace what they're lacking
*PTT elevated
*incurable
*avoid NSAIDS, acetylsalicylic acid (aspirin
thrombocytopenia
- Idiopathic thrombocytopenic purpura- an autoimmune disorder where the immune system mistakenly attacks and destroys the body's platelets (follows viral infection or immunization in children)
- Heparin induced thrombocytopenia (immune response to heparin)
*decreased platelets -> easy bruising, petechiae, bleeding
pulmonary embolism
obstruction of one or more branches of pulmonary artery. can be caused by thrombus (blood clot), piece of tumor, amniotic fluid, air, or fat
DVT greatest risk factor.
lab studies: ABGs, BNP, Troponin, D Dimer
imaging: xray, ecg, MDCTA (multidetector row computed tomography angiography- tells size and location), chest ct, V/Q scan (ventilation and perfusion scan= an imbalance shows likeliness of MI), pulmonary angiography (uses X-rays and contrast dye to visualize the blood vessels in your lungs)
PE management
anticoagulants and surgical management
-enoxoparin (lovenox)- low molecular weight heparin used to treat and prevent blood clots (give bubble, abdomen)
-unfractionated heparin- monitor PTT to make sure platelets aren't dropping
-thrombolytic therapy (activase)- only med that dissolves clot
surgical
-embolectomy- removes embolism
-coil in surgery to capture and remove clot
-inferior venacava filter (IVC) clot gets caught in filter to keep it from going to lungs
difference in ischemic stroke and hemorrhage stroke
ischemic is blockage of a blood vessel, hemorrhagic is bleeding into the brain.
*cerebrovascular accidents.
-CT within 20 mins
transient ischemic stroke TIA
can be warning of impending stroke
symptoms resolve within 24 hrs
FAST mnemonic
Face- look for uneven smile
Arm- check if one arm is weak
Speech- slurred
Time- call 911 at first sign
which stroke is sudden onset caused by sudden blockage of cerebral blood vessel causing lack of blood flow
ischemic stroke
-thrombotic caused by atherosclerosis
-embolic- blood clot travels from elsewhere and blocks artery in brain
manifestations of ischemic stroke
Symptoms depend on the location and size of the affected area
Numbness or weakness of face, arm, or leg, especially on one side
Confusion or change in mental status
Trouble speaking or understanding speech
Difficulty in walking, dizziness, or loss of balance or coordination
Sudden, severe headache
Perceptual disturbances
management of ischemic stroke
rt-PA: must present with 3-4.5 hours of stroke symptom onset
-no hemmorhage on head on CT
-symptoms present for 30 min, not rapidly improving or attributable to another disease
- imaging is consistent with acute ischemic stroke
mechanical intervention: endovascular thrombectomy, intra arterial mechanical thrombectomy: both using catheter to remove clot
left cerebral hemisphere stroke
weakness/paralysis RT side of body, right visual field deficit, aphasia (affects speech, writing, and ability to understand)
altered intellectual ability, slow cautious behavior
**LEFT BRAIN=LANGUAGE & LOGIC
right cerebral hemisphere stroke
left side of body
spatial perception defecit(impairs the brain's ability to process and interpret visual information regarding the location, distance, and orientation of objects)
increased distractibility
impulsive behavior and poor judgement
lack of awareness of deficits
**RIGHT BRAIN=RECKLESS &RUSHED
visual agnosia
eyes process but brain doesn’t comprehend what an object is
what meds are a risk factor of hemorrhagic stroke
sympathetic nervous system stimulants such as amphetamines, cocaine
symptoms of hemorrhagic stroke
severe headache described as worst headache they've ever had, early and sudden changes in LOC, n/v, bleeding, possibly seizures
complications of hemorrhagic stroke
cerebral hypoxia, decreased blood flow, vasospasm (sudden constriction of artery), increased ICP, HTN
-prevent and mitigate complications
-surgery can clip aneurysm or coil to keep from rupturing
nursing interventions strokes
-positioning to prevent contractures
-Botulinum toxin type A injected intramuscularly into wrist and finger muscles to prevent spasticity
-passive exercise
-standing/ambulation when ready
-self care
-approaching on visual side
-swallowing precautions
-catheters/bedpans
-speech therapy
-skin assessment
-family counseling
-vital signs due to ICP/pneumonia
inability of heart to pump enough cardiac output to meet the demands of the body
heart failure
defect in ventricular filling (diastolic)- ventricles not relaxing
ventricular ejection (systolic)