PTSD and Anxiety (HeadMed - 7/14)
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Adjustment Disorder Definition
Characterized by depressive symptoms, anxiety, and/or behavioral changes without fully satisfying criteria for a proper depressive or anxiety disorder
Follows an event experienced as stressful
Marked difficulty implementing adaptive response due to increased demand for cognitive and emotional resources
Adjustment Disorder Clinical Presentation
Symptoms start within 3 months after stressor
Last up to 6 months after stressor is removed
Low mood, anxiety, alterations in mood or behavior (self-harm, self-medication, etc.)
Adjustment Disorder Diagnostic Criteria
Emotional and behavioral symptoms develop after exposure to one or more stressful events, occurring within 3 months of exposure
Significant clinical impact evidenced by:
Pronounced distress disproportionate to the stressor, OR
Significant impairment in functioning across life areas (social, occupational)
Symptoms of another mental disorder cannot explain the disturbance
Symptoms do not represent normal grief
Once no longer exposed to stressor, symptoms do not persist beyond 6 months
Adjustment Disorder Treatment
Psychotherapy: Group and individual formats
Pharmacotherapy:
Anxiolytics (Benzodiazepines)
Antidepressants (SSRIs & SNRIs)
Dissociative Disorder Definition
Loss of mutual integration between systems underlying complex mental activity: consciousness, memory, identity, emotions, and perception
Normally experienced as continuum and in constant integration; in dissociative disorders these systems disconnect
Positive symptoms: Unwanted intrusions into consciousness and behavior; loss of continuity of subjective experience
Negative symptoms: Inability to access information or control mental functions generally easily accessible or controllable
Dissociative Identity Disorder (formerly "multiple personality disorder"): Two or more distinct personality states; failure of identity integration; each personality state may have separate personal history, self-image, identity, and name
Dissociative Disorder Epidemiology
1.4% female, 1.6% male
Dissociative Disorder Risk Factors
Trauma
Childhood sexual and physical abuse
Dissociative Disorder Comorbidities
PTSD
Borderline personality disorder
Avoidant personality disorder
Substance abuse
Depression
Somatoform disorder
Dissociative Disorder Diagnostic Criteria
Patient has two or more distinct personality states; disruption in identity characterized by marked discontinuity in sense of self and autonomy
Recurrent gaps in memory for everyday events, important personal information, and/or traumatic events
Symptoms cause clinically significant distress or impairment in social or occupational functioning
Disturbance is not part of widely accepted cultural or religious practice
Physiological effects of substance or another medical condition cannot explain symptoms
Dissociative Disorder Clinical Presentation
Feeling like depersonalized observers of own speeches and actions
Perception of voices
Strong emotions and egodystonic impulses (thoughts, urges, or behaviors in direct conflict with core values, self-image, or personal identity)
Sudden changes in attitudes, perspectives, and personal preferences
Perception of one's body as different
Non-epileptic seizures or other conversive symptoms
Dissociative amnesia: Gaps in remote memory of personal life events; memory errors related to acquired procedures; discovery of evidence of daily actions/tasks not remembered performing
Dissociative fugues: Common in these patients
Dissociative Disorder Treatment
Psychotherapy:
Psychoanalysis
Cognitive and behavioral therapy
Hypnosis
Family therapy
Pharmacotherapy:
SSRIs
Tricyclic antidepressants (TCAs)
MAOIs
β-blockers
Clonidine
Anticonvulsants
Benzodiazepine
Depersonalization Disorder Definition
Psychopathological condition where individual feels detached from themselves, from aspects of own self (feelings, thoughts, body or parts of body, sensations), or divided (out-of-body experience)
Derealization Disorder Definition
State where individual feels as if in fog, in dream, in bubble; as if veil or glass wall between themselves and world
Distinction between Depersonalization and Derealization Disorders
Depersonalization = detached from one's self
Derealization = detached from one's surroundings
Depersonalization and Derealization Disorder Risk Factors
Acute trauma
Other psychiatric disorders
Substance abuse
Childhood trauma
Sudden death of loved one
Growing up with parent with severe psychiatric issues
Disturbances or doubts about sexual orientation
Depersonalization and Derealization Disorder Comorbidities
Major depressive disorder
Anxiety disorders
OCD
Avoidant personality disorder
Borderline personality disorder
Depersonalization and Derealization Disorder Diagnostic Criteria
Patient experiences depersonalization, derealization, or both:
Depersonalization: Feels detached from own thoughts, feelings, sensations, body, or actions
Derealization: Feels detached from surroundings
Reality testing remains intact during depersonalization or derealization experiences
Symptoms cause clinically significant distress or impairment in social and/or occupational functioning
Physiological effects of substance or another medical condition cannot explain disturbance
Another mental disorder cannot explain disturbance
Depersonalization Clinical Presentation
Abnormal body experiences
Emotional or physical blunting
Temporal distortion with abnormal subjective memories
Macropsia: Neurological and optical phenomenon where objects appear larger than they are
Micropsia: Neurological and optical phenomenon where objects appear smaller than they are
Derealization Clinical Presentation
Subjective visual disturbances:
Blurring
Amplified acuity
Widening or narrowing of visual field
Macropsia or micropsia
Subjective auditory disturbances:
Amplified or muted voices or sounds
Depersonalization and Derealization Disorder Treatment
Psychotherapy:
Cognitive Behavioral Therapy (CBT)
Hypnotherapy
Pharmacotherapy:
SSRIs
Tricyclic antidepressants (TCAs)
Mood stabilizers
Typical and atypical antipsychotics
Post-Traumatic Stress Disorder (PTSD) Definition
Disease occurring in people who have suffered or witnessed a traumatic or violent event, or if traumatic experience happened to loved one
Triggered by various traumatic events: wars, robberies, child abuse, muggings, kidnapping, terrorist attacks, torture, natural disasters, serious car accidents
Onset varies: first weeks or several months after event
Includes emotional and cognitive symptoms and neuro-vegetative alterations
Characteristic: Re-experiencing traumatic event in recurring, involuntary, and intrusive way with vivid memories associated with sensory, emotional, physical, and behavioral components
Clinical presentation highly variable: dysphoric component may prevail in some; fear of reliving trauma central in others; dissociative symptoms prevalent in still others
Post-Traumatic Stress Disorder (PTSD) Epidemiology
Incidence: 8–15% in general population
Female: 10%; Male: 4%
30–50% of people exposed to violence, genocide, war veterans, medical providers, police and firefighters
Post-Traumatic Stress Disorder (PTSD) Prognosis
Typically chronic: 1/3 recover within year; 1/3 continue to have symptoms after 10 years
Positive prognostic factors:
Rapid onset
Duration less than 6 months
Good previous functioning
Good social support
Absence of other comorbidities
Has consequences in multiple areas: marriage, employment, suicidality
Post-Traumatic Stress Disorder (PTSD) Comorbidities
Depression
Bipolar disorder
Anxiety disorder
Substance abuse
Conduct disorder
Physical illness (endocrine, autoimmune, pulmonary, etc.)
In children specifically:
Separation anxiety
Oppositional defiant disorder
Major cognitive disorder
Post-Traumatic Stress Disorder (PTSD) Pathogenesis - Psychological Models
Psychoanalytic model: Trauma brings quiescent but unresolved psychological conflict to light; subject experiences state of repression, denial, and immobility
Cognitive-behavioral model: Subject unable to rationalize trauma; continuously relives it; implements avoidance behaviors to factors reactivating memory
Phase 1: Trauma (unconditioned stimulus) produces fear elicited by specific stimuli (physical or mental: sights, sounds, smells) causing conditioning
Phase 2: Repetition of conditioned stimulus evokes fear response even without original unconditioned stimulus; subject avoids both unconditioned and conditioned stimuli; secondary advantage (protection, compassion, care by others) should not be underestimated
Post-Traumatic Stress Disorder (PTSD) Pathogenesis - Biological Basis
Noradrenergic system
Dopaminergic system
GABAergic system
Endogenous opioids: Low concentration of plasma β-endorphins; analgesic response to opioid antagonists (e.g., naltrexone) observed in veterans with PTSD
Hypothalamic-pituitary-adrenal (HPA) axis:
Low levels of plasma and urinary cortisol
Increased glucocorticoid receptors in lymphocytes
Poor ACTH response after CRF stimulation
Cortisol hypersuppression may predict who will develop disorder given exposure to same traumatic events
Hyperactivation of axis differs from other mental disorders
Autonomic nervous system:
Increase in sympathetic tone leads to: increased heart rate, blood pressure, tremors, sweating, palpitations, sleep disturbance (fragmentation and increased sleep latency)
Desensitization of α₂- and β-adrenergic receptors via chronic downregulation
Increased concentrations of urinary catecholamines observed in laboratory tests
Post-Traumatic Stress Disorder (PTSD) Risk Factors for Development
Physical or sexual abuse
Female gender
Youthful age
Repeated exposure to traumatic events
Objective severity or degree of direct exposure
Personality disorder
Ethnic minority status, low socioeconomic status, poor psychosocial resources
Widowed, separated, or divorced status
Personal or family history of psychiatric illness
Recent excessive use of alcohol
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #1
Exposure
Direct or indirect exposure to actual or threatened death, serious injury, or sexual violence
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #2
Intrusion Symptoms (At least one required)
(a) Recurrence of memories related to traumatic event on involuntary basis and perceived as intrusive
(b) Recurrent nightmares related to traumatic event
(c) Experience of dissociative reactions where patient feels as if traumatic event was recurring
(d) Psychological suffering as result of exposure to factors symbolizing and recalling traumatic event
(e) Marked physiological reactions as result of exposure to factors symbolizing and recalling traumatic event
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #3
Avoidance
Avoidance of distressing feelings, thoughts, or memories associated with traumatic event AND/OR
Avoidance of external reminders that arouse distressing feelings, thoughts, or memories associated with traumatic event
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #4
Negative Changes in Cognitions and Mood (At least two required)
(a) Lack of ability to recall relevant aspects of traumatic event
(b) Persistence of exaggerated negative beliefs and expectations about oneself, others, and world
(c) Persistent, distorted thoughts about cause or consequences of traumatic event leading to self-blame or blaming others
(d) Persistent negative emotional state
(e) Markedly diminished interest in several activities
(f) Feelings of detachment or estrangement from others
(g) Persistent incapability of experiencing positive emotions
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #5
Alterations in Arousal and Reactivity (At least two required)
(a) Irritability
(b) Reckless or self-destructive behavior
(c) Hypervigilance
(d) Incremented startle response
(e) Difficulty in concentrating
(f) Difficulty in sleeping
Post-Traumatic Stress Disorder (PTSD) - Diagnostic Criteria #6
Duration
Symptoms last more than 1 month
Post-Traumatic Stress Disorder (PTSD) Clinical Presentation
Intrusive symptoms: Flashbacks
Avoidance: Avoidance of anything reminiscent of stressor
Psychogenic amnesia: Can't remember important aspects of stressor
Hyperarousal: Heightened arousal state
Suicidal ideation
Post-Traumatic Stress Disorder (PTSD) Treatment: Pharmacotherapy
First-line: SSRIs & SNRIs
Alternative medications:
Tricyclic antidepressants
MAOIs
Mood stabilizers
Trazodone (helps with both sleep and depression)
Hypnotics and sedatives for sleep (caution: can produce vivid nightmares)
Alpha blockers for nightmares
Antipsychotics
Post-Traumatic Stress Disorder (PTSD) Treatment: Psychotherapy
Cognitive Behavioral Therapy:
Exposure: Repeatedly exposing patient to traumatic thought, memory, or feeling
Eye Movement Desensitization and Reprocessing (EMDR):
Structured psychotherapy approach to alleviate distress associated with traumatic memories
Therapist has patient focus on specific memory, thought, or feeling while engaging in bilateral stimulation (e.g., following therapist's hands or light with eyes)
Trauma-Informed Care Definition
Framework that acknowledges effects of trauma on people and aims to help restore sense of safety and self-worth
Based on idea that traumatic experiences can be terrifying and overwhelming
Care teams need to understand patient's past and present life situation to provide effective care
Trauma-Informed Care Core Concepts
Safety (physical and emotional)
Trustworthiness
Choice
Collaboration
Empowerment
Stress vs. Anxiety
Stress: adaptive response to a threat; generally temporary; useful for motivation
Anxiety: the reaction to stress; may occur without identifiable trigger; can be disproportionate; may persist beyond trigger removal; interferes with daily functioning
Shared element: many interventions are helpful with both stress and anxiety
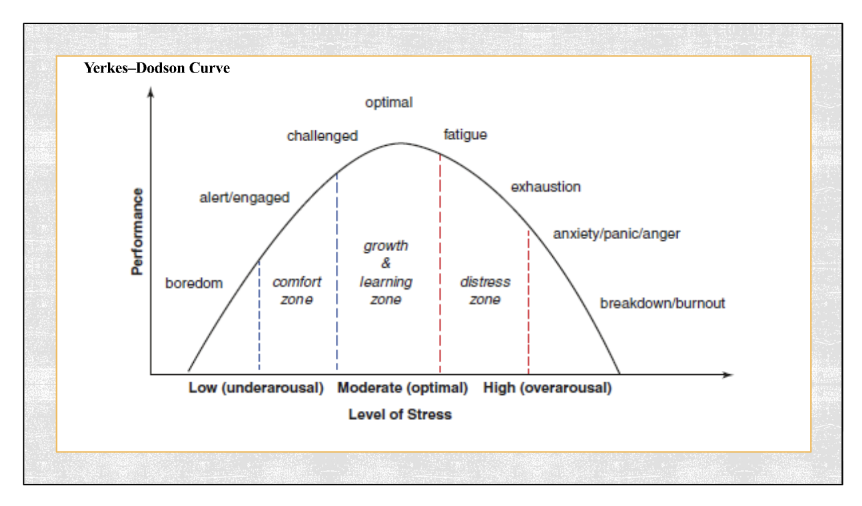
Yerkes-Dodson curve
Relates intensity of anxiety with efficiency of performance
Depicts continuum between physiological (adaptive) and pathological (maladaptive) anxiety
Normal anxiety level required for satisfactory performance
Phase 1: increased anxiety improves performance up to optimal level
Phase 2: continued anxiety increase leads to decreased physical and cognitive performance, progressing to dysfunctional state
General Epidemiology of Anxiety Disorders
Prevalence Data (U.S. Adults, 2019)
Approximately 15.6% had any anxiety disorder in past year
Higher in females (19%) than males (11.9%)
Estimated 31-34% experience any anxiety disorder at some point in lifetime
Among those with any anxiety disorder:
10.8% had serious impairment (interfering with individual’s ability to function in daily life)
13.5% had moderate impairment
Generalized Anxiety Disorder (GAD) Epidemiology
Affects approximately 4-7% of population
Higher rates in women (2x more than men), African-Americans, and ages less than 30
Can occur at any age; typically begins in early 20s
Chronic condition; may develop panic disorder later
50-90% co-occur with Major Depressive Episode, other anxiety disorders (panic disorder), or substance use disorders
Generalized Anxiety Disorder (GAD) General Etiology and Pathophysiology
still not fully understood ***
Multifactorial: genetic, environmental, and biologic factors
Genetic Factors
Psychosocial Factors
Neurobiologic Factors
Generalized Anxiety Disorder (GAD) Genetic Factors
First-degree relatives have 25% risk
Not fully understood
Generalized Anxiety Disorder (GAD) Psychosocial Factors
Conditioning
Stress or trauma
Chronic illness
Substance abuse (some substances cause anxiety, some patients self medicate and the substances exacerbate their symptoms)
Generalized Anxiety Disorder (GAD) Neurobiologic Factors
Functional imaging findings:
Hyperactivity of the amygdala
Decreased activity of the hippocampus
HPA axis hyperactivation leading to increased cortisol levels
Neurotransmitter imbalances/abnormal functioning: Norepinephrine, Serotonin, Dopamine, GABA (low)
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Cardiovascular System
Increased heart rate and output
Increased blood volume and blood pressure
Peripheral vasoconstriction
Coronary dilation
Positive cardiac inotropic effect
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Respiratory System
Increased oxygen exchange
Tachypnea
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Digestive System
Xerostomia (dry mouth)
Contractions of the esophagus
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Gastrointestinal System
Increase in gastric acid secretion
Changes in peristalsis
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Metabolic Effects of Catacholamines
Activation of glycogenolysis and lipolysis
Increase in free fatty acids, glucose, and lactate
Increased blood levels of glucose, free fatty acids, cholesterol
Generalized Anxiety Disorder (GAD) Psychosomatic Symptoms - Musculoskeletal, Skin, Immune System
Increased muscle tone
Increased smooth muscle contractions
Increased perspiration
Decreased skin temperature
Reduction of immune activity
Generalized Anxiety Disorder (GAD) Cognitive Symptoms
Feeling nervous or on edge/tightrope
Exaggerated alarm responses
Difficulty concentrating
Inability to relax
Insomnia
Irritability
Apprehensive attitude (fearful of being in situations they would not be able to handle)
Fear of being unable to deal with situations
***General feeling that everyone is out to get them
Generalized Anxiety Disorder (GAD) Diagnostic Criteria
A. Excessive anxiety and worry occurring more days than not for at least 6 months
B. Difficulty controlling the worry
C. 3 (or more) of the following six symptoms (only one required in children):
Restlessness or feeling keyed up or on edge
Being easily fatigued
Difficulty concentrating or mind going blank
Irritability
Muscle tension
Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep)
D. Symptoms cause clinically significant distress or impairment
E. Not attributable to drugs, medications, other medical condition, or other mental disorder
Generalized Anxiety Disorder (GAD) Differential Diagnosis
(what might be causing these anxiety symptoms)
Hyperthyroidism - can cause heart palpitations/weight loss/jittery/ on-edge/hyperactive/cardiac arrhythmias
Paroxysmal supraventricular tachycardia
Pheochromocytoma
Hypoglycemic crisis
Complex partial seizure
Mitral prolapse
Respiratory pathologies - ex. professor did a study where he semi-suffocated patients, high CO2 in the brain have increased feelings of anxiety
Dizzy syndromes
Anxiety disorder due to another medical condition
Induced anxiety disorder
Depression (50% of patients often have overlap; assess for both if one is present. Lots of drugs for anxiety will also cover depression)
Phobias
Conversion disorder
Generalized Anxiety Disorder (GAD) Screening Recommendations
70-90% of patients with anxiety present with somatic complaints
Evaluation/exclusion of other causes:
Cardiac: EKG, cardiac enzymes
Metabolic panel: electrolyte abnormalities
Thyroid studies: rule out hyperthyroidism
Cortisol levels: rule out Cushing syndrome (buffalo hump, round belly
Screen for other medications, illicit substances, vitamins, herbs, caffeine, alcohol, nicotine
USPSTF Screening Tools
GAD-7: 7 questions, rank 0 to 3 - Recommended for annual screening in adults 64 years and younger, including pregnant and postpartum persons
Scoring: 5 (mild), 10 (moderate), 15 (severe)
Cut-off of 10 yields sensitivity of 89% and specificity of 82%
screens for presence and severity of anxiety
GAD-2: Modified tool using only first 2 questions
Generalized Anxiety Disorder (GAD) Non-Pharmacologic Treatment
Can be as effective as medications
Cognitive Behavioral Therapy (CBT): has best level of evidence (see a counselor/psychologist. duration varies by patient and severity, how motivated they are to attend and implement changes. Approximately 6-12 months)
Education
Self-monitoring
Biofeedback/relaxation/breathing techniques
Cognitive restructuring
Exposure therapy
3 C’s of Cognitive Behavioral Therapy
Identify the thought that came before the emotion
Reflect on how accurate and useful the thought is
Change the thought to a more accurate or helpful one as needed
Generalized Anxiety Disorder (GAD) Pharmacotherapy
First-line therapy: Antidepressants
Selective serotonin reuptake inhibitors (SSRIs)
Serotonin norepinephrine reuptake inhibitors (SNRIs)
Tricyclic antidepressants (TCAs)
Atypical antidepressants
Combination therapy: Sometimes needed for severe/refractory disease
Secondary options, when you have exhausted all other avenues
Benzodiazepines (may be addictive and lead to tolerance and dependence)
Beta-blockers
Anticonvulsants
Duration: Treat 6-12 months (long-term acting treatment, follow up to wean dose down. Completely stopping the treatment can cause rebound)
Separation Anxiety Disorder Epidemiology
Childhood prevalence: 12-month prevalence ~4% (divorced parents)
Adult prevalence: 12-month prevalence 1-2% (divorce, separation from close friend)
Course in childhood: Usually does not progress into adulthood (attachment typically to parent)
Adult onset: Majority of adults develop symptoms in adulthood (attachment to spouse or friend)
Separation Anxiety Disorder DSM-5 Diagnostic Criteria
A. Clinical Presentation (at least 3 of following):
Recurrent excessive distress when anticipating or experiencing separation from home or major attachment figures
Persistent and excessive worry about losing major attachment figures or possible harm to them (illness, injury, disasters, death)
Persistent and excessive worry about experiencing untoward event (getting lost, being kidnapped, having accident, becoming ill) that causes separation from major attachment figure
Persistent reluctance or refusal to go out, away from home, to school, to work, or elsewhere due to fear of separation
Persistent and excessive fear of or reluctance about being alone or without major attachment figures at home or other settings
Persistent reluctance or refusal to sleep away from home or go to sleep without being near major attachment figure
Repeated nightmares involving theme of separation
Repeated complaints of physical symptoms (headaches, stomachaches, nausea, vomiting) when separation from major attachment figures occurs or is anticipated
B. Duration:
At least 4 weeks in children and adolescents
Typically 6 months or more in adults
C. Functional Impact:
Causes clinically significant distress or impairment in social, academic, occupational, or other important areas of functioning
D. Exclusion:
Not better explained by other condition
Separation Anxiety Disorder Treatment
Medication: SSRIs, benzodiazepines (in combination with psychotherapy)
Psychotherapy: Cognitive behavioral therapy, social skills training, graded exposure and relaxation training
Family involvement: Individual psychotherapy and potentially family therapy (social skills training, graded exposure)
Specific Phobias Epidemiology
Fairly common - Prevalence: ~7-12% of population
Typical onset: Childhood, before age 12
Gender: Women > men (2:1 ratio)
Genetic factor: Run in families - hyperactive stress response, conditioning from analyzing parent reactions
Nature: Irrational fears of specific objects, places, situations, or activities with associated avoidance behaviors that negatively affect quality of life
***Person’s reaction is excessive and inappropriate
Specific Phobias Clinical Characteristics
Fear of objects that could cause harm (snakes, heights, flying, blood) with excessive and inappropriate reactions
Person's reaction disproportionate to actual danger
Specific Phobias DSM-5 Diagnostic Criteria
A. Fear or Anxiety:
Marked fear or anxiety about specific object or situation (e.g., flying, heights, animals, receiving injection, seeing blood)
Note: In children, may be expressed by crying, tantrums, freezing, or clinging
B. Provocation:
Phobic object or situation almost always provokes immediate fear or anxiety
C. Avoidance/Endurance:
Phobic object or situation actively avoided or endured with intense fear or anxiety
D. Disproportionality:
Fear or anxiety out of proportion to actual danger posed by specific object or situation and to sociocultural context
E. Persistence:
Typically lasting for 6 months or more
F. Functional Impact:
Causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
G. Exclusion:
Not better explained by another condition
Specify type: Animal, natural environment, blood-injection-injury, situational, or other
Specific Phobias Treatment
Behavioral Interventions (Most Effective)
Cognitive Behavioral Therapy:
Systematic desensitization: Patient gradually exposed to feared situations, beginning with least-feared situation
ex. draw a bird, look at a photograph of a bird, went outside to look at bird in real life
Flooding: Patient enters situations associated with anxiety until anxiety subsides (e.g., eating in restaurants)
ex. throwing them in until they can tolerate fear
Requirement: Patient must be willing to confront feared situations
Pharmacologic Interventions
Generally ineffective for phobias
May use anxiolytics or beta-blockers for acute symptoms
ex. short-acting benzodiazepine for fear of heights in order to ride an airplane
***Most patients do not seek treatment (avoidance of trigger maintains disorder)
Social Anxiety Disorder Epidemiology
aka: Social Phobia - Fear of humiliation or embarrassment in social situations
Prevalence: ~13%
Gender: Women = Men
Typical presentation: Before age 25, usually in adolescence
Precipitating factors: No identifiable precipitating factor
Comorbidity: Frequently co-occurs with other psychiatric disorders (schizo - zero interest in socializing or avoidant personality disorders - insecure about the relationship) and/or substance abuse
both not fearful of the situation
Neurobiological factor: Dopaminergic pathways may play a role
Social Anxiety Disorder DSM-5 Diagnostic Criteria
A. Fear/Anxiety: Marked fear or anxiety about one or more social situations where individual is exposed to possible scrutiny by others
Note: In children, anxiety must occur in peer settings, not just during interactions with adults
B. Fear of Negative Evaluation: Individual fears acting in a way or showing anxiety symptoms that will be negatively evaluated (humiliating, embarrassing, leading to rejection, or offending others)
C. Provocation: Social situations almost always provoke fear or anxiety
Note: In children, fear/anxiety may be expressed by crying, tantrums, freezing, clinging, shrinking, or failing to speak in social situations
D. Avoidance: Social situations are avoided or endured with intense fear or anxiety
E. Disproportionality: Fear or anxiety is out of proportion to actual threat posed by social situation and to sociocultural context
F. Persistence: Fear, anxiety, or avoidance is persistent, typically lasting 6 months or more
G. Functional Impairment: Fear, anxiety, or avoidance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
H-J. Exclusion: Not caused by illicit substance or other medical or psychiatric condition
Specifier: If performance only—fear is restricted to speaking or performing in public
Social Anxiety Disorder Treatment Approaches
Most Effective: Combination of CBT and medications
Pharmacotherapy Options:
First-line: Fluoxetine, Paroxetine, Sertraline, long-acting Venlafaxine
Other SSRIs
MAOIs
Benzodiazepines (provide temporary relief but have long-term risks)
Tricyclic antidepressants (probably less effective)
Panic Disorder Definition
Recurrent, unexpected panic (or anxiety) attacks that are distressing and cause persistent worry or behavioral changes
May be caused by adverse event, but often no precipitating stressors before onset
Typically chronic with waxing and waning symptoms
Panic Disorder DSM-5 Diagnostic Criteria
A. Recurrent Unexpected Panic Attacks: Abrupt surge of intense fear or discomfort reaching peak within minutes
Note: Abrupt surge can occur from calm state or anxious state
Palpitations, pounding heart, or accelerated heart rate
Sweating
Trembling or shaking
Sensations of shortness of breath or smothering
Feelings of choking
Chest pain or discomfort
Nausea or abdominal distress
Feeling dizzy, unsteady, light-headed, or faint
Chills or heat sensations
Paresthesias (numbness or tingling sensations)
Derealization (feelings of unreality) or depersonalization (being detached from oneself)
Fear of losing control or "going crazy"
Fear of dying
B. Post-Attack Symptoms (1 month or more following at least one attack):
Persistent concern or worry about additional panic attacks or their consequences (losing control, having heart attack, "going crazy")
Significant maladaptive change in behavior related to attacks (avoidance of exercise, unfamiliar situations)
C-D. Exclusion: Not better explained by substance use or another medical/psychiatric condition
An abrupt surge of intense fear or discomfort reaching peak within minutes, with four or more of the following symptoms:
Panic Disorder Epidemiology
Prevalence: 1-4% of population
Genetic factors: 20% among first-degree relatives
Lifetime risk: 5% in women, 2% in men
Age of onset: Mid-20s (8 in 10 before age 30)
Theoretical basis: Conditioned response vs. biologic basis unclear
Neurobiological mechanisms:
Increased catecholamine levels in CNS (stress response)
Abnormality in locus coeruleus (brain stem area regulating alertness)
Carbon dioxide (CO₂) hypersensitivity
Abnormalities in lactate metabolism or γγ-aminobutyric acid (GABA) neurotransmitter system
Panic Disorder Treatments
Combined Approach: CBT + Pharmacotherapy
First-line Medications: SSRIs, 70-80% effective, safe, and well-tolerated
Fluoxetine
Paroxetine
Sertraline
Alternative Medications:
Serotonin-norepinephrine reuptake inhibitor (SNRI): Venlafaxine (long-acting)
TCAs
MAOIs
Benzodiazepines
Beta-blocking drugs (note side effects)
Duration: Continue medications for at least 1 year; relapse is common - most people take medication lifelong
Agoraphobia Definition
"Agoraphobia translates literally from Greek as 'fear of the marketplace'"
Anxiety related to being in embarrassing places or situations or from which it would be difficult to escape or in which help may not be available in event of panic attack
Agoraphobia Triggers and Impact
Common Triggers:
Leaving home alone
Crowded or closed places (stadiums, shopping malls, cinemas, means of transport, queuing in traffic, tunnels)
Wide-open spaces (freeways, bridges, wide streets, squares)
Consequence: Avoidance of triggers severely limits patient's autonomy and quality of life
Comorbidity: May co-occur with panic disorder; treatments are similar (exposure therapy + medications)
Agoraphobia DSM-5 Diagnostic Criteria
A. Fear/Anxiety About Two or More Situations:
Using public transportation (automobiles, buses, trains, ships, planes)
Being in open spaces (parking lots, marketplaces, bridges)
Being in enclosed places (shops, theaters, cinemas)
Standing in line or being in a crowd
Being outside of home alone
B. Avoidance Motivation: Avoidance of situations because of thoughts that escape might be difficult or help might not be available in event of panic-like symptoms or other incapacitating/embarrassing symptoms (e.g., fear of falling in elderly; fear of incontinence)
C. Provocation: Agoraphobic situations almost always provoke fear or anxiety
D. Response: Agoraphobic situations are actively avoided, require presence of companion, or are endured with intense fear or anxiety
E. Disproportionality: Fear or anxiety is out of proportion to actual danger posed by situations and to sociocultural context
F. Persistence: Fear, anxiety, or avoidance is persistent, typically lasting 6 months or more
G. Functional Impairment: Causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
H. Medical Exclusion: If another medical condition exists (inflammatory bowel disease, Parkinson's disease), fear/anxiety/avoidance is clearly excessive
I. Exclusion: Not better explained by other condition
Obsessive-Compulsive Disorder (OCD) Historical Classification Note
OCD was previously classified with anxiety disorders; now classified separately in the DSM-5
Obsessive-Compulsive Disorder (OCD) Definition
Obsessions: Definition and Characteristics
Recurrent and persistent thoughts, urges, or images
Experienced as intrusive and unwanted at some point during disturbance
Cause marked anxiety or distress in most individuals
Individual attempts to ignore, suppress, or neutralize with another thought or action
Compulsions: Definition and Characteristics
Repetitive behaviors that individuals feel driven to perform in response to obsession or according to rigidly applied rules
Aimed at preventing or reducing anxiety/distress or some dreaded event or situation
Not connected in a realistic way with what they are designed to neutralize or prevent (incongruent compulsion)
Obsessive-Compulsive Disorder (OCD) Epidemiology
Lifetime prevalence: 0.3-3% (mean 2%)
Age of Onset: Typically begins in late teens or early 20s; generally gradual onset
Gender Ratio: Women = Men (though earlier onset in men)
Course of Illness: 85% chronic course, 10% deteriorating course, 2% episodic course
Obsessive-Compulsive Disorder (OCD) Etiopathogenesis
** Multifactoral Approach
Genetic Factors
12% overall risk if first-degree relative affected
This represents 6x greater risk than general population
Neurobiological Abnormalities
Increase in metabolic activity in some cortical regions (orbitofrontal cortex) and subcortical regions (caudate nucleus, dorsomedial thalamus)
Neurotransmitter/receptor abnormalities: Serotonin, norepinephrine, dopamine abnormalities supported by response to drug therapy
Occurs more often in various neurologic disorders: epilepsy, Huntington's chorea, birth trauma
PANDAS Association: Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections - tics, vocalizations, OCD compulsions. Resolve with treatment of strep (abx)
Behavioral Factors
Conditioned responses (The OCD cycle)
Obsessive-Compulsive Disorder (OCD) Comorbidity Patterns
Mood Disorders: Major depression and bipolar disorder co-occur in up to 60% of cases (can precede or be consequence of OCD)
Anxiety Disorders: In particular panic disorder and phobias, co-occur in up to 70% of cases
Tic Disorders: Tourette's syndrome; up to 50% of Tourette's sufferers also develop OCD
The OCD Cycle
obsessive thought
anxiety
compulsive behavior
temporary relief
REPEAT
Obsessive-Compulsive Disorder (OCD) DSM-5 Diagnostic Criteria
A. Core Features: Presence of obsessions, compulsions, or both
B. Functional Impairment: Obsessions or compulsions are:
Time-consuming (taking more than 1 hour per day), OR
Cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
C-D. Exclusion: Not attributable to substance or other medical/psychiatric disorder
Specifiers: Specify if with good, fair, or absent insight; delusional beliefs; tic-related
Obsessive-Compulsive Disorder (OCD)
Combined Approach: Typically involves medication and behavioral/psychotherapy (exposure with response prevention)
First-line Pharmacotherapy: SSRIs particularly effective, usually higher dosage is needed for OCD, along with longer duration
Fluoxetine
Fluvoxamine
Paroxetine
Sertraline
Note: Higher dosages of SSRIs needed compared with depression treatment
Response may be delayed: 4-6 weeks typically, average 12 weeks
Continue for 2 years
Alternative Medication: Clomipramine (tricyclic antidepressant) is useful but limited by side effects
Refractory Cases: Neurosurgical procedures (cingulotomy, deep brain stimulation)