NR 602 Final Exam questions with 100% correct answers + rationales -Chamberlain
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
primary dysmenorrhea
- release of prostaglandins during ovulatory cycles and produces painful menstruation (more flow=more pain)(no ovulation, no pain)
-Sx within 48 hours
- Tx: NSAIDs
secondary dymenorrhea
- R/t structual changes (endometriosis, PCOS, fibroids, inflammatory disease)
PCOS (Stein-Leventhal syndrome)
-persistent anovulation
-sx: obesity, anovulatory cycles, ovarian cysts, hyperandrogenism, male-pattern baldness, acne, high insulin levels, insulin resistance, menstrual irregularities, high LH, low FSH, secondary amenorrhea, infertility, obesity
- Cause: ? genetics.
- Tx: wt loss, OCPs, spironolactone, metformin (as DM preventative & improve fertility). Clomiphene citrate (estrogen receptor modulator), or human menopausal gonadotropin to produce ovulation(when desiring pregnancy)
Bartholin's cysts
- 2 glands provide lubrication during sex, 8-10mm in size, not normally palpable
- sx: dyspareunia, pain,
-tx: if chronic, may require surgery, noninfectious: sitz bath, needle-aspiration. may resolve spontaneously
- chlamydia, gonorrhea, staph,
Fibroadenoma
- most common benign breast tumor
-circumscribed lesion, solid, non-cancerous, painless, slow-growing, hormone dependent, regress after menopause, relatively moveable, non-tender
-proliferating glandular and connective elements
-giant lumps may occur
- 15-35yo
-Dx: Core biopsy or excision (definitive dx). cryoablation after dx.
- does not increase risk for brease CA
fibrocystic breast disease
-numerous small sacs of fluid surrounded by dense strands of fibrous tissue in the breast
- >50% of women have
- -tx: avoid caffeine, supportive bra, low-fat diet, evening primrose oil, NSAIDs/APAP, tamoxifen if severe
Fat necrosis of the breast
- necrotic fat cells with lipid-filled macrophages and neutrophils
- Sx: skin/nipple retraction, mass that is indistinguishable from cancer, tenderness (sometimes)
- mass ususally resolves after several weeks w/o treatment- if not, need biopsy
- r/t trauma/surgery of breast
Breast cancer
-risk: family hx, white, nulliparous, first pregnancy after 30yo, early menarche (before 12), late menopause (after 50),
- Sx: painless, firm mass with poorly delineated margins, itching, retraction, dimpling of skin,
- sx of advanced tumor: large mass, nodularity, edema, redness, skin ulceration, fixation to chest wall, breast size change, axillary lymphadenopathy that are fixed
- Tumor grading: TNM (1-3pts each)- 3-5pts= low grade, well-differentiated, 6-7= intermediate, 8-9= high grade, poor differentiated cells
- surgery done 1-2 weeks after biopsy
- ER + tumors= mets to bone, soft tissue & genital organs. ER -= mets to liver, lung, and brain
Paget's disease of the breast
- Eczematoid eruption and ulceration from the nipple. may spread to areola
- associated with underlying cancer
- uncommon
Mammography
- screening to begin 40, no later than 50.
- done every 1-2 years
- continue until age 75
STDs
-Chlamydia: purulent discharge, red, congested cervix, urethritis, salpingitis, UTI sx,(Tx: azithromycin). NAAT test
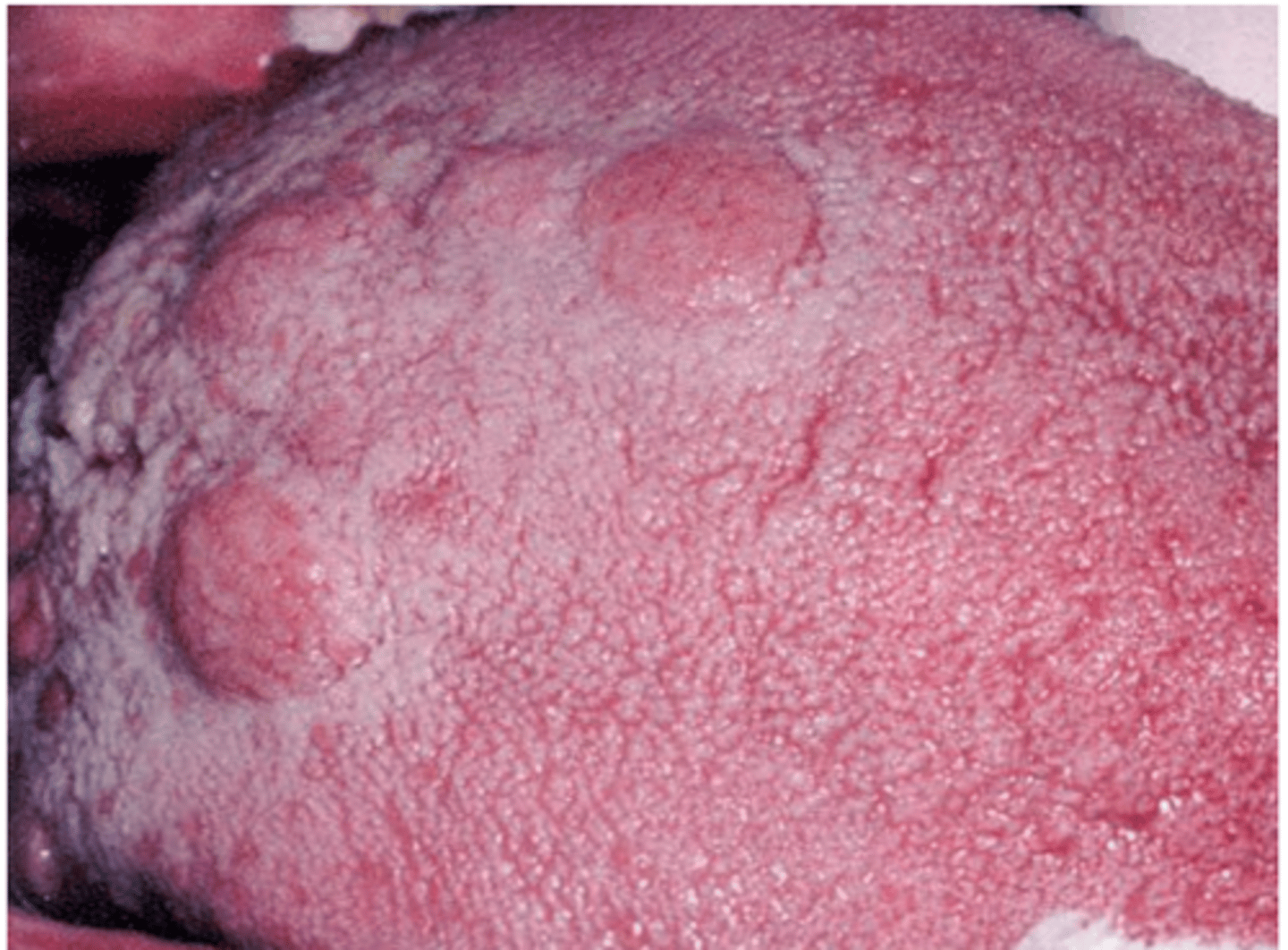
-Trich: Foamy, greenish-white discharge, strawberry-like appearance covers the endocervix and may extend to vaginal mucosa, double hairpin capillaries, flagellated organisms , friable, red cervix. protozoa (Tx: metronidazole)
-Ghon: thick, creamy discharge, inflamed cervix, urethritis, UTI sx, ( Tx: Cefixime, or ceftriaxone)
- Bac. vaginosis: gray or white d/c, "clue cells", fishy odor, pH >4.5, gram stain for dx, (Tx- metronidazole)
- Syphilis: Trep. pallidum, painless sore (indurated, papule or ulcer with raised borders) then 6 weeks later more appear, painless regional lymphadenopathy. spirochetes (Tx-penicillin parenterally) Jarisch-herxheimer reaction
Hepatitis
- B: Acute, asymptomatic, may lead to chronic carrier state, vaccination available, incubation 6w-6m. mucous membrane exposure to blood or body fluids, sx= jaundice anorexia, RUQ pain, fatigue. Tx=supportive
- C: RNA virus, no vaccine, no sx, no tx, rarely sexually transmitted, usually parenteral route (iv drug users), 1-3w incubation and 8-9 weeks to antibodies, 50% get cirrhosis
HIV/AIDS
- RNA retrovirus attaches to CD4 receptor of target cell. When CD4 <200, infections happen & AIDS dx, antibodies 12 weeks after exposure (=current infection)
- from sexual contact, or exposure to blood/body fluid or mom to baby.
-HIV highly concentrated in semen (circumcision decreases transmission)
- sx: retroviral infection: wt loss, fever, night sweats, pharyngitis, lymphadenopathy, red maculopapular rash- resolves in weeks and then asymptomatic
- Aids= specific opportunistic infection (pneumonia/ cns toxoplasmosis), neoplasia, dementia, encephalopathy, wasting syndrome rapid cervical dysplasia to cancer or CD4 <200.
-Tx: HAART & ATB prophylaxis for CD4 200-500, HAART & c-section & Zidovudine in pregnancy
Contraceptives
- Levonorgestrel IUD: Mirena, Liletta, Kyleena, Skyla (low dose & smaller- nulliparous and small women). Thicken cervical mucus & inhibit sperm motility & function & thinning endometrium. amenorrheic. prevent fertilization, not disrupt implantation. Contra- current breast CA
- Implant: progestin only. 3 years. Suppress ovulation, thick cervical mucus, alters endometrium. use backup x4 days. ovulate 3m after removal. breastfeeding ok. contra- current breast CA
- Shot: subq (more $$)or IM. progestin. Prevent ovulation reduce production of estrodiol. breastfeeding ok. reduce endometrial cancer. contgra-current breast CA. > 4 years = decrease BMD.
- COC: progestin suppresses secretion of gonatropins (LH). estrogen inhibits FHS secretion. reduce ovarian CA by 40-80%/ endometrial CA by 40-50% for 15-20 years.
Lichen Sclerosus
- most common nonneoplastic epithelial vulvar disorder
- intense pruritus, vulvar skin is thin, wrinkled, and white, with areas of lichenification and hyperkeratosis. Anterior labia minora sides agglutinate, erosions, fissures, ulcerates result from scratching. inability to retract skin around clitoris or labia, women >60
-biopsy required- thin, hyperkeratosis layer, thinning epithelial layer, plattening papillae, homogenization of stroma, and deep lymphocytic infiltration.
- Tx: vulvar hygiene, oral antihistamine @ bedtime. Steroid cream (dermovate) BID and PRN lifelong

Vulvar Lichen Simplex Chronicus
- benign epithelial thickening & hyperkeratosis from chronic irritation (from use of perfumed pads, or infection)itching, raised white lesions
- biopsy
- Tx: vulvular hygiene, sitz baths, lubricants, oral antihistamine, topical steroid

vulvodynia
- chronic pain that affects the vulva or vaginal entry, vestibular tenderness (pressure from Q-tip produces pain), no other lesions, erythema rare
- usually affects women 20-30
-tx: unprovokes= oral tricyclic antidepressants, local anesthetics
- no prevention
- needed for dx: 1) introital pain on vestibular or vaginal entry. 2) vestibular tenderness (Q-tip pressure makes pain)
- Tx: 1) pelvic floor therapy with biofeedback. vulvar hygiene, topical lido.2) if after 3 months, tricyclic antidepressant amitriptyline or gabapentin x 3m. 3) surgical therapy.
Amenorrhea (primary)
- no period by 13yo in absence of normal growth/secondary sexual development or 15yo with normal growth/development.
- Cause: gonadal dysgenesis (group of sex chromosomal abnormalities), ovarian dysgenesis (low estradiol), turner/swyer's syndrome, testicular feminization (defective androgen receptors), mullerian agenesis (vaginal absence), PCOS,GnRH deficiency
- Tx: usually cannot be made to ovulate.May use in vitro with donor oocytes
Amenorrhea (Secondary)
- cessation of regular menses for 3m or irregular for 6m.
- Cause: pregnancy, hypothalamic, pituitary , androgen disorders, galactorrhea (pituitary), sheehan's syndrome, systemic illness
- Tx: treat the disorder to stimulate ovulation. hyperprolactinemia: dopamine agonist (cabergoline), surgical therapy, if low estrogen, need replacement (OCs)
ASCUS/HSIL
- ASCUS: atypical squamous cells-undetermined significance. Most common abnormal pap result. could mean HPV infection, cyst, polyp. repeat pap, HPV test, or colposcopy
- HSIL: High-grade squamous intraepithelial lesion. CIN 2-3. Associated with HPV. May or may not progress to cancer, but is considered a precancerous lesion. usually treated aggressively.
Pelvic mass
- Benign: unilateral, mobile, cystic, smooth, < 10cm, calcification, gravity dependent layering of cyst contents
- Malignant: bilateral, fixed, solid/firm, nodular, multiple septations <2mm, ascites
- enlarging mass or with pain= immediate evaluation
- ascites or upper abd mass, abd distention= ovarian CA
- Ultrasound= benign or malignant, color flow doppler studies= vascular pattern, surgery is needed for malignancy histology
Vulvar carcinoma
- uncommon. Risk: poor, Postmenopausal (60-70) women with Hx of pruritus, bloody d/c.
- early lesions= chronic vulvar dermatitis
- late lesions= large cauliflower or hard ulcerated area in vulva
- biopsy needed for Dx
- squamous cell carcinomas
- Risk: smoking, hx of cervical CA, HPV, vulvar dystrophy, venereal disease, diabetes, obese, CV disease
- Tx: complete surgical removal
Condyloma acuminate (genital warts)
- asymptomatic white, exophytic, papillary growths, small at first, test to coalesce, affect vulva, vagina, & cervix penis, scrotum, pubis, perianal, oropharyngeal. Grow to large cauliflower masses
-cause: HPV (6 & 11)
- biopsy to rule out neoplasia
- incubation: weeks to years
- Tx: by provider: B. acid or T. acid, podophyllin in tincture of benzoin, cryosurgery, electrosurgery, laser. By pt: podofilox gel, imiquimod cream

Condyloma lata (secondary syphilis)
- wart-like lesions in genital area. rash resolves spontaneously within 2-6 weeks.
androgen insensitivity syndrome
- absence of pubic hair
- external genitalia cannot respond to androgens because the receptors are either absent or defective.
- phenotypic females lacking a uterus and a complete vagina. produce some estrogen, develop breasts
-present with amenorrhea
-inherited X-linked recessive, removal of testes
Turner Syndrome
-Xo female
- Sx: congenital lymphedema, short stature (<3rd percentile), gonadal dysgenesis, broad chest, small nipples, webbed neck, coarctation of the aorta, renal abnormalities, prominent epicanthal folds, redundant nuchal skin.
- risk for bone loss and early heart disease
- Tx: gonadal hormone therapy low-dose estradiol with growth hormone
painful bladder syndrome/interstitial cystitis
tx: amitriptyline, PT, pentosan, hydroxyzine
UTI
- e.coli (80%), then staph aureus, enterococcus, group b strep
- Tx: Empiric Nitrofurantoin, sulfa (bactrim), or ceph.
- no sulfas late in pregnancy, no tetracyclines, or TMP/SMX in pregnancy
PID
-Tx: Ceftriaxone 250mg IM single dose, plus Doxycycline 100mg PO BID x 14 days, with or without Metronidazole 500mg PO BID x 14 days
-met for recent gyn. instrumentation or BV
Pyelonephritis- Kidney infection
- one of the most common causes of hospitalization while pregnant
- presence of bacteria in urine culture with pyuria
- sx: flank pain, and/or fever, chills, n/v, CVA tenderness, dysuria
- Tx: evaluate in the hospital, parenteral cefazolin or ceftriaxone. When pt afebrile x 48 hours, may switch to PO abx x 14 days.
Skene's glands
glands located on the anterior wall of the vagina, around the lower end of the urethra
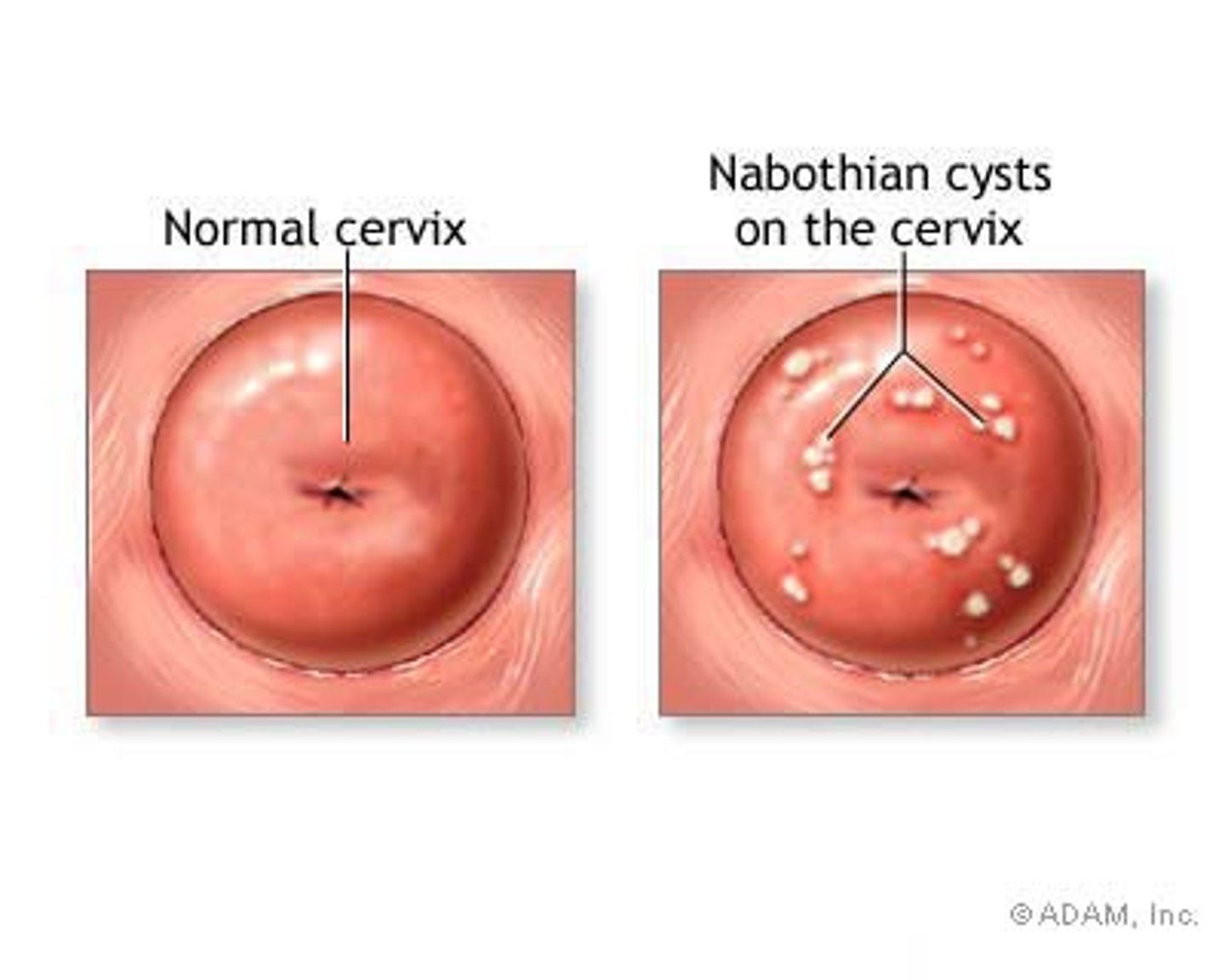
Nabothian glands/cyst
- cysts usually appear translucent or yellow and may vary in diameter from a few mm to several cm.
- usually nonpainful
- occur after minor trauma or childbirth
- asymptomatic cysts do not require treatment- painful=ablation
Bartholin's glands
- secrete clear, viscid, stringy mucoid substance with alkaline pH during sexual activity.
- if opening of the gland gets clogged, a cyst may develop.
- Sx: pain, tenderness, dyspareunia, difficulty walking with adducted thighs. inflammation.
- Tx: sitx bath, surgical drainage, marsupialization, insertion of word catheter

Current pap recommendations
- Everyone at 21 yo, regardless of sexual experience.
- every 3 years until 29 yo
- 30-65yo= pap & HPV test every 5yrs, but cytology screening alone every 3 years is ok.
- annual screening for high risk pts.
- HIV= cervical cytology every 6m after diagnosis for the first year, and then annually.
- HPV vaccination status does not change recommendations
- May DC pap a@ 65yo if pt has >3 neg results in a row, or 2 neg HPV tests in the past 10 years and no hx of cervical CA.
USPSTF Breast Cancer screening
- Biennial screening mamo 50-74yo
- with parent, sibling, or child with breast CA, may begin screening in their 40's
After sexual assault
- motile sperm in vagina x 8 hours. 2-3 days in cervical mucus
- nonmotile sperm in vagina x72 hours. x17 days in cervix. x24 hours in rectum.
- Acid phosphatase, enzyme found in semen, may be found in vaginal secretions & rectum, in case male had vasectomy
- prophylactic treatment: ceftriaxone 125mg IM + metron. 2g, azith 1g + hep B immunoglobulin IM within 14 days + EC
- HIV infection unlikely