11PSYCH Brain Plasticity and development
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
73 Terms
Brain Development During Adolescence
During adolescence there is significant development of structures within the brain that have a role in learning, behaviour, and emotion.
Cerebellum, Amygdala, Corpus Callosum, Frontal Lobe
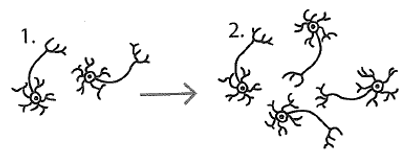
Synapse Formation – Learning
· During learning new neural pathways are either created or current ones are strengthened.
· The new pathways allowed for information to be transferred from one neuron to the next more efficiently and the more that pathway is activated the more likely it is to be strengthened and less likely that the learning will be forgotten.
· E.g. Math student taking three subjects has better ability at interpreting math info in ATAR, than someone who takes general maths - strengthening pre-existing pathways.
The Role of Brain Plasticity in Adolescence
· Circuit formation continues during childhood and by approximately age eleven in females and twelve in males the volume of grey matter is at its maximum.
· Synaptic pruning continues throughout adolescence and into early adulthood increasing brain efficiency and specialization of brain areas in response to sensory experiences.
· Loss of grey matter because of synaptic pruning progresses from the back to the front.
Cerebellum during adolescence:
· During adolescence the cerebellum continues to grow in volume with total volume being reached at approximately twelve years of age in females and fifteen in males.
· In addition to the increase in volume, synaptic pruning affects behaviour and emotion in adolescence, the influence being significant since the cerebellum, taking up only 10% of the brain volume, consists of more than 50% of the total neurons in the brain.
· Activity in the cerebellum has been linked to decision-making, reward learning (classical conditioning, operate conditioning: do the right thing, get reward, understand that the thing is good), motivation, emotional control, and processing mood. It is therefore understandable that teenagers who are yet to have a fully grown cerebellum typically display impulsive decision-making and have some difficulties regulating their emotions. (when put under CAT scan seen that there is a shrinkage or underdeveloped cerebellum) (boys have fully developed cerebellum but not prefrontal cortex therefore no impulse control)
· The cerebellum is the part of the brain responsible for balance, muscle tone and the performance of motor skills (fine motor skills (smaller muscles for fine precision movement, writing) and gross motor skills (large muscle group, kicking a ball)).
· Within the cerebellum there is an increase in the number of neurons and synapses in the cerebellum.
Corpus Callosum during adolescence:
· The thickness of the corpus callosum increases during adolescence through the process of myelination, however rather than the corpus callosum growing uniformly across the structure, various regions grow at different rates. Research suggests hormonal surges during adolescence may account for these growth patterns. (certain hormones affect different growth rate)
· Neural networks within the corpus callosum strengthen, leading to a stronger connection between the two hemispheres, behavioural and emotional regulation continue to improve. (nerve impulse transport is faster, more efficient helps with many aspects in a person)
Amygdala during adolescence:
· The amygdala grows in volume during adolescence, thought partly to be due to pubertal changes.
· In adults the pre-frontal cortex regulates the amygdala but not during adolescence as the prefrontal cortex is still developing connections between the amygdala and pre-frontal cortex. Instead of the pre-frontal cortex leading actions, based on rational and logical thinking, the volatile amygdala guides many of the autonomic actions. (e.g. why yr. 7s cry when confronted with difficult situations vs yr. 12/11 hiding their emotions)
· The amygdala is highly reactive to emotional stimuli such as the facial expressions of other people and situations perceived to be stressful. This leads to teenagers being more likely to misinterpret emotions of others and social cues and as a result get into accidents or behave inappropriately (not thinking before acting). Another example of an immediate reaction to emotions such as fear is aggressive behaviour towards other people. (girls cry without knowing why, hormonal changes in amygdala and prefrontal cortex)
· A paired structure (meaning there is one on either side) that is part of the limbic system (system of body that controls emotion). The amygdala is involved in mediating many aspects of emotional learning and behaviour.
· In adolescence the amygdala becomes more active. (underdeveloped amygdala = serial killer behaviours, limits on fear)
· If there is damage or it is underdeveloped people will not be able to learn fear – they will be unable to associate something dangerous with the feeling of fear.
Amygdala
a collection if nuclei deep within each temporal lobe that play a role in emotional response (including modulation of fear) and the immediate behavioural reactions as a response to emotion. (anger, fear, violence)
Frontal Lobes during Adolescence:
· Evaluate emotions and use rational thinking when referring to past experiences before responding in a conscious manner. (improving rational thinking, understanding of consequence) This control of voluntary behaviour is not characteristic of teenagers as these lobes are one of the last regions of the brain to mature. The frontal lobes are not completely myelinated until around the age of 30 therefore teenagers have less white matter (myelinated axons) in this region compared to adults.
· Myelinated neurons improve connectivity between parts of the brain and with the frontal lobes not yet fully connected the reduced ability to integrate information from brain regions affects cognitions and emotional processes. The connection between frontal lobes and amygdala for example is still strengthening during adolescence therefore teenagers may exhibit limited impulse control, poor decision making and planning and reduced emotional regulation (typically leading to mood swings).
Pre-frontal cortex during adolescence:
· the layer of the frontal lobes just beneath the forehead. They continues to undergo myelination during adolescence leading to an increase in white matter. In addition to myelination, synaptic pruning continues in the pre-frontal cortex during this period of development, reducing the amount of grey matter and allowing for increasingly complex and efficient connections to be created in the brain.
Pre-frontal cortex development during adolescence
· Synaptic pruning begins at the back of the brain and continues forward with the pre-frontal cortex being the last part of the brain to develop. This region is responsible for problem solving, attention and the ability to predict consequences of behaviour by referring to past experiences and assessing whether these behaviours will lead to reaching a desired goal. This makes it easier to understand why some teenagers do not seem to assess potential risks and end up engaging in risky and dangerous behaviours.
· The ability to regulate emotion continues to improve during adolescence as does the ability to recognize emotions in other people.
Overview of Frontal Lobe
· Includes the prefrontal cortex and leads to an improvement in motor movement and higher order thinking.
- Focusing, organizing, prioritizing
- Linking actions to logical consequences
- Controlling impulses, regulating emotions, and moderating behaviour
- Balancing short term rewards with long-term goals. (experiment of child with waiting for six marshmallows or having one straight away, because this section is not fully developed)
· Not fully developed until the mid-twenties
Plasticity of the brain
· refers to the way it changes in response to stimulation from the environment. Due to experience and learning, by altering its function and structure. The ability of neural connections to grow and reorganize.
The process of plasticity
· The process of plasticity occurs at the synaptic connections in the brain. Brain continuously creates new connections in response to experiences.
· Plasticity is necessary for learning to take place and is present throughout a healthy person’s lifetime.
· Changes can be due to learning new skills, development from infancy to adulthood, or traumatic events like strokes.
· Infancy sees rapid growth in synaptic connections, followed by synaptic pruning in adulthood.
Neuronal Cell Death:
Direct and indirect factors like brain swelling can lead to cell death, requiring the brain to compensate for damaged areas.
Functional Recovery
Healthy brain areas compensate for lost or damaged areas through functional reorganization. Functions of lost areas are taken over by other healthy areas.
Neuronal Pathways:
New information leads to the formation of new pathways, strengthening with use and weakening with disuse (synaptic pruning).
Neuroplasticity
Refers to the brain’s ability to change throughout life. Occurs at 3 different points:
- Fetal and early stages of life: when the immature brain organizes itself. Growth of dendrites and axons, Synaptogenesis: formation of new synapses, pruning: death of certain neurons and removal of connections that aren’t useful., Myelination: formation of the myelin sheath.
- Adolescence and adulthood: whenever something new is learned and memorized.
- Brain injury: to compensate for lost functions of maximise remaining functions.
Developmental plasticity:
The ability of neural connections in the brain to reorganize in response to sensory input from the environment. The ability of synapses to be modified in an infant or child.
Adaptative plasticity Info
• Developmental Plasticity will decrease with age, but areas of the cerebral cortex retain plasticity throughout life-adaptive plasticity.
• Brain changes/develops, new experiences shaped by learning and experience.
• Stem cells create neurons throughout life, enabling the brain to adapt and cope with any new experience.
• E.g. a stroke patient suffering from Broca’s aphasia due to damage to Broca’s area in the left frontal lobe. Spontaneous speech is initially diminished over time the brain experiences heighted plasticity, neural connections are rearranged and re-established. Speech therapy has the greatest impact on rehabilitation, helps reenforce the rewiring and enhance the plasticity.
• Infants who experience brain injuries recover more fully than adults who experience similar injuries because the brain’s plasticity is greatest during the first few years of life. As brain regions are not yet specialized in the developing brain, other areas of the brain can take over the function of damaged areas.
Adaptive Plasticity-Response to Injury
• allows the brain to also ‘rewire’ (or reorganise) after damage to compensate for a lost function or to maximise existing functions.
• Brain constructs other neural pathways to compensate for functional loss.
• Depending on the type and extent of brain injury, plasticity may also allow the damaged brain neurons to repair or regenerate.
Functional Recovery
Ability of unaffected brain areas to compensate for damaged areas after trauma.
· Healthy areas take over functions of damaged areas.
· Process may require rehabilitative therapy after initial adaptation.
Brain's Adaptation:
· Rewiring and reorganizing by forming new synaptic connections near damaged area.
· Activation of secondary neural pathways to maintain functioning.
· Structural changes like axonal sprouting, blood vessel reformation, and recruitment of homologous areas.
Factors Affecting Recovery
Age and Gender: Younger individuals, especially children, show higher resilience and recovery from brain damage.
Women tend to recover better from brain trauma than men.
Rehabilitation Importance: Access to focused rehabilitation efforts, like constraint-induced therapy, aids in functional recovery by promoting neuronal reorganization.
Developmental Plasticity Info
Generally, an infant or a child’s brain will have more plasticity than an adult’s brain. This is referred to as developmental plasticity (the ability of synapses to be modified)
- Developmental Plasticity: fetal, babies, children, and adolescents
- Adaptive plasticity: throughout life.
Prior to birth and for the first years of life a child’s neurons are quite flexible in terms of their function. The development of the nervous system starts before birth when the brain and spinal cord are formed. It then goes through 5 stages:
Proliferation
- Proliferation is the growth and division of cells, including neurons that leads to the increase in total cell number.
While most neurons are already formed when the infant is born, some neurons are still created during infancy
Migration
• While an infant is born with around 100 billion neurons, there are still neurons being generated after birth from deep inside the brain.
• Newly generated neurons move throughout the brain until reaching their final position; this positioning allows for connections between neurons (neural circuits) to be made.
• Neurons migrate by following chemical trails laid down by other neurons or by moving along scaffolding fibres in the brain.
• Research has shown that the migration of neurons ends around the age of 5 months.
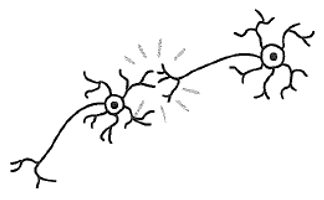
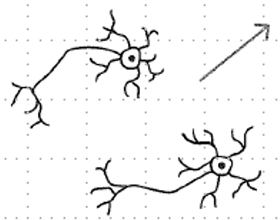
Circuit formation
• After neurons have migrated, they can form neural circuits whereby neurons send electrochemical messages between each other. These connections can be within clusters of neurons as well as over larger distances within the brain.
• During infancy neural circuits develop rapidly especially in the primary sensory cortex and primary visual cortex.
Synaptic pruning
• As infants are born with more neurons than required neurons that do not form active neural connections with other neurons die.
• Synaptic pruning increases the efficiency of the nervous system by allowing remaining neural connections to strengthen and grow in complexity.
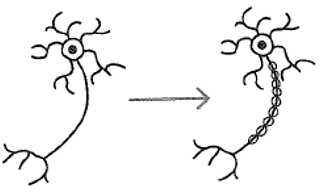
Myelination
• fatty substance called myelin starts growing over the axons of neurons insulating neural connections and allowing for faster and more efficient nerve impulse travel throughout the brain.
• Myelination contributes to the dramatic brain growth typical in infants.
• Myelination begins in the spinal cord then in the hindbrain, midbrain, forebrain and finally in the peripheral nervous system.
• The greater the number of myelinated neurons, the more efficient and faster the neural pathways work in that part of the brain.
• The more developed – or myelinated – the brain becomes, the more you can integrate information from multiple brain areas.
Research Studies on plasticity
McGuire Study: London taxi drivers showed increased grey matter volume in the posterior hippocampus due to memorization demands, indicating brain plasticity.
Den Le Case Study: Infant EB underwent hemispherectomy but recovered speech abilities over time, showcasing brain's ability to reorganize functions.
Research by Ku et al. (2014): Compared control group with video game training group (Super Mario). Video game training led to significant increase in grey matter in brain areas related to skills used in the game.
Implications and Further Research on plasticity
Physiotherapy Benefits: Understanding brain recovery aids in helping clients regain lost functions and independence.
Individual Differences: Cognitive reserve, IQ, and educational background influence recovery outcomes post-trauma.
Cognitive development
• refers to changes in the ability to think and reason which includes changes in language.
Verbal fluency:
• The ability to produce words that are retrieved from memory. Whisk 5 test.
Tip of the tongue phenomenon:
• An individual knows what they would like to say but are unable to recall the specific word required. If it’s a one off its fine, but if its common there may be a cognitive issue.
Prenatal: Conception-Birth cognitive developments
• Unborn babies of 30 weeks listen to their mothers talk and learn speech sounds. (Attachment, distressing if they can’t hear their mother’s voice}
Infancy: Birth-1 Year cognitive devlopments
• Shows a desire to communicate with others.
• Infants can read and react to facial expressions from their caregivers.
• Infants use vocalisations (cooing), babbling, cries, gestures, and facial expressions to communicate their needs. (correlation studies done on infants’ interpretation of facial expressions, mother smiles, child smiles, affecting feeling of warmth and support)
Childhood:1-12 years cognitive developments
• Around age one babies may use partial words (da instead of dad) and vocabulary rapidly grows to around fifty words. cognitive development of brain for language Broker’s and Wernicke’s area.
• By age 3 vocabulary includes around 200 words, sentences of three or four words are used. Basic communication.
• By age 5 children can speak clearly, tell simple stories, and understand basic grammar rules.
• By age 11 children have a vocabulary of around 19,000 words. (different depending on individualistic or collectivist cultures)
Adolescence: 12-20 years) cognitive developments
• Improvement in language comprehension.
• Able to comprehend abstract language such as similes and idioms.
• Vocabulary continues to increase.
• Impediments e.g. terrets become less significant due to neuroplasticity.
Early adulthood: 20-40 years cognitive developments
• Improvement in the knowledge of words and their meanings.
• Verbal fluency starts to decline after age 35.
Middle Age: 40-65 years cognitive developments
• Tip of the tongue phenomenon increases with age.
• Improvement in the knowledge of words and their meanings (wisdom)
• Verbal fluency continues to decline.
Old Age: 65+ cognitive developments
• Tip of the tongue phenomenon continues to increase.
• Speed of language processing declines (Wernicke’s and Broker’s area)
• Difficulties with language production may occur-slower speech, increase number of fillers (example ah, er) and pauses in speech.
• Verbal fluency continues to decline.
Social and Emotional development,
also known as psychosocial development, encompasses changes in a person’s view of themselves, their emotions, and their relationships with others.
Self-awareness:
· the ability for an individual to observe their own thoughts, emotions, and behavior’s
o E.g. – knows what annoys them, children won’t know until it happens, whereas adolescences can predict, and how to emotionally regulate.
o Understand ‘who you are.’
Self-concept:
· the view an individual has about their beliefs, likes, and dislikes and strengths and weaknesses.
o Can affect people and lead them to negative places if their belief in themselves is negative.
o Links into self-identity.
o Know ‘who you are.’
The domains of development interrelate and may be more dominant in some
Social Development:
· Refers to how well a person can function in groups.
· During a child’s social development, they need to be able to change/adapt their behavior’s so that they can accommodate and work with other people withing a social context.
Prenatal Stage – Conception to Birth social emotional development
· Some research has suggested that the fetus can sense and react to their mother’ emotions.
o Mother with mental illness/anxieties while pregnant, and when the baby is birthed, it is anxious.
Infancy – Birth to 1 year social emotional development
· Stages:
o 2 months infants start smiling at people.
o 4 months like to play with others.
o 6 months, start responding to the emotions of others.
o 9 months is clingy with primary caregiver.
o 1-year plays games (such as peek-a-boo), has favorite people and is shy around strangers.
· Imitate facial expressions of others.
· Forms attachments with primary caregivers – attachment is very important.
o Positive attachment
o Disordered attachment
· Infants give and accept toys to each other.
· The first emotions recognized in babies are anger, sadness, fear, and joy.
· Cognitive links in, in infancy understand rules, fairness in rules in games (such as peek-a-boo)
15 months – 2 years social emotional development
· Between 15 months and two years (around 18 months) of age children begin displaying self-awareness by recognizing themselves in a mirror. The rouge test is used to assess whether a young child can recognize themselves in the mirror.
§ Linked to growth in cognitive ability.
· Picture themselves as ‘central characters.’
2 years social emotional devlopment
· At age two children show affection for those they are familiar with, engage in pretend play, will have temper tantrums and play alongside children (rather than with them) as they haven’t developed social ques and how to interact with others.
5-6 years social emotional development
· Cooperate with other children, take turns in games, show a range of emotions, tell people about their interests, and play along with other children.
· Develop self-concept as this develops, they show complex emotions such as surprise, shame, guilt, embarrassment, and emotional responses such as jealousy.
· Self-esteem develops and is generally high and then starts to decline around age 12.
· Children between 6-12 form relationships with people outside of their family.
Adolescence (12-20 years) social emotional development
· 12-year-olds are getting better at regulating their own emotions.
· Adolescents have an increased understanding of their self-concepts. (Challenging authority figures that may challenge their own self concepts/beliefs)
· Mood becomes unpredictable. (hormonal changes and adaptive plasticity)
· More time is spent with friends than with family. (links understanding of self-concept) (friends with people who support and strengthen self-concept)
Early Adulthood (20-40 years of age) (love and work era) social emotional development
Intimate relationships tend to form in the mid to late twenties (close friendships or romantic relationships).
Dependence on family decreases. (move out of home, further study etc.)
Middle Age (40-65 years of age) social emotional development
· Decrease in negative emotions (example anger and an increase in positive emotions like contentment).
· Individuals may experience a mid-life crisis where they desire to feel youthful, want to spend more time alone, or wish to spend more time with particular people.
· 51 is the average age women experience menopause which is when mood swings can occur.
Older Age (65+ Years of Age) social emotional development
· It has become common to have smaller and tighter social networks.
· Life experiences have allowed for greater regulation of emotions.
· Elderly adults become more dependent on others and may feel depressed, shame and guilt due to this dependency.
· Maintaining an active social life increases feelings of self-worth and self-esteem.
We study lifespan psychology
· To offer an organized account of development across the lifespan.
Purpose of Lifespan Psychology
· Research shows that what happens at an early age affects a person later in life, often affecting other areas of a person's life.
· Example: attractive young people generally develop good self-esteem, giving them better self-esteem than that of the public as older adults.
Children who are abused are more likely to abuse children as adults.
Motor skills
are skills that enable the movements and tasks we do every day. Learning these skills is a crucial part of child development. These skills enable the movements children need for everyday tasks, from playing and feeding themselves to moving from place to place.
Typically, children develop certain skills at specific ages, but not every child will reach milestones at precisely the same time. A child with motor impairments has trouble moving in a controlled, coordinated, and efficient way.
Motor development occurs in an orderly sequence
infants move from reflexive reactions (e.g., sucking and rooting) to more advanced motor functioning.
This development proceeds in a cephalocaudal (from head-down) and proximodistal (from centre-out) direction. For instance, babies first learn to hold their heads up, then sit with assistance, then sit unassisted, followed later by crawling, pulling up, cruising, and then walking.
Fine motor skills
involve the small muscle movements of the body, for example handwriting which uses small muscles in the hand.
require a high degree of control and precision and use the small muscles of the hand or wrist (such as using a fork or crayon).
inclove manual dexterity and often require coordinating movements of the hands and fingers with the eyes, which is known as hand-eye coordination.
Components include griping and manipulating objects, using both hands for a task, and using just the thumb and one finger to pick something up rather than the whole hand.
Gross motor skills:
involve the large muscle movement of the body, for example, walking, which uses the large muscles in the legs.
movements involving large muscle groups are generally broader and more energetic than fine motor movements.
Some milestones involve eye-hand coordination, such as throwing or catching a ball.
Milestones
are behaviours that indicate typical stages of growth and development. Milestones occur at every age. Gross and fine motor milestones occur within a range of time, so list should be used as a guideline as each child develops at their own pace.
Prenatal: Conception to Birth fine and gross motor skills
· By 14 weeks the fetus can curl their toes, suck their thumb, and move their arms and legs. (gross motor movement with little amount of control)
· Small muscles in the face are used to smile and grimace.
Infancy: Birth to 1 Year fine and gross motor skills
· Survival reflexes:
· Primitive reflexes:
Gross motor skills: used when babies hold their head up when lying on their stomach, when they roll over, crawl, sit without support, stand up and walk.
Fine motor skills are used when small muscles in the face create facial expressions.
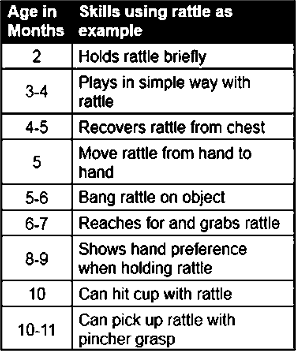
Fine motor skills are used when the baby grasps reflexively anything that touches the palm of their hand when they pick up items between their index finger and thumb (pincer grip) and poke with their index finger.
Every basic motor skill (any movement ability) develops over the first two years of life.
The sequence of motor skills first begins with reflexes involuntary movements in response to stimulation, and some are necessary for survival.
These include the breathing reflex, or the need to maintain an oxygen supply (this includes hiccups, sneezing, and thrashing reflexes), reflexes that maintain body temperature (crying, shivering, tucking the legs close, and pushing away blankets), the sucking reflex,
Other reflexes are not necessary for survival but signify the state of brain and body functions. Some of these include: the Babinski reflex (toes fan upward when feet are stroked), the stepping reflex (babies move their legs as if to walk when feet touch a flat surface), the palmar grasp (the infant will tightly grasp any object placed in its palm), and the motor reflex (babies will fling arms out and then bring to chest if they hear a loud noise).
These movements occur automatically and are signals that the infant is functioning well neurologically. Within the first several weeks of life, these reflexes are replaced with voluntary movements or motor skills.
survival reflexes
Meet physical needs-breathing, sucking, swallowing, blinking. Allow for child to live.
primitive reflexes
May be vestiges (things that happen that like to primitive ancestors (past organisms)) of earlier evolutionary stages: Grasping, stepping, Babinski (reflex of toes expanding out when foot is touched lasts until 2 years old, if lasts after it is abnormal, common test to check child’s development).
Childhood: 1-12 years (primary school) fine and gross motor skills
· Gross motor development correlates to cognitive development, especially important to stimulate the brain. Painting shows representation of cognitive development and symbolic representation.
· Limbs lengthen.
· Brain develops (increase in myelin/myelination) (90% by age 6)
· The skeleto-muscular system strengthens.
· Due to greater gross motor movement more injuries occur during this developmental stage because they are exploring.
Children of one to two years of age use fine motor skills when using a spoon, scribbling with a pen, unzipping zippers, and painting. (Manipulative skills improve)
When children draw it is the precursor to writing
Gross motor skills are used to walk up steps, run, kick, or throw a ball and climb on furniture.
By age 5 children use gross motor skills to hop, swing, catch and bounce a ball, ride a bike, and run. Fine motor skills are used to turn pages of a book, using scissors and writing.
Adolescence: 12-20 years fine and gross motor skills
• Adolescents should be able to use fine motor skills to sew, write, draw, and play an instrument requiring fine muscle coordination.
• Gross motor skills become developed enough to play adult sports.
Early Adulthood: 20-40 years fine and gross motor skills
• Motor skills operate at their best.
• Good control over fine motor movements.
Middle age: 40-65 years fine and gross motor skills
• Older adults find it more difficult to learn and maintain a new motor skill than younger adults (example using a walker to get into a car with no prior experience using a walker.)
Older age: 65+years fine and gross motor skills
• Control over fine motor movement declines.
• Gross motor movements are performed slower.
• Complex motor tasks require more brain activity than they are used to.
Fine motor control requires:
Awareness and planning.
Coordination.
Muscle strength.
Normal sensation in your hands and fingers (or feet and toes).
Precision (dexterity).
Importance of fine motor skills
· Tasks that are important for independence and self-care.
· For a child, fine motor skills are important for doing schoolwork, like drawing and writing. Several work-related tasks involve fine motor skills, too — like using construction tools or a computer or performing surgery.
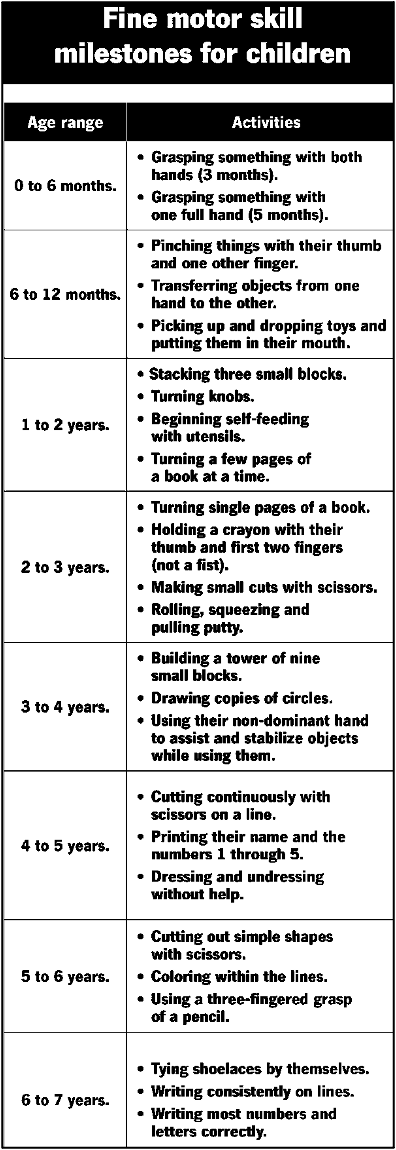
What are fine motor skill milestones?
· Behaviours that mark stages of typical growth. Children all develop at their own pace. However, most children pass through specific changes at roughly the same time as they get older.