medchem exam 2 ADMET 2
1/49
Earn XP
Description and Tags
march 30th class, 10, all done
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
dose formula
f(time (of exposure), []); think about how stable it is when exposed - repeated doses, or one dose and then wait, depends on ADME
risk assessment
This discipline bridges the intricate relationship between a drug's physical and chemical properties, its formulation, delivery, and the biological systems it interacts with. By focusing on the absorption, distribution, metabolism, and excretion (ADME) processes, biopharmaceutic risk assessment provides critical insights that guide the optimization of drug bioavailability and therapeutic effectiveness, while mitigating safety concerns.
transporters role in excretion
specialized transporters - diff kidney cells look different, diff face that is in direction of urine, diff to blood
blood and drugs
plasma cells - contain proteins that can bind drugs; free drug amount - unbound; the more protein binding - the less efficient effective drug concentration at the target site; drug unbound to protein: plasma [] == effective []
how to see if a drug is viable in terms of blood []
use serum which also has proteins - can see effective [] then
St Johns Wort descr
herbal compound, inhibits drug availability, induce P-glycoprotein and intestinal and liver CYP3A4
High metabolism, lower drug availability
point of toxicology
to find what else a drug can do- side effects, how it can be harmful
how to find MEC
usually tested in animals and then approximated to humans, does not work 100% though; different again with children
phase I clinical studies how
do not take the min effective dose, go slowly and build it up, ONLY CARE ABOUT dose finding/safety, PK/PD, not effectiveness yet!! 20-100 healthy volunteers
animal timelines
Acute: 14 days, chronic: 90 days, carcinogenicity: 2 yrs, reproductive/developmental
LD50 test
lethal dose 50%, test to determine the single dose of chemicals that would kill half of the animals exposed to it
comparative toxicity index
allows to compare relative toxicity of compounds for the first time - a lot of appeal to government regulators
phase II clinical trial
100-300 patients, efficacy, safety
phase III clinical trials
300-3000 patients, efficacy, safety, more people
clonal cell models
each represents a unique patient/animal/tissue; cell models + metabolism/transporters = nuclear receptors, signal transduction, stress response pathways, immune system, etc
genetic variation and drug action (3)
drug transporters (eg P glycoprotein, variability in drug absorption/distribution/elimination)
drug metabolizing enzymes (eg P450s, variability in drug metabolism, side effects/toxicity)
drug targets (eg receptors, variability in drug effects)
SNPs in drug discovery (3)
SNP variant causes of disease (eg LH receptor), SNP variant less/not sensitive to drug, SNP variant modulates drug response indirectly
how to adjust drug [] based on patients metabolism
if poor metabolizer - lower drug []
if higher metabolizer - higher drug []
Multi drug resistance gene
MDR-1: P glycoprotein (PGP), in cancer cells/intestine/BBB; pumps substance out of the cell - protects against toxic metabolites; many drugs are PGP substrates (eg cancer resistance, limits oral availability, limits brain penetration)
what else do you need to consider for side effects
metabolites - eg from an active drug can have an inactive metabolite, an active metabolite and a reactive intermediate that leads to an inactive metabolite but also through reaction w/ cellular macromolecules can be bioactivated into toxicity
genetic variations of P450 enzymes and the results
deletion in gene - no enzyme - no metabolism
SNPs in gene - ““ , unstable enzyme - reduced metabolism; normal enzyme - normal metabolism; altered substrate specificity - other metabolites possibly formed
duplicate or multiple copies of gene - higher enzyme levels - increased metabolism
multicopy P450-2D6 genes effect on plasma kinetics
extensive metabolizers
look at diagram
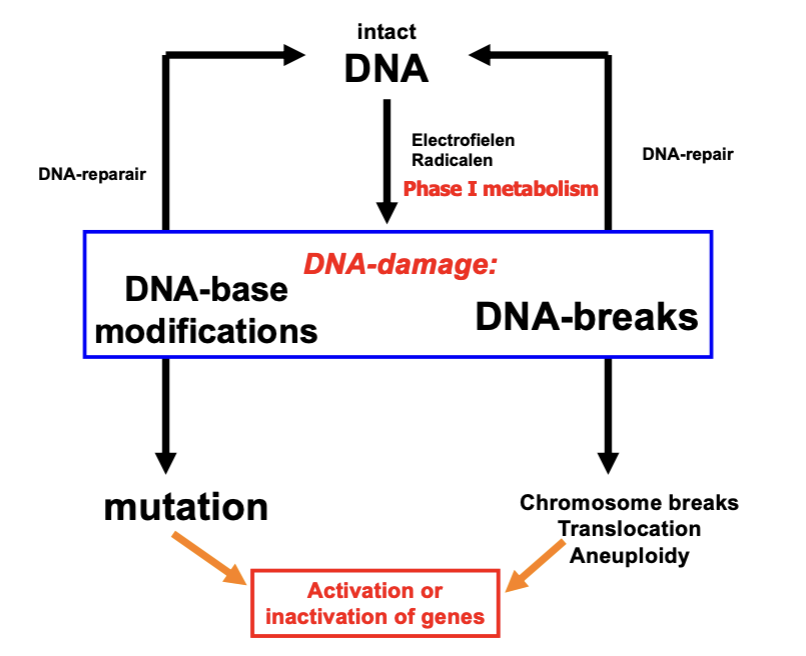
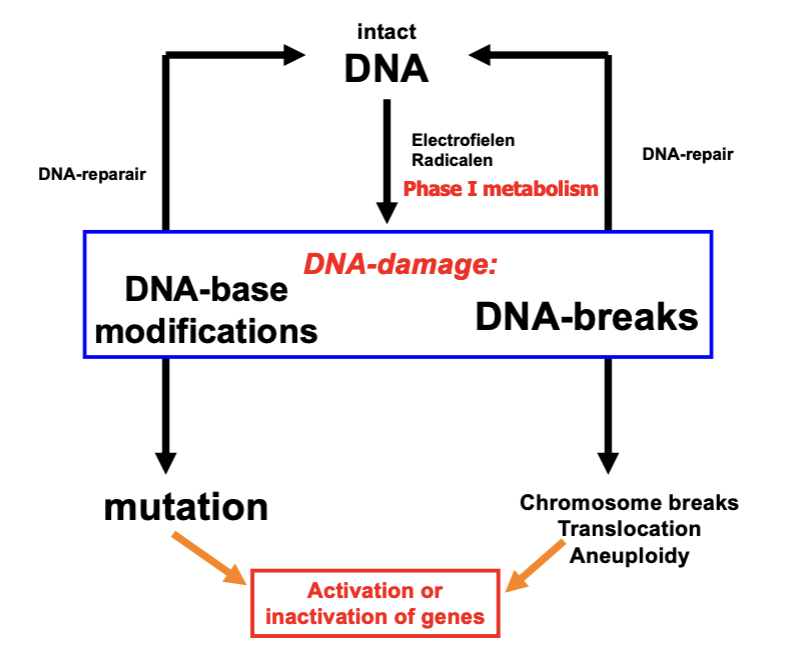
what can lead to activation or inactivation of genes after diff types of DNA damage
DNA base modifications → mutation
DNA-breaks → chromosome breaks, translocation, aneuploidy
how to end up w/ intact DNA after diff DNA damage
DNA base modifications - DNA repair
DNA-breaks → DNA repair
intact DNA through elecrophiles, radicals or phase I metabolism can lead to DNA damage again
AMES test descr
genetically engineered Salmonella (bacteria), site-directed mutation or frameshift-mutation in gene for protein involved in histidine-biosynthesis, unable to grow in histidine-free medium (bc histidine is an essential aa), after exposure to mutagen MUTATION to functional gene: growth in histidine-free medium
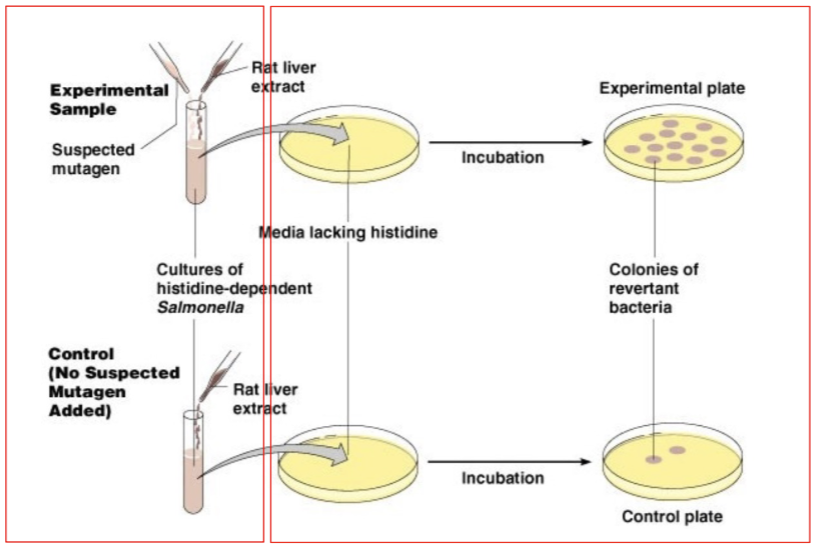
what is this
ames test
test systems (3 catergories and many types (7:1:)
animals: apes, dogs, rat, mice, fish, flies, worms
bacteria
in vitro cell systems: cell lines, primary cells from donors, iPS cells from donors, complex cell systems (eg organs on a chip)
pros/cons of whole animal models (3, 4)
pros: complete physiological system, generational studies possible, genetic manipulation possible (KO animals)
cons: adverse drug rxns often diff than huamns (30-50% of false negatives, also false positives), valid ethical concerns, expensive, not well suited to molecular investigations at cellular level
pros/cons of human based in vitro systems (2: 8)
cons: incomplete/reductionist physiological system, easy to do bad experiments
pros: human derived (although cancer cells can be very different from normal), no animal suffering, potentially cheaper and quicker, applicable to high through-put, ideally suited to molecular investigations - much deeper mechanistic info, genetic manipulation easier than in whole animals, can capture human population variation, can study human genetic diseases directly
IC50 descr
50% inhibition of activity (amount of enzyme activity needed for)
gold standard for tests
primary human cells - eg liver cells from liver biopsy
primary human cells pros/cons (3:5)
pros: already differentiated, mortal - therefore “normal” cell cycle, epigenetic imprint of the donor prevails
cons: dedifferentiated during culturing, limited donor data, limited expansion possibilities, limited availability, unique source
human cell lines pros/cons (3:)
pros: unlimited lifespan, easier to standardise, high reproducibility
cons: may have gained/lost characteristics, may be altered due to immortalisation, genetically less stable
what is needed for iPSCs
transfect adult somatic cells with Yamanaka factors
iPS cells pros/cons (4:4)
pros: mortal, represents specific indivs, multiple target cells possible, genetic background usually known
cons: elaborate differentiation protocols, need for characterisation every differentiation, not as good (yet) as primary target cells, loss of epigenetic imprint likely
iPSCs; continous cell lines from (living) donors (5)
relatively simple to generate (also from non invasive sources like urine), large biobanks available, genetic background of donor maintained (unlike cancer cells), cells mortal w/ normal cell cycle characteristics, can perform coculture w/ autologous cells
3 egs of human in vitro models
liver, intestine, lung
can protein damage, DNA damage and reactive chemicals/metals lead to?
sensor proteins → effector proteins → stress responses
3 lines of defense after stress/drug/metabolite/ROS
1st line: drug metabolism - basal expression of genes co-ordinating cell defense, phase II enzymes, antioxidant proteins
2nd line: antioxidant response, induction of genes co-ordinating cell defense: phase II enzymes, antioxidant proteins, Nrf2 response
3rd line: apoptosis - suicide of the cell
finally - necrosis
oxidative stress response
oxygen radicals/reactive metabolites → (in cytosol) Keap1 (sensor) and Nrf2 (effector) → stress response → (in nucleus) Nrf2, upregulation of protective enzymes
what is Nrf2
transcription factor
HERG channel - Torsade de Pointes decsr
most common cause of withdrawl/restriction of drugs, prolongation of QT-interval via interaction w/ HERG K+ channel - irregular heart beats, acute cardiac arrest → sudden death; need to test for it to get approval for your drug
2 important transporters
BSEP and MRP
MPR2 descr
export of conjugates of lipophilic substances w/ sulphate, etc.
when is pharmacogenomics relevant
at all stages of drug discovery: absorption (P-glycoprotein), metabolism (cytochrome P4502D6), pharmacology (receptors), etc
pros/cons personalized medicine
select right patients for clinical trials, give patient right drug → better response of drug treatment → better compliance, BUT with smaller patient populations will huge costs of development be covered
DDI long
drug drug interactions
important note about PH
large interindividual differences in pharmacokinetics
take home messages toxicology (3)
new opportunities for human-based cell models (replacing animal studies), in silico models keep improving (also PK/PD), animals still only real-life physiology model available w/ all vital organs and immune system