Ortho 10 - Introduction to Orthognathic Surgery (Dr. Salam)
1/135
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
136 Terms
True
T/F: Orthodontics alone can provide dental correction but can not alter underlying disharmony
Before and during the circum-pubertal growth spurt
When are growth modification appliances most effective?
Children with skeletal discrepancies
In which patient population are orthopedic growth modification appliances primarily used?
Orthognathic surgery combined with orthodontics
What is the preferred treatment for a severe skeletal discrepancy in an adult?
Adults have completed skeletal growth
Why are growth modification appliances generally ineffective in adults?
No - need to look at other factors (ex: skeletal maturity through CVM or hand-wrist)
Does chronological OR the level of dental development demonstrate sufficient correlation with individual maturational development to provide adequate basis for the timing of therapy?
- Chronological age
- Dental age
- Secondary sexual characteristics
- Peak height velocity
- Indicators from Hand wrist radiography
- CVM indicators
- Serial cephalometric tracings super impositions
What are the seven biological indicators of skeletal maturity?
True
(Deviations were found between chronological & skeletal age, from Handwrest radiograph, in both male and female KIDS - Chronological age can be a misleading piece of information)
T/F: Neither chronological nor the level of dental development demonstrate sufficient correlation with individual maturational development to provide adequate basis for the timing of therapy
Skeletal age
What can lend itself to more accurate, thereby more clinically beneficial results: skeletal or chronological age?
18 months (+ or - 3 )
Growth spurt was _____ months earlier in girls than boys
- C2
- C3
- C4
Skeletal maturation can be assessed by evaluating the morphology of which cervical vertebrae?
- Hand wrist radiography
- Cervical vertebral maturation
What are two indirect method of assessing growth completion?
G) Serial cephalometric tracings super impositions
Of the following, what is the best indicator of skeletal maturity?
A) Chronological age
B) Dental age
C) Secondary sexual characteristics
D) Peak height velocity
E) Indicators from Hand wrist radiography
F) CVM indicators
G) Serial cephalometric tracings super impositions
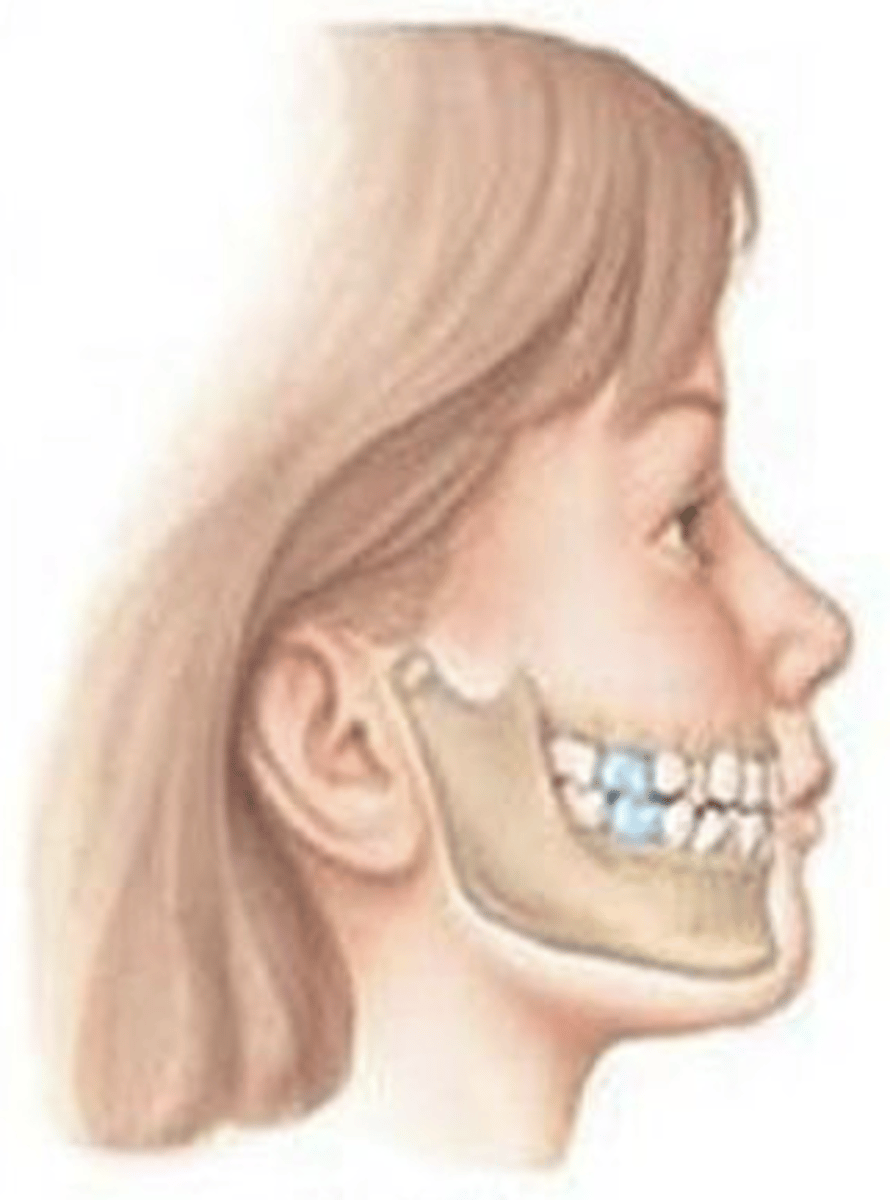
Class I
ID the occlusal classification:
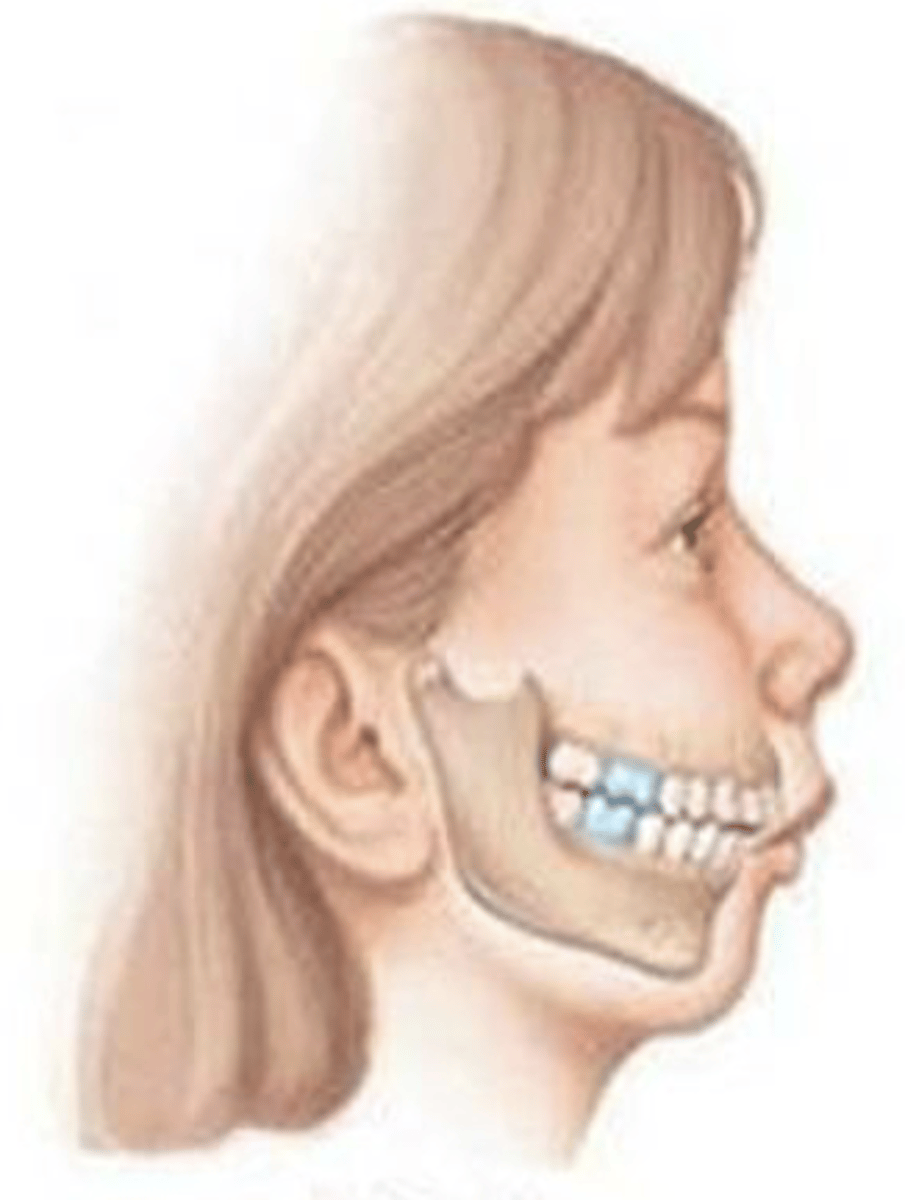
Class II
ID the occlusal classification:
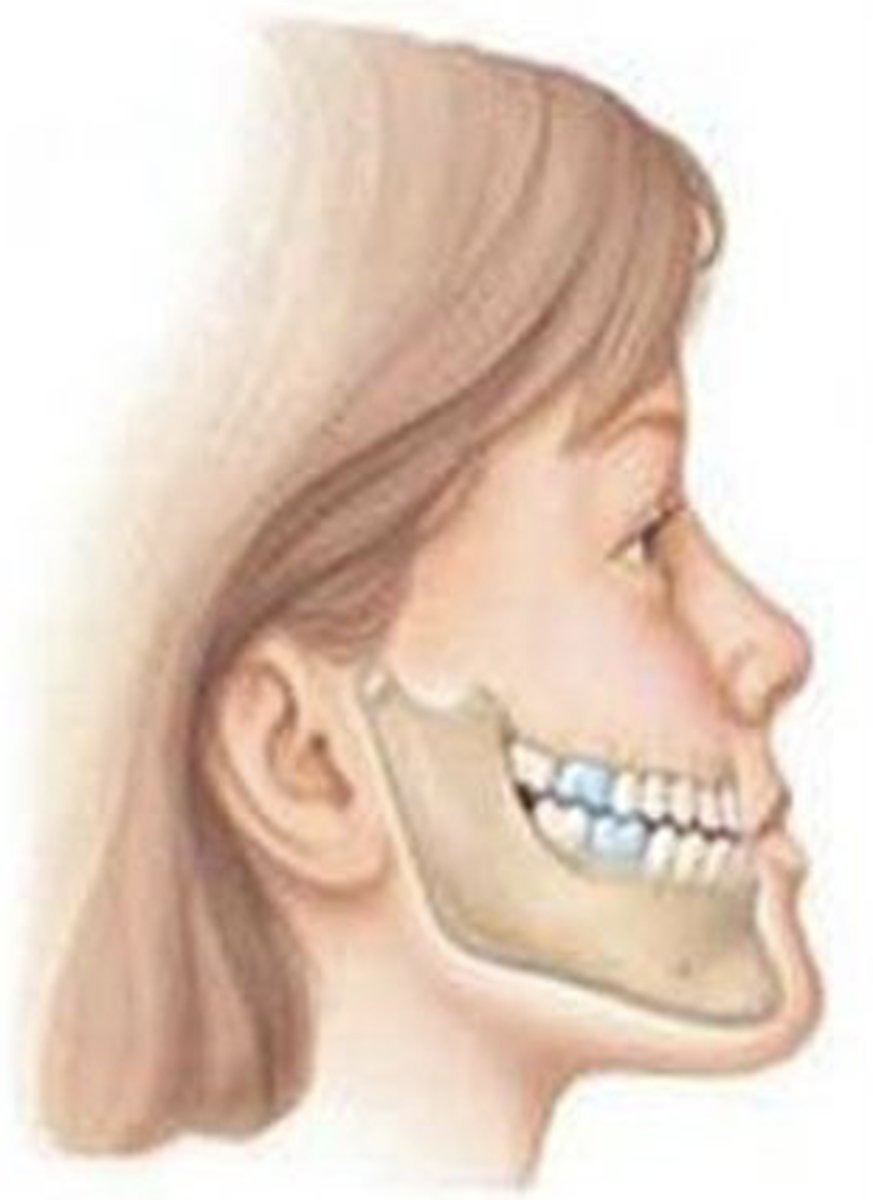
Class III
ID the occlusal classification:
- Facial profile divergence
- Desire for soft-tissue/aesthetic improvement
What are the primary reasons for considering an orthognathic approach?
True
T/F: Since soft-tissue changes are inherent to the procedure of the orthognathic surgery, they must be considered in the surgical work-up. To produce the optimum postoperative profile, the imbalance of the soft tissue contours and the relative anteroposterior positions of the nose, lips, and chin must be evaluated.
Postoperative
The primary purpose of soft-tissue facial profile analysis before orthognathic surgery is to assess facial esthetics and predict ________ soft-tissue changes
Surgical movement of the jaws alters the overlying soft tissues and facial profile
Why is soft-tissue analysis an essential part of the orthognathic surgery work-up?
Vertical
The facial thirds are divided in which dimension?
1/3s
In an ideal frontal facial analysis, the distance from the hairline to the glabella should represent approximately what proportion of the total facial height?
Horizontal
The facial fifths are divided in which dimension?
1/5
In an ideal frontal facial analysis, the width of one eye is approximately what proportion of the total facial width?
- Syndromes and sequelae of facial trauma
- Identify skeletal cross bites
- Severe asymmetry
- Planning for surgery in 3D
- Evaluate impacted tooth
- TMJ evaluation
What are six benefits of using a CBCT as a diagnostic record?
Compensation
Define the following:
When the teeth compensate for a skeletal discrepancy
Decompensation
Define the following:
Pre-surgical process of achieving normal dental position within the individual's supporting bone so the teeth are in more ideal occlusion after surgery
- Upper incisors retroclined
- Lower incisors proclined
In a skeletal Class II malocclusion, how do the incisors typically compensate for the underlying skeletal discrepancy?
- Procline upper incisors
- Retrocline lower incisors
During presurgical orthodontic decompensation for a skeletal Class II patient, how should the orthodontist adjust the teeth?
Lower bicuspids (premolars)
Where are extractions typically performed during decompensation of a skeletal Class II malocclusion?
Return the teeth to their normal position within the supporting alveolar bone before surgery
What is the goal of presurgical orthodontic decompensation?
- Upper incisors proclined
- Lower incisors retroclined
In a skeletal Class III malocclusion, how do the incisors typically compensate for the underlying skeletal discrepancy?
- Retrocline upper incisors
- Procline lower incisors
During presurgical orthodontic decompensation for a skeletal Class III patient, how should the orthodontist adjust the teeth?
Upper bicuspids (premolars)
Where are extractions typically performed during decompensation of a skeletal Class III malocclusion?
Their malocclusion may temporarily appear worse before surgery (profile will look more concave)
What should you inform patients undergoing decompensation for Class III orthognathic surgery?
Dentoalveolar compensation (camouflage treatment)
What is most appropriate when the patient rejects orthognathic surgery?
Dentoalveolar compensation (camouflage treatment)
What is it called when an orthodontist purposely compensates for a skeletal malocclusion just by moving the teeth (NOT correcting the skeletal relationship)?
Camouflage treatment
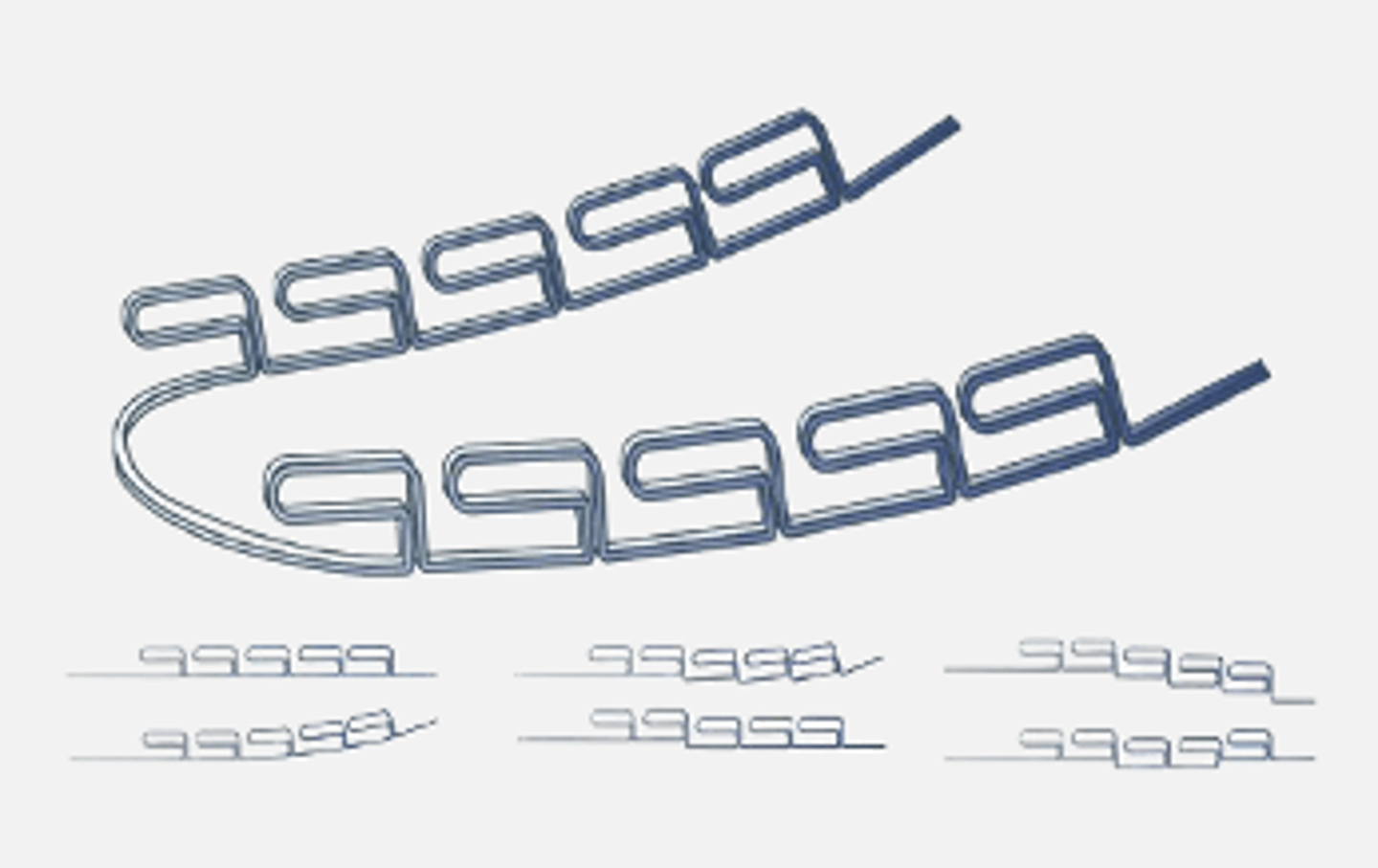
What type of treatment is the Multiloop Edgewise Archwire (MEAW) involved in?
- Anterior open bite
- Skeletal Class III
MEAW therapy is commonly used in patients with what occlusion?
Increases compensation with limited facial profile change
When using the Multiloop Edgewise Archwire (MEAW) treatment, do you suspect any facial changes, profile improvement, or compensation?
- Transverse: Skeletal Asymmetries
- Vertical: Skeletal open bite especially skeletal Cl III (ANB < -3°), impinging skeletal deep bite especially Cl II (ANB > 9°)
What skeletal discrepancies are generally considered too severe for orthodontic camouflage and are an indication for orthognathic surgery?
Orthognathic surgery with orthodontics
A patient with a severe skeletal Class III malocclusion and an ANB angle less than -3° is most likely to require what treatment?
Orthognathic surgery with orthodontics
A patient with a severe skeletal Class II malocclusion with an impinging skeletal deep bite and an ANB angle > 9° is most likely to require which treatment?
Impinging skeletal deep bite
A patient with a severe skeletal Class II malocclusion and an ANB angle greater than 9° is most likely to have what type of bite?
True
T/F: Psychosocial factors can significantly influence a patient's motivation and treatment choice in deciding whether to pursue orthognathic surgery
False - MORE likely
T/F: Children with an overjet greater than 7 mm are less likely to report being bullied than children with smaller overjets
True
T/F: All of the following are factors that may influence the decision-making process for orthognathic surgery
- Social issues
- Psychologic well-being
- Social support
- Self-worth
- Expectations for self and future
- Patient/clinician interaction
- Financial resources
- Health care provider
- Time availability
- Morphologic findings
- Physical problems
- Align teeth
- Treat upper and lower arches separately
- No attempt is made to correct the bite
- Decompensation
What are some goals for pre-surgical orthodontics?
8-12 months
What is the timeline for pre-surgical orthodontic treatment?
Increase
In presurgical orthodontics for a skeletal Class II patient, extraction of the lower first premolars followed by retroclination of the lower incisors will most likely ________ the overjet as part of decompensation
~6-8 weeks
Stabilizing archwires with soldered or crimpable hooks are typically placed ___-___ weeks before surgery
Anterior teeth (incisors)
In skeletal malocclusions, which teeth most commonly compensate for the underlying jaw discrepancy?
To provide the surgeon with greater freedom to achieve optimal skeletal (basal) correction
Why is dental decompensation performed before orthognathic surgery?
Before
(and immediately before orthognathic surgery, patients should undergo a re-evaluation)
Orthognathic surgical planning should be completed _______ orthodontic treatment begins
- Anteroposterior
- Vertical
- Transverse
Surgical planning in orthognathic surgery requires assessment in which three dimensions?
Roll
Define the following:
Rotation around the anterio-posterior longitudinal axis
Pitch
Define the following:
Rotation around the medio-lateral axis
Yaw
Define the following:
Rotation around the superior-inferior vertical axis
Roll
Which rotational movement is used to correct occlusal canting?
Pitch
Which rotational movement is primarily used to correct excessive gingival display (gummy smile) or deep/open bites?
Yaw
Which rotational movement is primarily used to correct transverse facial asymmetry?
Convex
Which facial profile is most commonly associated with a skeletal Class II malocclusion?
Mandibular deficiency (retruded mandible)
The weak or receding chin seen in skeletal Class II patients is primarily due to what?
- Everted lower lip
- Protrusive maxilla/upper lip
Which lip finding is commonly associated with skeletal Class II malocclusion?
Posterior positioning (retrusion) of the mandible relative to the maxilla
Increased overjet in a skeletal Class II Division 1 patient is primarily caused by what?
They are dentoalveolarly compensating for the skeletal discrepancy
What are the lower anterior teeth in skeletal Class II patients are often tipped forward?
Skeletal class II
What skeletal presentation do you suspect with the following?
- Convex profile
- Weak chin
- Everted lower lip
- Protrusive maxilla/ upper lip
- Increased overjet
- Lower anterior teeth tipped forward
Skeletal deep bite
What skeletal presentation do you suspect with the following?
- Long ramus
- Mandibular overclosure (flat mandibular plane/ reduced mandibular plane angle)
- Reduced lower facial height
- Short, square facial appearance (Brachiocephalic)
- Severe dental attrition secondary to excessive overclosure
Long
A patient with a skeletal deep bite typically has a ______ ramus
Short, square face (Brachiocephalic)
A patient with a skeletal deep bite typically has which facial appearance?
Reduced
Mandibular overclosure in skeletal deep bite is associated with ______ mandibular plane angle and anterior dental deep bite
Class III
Excessive mandibular overclosure may contribute to Angle Class _____ malocclusion
Severe dental attrition due to excessive overclosure
What is a common long-term consequence of untreated skeletal deep bite?
Decrease (low-angle patient)
If a patient has a skeletal class II, retrognathic mandible, and deep bite, you would expect a ______ Frankfort-Mandibular Plane Angle (FMA)
Decreased
A patient with a skeletal Class II and skeletal deep bite would most likely exhibit a ________ lower anterior facial height
Deep
What type of mentolabial fold would you expect of a skeletal Class II patient with a deep bite?
Skeletal class II with deep bite
What type of skeletal and dental findings would you suspect with the following characteristics?
- Low-angle patient
- Decreased lower anterior facial height
- Deep bite
- Deep mentolabial fold
- Increased overjet and overbite
Skeletal Class II (Mandibular retrognathia)
A Bilateral Sagittal Split Osteotomy (BSSO) advancement is primarily performed to correct what malocclusion?
- Advance the mandible
- Increase lower facial height
- Correcting the deep bite
In a patient with a skeletal Class II deep bite, a BSSO advancement with clockwise rotation primarily aims to what?
Short
A patient with a skeletal open bite typically has a ______ ramus
Increased
A patient with skeletal open bite typically presents with _______ lower facial height (LFH)
Lip incompetence
An increased interlabial gap (ILG) is most commonly associated with what type of lips?
Because they contract the mentalis muscle to achieve lip closure due to lip incompetence
Why do patients with skeletal open bite often demonstrate mentalis strain?
Skeletal Open bite with dental open bite
What type of skeletal and dental findings would you suspect with the following characteristics?
- Maxillary vertical excess
- Increased lower facial height (LFH)
- Incompetent lips
- Short ramus
- Increased interlabial gap (ILG)
- Mentalis strain
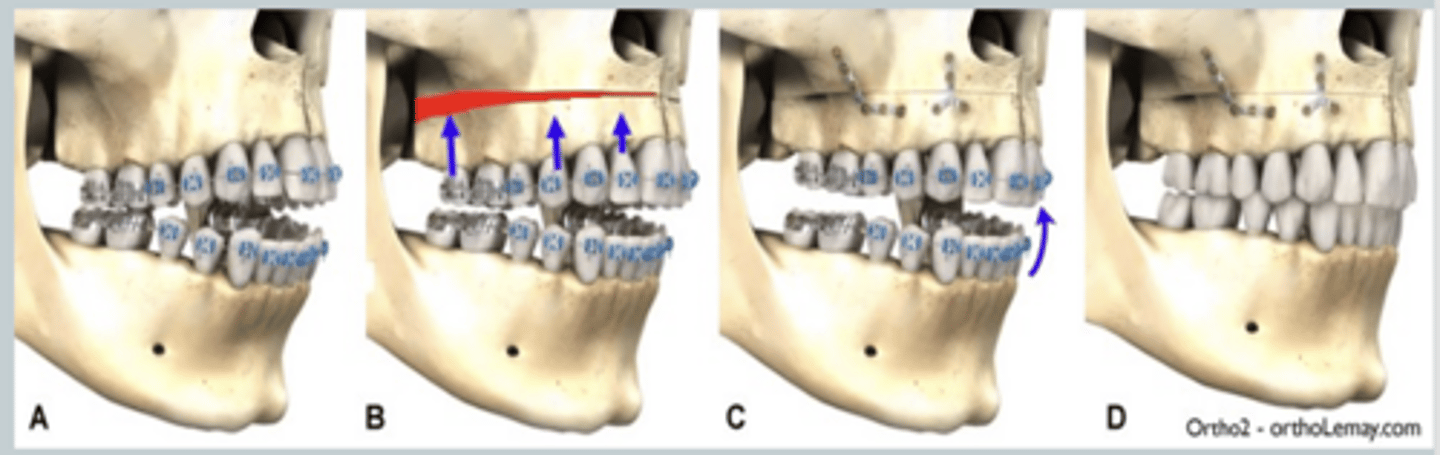
Le Fort I maxillary impaction
A patient with excessive gingival display due to maxillary vertical excess is most appropriately treated with what treatment?
- Hard tissue component
- Soft tissue component
Excessive gingival display (gummy smile) may result from which tissue components?
Short or hypermobile upper lip
What soft tissue feature may contribute to a gummy smile?
Le Fort I maxillary impaction
What type of surgery does this show?
Unstable
(due to stretching of the pterygomandibular sling muscles)
In a patient with a long face (skeletal open bite), BSSO with rotation of the gonial angle down and the chin up is considered (stable/unstable)
Stable
In a patient with a short face (skeletal deep bite), BSSO with rotation of the gonial angle up and the chin down is (stable/unstable)
It is less stable because mandibular rotation stretches the pterygomandibular sling muscles
Why is isolated BSSO often avoided in patients with severe skeletal open bite?
Bimaxillary surgery
(Reduces mandibular counterclockwise rotation after surgery in class III patients with severe anterior open bite)
For a patient with a severe skeletal Class III and anterior open bite, which surgical approach generally provides better skeletal stability?
Long face (skeletal open bite)
The following surgical technique is used on what type of facial structure?
- BSSO
- Rotating gonial angle down & chin up
- Unstable (stretching pterygo-mandibular sling muscles
Short face (skeletal deep-bite)
The following surgical technique is used on what type of facial structure?
- BSSO
- Rotating gonial angle up & chin down
- Stable
C) Grafts NOT needed (overlapping of segments)
The following are all advantages of bilateral sagittal split osteotomoy (BSSO) EXCEPT:
A) Intra-oral (↓ morbidity)
B) Used for all movements
C) Grafts needed (overlapping of segments)
D) Broad interface of medullary bone (↑ healing)
E) ↑ fixation by plates/miniplates or bicortical screw
F) ↓ load on elevator muscles (↑ stability)
G) ↑ control of condylar segments
Monocortical miniplates
What showed better stability: monocortical miniplates or bicortical screw fixation during BSSO?
Tooth-bearing portion of the mandible
During a BSSO, the distal segment refers to what?
Condyle
During BSSO, the proximal segment contains what?
Inferior alveolar neurovascular bundle
Which neurovascular structure is at greatest risk of injury during a BSSO?
Inferior alveolar nerve (injury or tension or edema)
What nerve could possibly have paresthesia with BSSO surgery?