BIOL 4106 - Exam 2
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Life Cycle of Hematozoa Apicomplexans
Infective stage for vertebrate host: Sporozoite
Infective stage for vector: Gametocytes
Three Phases of Apicomplexan Life Cycle
Merogony (Host)
Multiple nucleus division → merozoites
Gametogony
(Part one: Host)
Merozoites → gamete
Microgamete: male
Macrogamete: female
(Part two: Vector)
Fertilization; microgamete → macrogamete
Results in an ookinete (zygote) → oocyst
Sporogony (Environment)
Replication within oocyst → sporozoites (INFECTIVE STAGE)
Must ingest sporulated oocyst
Malaria Life Cycle
Sexual Phase
Occurs in female Anopheles mosquitos
Asexual Phase - Two Locations
Extraerythrocytic
Sporozoites will attach to hepatocytes (Circumsporozoite protein)
Merogony (nuclear division) → merozoites
Merozoites rupture hepatocytes
Erythrocytic
Merozoite → ring stage → trophozoite → schizont → merozoites
attach to RBC and enter via apical complex looking for receptors
P. vivax uses Duffy Antigen which is lost in Sickle Cell Anemia people (those people can’t get it)
Eats hemoglobin (toxic to the parasite)
Ring stage → gametocyte for infective stage of the mosquito
Schüffner’s Dots
Dotted appearance of trophozoites seen in P. vivax and P. ovale ameboid trophozoites infected RBC when stained with Giemsa
Maurer’s Clefts
Large course dots were observed in P. falciparum infections containing older ring-form trophozoites and asexual stages.
Maurer’s clefts resemble the Schüffner’s dots but are usually larger and coarser.
Band / Basket form
[P. malariae]
Trophozoites have compact cytoplasm and a large chromatin dot.
Occasional band forms and/or “basket” forms with coarse, dark- brown pigment can be seen.
Clinical Presentation of Plasmodium falciparum
Malignant tertian malaria
Clinical Presentation of Plasmodium vivax
Benign tertian malaria
Clinical Presentation of Plasmodium malariae
Quartan malaria
Clinical Presentation of Plasmodium ovale
Very Benign tertian malaria
Benign Malaria
All four Plasmodium spp.
Treatable
No signs of severe organ dysfunction
Symptoms:
Headaches
Extreme fatigue
Mild jaundice (destruction of hepatocytes)
Malarial hepatitis
Splenomegaly (RBC get stuck during blood filtering)
Malignant Malaria
[P. falciparum]
Most serious and can be fatal
Severe organ dysfunction
Hyperparasitemia
Anemia (Hemolysis & Bone marrow suppresion)
Cerebral malaria
Hypoglycemia
Hemoglobinuria (Blackwater)
Acute respiratory distress syndrome
Low BP
Jaundice
Heme → bilirubin; liver cannot break it down fast enough and deposits in tissue
Recrudescence
[P. malariae → chronic infection]
From not finishing your meds or drug resistance to malaria with a very low level RBC infection and asymptomatic
Relapse
[P. ovale and vivax]
Cleared merozoites in the blood but still have hypnozoites in the liver
Reinfection
Was effectively treated but had a new infection
Paroxysm
Cold shiver → Hot → Sweat (Malaria)
Deep vascular schizogony
[P. falciprium]
Sticky RBC with profusions (knobs) by mature trophs
Deadly → Cerebral Malaria
Fetal Death from P. falciprium
Lack of oxygen
Mom’s anemia
Hyperthermia
Mom’s high fever
(Baby doesn’t get infected)
Hemozoin crystal
A dark-brown granular pigment from undigested toxic heme from hemoglobin
Gametophytes differential
Plasmodium falciparum is a banana-shaped while the rest are circular
Vector for Babesia
Ixodes scapularis
Vector for Malaria
Female Anopheline mosquitoes
Merozoites per Sporozoite in the liver
P. vivax 6-8 days 10,000 merozoites per sporozoite
P. ovale 9 days 15,000 merozoites per sporozoite
P. malariae 12-16 days 2,000 merozoites per sporozoite
P. falciparum 5-7 days 40,000 merozoites per sporozoite
Pathology from Malaria
Synchronized rupture of RBCs by merozoites that starts paroxysm
Can release hemozoin and other parasite metabolic wastes
Can result in spikes of fever, chills, onset of malaise (discomfort) & headache, and anemia (ruptured RBC’s = blood cell loss)
Hallmarks of P. falciparum
Ring form: 2 distinct chromatin dots in ring
Gametocyte: Crescent or banana shaped within RBCs
Multiple infections of a single RBC (more than 1 ring per cell)
Normal sized RBCs
Diseases caused by P. falciparum
Cerebral Malaria
Blackwater fever (renal failure → death)
Massive intravascular hemolysis of RBCs causing a spillover of hemoglobin into the urine (hemoglobinuria)
Hallmarks of P. vivax
Enlarged RBCs (ameboid shape)
Schuffner’s dots
All stages found in peripheral blood
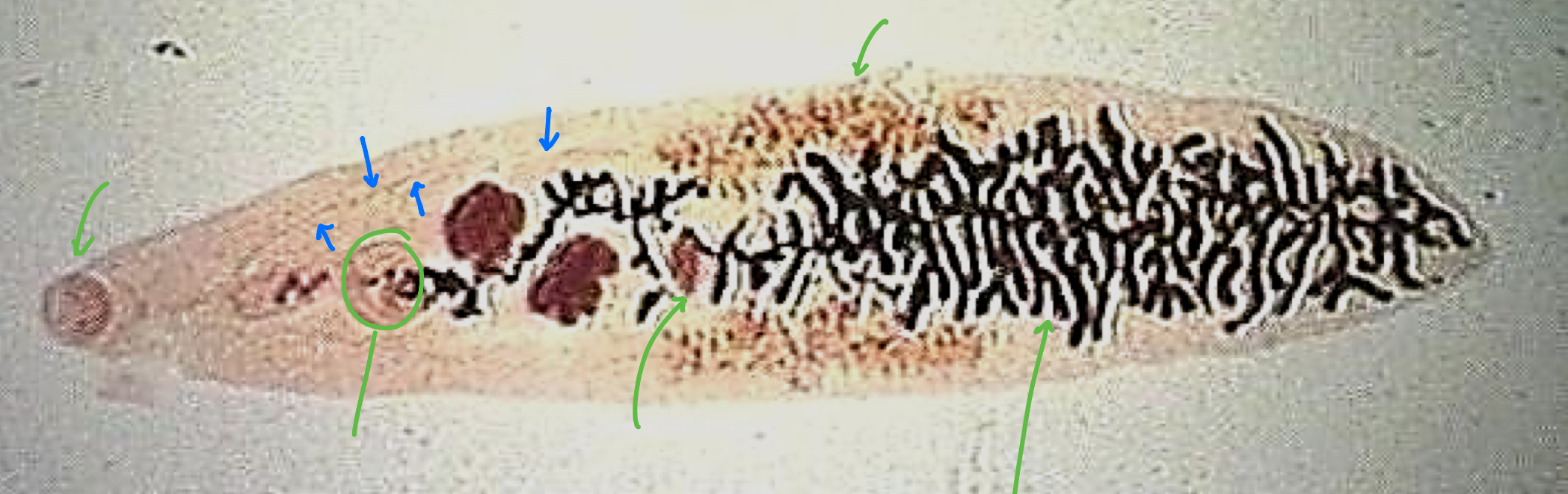
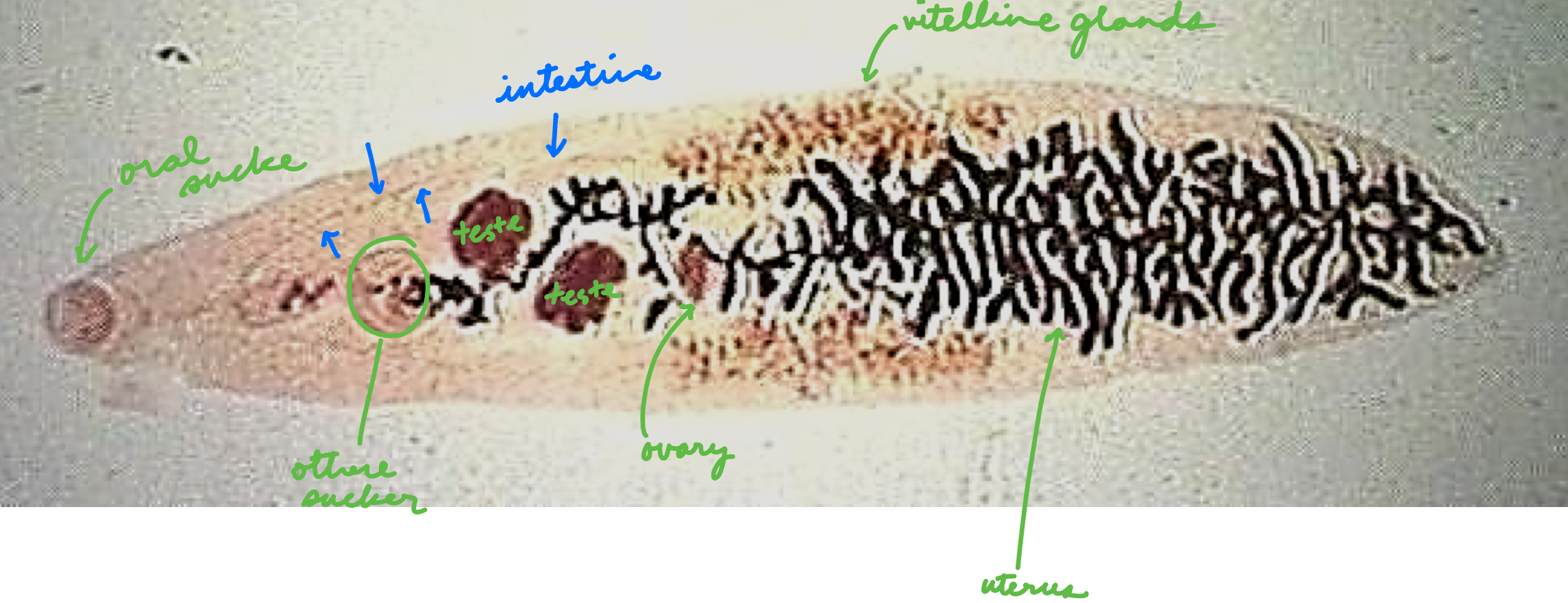
Fasciola hepatica
Sheep Liver Fluke → Liver Rot
Intermediate Host: Lymnea sp (aquatic snail)
Definitive Host: humans, sheep, cattle
Infective Stage: metacercaria
Transmission: fecal-contaminated water with metacercaria
Ex: watercress
Life Cycle:
Ova → miracidium* → sporocyst → redia → cercaria → metacercaria** → adult fluke
Niche: Liver & Bile Duct
Disease: Fascioliasis - migration of flukes
Hepatomegaly
Liver abscesses → jaundice
Eosinophilia
Scarring and fibrosis of liver and bile ducts
Morphology:
Leaf shaped, large cone projection (anterior cone and shoulders)
Extensive vitellaria
Fasciola gigantica
Liver fluke
Morphology: similar to F. hepatica but LARGER
Different snail vector
Distribution: Asia, Africa, Hawaii
Fascioloides magna
Liver fluke
Cycle similar to F. hepatica
Niche: Liver
Definitive Host: Herbivores — deer, sheep, cattle
Morphology: similar to F. hepatica except NO anterior cone or shoulders
Fasciolopsis buski
Intestinal fluke - common in humans and pigs
LARGEST fluke to infect humans (DH)
Biology similar to F. hepatica
Feed on intestinal epithelial cells
Niche: small intestine
Intermediate Host: Snail
Transmission: metacercaria in underwater vegetation
Ex: Water chestnuts, bamboo, etc.
Boiling can kill metacercaria
Disease: causes ulceration, hemorrhage, and abscesses of small intestine
HALLMARK:
Intestinal ceca not branched (wavy)
Acetabulum large and close to oral sucker
Clonorchis sinensis
Chinese liver fluke
Reservoir: dogs and cats
1st Intermediate Host: aquatic snail
2nd Intermediate Host: freshwater fish
DH Infective Stage: metacercaria in 2nd IH (FW fish)
Definitive Host: human, dog, cat
Niche: lumen of bile duct (bile duct epithelium)
Infections of Clonorchis sinensis
Light infection: asymptomatic
Moderate to Heavy infections: clinical disease presentation → cholangiocarcinoma (bile duct cancer)
Dx of flukes
Eggs in stool
Heterophyes heterophyes
Morphology: Very tiny flukes
Niche: small intestinal villi
Distribution: Africa, Asia, Middle East, and FAR EAST (Far East is called Metagonimus yokogawai)
1st IH: snail
2nd IH: fresh / brackish water fish
Disease: gastric distress, malaise, fatigue, diarrhea → heart failure, eggs in brain and spinal cord, death
Dicrocoelium dendriticum
Lancet fluke
Life cycle on LAND ONLY
Distribution: Not Africa or South America
1st IH: Cionella lubrica (LAND snail)
2nd IH: Formica fusca (common brown ant)
Definitive Host: ruminants like cattle, sheep, and deer
Niche: bile ducts of DH
Prosthogonimus machrorchis
Oviduct fluke of birds
1st Intermediate Host: snail
2nd Intermediate Host: dragonfly nymph
Definitive Host: bird
Paragonimus westermani
Human lung fluke
Distribution: Japan, China, Vietnam, Thailand, Cambodia, Africa, Central and South America
Paragonimus kellicotti
Distribution: North America
Definitive Host: multiple mammalian animals, including humans
1st Intermediate Host: aquatic snail
Live in fast-moving streams
2nd Intermediate Host: crustacean (crayfish or crab)
Schistosomatidae Characteristics
Blood fluke
No second intermediate host
Distribution: USA
Definitive Host: humans, birds, fishes, and turtles
Infective Stage: Cercaria
Does not have redia or metacercaria
Mature in blood vascular system of definitive host
Dioecious (separate sexes)
Identify based on egg
Schistosoma haematobium
Eggs in urine have a terminal spine
Distribution: Africa and Middle East
Niche: veins of urinary bladder plexus (veins draining urinary bladder)
Blood in urine (hematuria)
Can cause bladder cancer
Schistosoma mansoni
Eggs in feces have large lateral spine
Distribution: Africa (Egypt and Sudan), Middle East, South American, and Caribbean
Niche: veins draining large intestine (Inferior Mesenteric Veins)
Schistosoma japonicum
Eggs in feces with rudimentary spine
Distribution: Far East = China, Malaysia, Philippines, Indonesia (eradicated from Japan)
Niche: veins draining small intestine (Superior Mesenteric Veins)
Schistosomiasis
Caused by the eggs
Tranverse through wall of vein → tissue of intestine or bladder → lumen to go out with feces or urine
S. mansoni & S. japonicum: gut wall to gut lumen to go out with feces
S. haematobium: bladder wall to bladder lumen to go out with urine
2/3 of eggs don’t make it to the lumen of intestine or bladder
Trapped in intestinal or bladder wall
Some get lodges in capillaries of liver
Trapped eggs secrete soluble egg antigens (SEA’s) which are hydrolytic enzymes which trigger inflammatory and immune responses
Chronic, granulomatous fibrosis lesions in tissues containing trapped eggs (swirly)
Monecious
Hermaphroditic
Majority of platyhelminths
Self fertilize
Cross fertilize between two hermaphroditic individuals [Paragonimus sp.]
Dioecious
Separate sexes [Schistosomes sp.]
Female lives inside male and cannot survive without him
Fill in the arrows
Dendritic
Ovum
An egg that encloses the embryo (miracidium)
Operculum - opening at one end of egg through which larva will escape
Miracidium
Infective stage for IH
Ciliated free-swimming larva hatched from ovum
Will lose cilia after ingestion
Some can penetrate; some need to be ingested
Sporocyst
From metamorphosis of miracidium as it elongates to form a sac-like structure
No mouth, no digestive system, absorbs nutrients from the host
Germinal sac
Embryos develop asexually within
Can produce generations of sporocysts: daughter sporocysts, redia, or cercaria (depending on species)
Redia
Either bursts out of sporocysts or leave by birth canal
Active in host (crawls around)
Rudimentary digestive system and actively feeds on host tissue
Muscular pharynx and short sac-like gut
Can develop embryo to form daughter redia or cercaria
Cercaria goes out of birth pore
Cercaria
Infective stage for DH [Schistosoma sp.]
Free-swimming with a tail or no tail
Has a mouth and digestive system but doesn’t feed
Penetration gland
Considered a juvenile fluke
Metacercaria
Ingested by DH (except Schistosoma)
DH does not need to feed on IH
Encysted form
General Life Cycle of Trematodes
Ovum → miracidium → sporocyst → redia → cercaria → metacercaria → adult fluke
Prosthogonimus machrorchis

Babesia bigemina
Cattle, deer, and rarely humans
Distribution: Central and South America
Vector: Boophilus annulatus (North American Cattle Tick)
Babesia canis
Infects dogs by tick bites that can be fatal
Distribution: Worldwide
Vectors:
Rhipicephalus sanguineus (Brown dog tick)
Dermacentor variabilis (American dog tick)
Babesia microti
Infects rodents and humans
Distribution: USA, Northeast and Midwest
Vector: Ixodes scapularis (deer tick)
Life Cycle:
Sporozoites enters vertebrates via saliva → RBC (no hemozoin) → merogony → merozoites → gametogony → gametocytes → blood meal → syngamy (gametocytes fuse) → kinete → sporogony → sporozoites
How to identify babesia sp./babesiosis
If there are any symptom for tick-related diseases
Mild malaise
Maltese crosses