DIG Exam 3 ILA Histopath of IBD Sos
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
Diseases characterized by chronic inflammation of the gastrointestinal tract resulting in permanent damage possibly leading to adenocarcinoma
IBD
Combination of genetic factors and up-regulated immunity
Cause of IBD
Abdominal pain
Persistent diarrhea
Rectal bleeding
bloody stools
Weight loss
Fatigue
IBD Symptoms
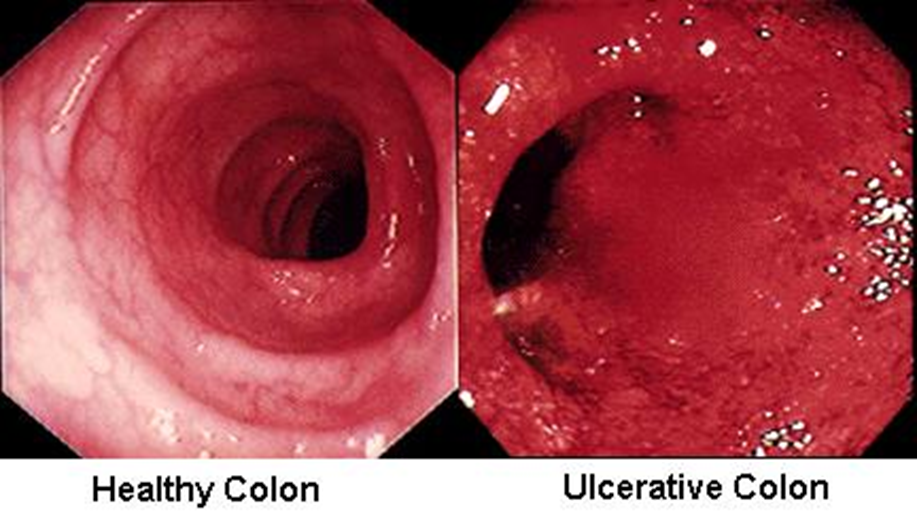
Starts in the rectum and progresses to the cecum in a linear fashion
UC
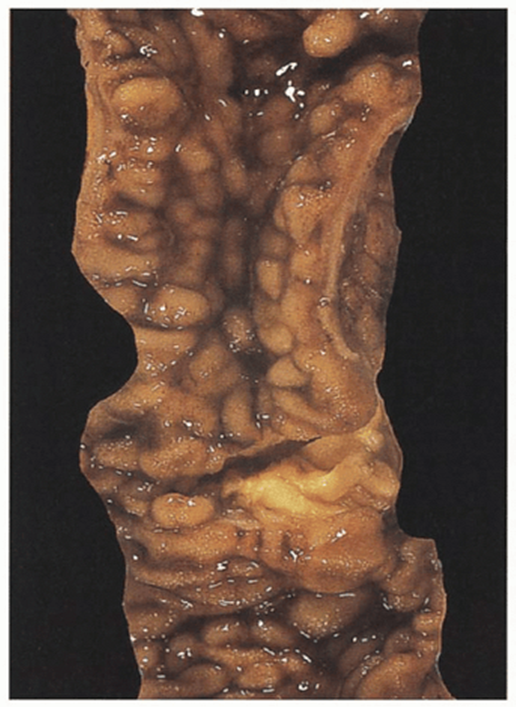
The large intestine grossly lose haustra and contains pseudopolyps (normal mucosa surrounded by erosion)
“lead pipe” appearance on imaging
UC
Inflammation restricted to the mucosa and submucosa
UC
Crypt abscesses (neutrophils)
UC
Symptoms focused on left lower quadrant abdominal pain and bloody diarrhea
UC
Associated with primary sclerosing cholangitis and pANCA
UC
Can develop toxic megacolon and adenocarcinoma (10-15 yrs of disease process)
UC

UC
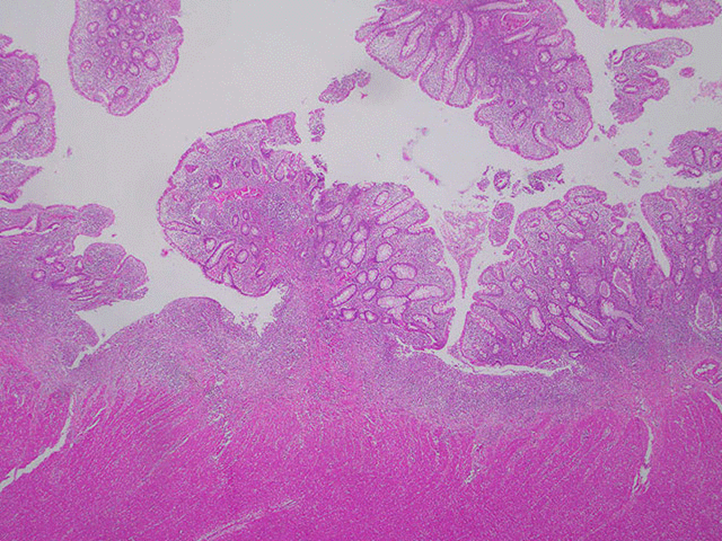
pseudopolyps
UC


UC lead pipe

UC
Pseudopolyps
___________ consist of inflamed mucosa surrounded by erosion. Start at the rectum and progress linearly towards the cecum
pseudopolyps
UC
UC
pseudo polyp
erosions surrounding
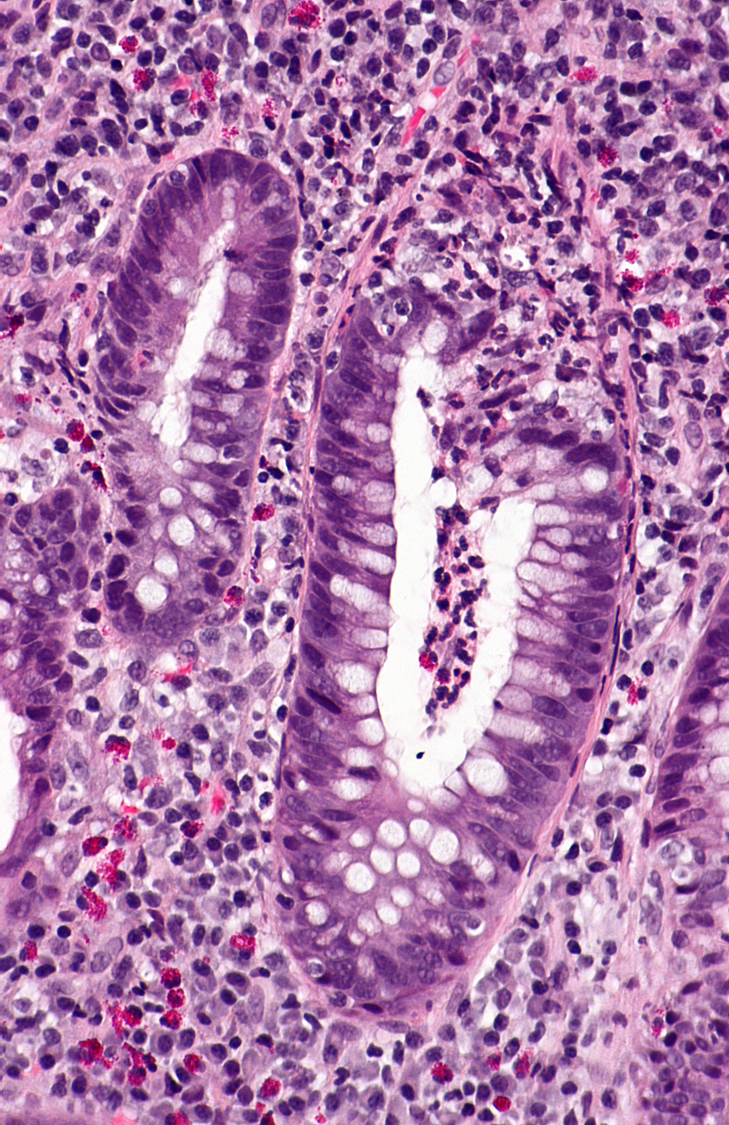
UC
neutrophils in crypts
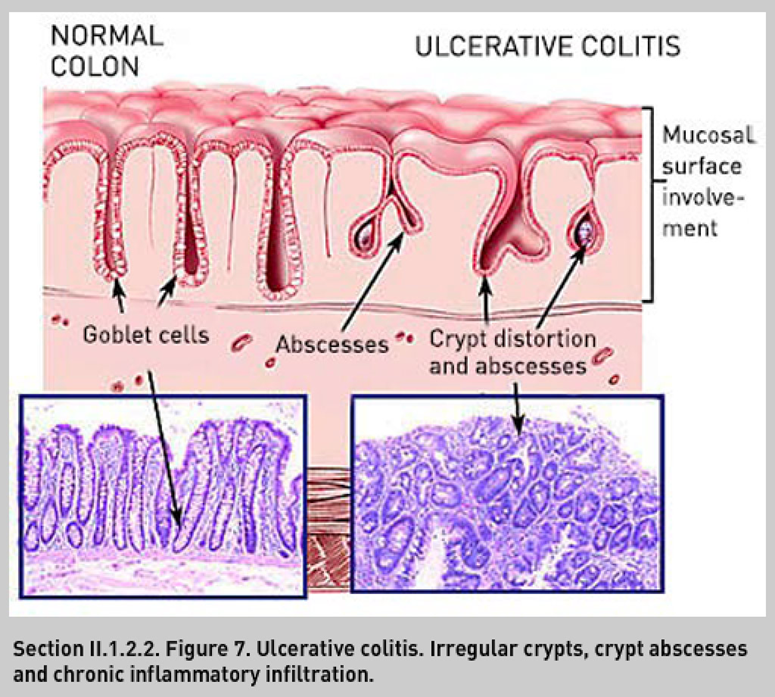
UC illustration


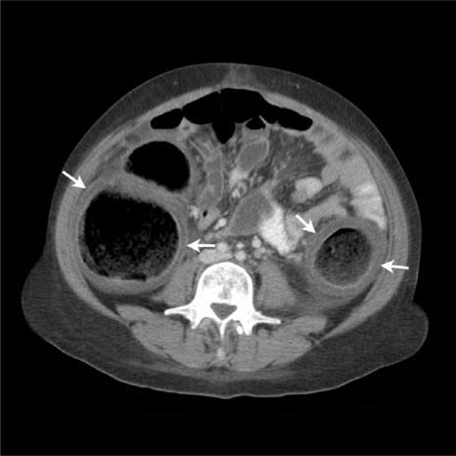
Toxic megacolon
Occurs in days
Segmental nonobstructive colonic dilatation and ischemia followed by necrosis
IBD is a common cause
Toxic megacolon
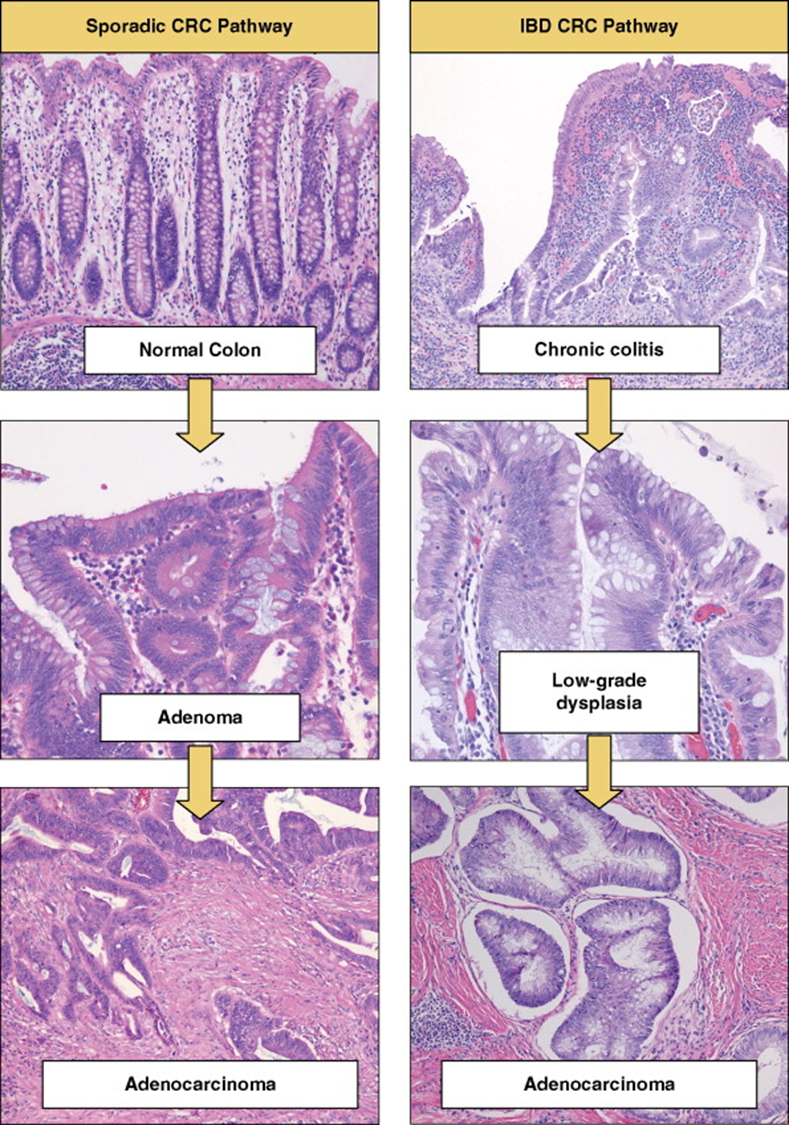
UC to adenocarcinoma
Increased risk of _______ adenocarcinoma with Ulcerative Colitis
Colorectal
Age 15-30 and 50-70 yrs
UC
Age 15 to 35 yrs
CD
Lesions found anywhere in the GI tract from oral cavity to rectum, the ileum and ascending colon region is most common site and the rectum is least common site
CD
Skip lesions
CD
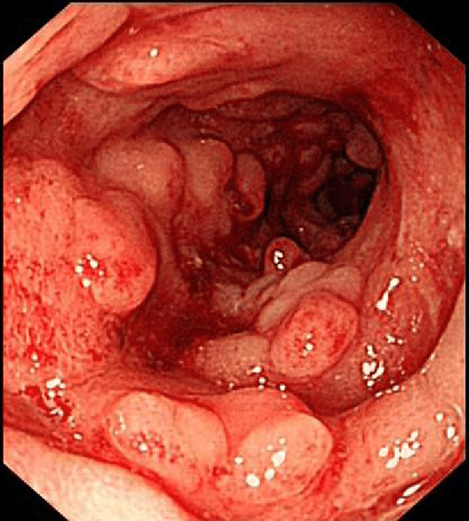
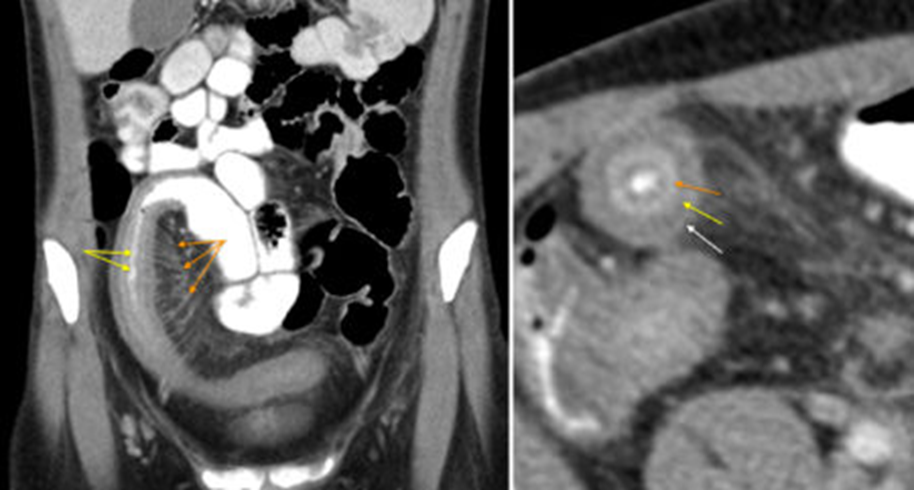
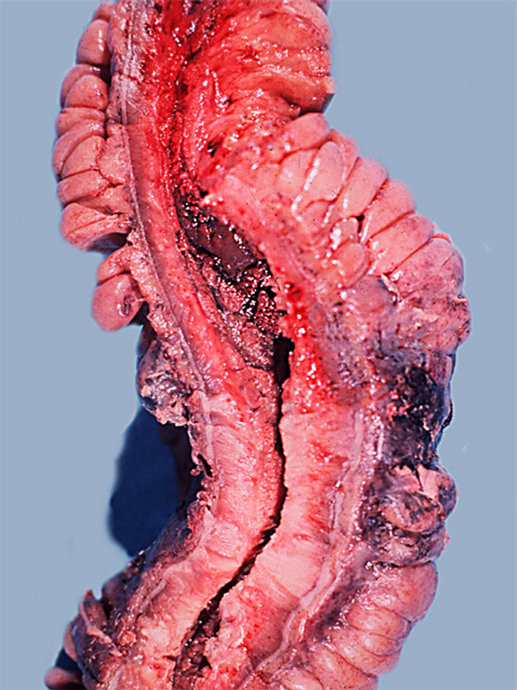
The large intestine grossly contains thickened constricted intestinal wall with strictures, mucosal “cobblestone” appearance, mesenteric fat wraps around “creeping fat” the serosa
CD
Cobblestone
CD
Creeping fat
CD
string sign of Kantor
CD
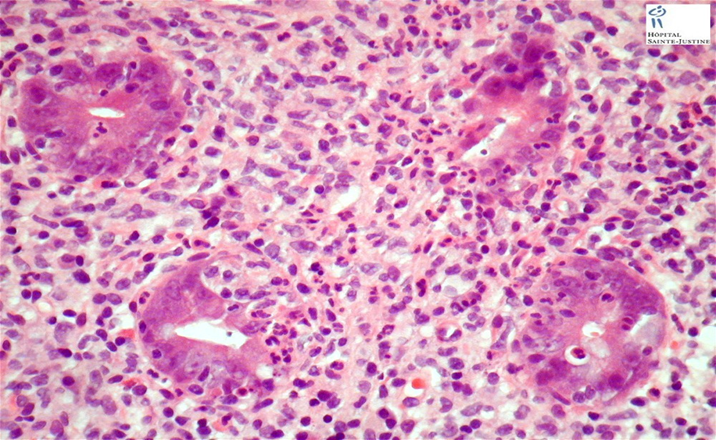
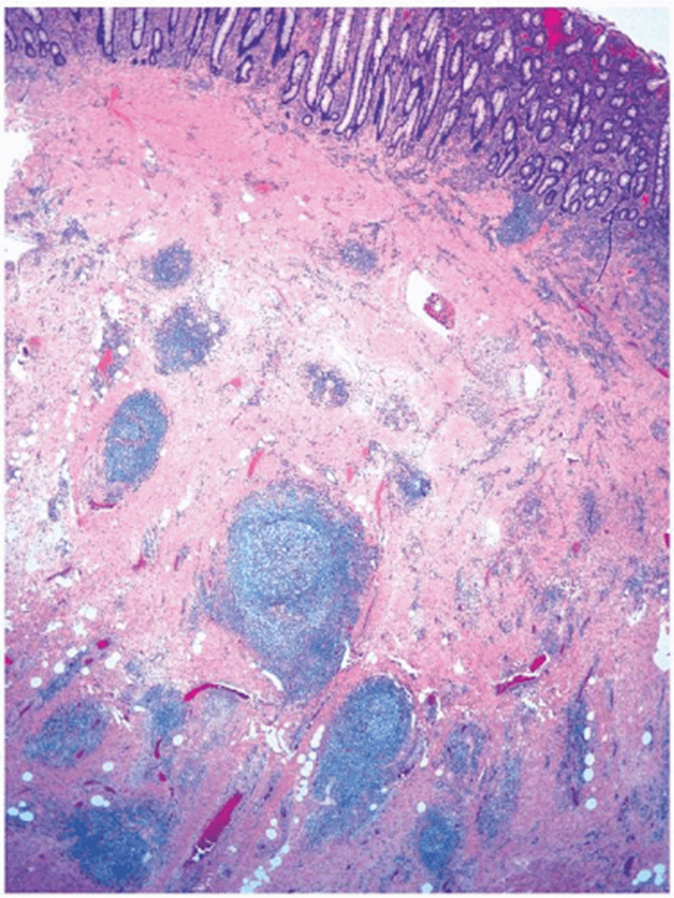
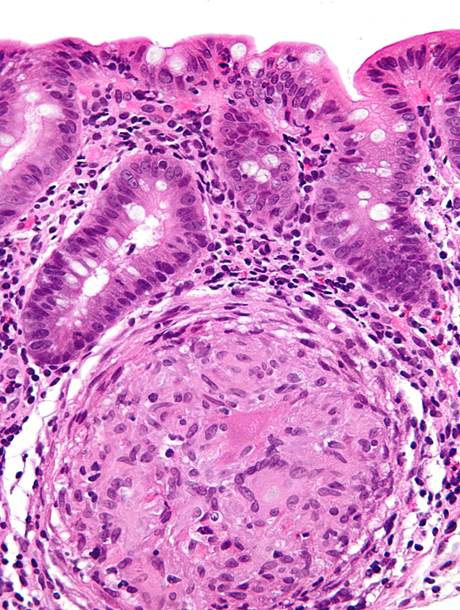
transmural Inflammation with lymphoid aggregates and granulomas
CD
Symptoms focused on right lower quadrant abdominal pain and non-bloody diarrhea
CD
Associated with ankylosing spondylitis, sacroiliitis, uveitis, polyarthritis and erythema nodosum
CD
Can develop malabsorption with nutritional deficiency, fistula formation and calcium oxalate nephrolithiasis
CD
Fistula formation
CD
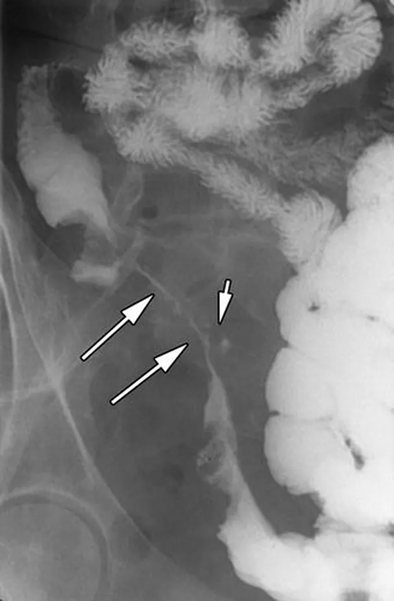
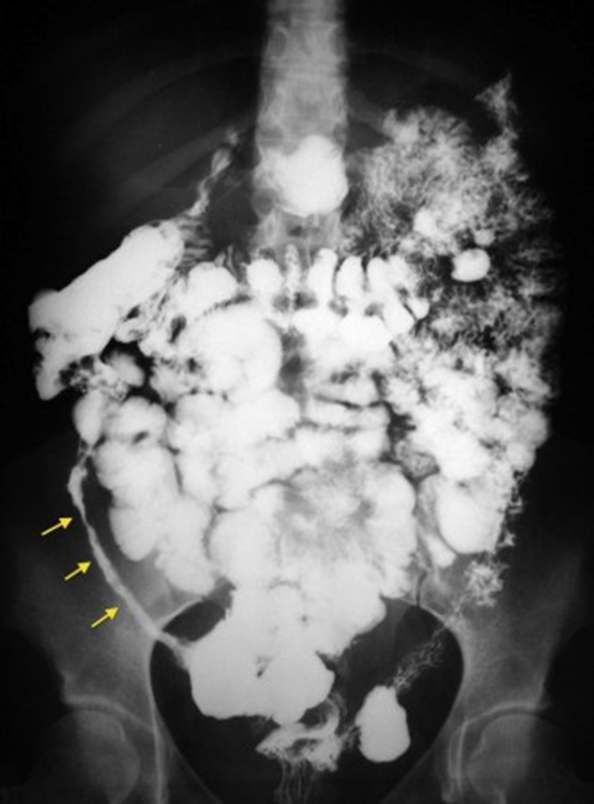
String sign of Kantor
CD

Erythema nodosum
Can be associated with CD

CD
cobblestone
CD
Ileum with thickened wall and
increased mesentery fat lines
CD
Thickened wall and creeping fat
CD
Cobblestone
Internal fistulae
Enteroenteric
Enterovesical
Rectovaginal
External fistulae
Perianal
Enterocutaneous
Peristomal
Types of fistulae in CD
CD
Lymphoid follicles within wall, transmural inflammation
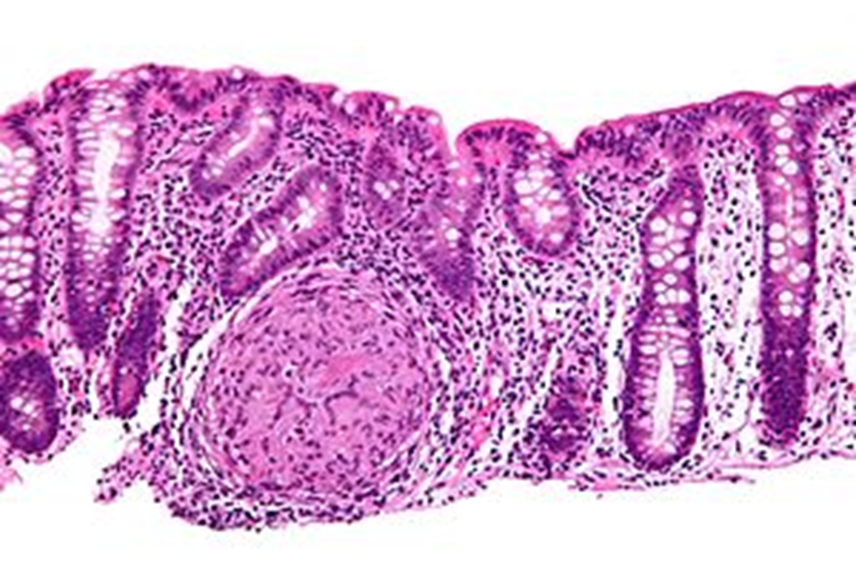
CD
granuloma
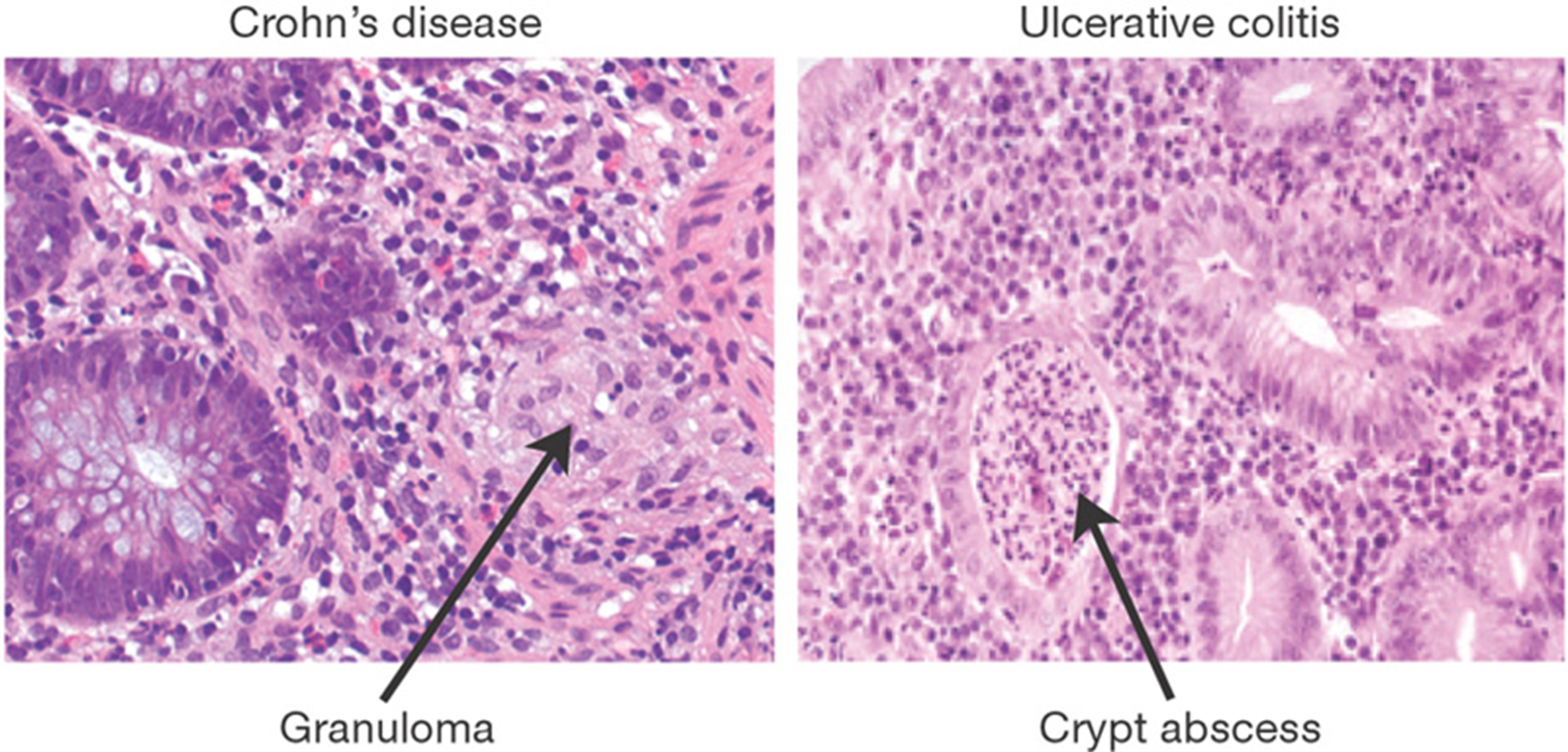
CD vs UC
A common chronic disorder involving the large intestine, unknown cause
Most can control their symptoms with stress reduction, diet management, and healthy lifestyle choices
Symptoms include cramping, abdominal pain, bloating, gas and diarrhea or constipation or both
No histopathologic findings or increase chance of colorectal adenocarcinoma
IBS