NPTE: Bonus Class Cardio
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
Asthma
Is a condition in which your airways narrow, swell, and may produce extra mucus. This can make breathing difficult and trigger coughing, a whistling sound (wheezing) when you breathe out and shortness of breath.
-obstructive
Chronic bronchitis
Is inflammation (swelling) and irritation of the bronchial tubes. These tubes are the airways that carry air to and from the air sacs in your lungs. The irritation of the tubes causes mucus to build up.
-obstructive
Emphysema
Is pathologically defined as an abnormal permanent
enlargement of air spaces distal to the terminal bronchioles, accompanied by the destruction of alveolar walls and without obvious fibrosis. This process leads to reduced gas exchange, changes in airway dynamics that impair expiratory airflow, and progressive air trapping.
Pneumonia
Is an infection in one or both lungs. Bacteria, viruses, and
fungi cause it. The infection causes inflammation in the air sacs in your lungs, which are called alveoli. The alveoli fill with fluid or pus, making it difficult to breathe. water in lungs
-restrictive
Pleural effusion
The pleura are thin membranes that line the lungs and
the inside of the chest cavity and act to lubricate and facilitate breathing. Pleural effusion, sometimes referred to as “water on the lungs,” is the build-up of excess fluid between the layers of the pleura outside the lungs. water on lungs
-restrictive
Pneumothorax
Is a collapsed lung. A pneumothorax occurs when air leaks
into the space between your lung and chest wall. This air pushes on the outside of your lung and makes it collapse. Pneumothorax can be a complete lung collapse or a collapse of only a portion of the lung.
Atelectasis
Is a complete or partial collapse of the entire lung or area (lobe)
of the lung. It occurs when the tiny air sacs (alveoli) within the lung become deflated or possibly filled with alveolar fluid. Atelectasis is one of the most common breathing (respiratory) complications after surgery.
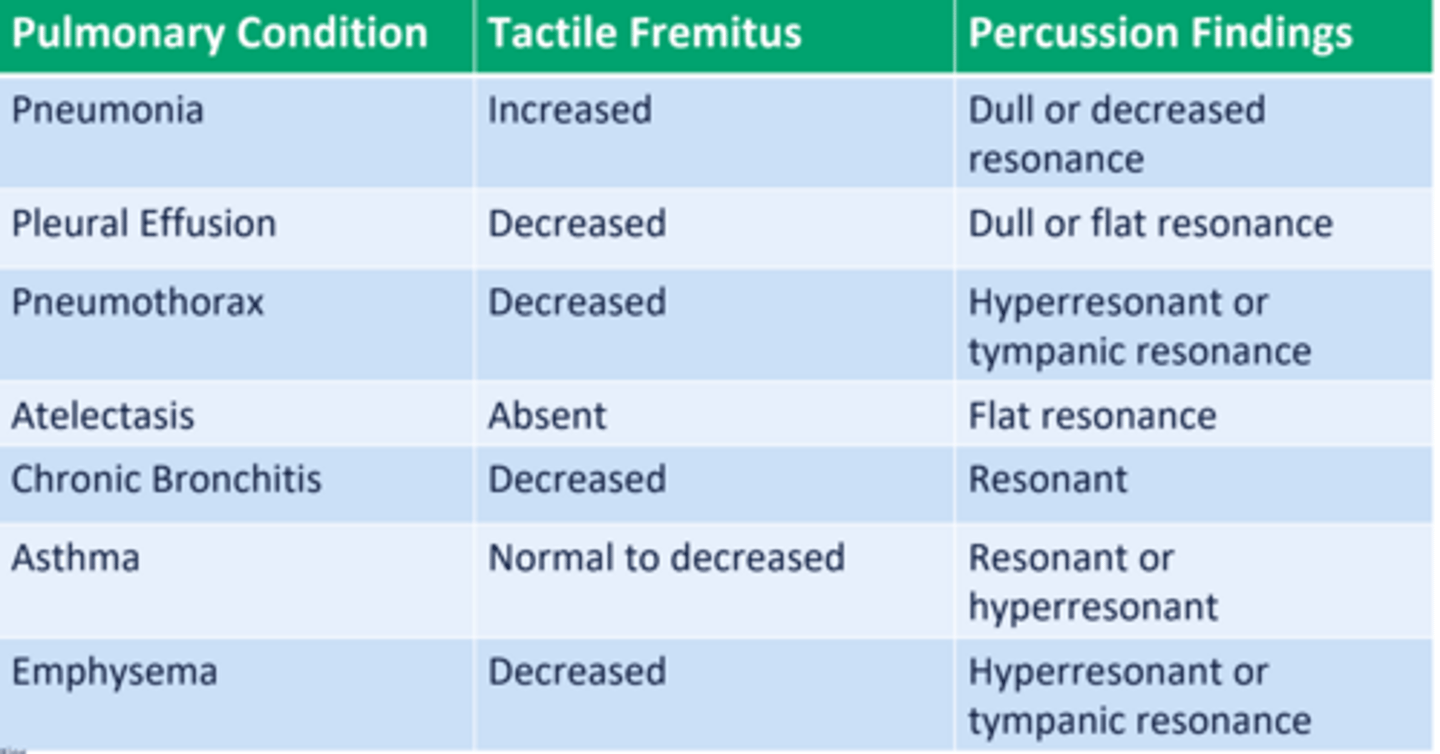
Fremitus
Refers to vibratory tremors that can be felt through the chest by
palpation. To assess for tactile fremitus, ask the patient to say "99" or "blue moon". While the patient is speaking, palpate the chest from one side to the other.
-more air = quieter
-consolidation = louder
Percussion
Is an assessment technique which produces sounds by the
examiner tapping on the patient's chest wall. Just as lightly tapping on a container with your hands produces various sounds, so tapping on the chest wall produces sounds based on the amount of air in the lungs.
-more air = louder
A patient presents with fever, productive cough with purulent sputum,
and localized crackles upon auscultation. Chest X-ray reveals lobar
consolidation. What is the MOST LIKELY diagnosis?
Pneumonia
On evaluation, the physical therapist notes the patient has increased
respiratory rate, fremitus is reduced and on percussion the patient presents
with hyperresonant sound. Based on this presentation, which of the other
following findings would MOST LIKELY be seen in this patient?
Increased Functional Residual capacity
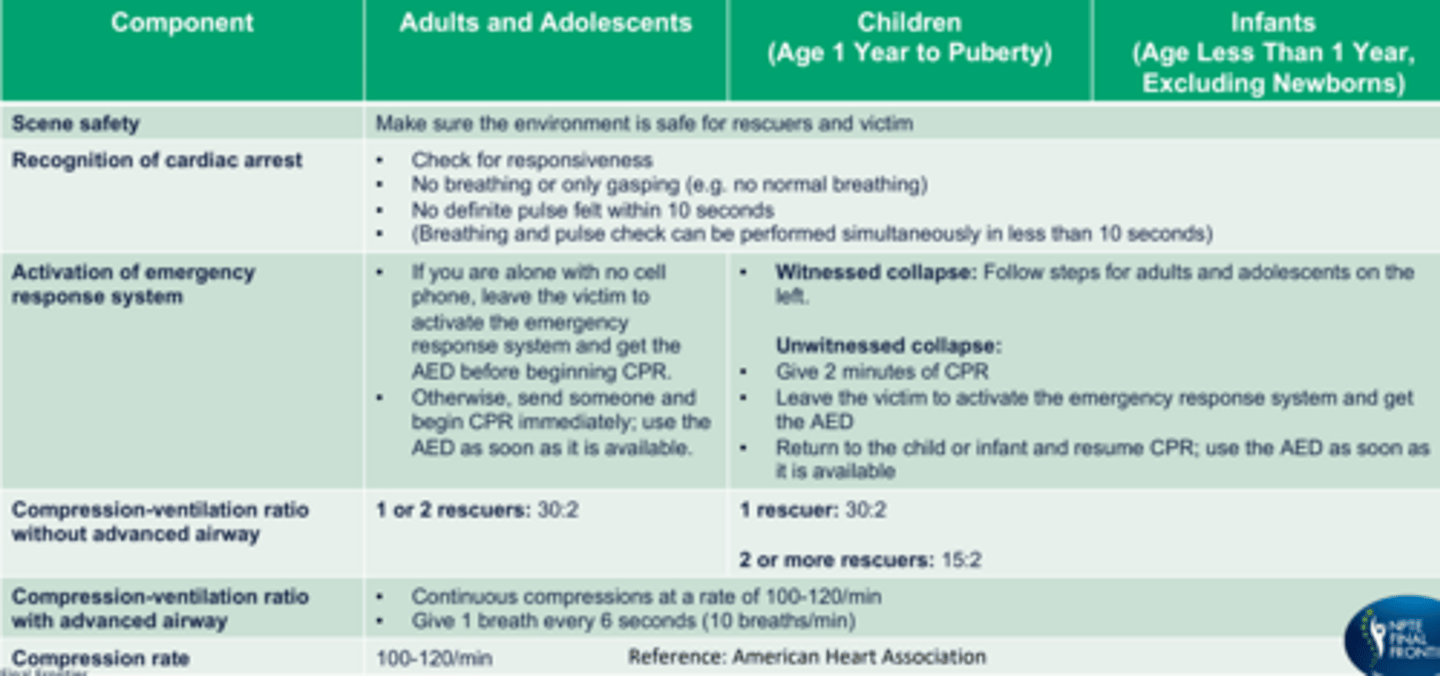
CPR components, compression:ventilation ratio, compression rate
CPR compression depth, hand placement, chest recoil
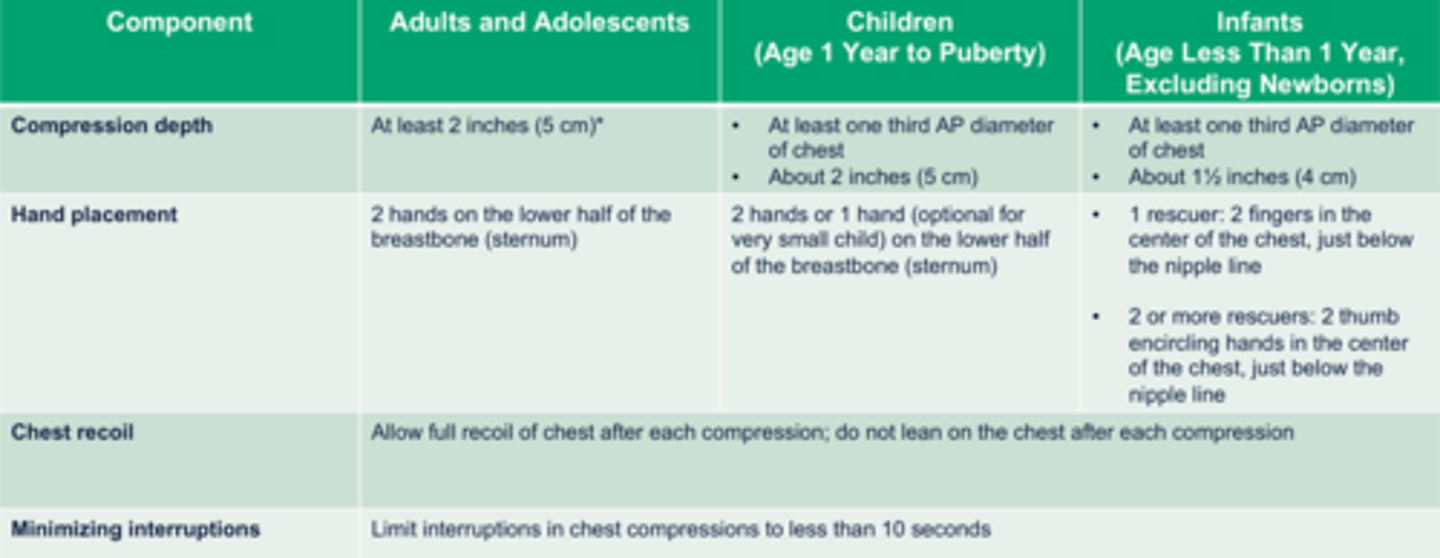
An elderly patient with a history of hypertension, obesity, and moderate osteoarthritis collapses suddenly while exercising in the clinic. You are the first responder and find the patient unresponsive and pulseless. You immediately initiate EMS. Which of the following strategies should be emphasized to optimize chest compressions in this patient, considering their comorbidities?
Perform chest compressions with a depth of at least 2 inches while maintaining the correct hand placement over the lower half of the sternum.
FITT principle diabetic patients
3-7days/wk for at least 150 min/wk up to 300 min/wk. Initially 40-60% VO2 and then progress to 75% VO2 . Aerobic type of exercises.
FITT principle for metabolic syndrome and obesity
For weight loss: 60-90 minutes sessions.
FITT principle for eldery
5 days/wk for moderate intensity activities, 3 days/wk for vigorous. 40-60% VO2 initially, progressing as tolerated. 30-60 min sessions for moderate, totaling 150-300 min/wk, or 20-30 min/ day for vigorous, totaling 75-100 min/ wk.
FITT principle for pregnancy
3-4 days/ wk, moderate intensity, 15-30 min sessions, accumulating to 120 - 150 min/ wk of dynamic, rhythmic physical activity using large muscle groups.
FITT principle for cancer
3-5 days/ wk of aerobic exercise, 2-3 days/ wk for resistance training. 40-60% VO2 max. 150 min/ wk for moderate intensity, 75 min/ week for vigorous activity.
An outpatient physical therapist gets a referral from a bariatric surgeon for a patient who is moderately obese with poor cardiovascular endurance. Which exercise program prescription is the MOST APPROPRIATE to start with?
5 times a week, a combination of cycling and walking for 45 mins/day at normal walking/cycling pace
A patient underwent an ACL reconstruction surgery 6 months ago. While
treating this patient, the patient states that they are experiencing an intense
pressure feeling in their right lower leg when they are trying to run on the
treadmill. They mention that their leg feels numb, and upon assessment, it
looks very pale. The physical therapist notices that there is tenderness in the
midshaft area of the lower leg. What should the physical therapist be
thinking as the MOST LIKELY cause, and what next step of action should be
taken?
Acute Compartment syndrome – Call EMS
6 P's: pain, pallor, pulselessness, paresthesia, palpable pressure, paralysis
DVT
hallmark signs and symptoms are sudden onset of SOB and rapid and shallow breathing (tachypnea)
-Other signs and symptoms include swelling in the lower extremities, anxiety,
fever, excessive sweating (diaphoresis), a cough, and blood in the sputum (hemoptysis).
Aortic abdominal aneursym
Pulsating feeling in the abdomen, abdominal bulge
Appendicitis
Tenderness at McBurney's point, RLQ pain, mild fever
Acute compartment syndrome
6 'P's: Pain, Palpable tenderness, Paresthesia, Pallor, Paresis, Pulselessness
Myocardial ischemia/cardiac arrest
Left neck and jaw pain along with chest pain
Cauda equina
Saddle anesthesia, loss of bowel bladder function, urine retention, lower extremity weakness
Anaphylaxis (allergic reaction)
Sudden hives, itching, shortness of breath, rapid or weak pulse
Diabetic ketoacidosis
Excessive thirst, confusion and difficulty concentrating and fruity odor in breath
Heat stroke
High Body Temperature (>104°F), Altered Mental Status (confusion,
disorientation, loss of consciousness), Hot, Dry Skin, Tachycardia, Headache
A patient presents with sudden onset of sharp chest pain, shortness of breath, and hemoptysis. They have a history of recent long-haul travel. Physical examination reveals tachypnea and a heart rate of 110 beats per minute. What is the MOST LIKELY diagnosis?
pulmonary embolism
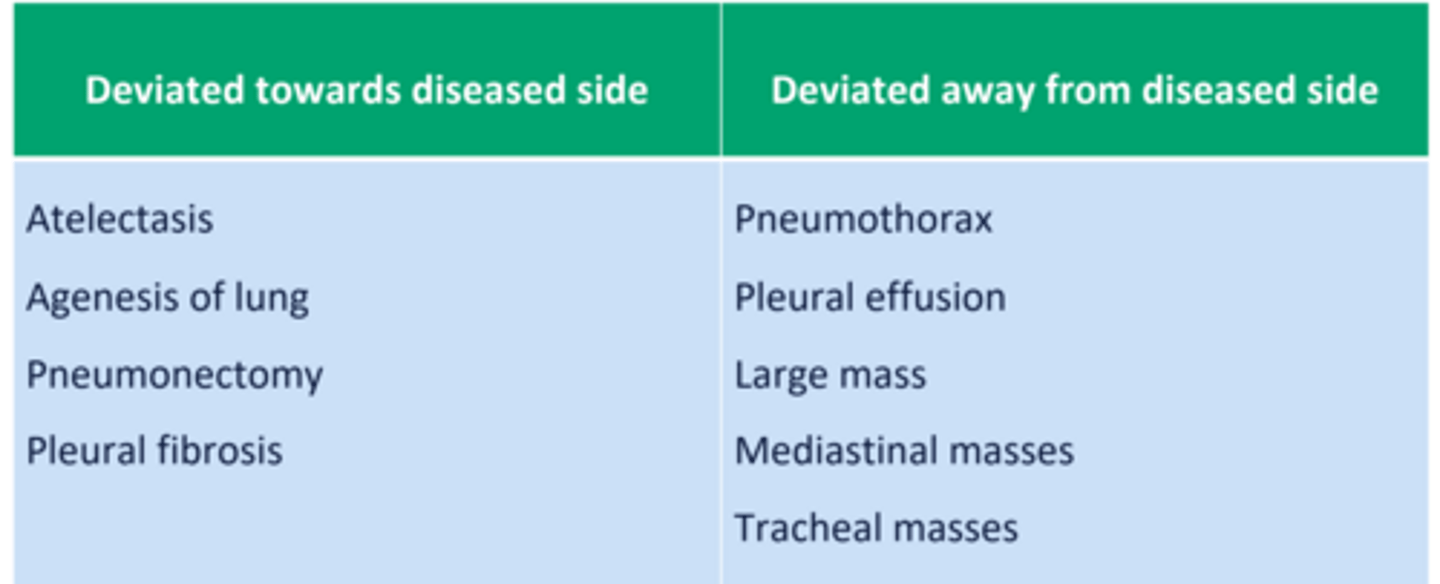
Tracheal deviations
more space present: pull towards
less space: push away "inn is full"