Neuropathology of Brain Tumors
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
15 Terms
What is the difference between an extra-axial and intra-axial tumor? What are the miscellaneous cell types that can give rise to tumors?
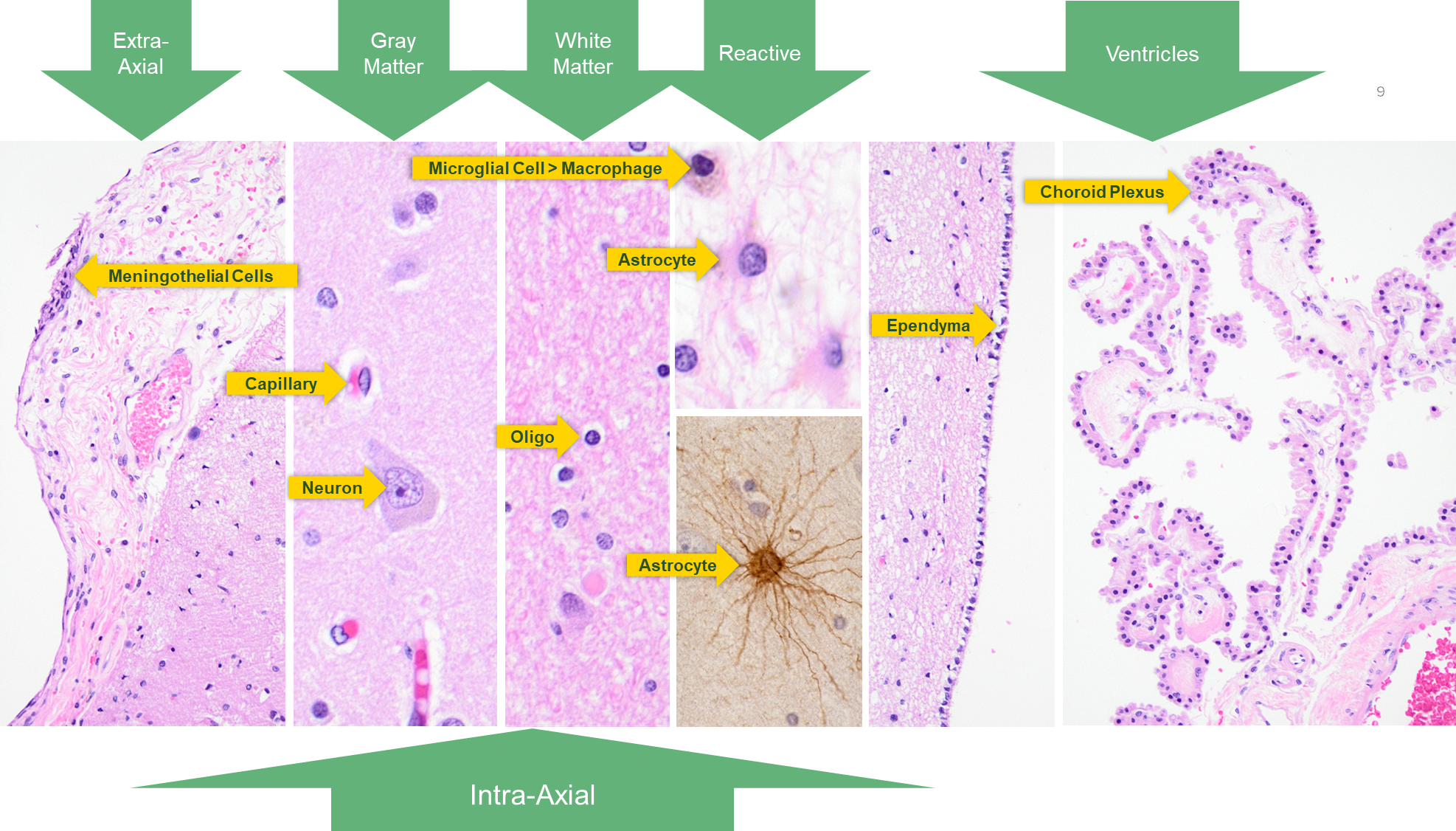
Extra-axial with a common example being a meningioma is a tumor that affects the outside of the brain
→ Meningothelial Cells
Intra-axial means inside the brain with the most common example being infiltrating/diffuse gliomas. Originate from the brain parenchyma
→ Neurons
→ Vessels
→ Glial Cells
Other cell types that can cause tumor formation are:
→ Ependymal cells
→ Choroid Plexus
→ Schwann Cells
What does meningioma look like?
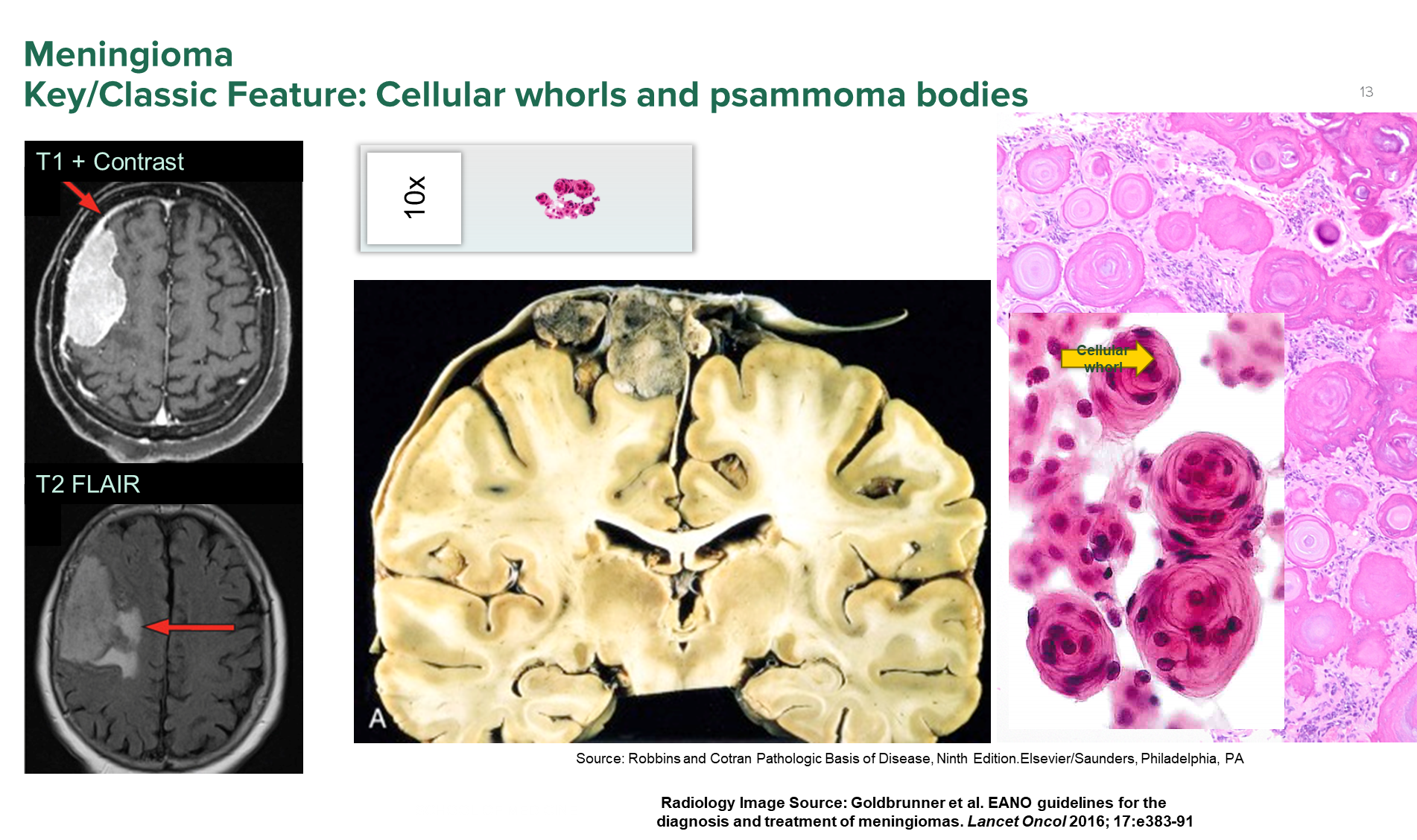
Meningioma is a extra-axial tumor that grows on the meninges
1) On CT imaging, it will appear very bright on T1 imaging
→ The tumor will appear on the outside of the brains surface, pushing down on the brain parenchyma itself
2) On histology you will see cellular whorls and psammoma bodies
What are meningiomas?
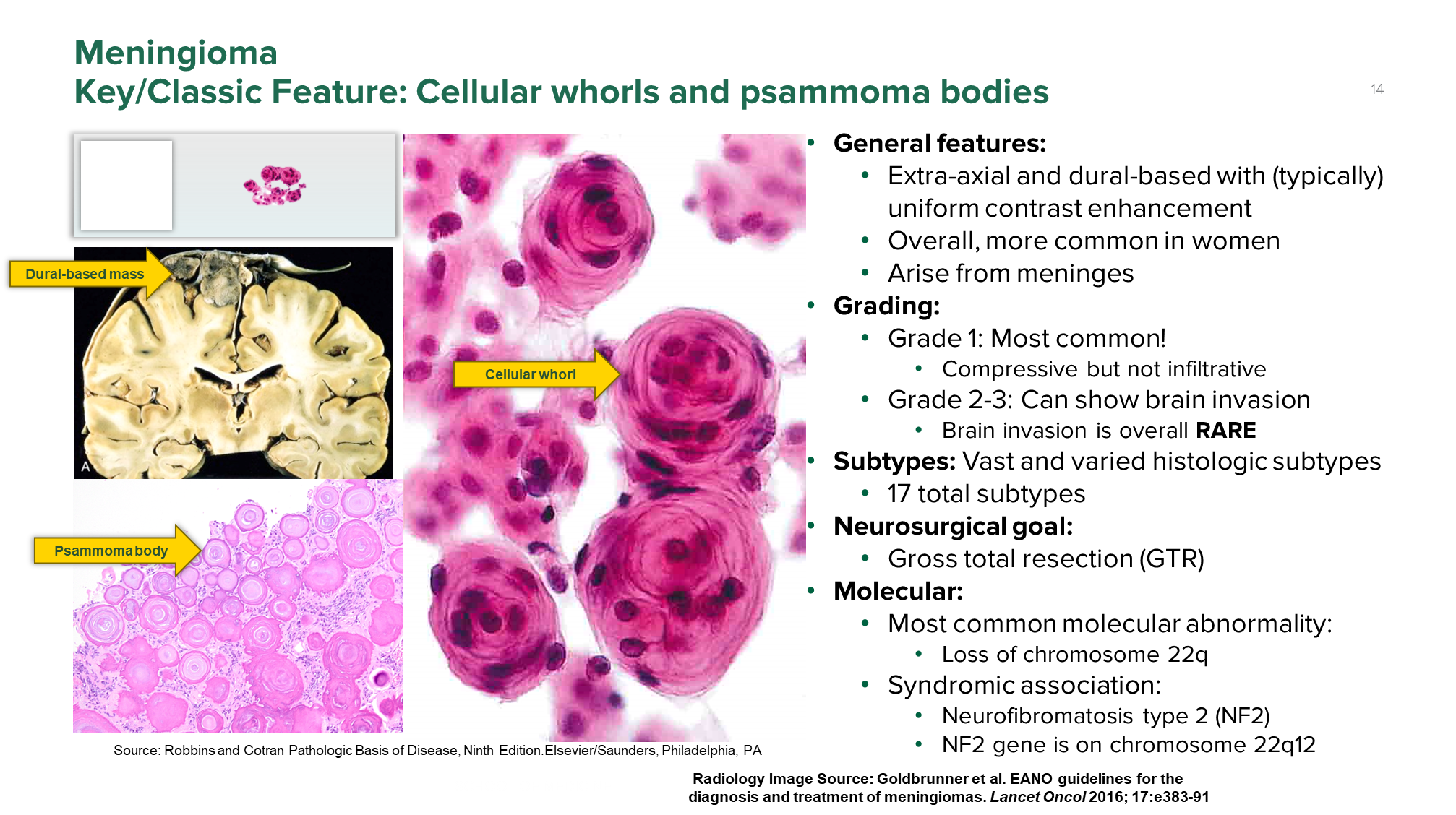
Meningioma is a extra-axial tumor of the meninges that will commonly appear in women
1) Subdivided into three grades, with grade 1 being the most common and the form that compresses the outside of the brain
→ grades 2-3 can show brain invasion but is very rare
→ further subdivided into 17 subtypes
2) Most commonly caused by a loss of chromosome 22q
→ is also associated with neurofibromatosis type 2 (NF2) which is an autosomal dominant condition associated with a mutation on chromosome 22q
3) Main treatment is surgical resection
What is the classic gross/histological presentation of Pilocytic Astrocytoma?
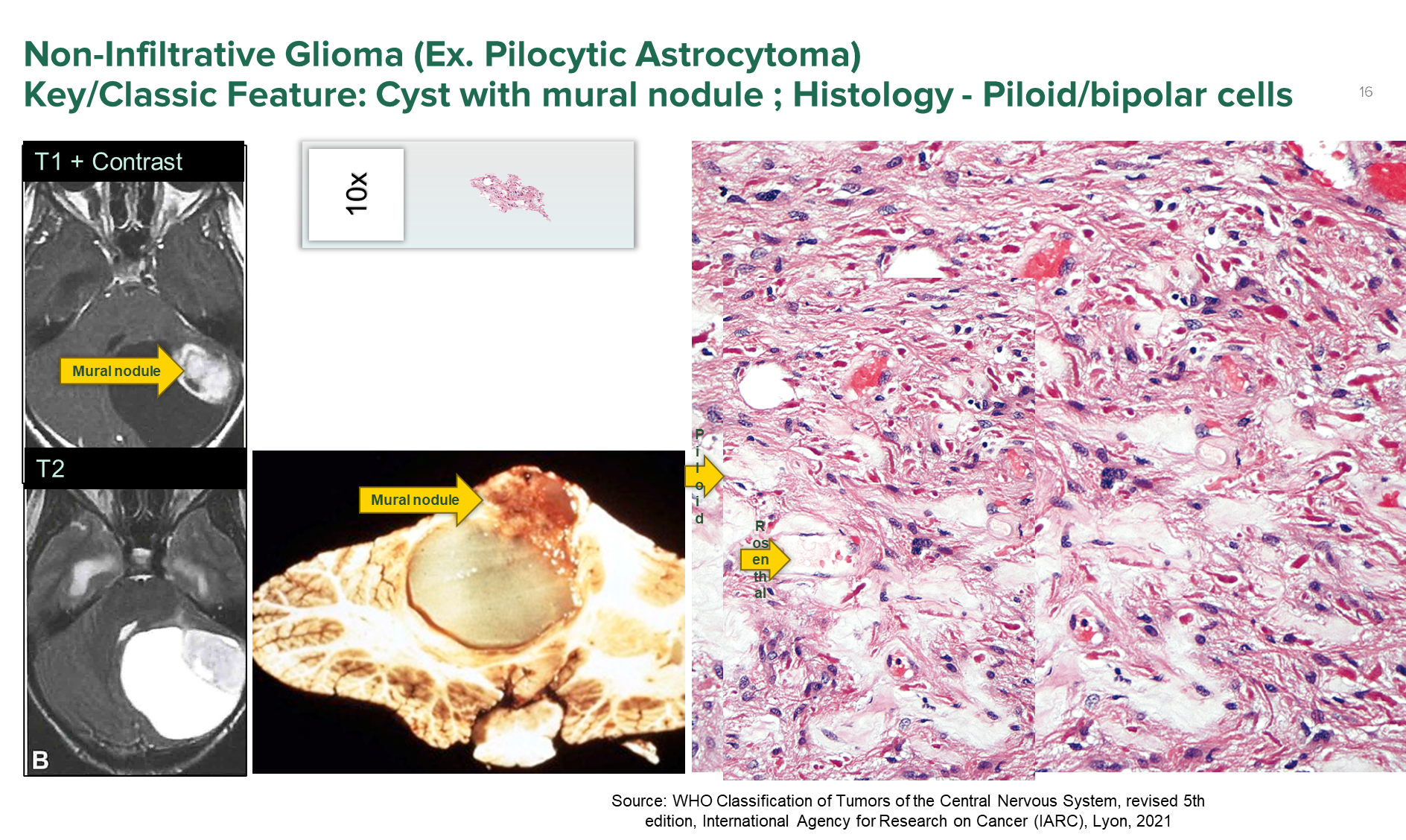
Pilocytic Astrocytoma
1) on imaging patients will have a cyst with a mural nodule (cyst with a nodule on the inside)
2) on histology there are two identifiable cells: piloid (bipolar cells) and rosenthal fibers
→ piloid cells are abnormal cells originating from astrocytes that look like hairlike bipolar processes
→ rosenthal fibers are corkscrew shaped inclusions of astrocytes
3) grade 1 tumor
What is the classic gross/histological presentation of Oligodendroglioma?

Oligodendroglioma is a lower grade infiltrating glioma
1) Classically presents as a fried egg appearance in the histology caused by round monomorphic tumor cells
2) Caused by a IDH 1/2 mutation and co-deletion of chromosome 1p/19q
→ both are required in order to have oligodendroglioma
What is glioblastoma?
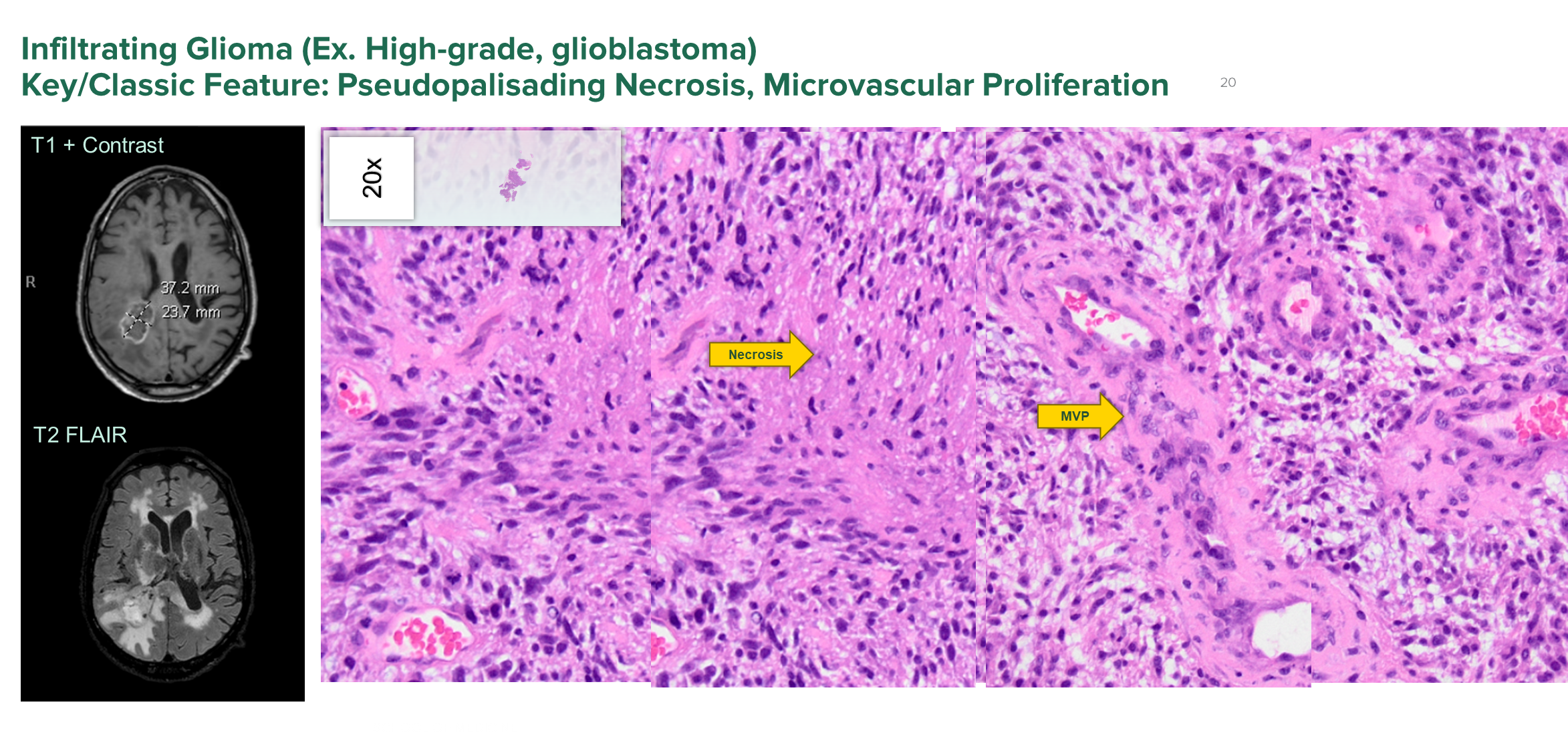
Glioblastoma is a high-grade glioblastoma which is a form of infiltrating glioma
1) Classically seen with pseudo-palisading necrosis and microvascular proliferation
→ pseudopalisading necrosis is where the cells will cluster around a central area of necrosis
→ MVP is where cells secrete cytokines in order to create their own vasculature
2) Tumors are grade 4 and is the most common primary malignant brain tumor in older adults
→ has a very poor prognosis
What is Diffuse Midline Glioma, H3K27-altered?
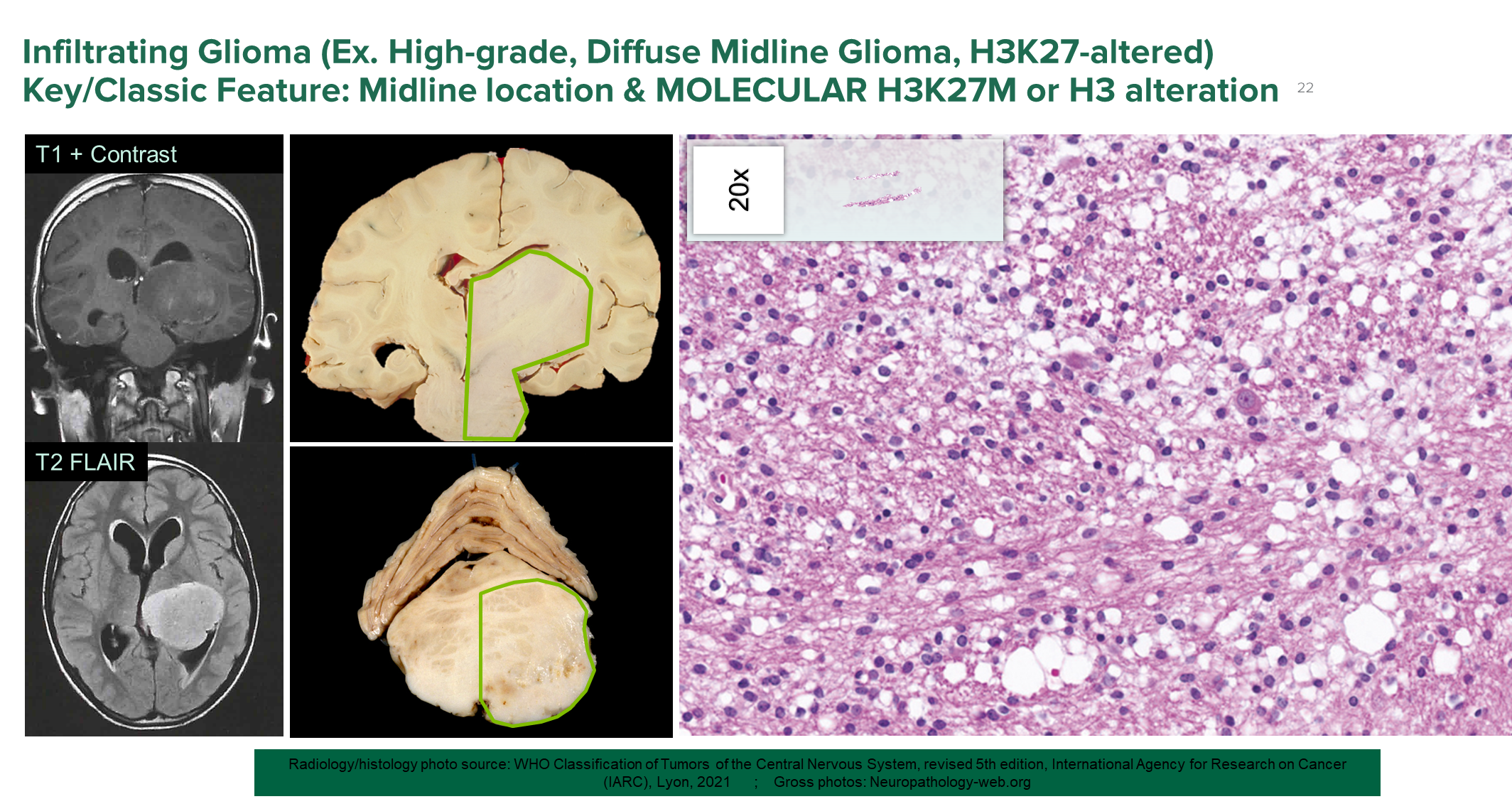
Diffuse Midline Glioma is a infiltrating glioma that is located in midline locations
1) Caused by an alteration of histone 3 due to a H3 K27M mutation leading to an expansion of the basal ganglia area or some other midline location
→ can often appear bland histologically with no major features, but is very aggressive grade 4 tumor
2) Is only biopsied but is not-resected as you can’t remove parts of the pons and stuff
What is an Ependymoma?
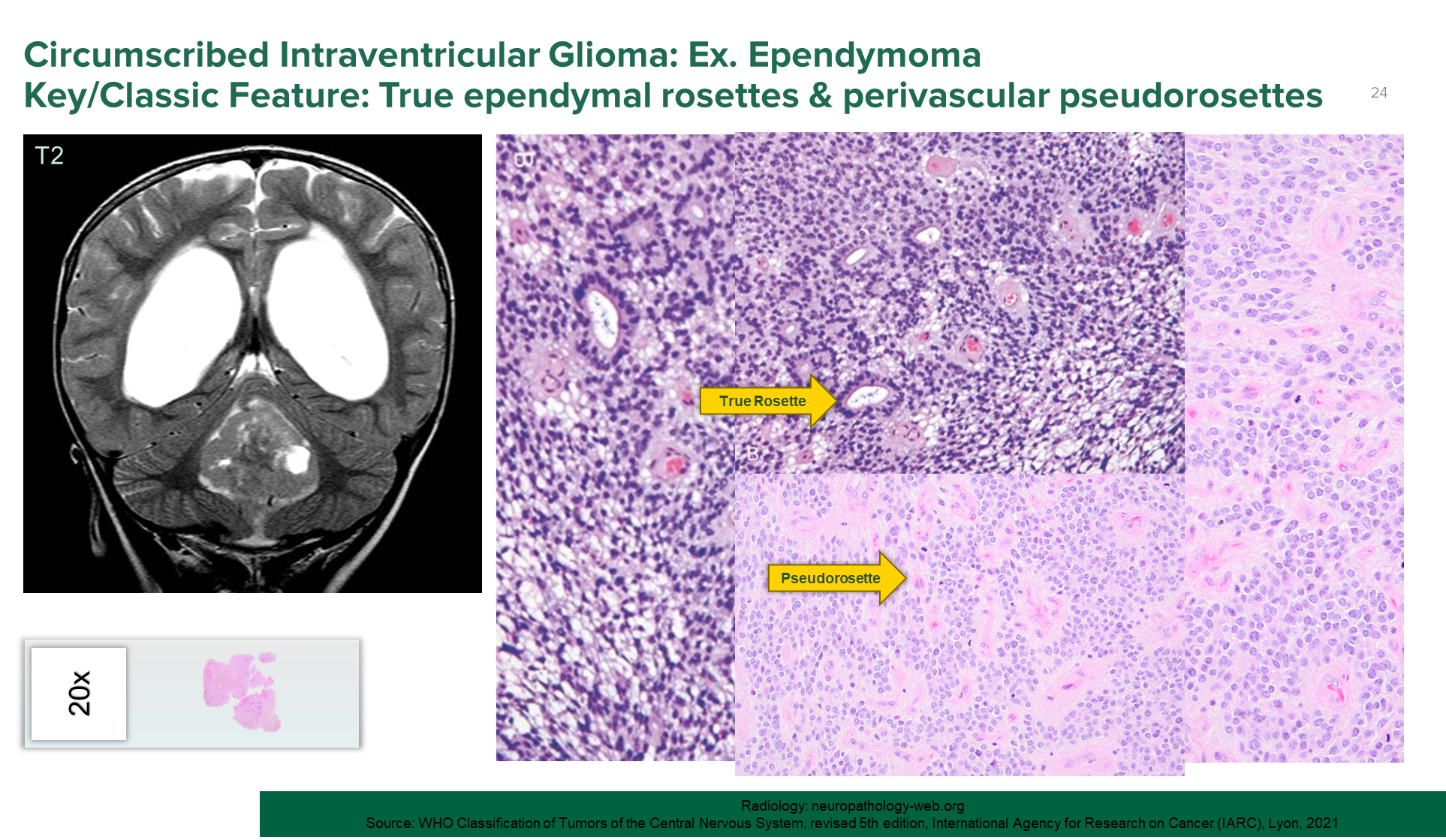
Ependymoma is a circumscribed intraventricular glioma and is caused by a tumor formed from the ependymal cells lining the ventricles
1) Patients will have enlarged ventricles and a posterior fossa mass
→ causes a blockage of CSF drainage leading to obstructive hydrocephalus
2) Histologic features are true rosette and pseudorosettes
→ true rosette is a tumor cell arranged around empty central lumen
→ pseudorosette are tumor cells arranged around a central structure like a blood vessel
What is Primary CNS Lymphoma?
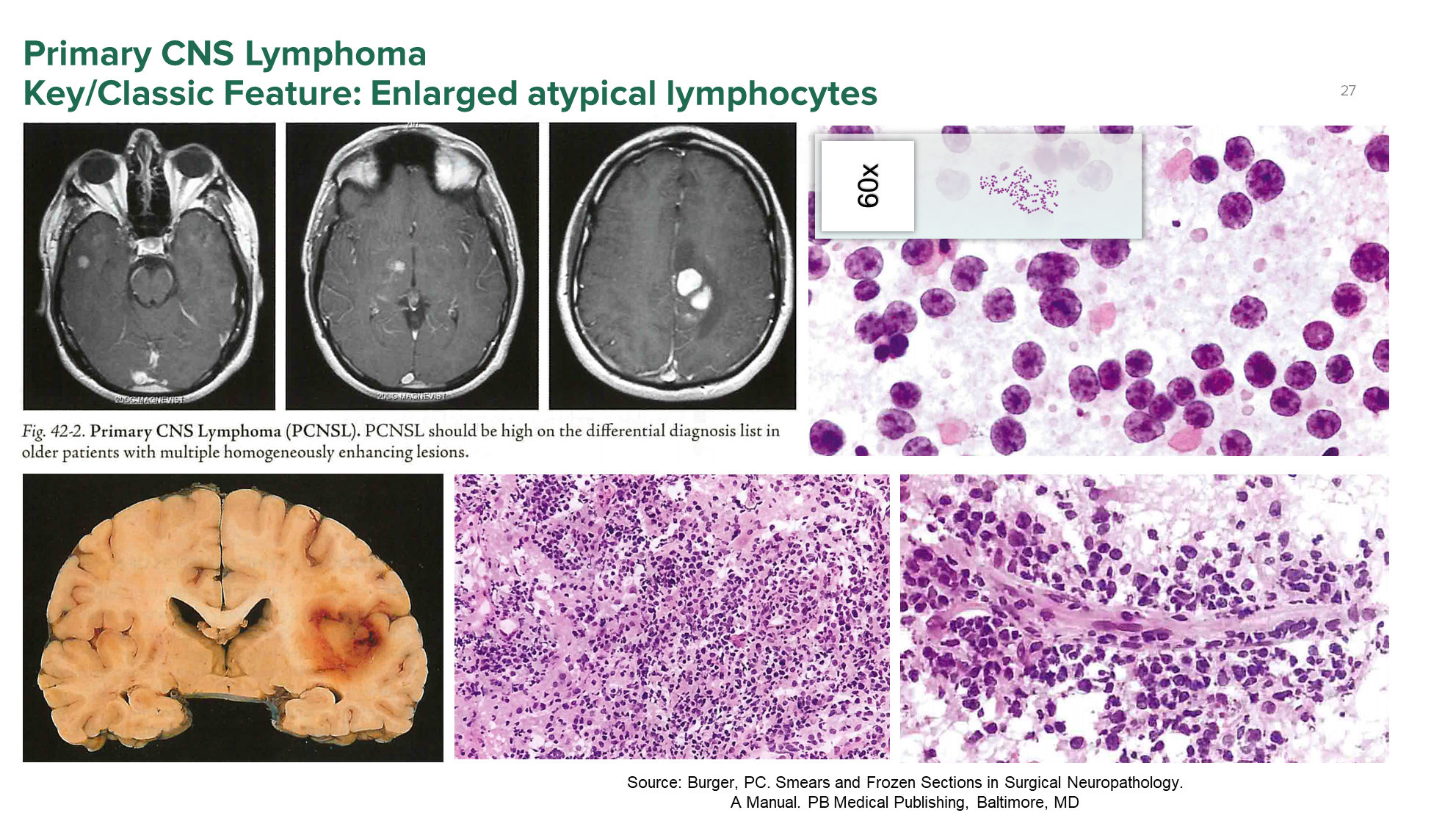
Primary CNS Lymphoma is a tumor that originates from B-cells/lymphocytes
1) Identifiable on histology from enlarged atypical lymphocytes
→ round blue cells that will typically line up around vessels
2) Lymphoma are not resected but treated with methotrexate
→ if these lymphomas are CD20+, rituximab can be used as well
What is Medulloblastoma?
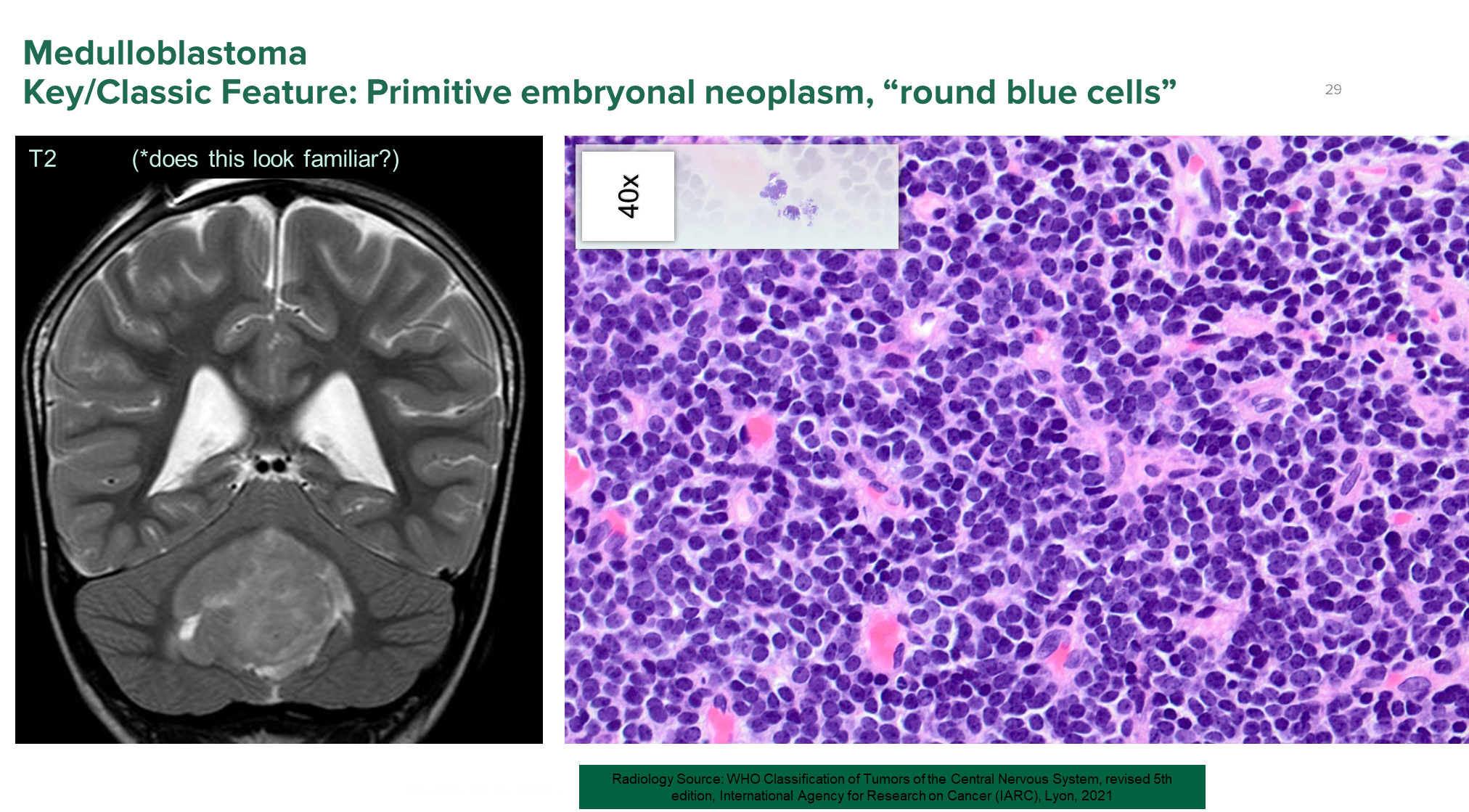
Medulloblastoma is a tumor commonly seen in pediatric patients and is a malignant brain tumor of the cerebellum (posterior fossa)
1) Histologically presents as round blue cells similar to a lymphoma while grossly appearing like an ependymoma due to midline involvement of the cerebellum
→ All are grade 4
2) Most common tumor to cause spinal drop metastasis or spread of cancer cells to the spine
What is a Pituitary Adenoma?
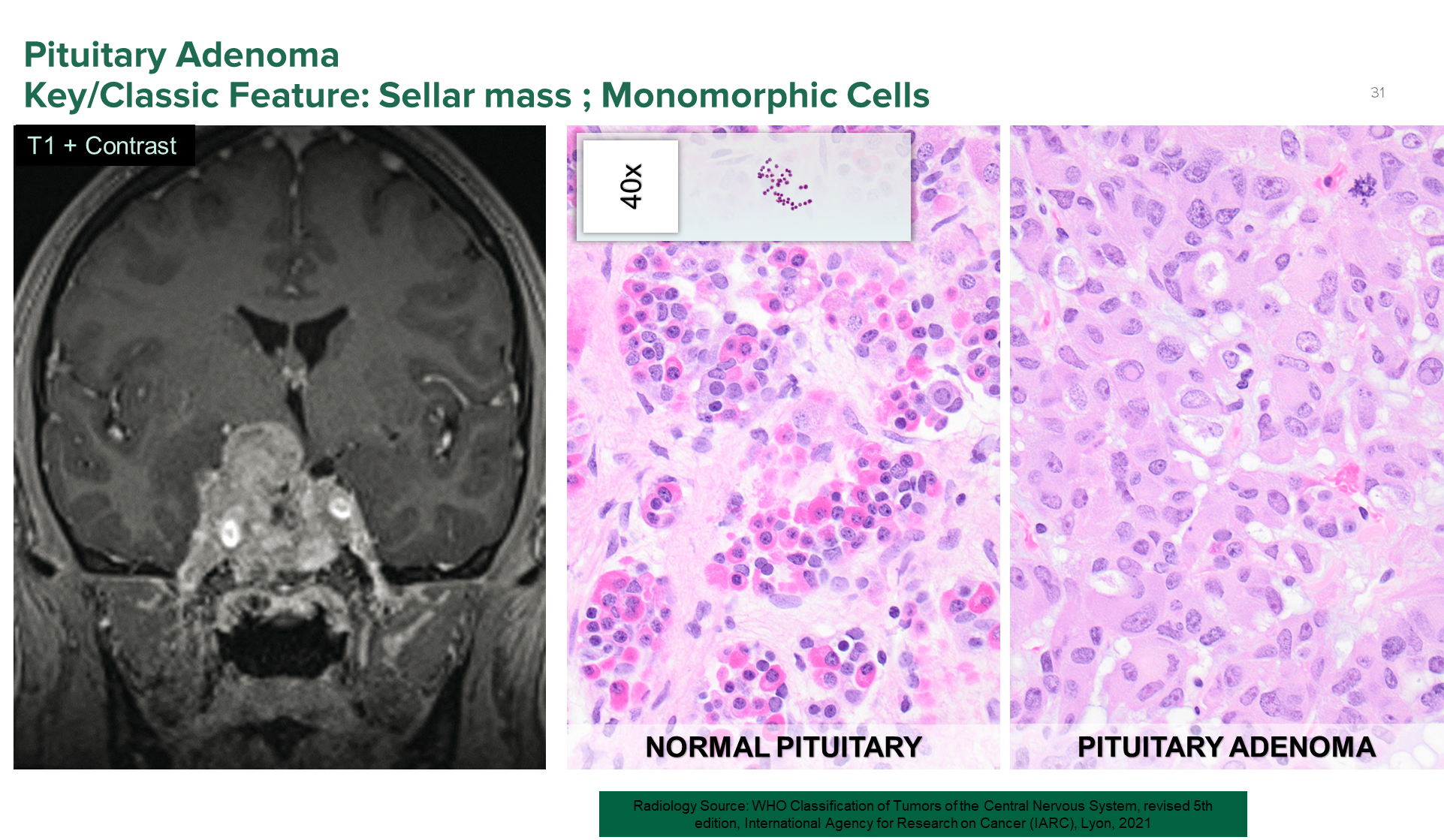
Pituitary Adenoma is a tumor of the pituitary gland situated in the sellar diaphragm
1) These tumors are often slow growing, but may expand to compress the surrounding tissue
→ if they compress the optic chiasm it can cause bitemporal hemianopsia
→ will often secrete hormones such as prolactin leading to milk production
→ may also have acetylcholine production or Cushing’s disease
2) Normally you should see a colorful tissue characteristic of glandular tissue
→ if you see sheets of tissue that all looks monochromatic and uniform you would be concerned for adenoma
What is a Crangiopharyngma?
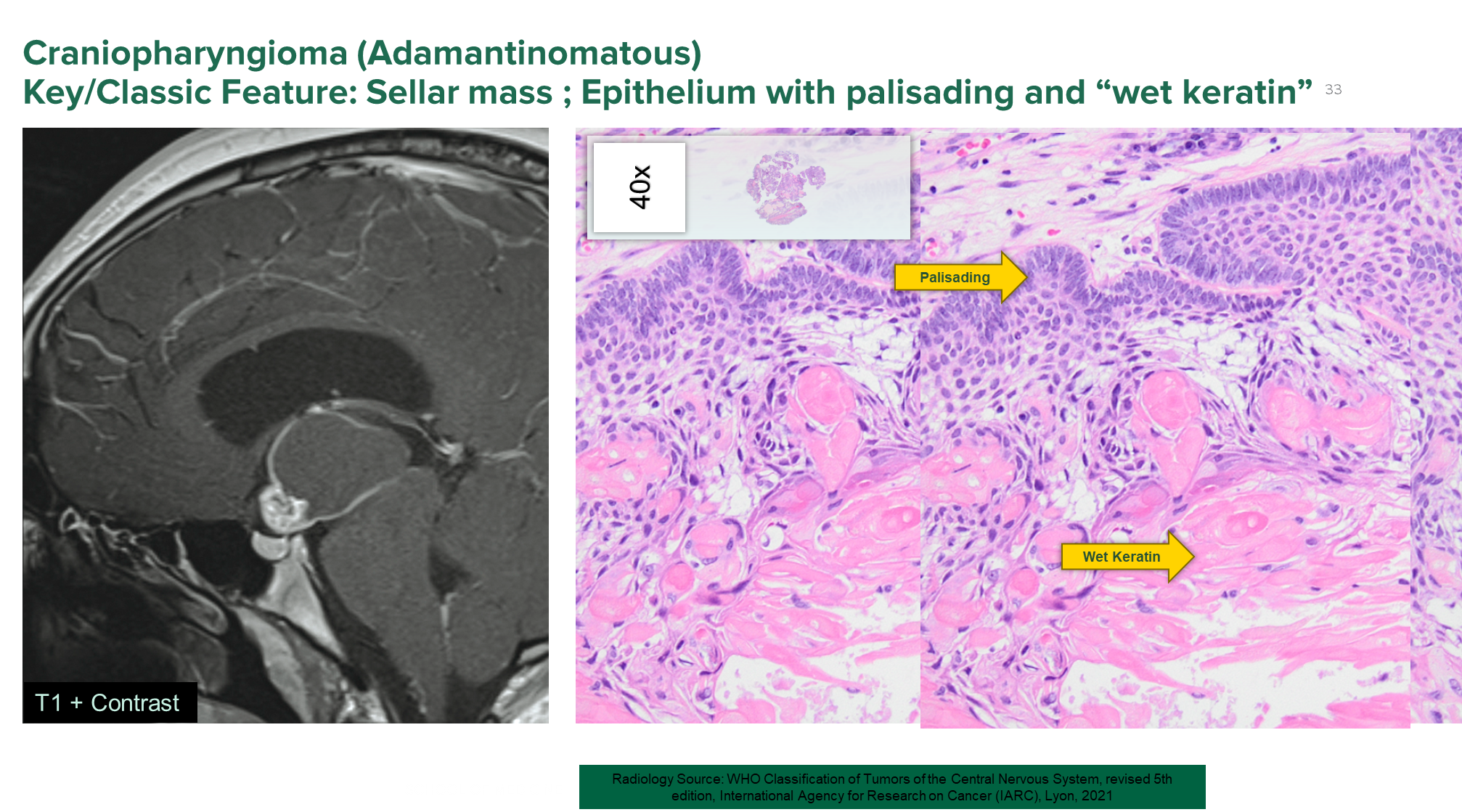
Crangiopharyngioma is a local tumor derived from Rathke’s pouch or the embryological precursor to the anterior pituitary - suprasellar
1) Described as having wet keratin or squamous epithelium that is producing large amounts of keratin
→ also described as having palisading epithelium or a fence like formation with cells lining up along the basement membrane - looks like skin
2) Grade 1 Tumor, but has two subtypes
→ Adamantionmatous - common form caused by beta-catenin mutations
→ Papillary - caused by BRAF-V600 mutations
What is a Schwannoma?
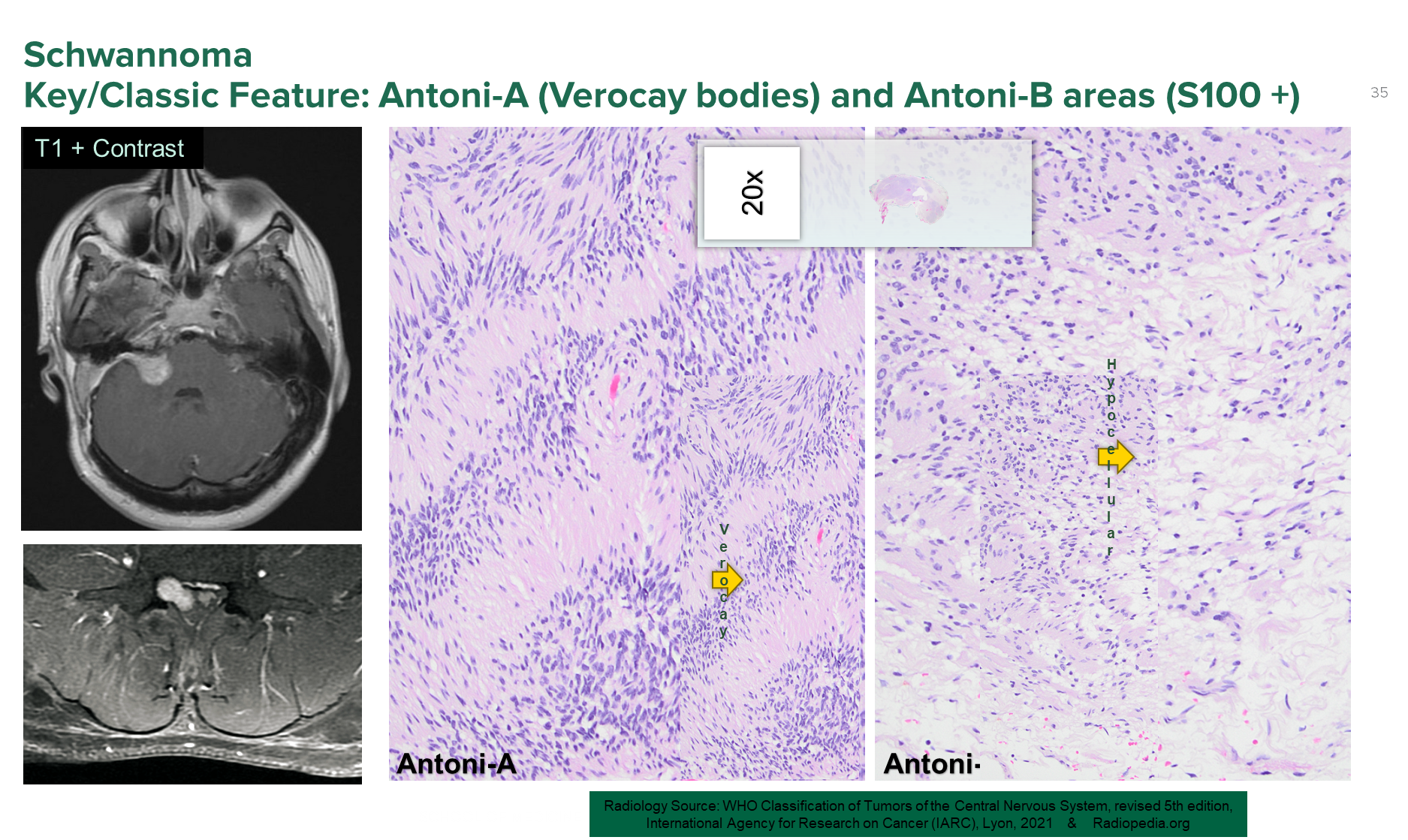
Schwannoma are tumors of the Schwann cells located at points where the CNS meets the PNS and is found commonly at the cerebellopontine angle
1) Radiologically causes a small dumbbell shaped mass where the CNS enters the periphery
→ Antoni-A areas or highly cellular regions with Verocay bodies
→ Antoni B areas or hypocellular loose regions
2) These tumors will stain for S100+ protein which is found in neural-crest cell derived cells
→ because these tumors are Schwann cell derived they will stain positive for S100
→ may also produce melanin because they are related to melanocytes which are also neural crest cell derived (caused by a mutation in PRKA1A)
How would you identify metastatic cancer in the brain
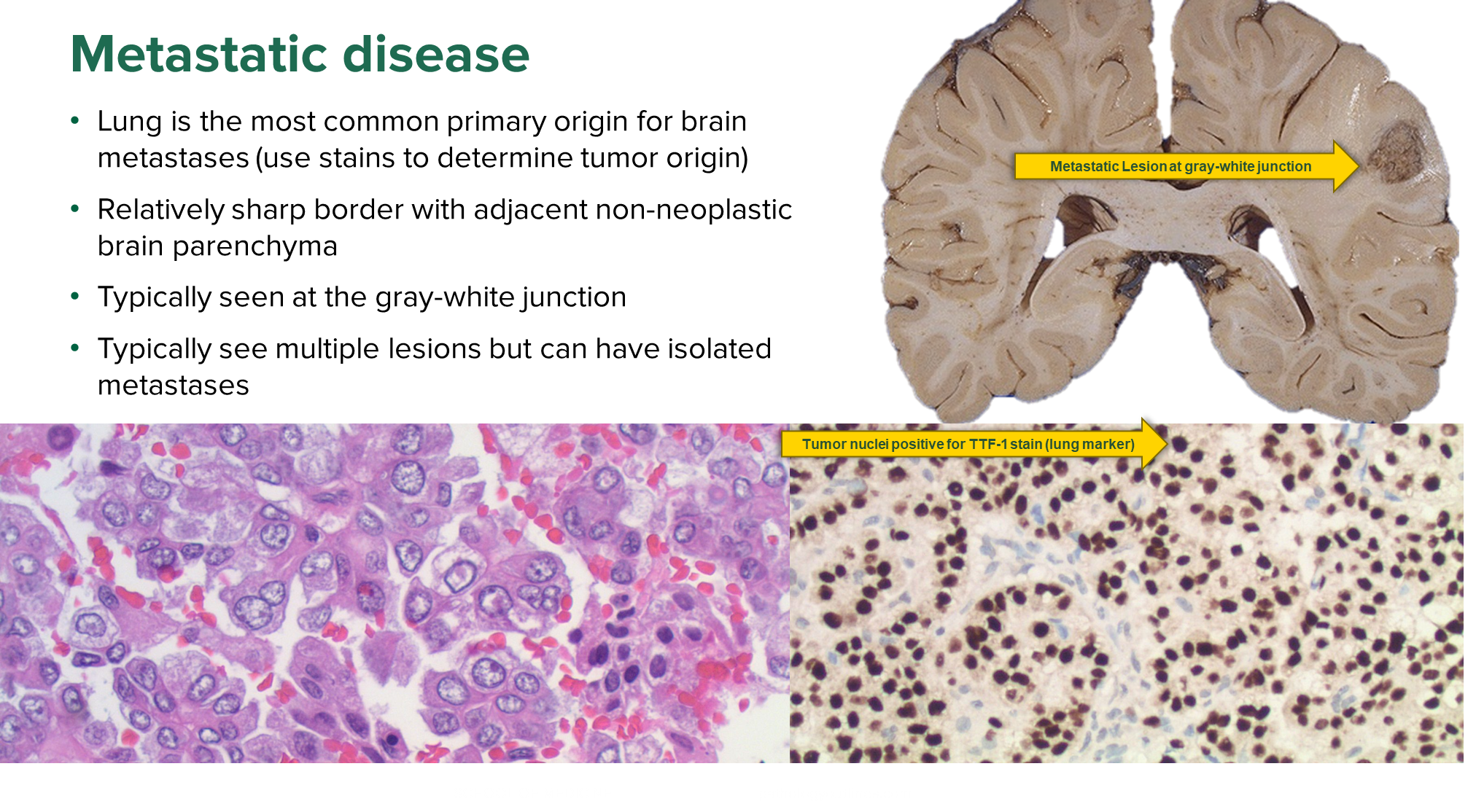
Metastatic cancer typically originates from the lungs
→ identified by a sharp border/well circumscribed mass and will be around the gray-white junction
→ often presents with multiple lesions
When would a lumbar puncture be contraindicated? (5)
Absolute Contraindications
→ infected skin over the needle
→ unequal pressure between the supratentorial and infratentorial compartment
Relative Contraindications (inadvisable)
→ increased intracranial pressure
→ coagulopathy
→ brain abscess