Stress Echo - week 13
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
92 Terms
What is stress echo?
non-invasive diagnostic method to assess known or suspected CAD
What is one basic form of stress echo?
Using a treadmill or an ergometer (upright or supine) to exercise the heart
What is the other basic form of stress echo?
Using various drug agents to simulate exercise (inotropic positive) = pharmacologic stress test
What is the goal of stress echo?
to induce myocardial ischemia by augmentation of oxygen demand to the heart in the absence of adequate supply
During the stress echo test what is recorded?
EKG and BP
Why are ultrasound images captured?
To detect changes in wall motion that may occur
What are the types of stress tests performed?
ETT
SE
DSE
What is ETT?
exercise treadmill test
recording EKG and BP changes during exercise
What is SE?
stress echocardiography
in addition to EKG and BP changes, capture of US images before and after exercise is performed to indirectly assess coronary perfusion to different wall segments of the LV
What is DSE?
dobutamine stress echocardiography
pharmacologically induced high HR to mimic exercise with recording of EKG, BP and US images
What are the objectives for stress echo?
Evaluation of known or suspected CAD
Risk stratification of patients before non-cardiac surgery after MI or interventional procedures and prior to start an exercise/diet program
Evaluation of LV systolic function - global and segmental
Identification of viable, hibernating or stunned myocardium with LV dysfunction
Evaluation of the LV function and valvular hemodynamics and/or cardiomyopathies
At rest, the myocardium is well supplied with?
oxygenated blood through the coronary artery and LV systolic function is normal
As stress and demand for oxygen ____ during exercise or drug induced ______ __, the region supplied by specific vessels will display ____
Increases
increased HR
WMA (hypokinesis, akinesis, dyskinesis) if lesions are present in vessels or their branches
What do WMA generally precede?
EKG changes
How can WMA be assessed?
From the wall score index
What are the 2 categories of contraindications?
Absolute and relative
What are 3 absolute contraindications?
Acute MI less than 72 hours old
Unstable angina
Hemodynamic instability ( systolic BP > 210 mmHg or < 90 mmHg; diastolic BP >110 mmHg)
What are 3 more absolute contraindications?
Uncontrolled cardiac arrhythmias
Symptomatic aortic or subaortic stenosis with pressure gradient > 50 mmHg
Uncontrolled symptomatic HF
What are 3 more absolute contraindications?
Acute myocarditis, pericarditis and infective endocarditis
Acute aortic dissection/large aortic aneurysm
Acutely ill patients
What are 4 more absolute contraindications?
Patients with ambulation problems
Pregnancy
Combative patients or patients who are otherwise judged uncooperative
Patients who refuse the procedure and/or consent may not be obtained
What are relative contraindications?
risk/benefit assessment is performed by the physician
What are 3 relative contraindications?
Unstable angina but asymptomatic for the previous 12 hours
Left main coronary artery disease
Severe arterial hypertension ( systolic BP>170 mmHg, diastolic BP > 100 mmHg)
What are 3 more relative contraindications?
Increased cardiac enzyme levels or electrolyte abnormalities
Significant ischemic EKG changes
Hypertrophic obstructive CM or other forms of outflow obstruction
What are 3 more relative contraindications?
PHTN with MPAP > 50 mmHg or SPAP > 70 mmHg
Tachyarrhythmias/Bradyarrhythmias - high degree of A-V block
Mental or physical impairment leading to inability to exercise
If the echo images are suboptimal, it should be the cardiologist’s decision to? (relative contraindications)
to abort, use contrast agents or continue the SE
Maximal HR =
220 - age
Target HR (85% of age predicted MHR) =
MHR x 0.85
% maximal HR achieved =
MHR achieved/MHR calculated
Double product =
MHR achieved x systolic BP
Rate pressure product =
HR x systolic BP
What is the procedure of flow?
Explain test to the patient
Position EKG electrodes to ensure that echo windows are not obstructed
Obtain resting echo images (digital capture)
Exercise patient
Prepare probe and system for immediate post exercise study
Obtain and record post images rapidly
Select post exercise images, shuffle and review pre and post exercise images
For patient prep, pt should be NPO for?
3 hours prior to test
What is the short cardiac patient hx questionnaire for pt prep?
risk factors for CAD
previous CAD (PTCA, MI, CABG)
previous tests/procedures, medications, indication
goal of the test
What should the pt sign for pt prep?
consent form
informed of procedure
What should be obtained for pt prep?
Resting BP supine and standing
a resting 12 lead EKG
What are the exercise protocol?
Standard Bruce protocol
Modified Bruce protocol
Naughton protocol
What is the modified Bruce protocol utilized in?
in pts with lower exercise capacity
Resting images =
Baseline images
What does the Bruce standard protocol do?
will run on stages of 3 minutes when the treadmill settings change to higher speed and incline and BP is recorded at min 2:30 of every stage until termination
What happens when the endpoint is reached?
the patient is moved quickly on the bed and post-exercise images are acquired promptly ( within 60 seconds) with HR maintained at high rate
What are 2 of the end points?
When target or predicted HR is achieved = 90% of MHR for 1 minute
Intolerable symptoms
What are 3 more end points?
Significant ST segment changes occur
elevation of >1mm or depression of >2 mm when compared to baseline EKG
Severe angina pectoris
What are 2 more end points?
Sustained SVT, ventricular arrhythmias or A-V block
Hypertensive or hypotensive response
In recovery what do you monitor and obtain?
monitor vital signs
obtain EKG recordings
When do you obtain EKG recordings for recovery?
every 2 minutes for 10 minutes or until the BP and HR return to baseline
For interpretation, what do you note?
patient symptoms during exercise
For interpretation, what do you record?
EKG changes
arrhythmias
For interpretation, what do you evaluate?
global and segmental LV systolic function pre and post exercise
For interpretation, what is assigned?
Assign a wall score to each segment well visualized
calculate a wall motion score index
What is a normal response?
All walls become hyperdynamic with symmetric wall thickening and equal excursion in all segments
What are 2 more normal responses?
EF increases minimum 5% post exercise
LV end -systolic dimension decreases
What is an abnormal response?
Resting hypokinetic wall segment that worsens with exercise may represent hibernating myocardium
What are 2 more abnormal responses?
New segmental WMA using wall motion score index
Decreased EF and longitudinal strain - global LV systolic dysfunction
What is a Dobutamine Stress Echo?
pharmacologic alternative to exercise echocardiography for those who are unable to exercise or have specific indications
What are the advantages of Dobutamine Stress Echo?
useful for myocardial viability assessment
allows Doppler interrogation during the test and allows immediate detection of an abnormal response and facilitates cessation of testing
How long should a pt be NPO for dobutamine stress echo?
3 hours prior to test
What should be obtained for pt prep (dobutamine)?
Cardiovascular history
What should be explained and signed for pt prep (dobutamine)?
The procedure
side effects Dobutamine
potential complications explained
Patient consent form signed
What should be placed and recorded for pt prep (dobutamine)?
Placement of EKG leads
resting EKG recorded
What should be started and prepared for pt prep (dobutamine)?
Starting IV access
What is Dobutamine?
synthetic catecholamine that augments myocardial contractility
What is the dobutamine calculation?
to determine the number of ml/hr which equals 1mcg/kg/min, determine the patient’s weight in kilograms (pounds/2.2)
What is the equation for the dobutamine calculation?
Weight x 60 min/100 mg/ml
What will the answer of the dobutamine calculation provide and determine?
The answer will provide the ml/hr and to determine the amount of the Dobutamine to be administered
multiply the ml/hr by 5, 10, 20, 30 and 40 respectively
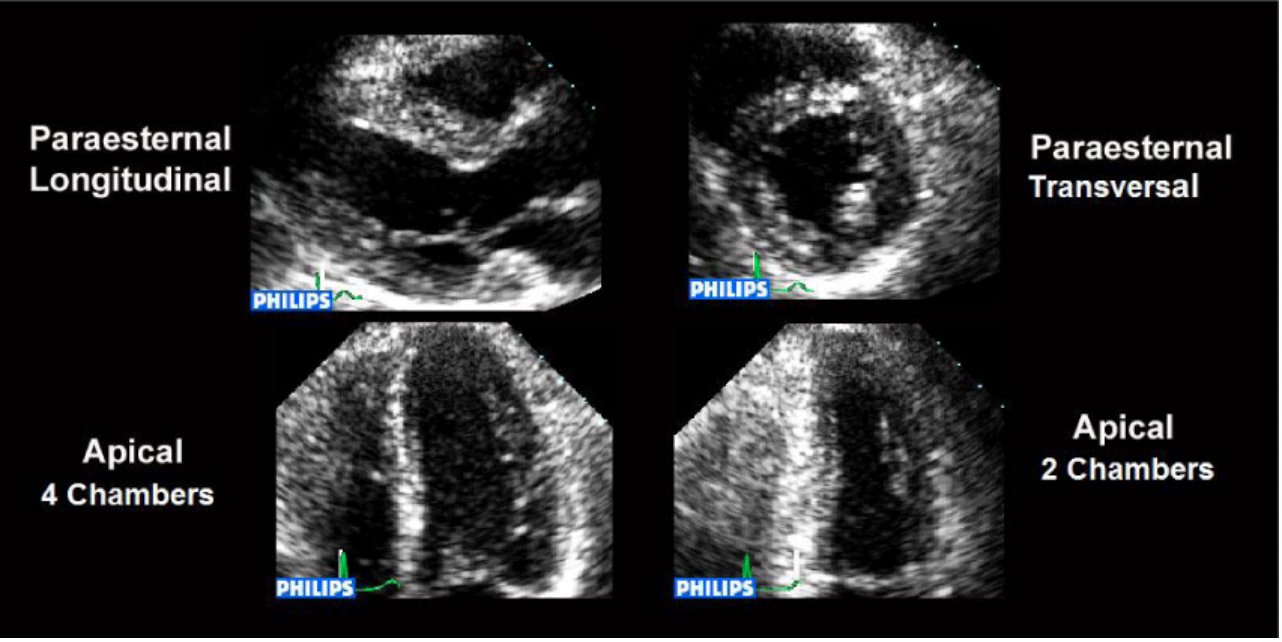
What are the views for resting images (after a baseline echo)?
PLAX
PSAX
AP-4Ch
AP-2Ch
AP-3Ch (optional)
Views demonstrating valvular color flow
What is the first step of a dobutamine procedure?
Infuse Dobutamine with a starting rate of 5 mcg/kg/min or 10 mcg/kg/min
What is the 2nd and 3rd step of the procedure (dobutamine)?
At 2:30 min begin obtaining views, BP, EKG
Increase Dobutamine infusion to 10 mcg/kg/min at 3 min
What is the 4th and 5th step of the procedure (dobutamine)?
At 5:30 min obtain a second set of views, BP and EKG
Increase Dobutamine to 20 mcg/kg/min at 6 min
What is the 6th and 7th step of the procedure (dobutamine)?
at 8:30 min obtain third set of views, EKG, BP
Increase Dobutamine to 30 mcg/kg/min at 9 min
What is the 8th, 9th and 10th step of the procedure (dobutamine)?
At 11:30 min obtain fourth set of views, BP, EKG
Increase Dobutamine to 40 mcg/kg/min at 12 min
At 14:30 obtain a fifth set of views, BP and EKG
What is the last step of the procedure (dobutamine)?
At 15 min obtain 12 lead EKG, note HR and increase Dobutamine infusion up to 50mcg/kg/min until peak HR is achieved
What is the procedure for dobutamine stress echo?
Infuse Dobutamine with a starting rate of 5 mcg/kg/min or 10 mcg/kg/min
At 2:30 min begin obtaining views, BP, EKG
Increase Dobutamine infusion to 10 mcg/kg/min at 3 min
At 5:30 min obtain a second set of views, BP and EKG
Increase Dobutamine to 20 mcg/kg/min at 6 min
At 8:30 min obtain a third set of views, BP and EKG
Increase Dobutamine to 30 mcg/kg/min at 9 min
At 11:30 obtain a fourth set of views, BP and EKG
Increase Dobutamine to 40 mcg/kg/min at 12 min
At 14:30 obtain a fifth set of views, BP and EKG
At 15 min obtain 12 lead EKG, note HR and increase Dobutamine infusion up to 50mcg/kg/min until peak HR is achieved
What happens if no endpoint is reached?
Dobutamine infusion is continued up to 50mcg/kg/min with atropine sulfate administered to increase HR
(additional doses of 0.25 to 0.5 may be repeated at 1 min intervals to a maximum of 2mg)
What may be the remaining images for dobutamine?
a combination of
low stress
intermediate stress
post atropine images or recovery images
What are 3 endpoints for dobutamine?
Development of new segmental WMA or worsening preexisting segmental WMA
> 1mm downsloping ST segment depression with segmental WMA
Angina pectoris
What are 3 more endpoints for dobutamine?
Achievement of >85% of MPH determined by age
BP > 210/120 mmHg
Symptomatic hypotension with a fall >40 mmHg
What are 3 more endpoints for dobutamine?
Tachyarrhythmias
Significant increase in valvular pressure gradient
Maximum dose of Dobutamine at 50 mcg/kg/min
What are 2 more endpoints for dobutamine?
Side effects due to Dobutamine (nausea, vomiting, headache)
Patient request to end test
What is the recovery for dobutamine?
Evaluate BP
12 lead EKG at 2 min interval until back to baseline or HR below 100 bpm
finalize US images.
What is a normal response for dobutamine?
hyperdynamic wall motion and increased EF
What are 2 abnormal responses for dobutamine?
Hypokinesia, akinesia or dyskinesia or failure of a wall to increase systolic thickening and excursion or increase in LV volume
Improvement of a hypokinetic, akinetic segment during administration of low dose Dobutamine (5 or 10 mcg/kg/min) suggests the presence of viable myocardium
What are 2 more abnormal responses for dobutamine?
Determine wall motion index
Determine E/e’ ratio at rest and peak dose - LV diastolic function
What is the determination of myocardial viability performed to evaluate?
evaluate if revascularization can improve myocardial contractility and LV systolic function
What are the 4 different clinical scenarios when evaluating myocardial response to low and high dose of dobutamine, with resting akinetic hypokinetic segment?
Monophasic (sustained) response
Biphasic response
Nonphasic response
Ischemic response
What is a monophasic (sustained) response?
if the myocardium is viable with NO stenosis of the coronary artery perfusing the akinetic/hypokinetic segment
myocardial contractility increases continuously with low/high dose of Dobutamine
What is the biphasic response?
if the myocardium is viable but the coronary artery that perfuses the segment is severely stenotic
myocardial contractility improves initially with low dose of Dobutamine but worsens with higher dose
What is a biphasic response a typical response for?
hibernating myocardium
suggests increased potential for recovery of function
What is a nonphasic response?
when the myocardium is scarred, with NO myocardial viability
there is NO myocardial thickening at rest or with low/high dose of Dobutamine
What is an ischemic response?
a worsening of function without contractile reserve suggests a stress-induced ischemic myocardium due to flow limiting stenosis of the corresponding coronary artery
(restenosis)
What is Diastolic function evaluation for stress echo in non-ischemic HD evaluation?
in patients with HF to detect diastolic filling impairment with exercise
(restrictive CM)
What is cardiomyopathy for stress echo in non-ischemic HD evaluation?
hypertrophic and dilated CM
What is native valvular disease for stress echo in non-ischemic HD evaluation?
mild to moderate AS, MR or stenosis severity evaluation