CVR - Cardiac Electrical Activity and Pathologies
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
12 Terms
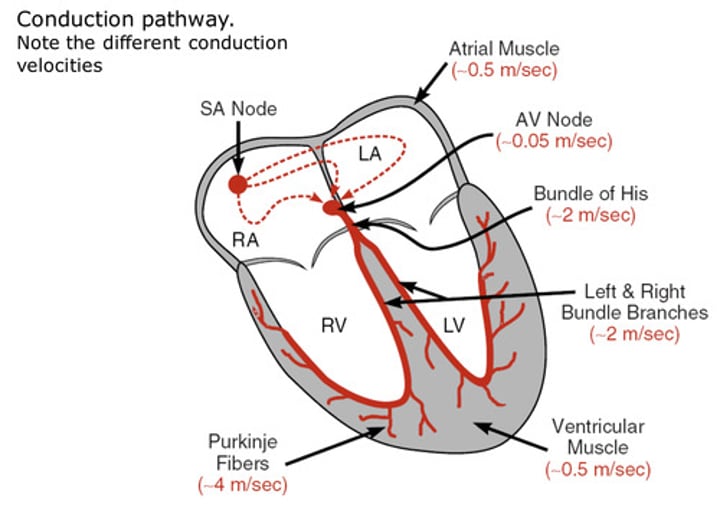
Describe the electrical conduction pathway of the Heart
- An action potential is spontaneously generated at the Sino-Atrial Node
- This action potential moves throuh the Atria to the Atriaventricular Node, causing Atrial systole as it moves, and slows down the electrical signal to allow Ventricle filling
- The action potential then moves down quickly the Bundle of His to the apex of the heart, and spreads out through the Ventricles via the Purkinje fibres
- Ventricular systole then occurs, from the bottom up to force blood out the Aorta and Pulmonary Artery
- Propagation through muscle is slow to allow time for contraction to move all the blood out of the chamber
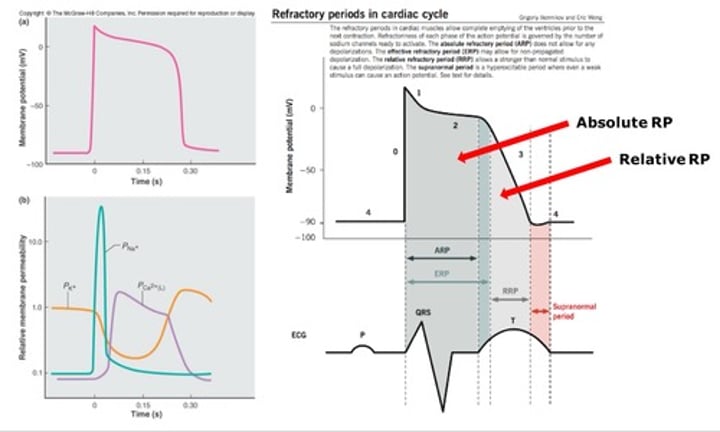
Describe the action potential of Cardiomyocytes
- The action potential of cardiomyocytes is much longer than neurones, with delayed repolarisation facilitated by an immediate fall in K+ permeability and rise in Ca2+ permeability, allowing time for contraction before cell is repolarised for further action potentials
- Generally, cells are more permeable to K+ and impermeable to Na+, allowing K+ in and Na+ out the cell at rest
- When a few LG Na+ channels open and depolarise the cell to threshold, this opens a lot of VG Na+ channels, allowing for faster depolarisation
- Na+ channels become inactivated shortly after opening, causing the refractory period, during which repolarisation occurs (helps unidirectional propagation)
- Absolute RP is inactivated receptors so no depolarisation is possible, while Relative RP is closed receptors so depolarisation possible with strong enough signal
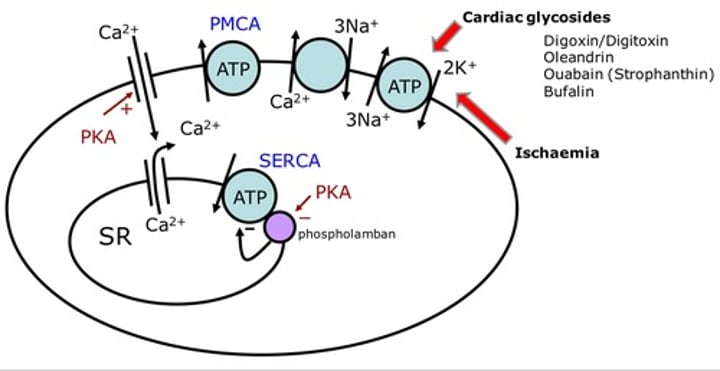
Describe the removal pathways for Calcium from Cardiomyocytes
- PMCA (plasma membrane Ca2+ ATPase) and SERCA (sarcoplasmic reticulum Ca2+ ATPase) are most effective in removing Ca2+, and both are active transporters, moving Ca2+ out of the cell and back into the Sarcoplasmic reticulum respectively
- SERCA is negatively regulated by Phospholamban, so it inhibits the reuptake of Ca2+, which is one mechanism for controlling contraction rate
- Protein Kinase A causes phosphorylation of Phospholamban, inhibiting its action, and opens membrane Ca2+ channels so allows increased force and rate of contractions
- NCX (Na+/Ca2+ exchanger) is less effective than PMCA and SERCA because NCX depends on concentration gradient of Na+, which is controlled by Na+/K+ ATPase pump, so inhibiting the pump inhibits action of NCX
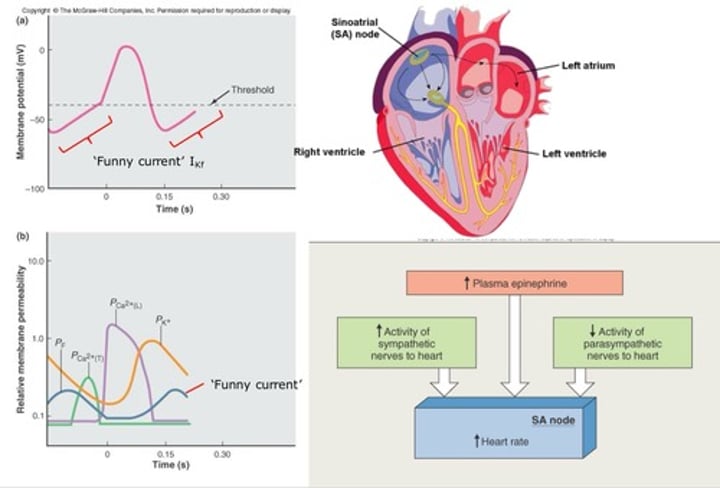
What is the role of the Sino-Atrial Node in Heart electrical activity?
- The Sino-Atrial Node (SAN) is the site of spontaneous action potentials that cause heart contractions, making it the pacemaker for the heart
- The SAN can be modulated by activity from the sympathetic and parasympathetic NS, causing increase or decrease in heart rate through noradrenaline and acetylcholine
- The rate of depolarisation of the SAN is called the Funny Current, where a faster Funny Current means faster action potential generation
What is an ECG?
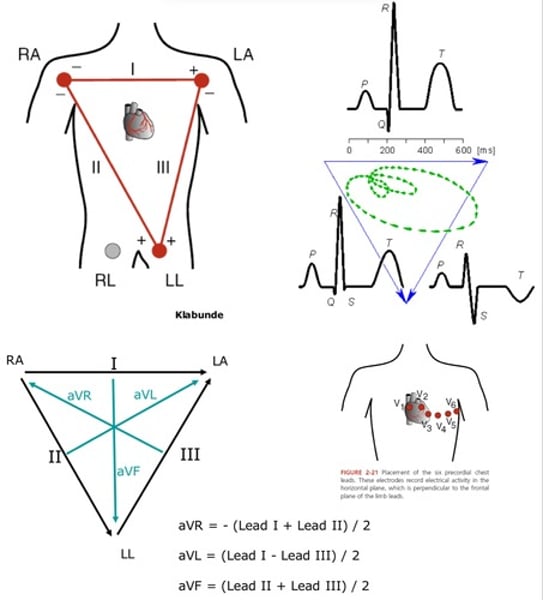
- An ECG (electrocardiogram) is a way of measuring the electrical activity of the heart, using Einthoven's triangle where 3 electrode leads are placed around the Right Arm, Left Arm and Left Leg
- The leads are polarised so current can move in certain directions, where lead I is RA to LA, lead II is RA to LL and lead III is LA to LL
- The positive and negative inflections show the direction of depolarisation in the heart relative to each lead
- Augmented leads and Precordial leads (placed around the chest for transverse perspective) are used to give more information for diagnosis
What information is given by an ECG?
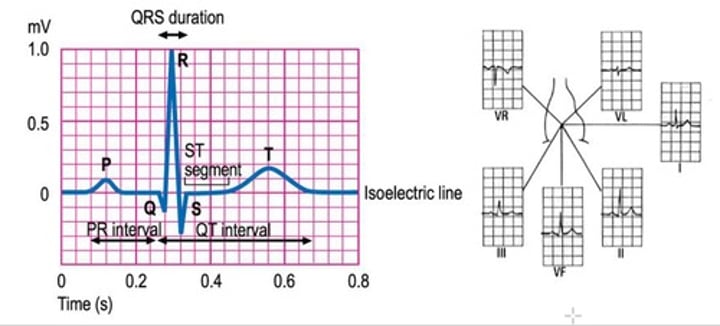
- Information from an ECG is referred to as the PQRST sequence
- P wave = atrial depolarisation (associated with atrial systole)
- QRS complex = ventricular depolarisation (associated with ventricular systole)
- T wave = ventricular repolarisation (associated with cardiac diastole)
- PR interval = time it takes signal to move from atria to ventricles through the AV node
- ST segment = flat isoelectric segment (changes represent myocardial injury)
- QT interval = time between ventricular depolarisation and repolarisation
What are changes from a Normal ECG signs for?
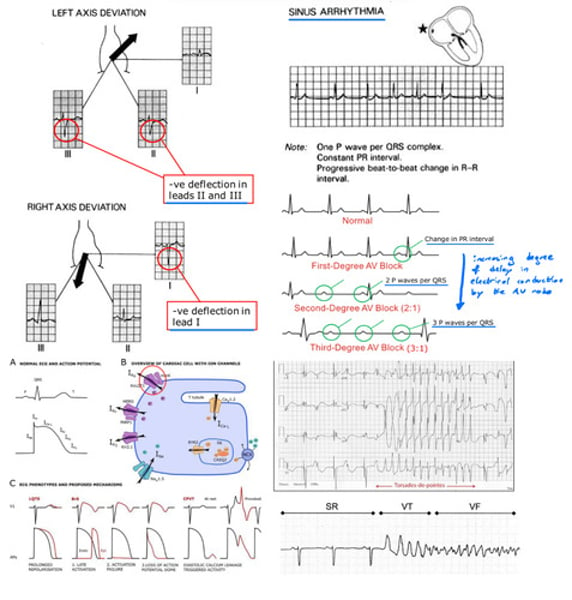
- Deviations from the axis (negative inflections in certain leads) can be a sign of hypertrophy of a part of the heart, physical displacement of the heart or conduction defects
- Sinus Arrhythmia can be seen with differing R-R intervals, showing signs of heart rhythm irregularities, usually due to interactions between cardiovascular and respiratory control centres in the brainstem
- AV node blocks can be seen by an increase in delay from P wave to QRS complex, where increases number of P waves is a sign of AV node block
- Ventricular Tachycardia (Torsades de pointes) seen by faster rate of PQRST sequences, leading into Ventricular Fibrillation (lethal if not treated quickly)
- Channel pathologies or Hyperkalaemia may be seen by arrhythmias, by changes in repolarisation times that lead to inference with generation and propagation of action potentials
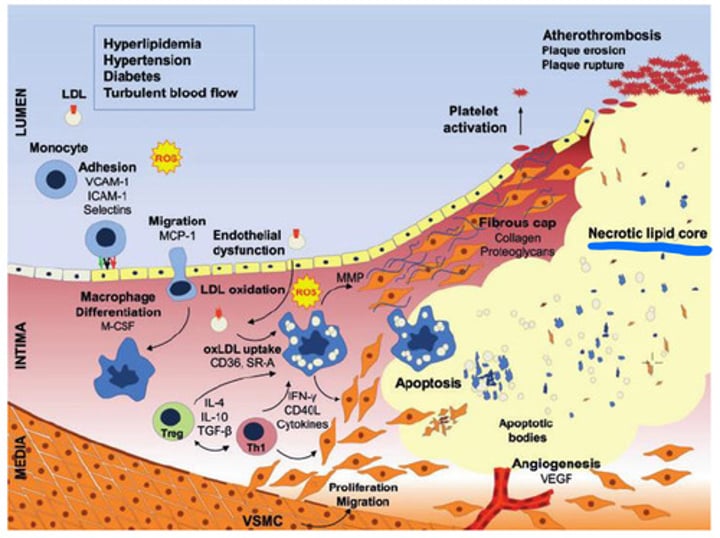
What is Atherosclerosis?
- Atherosclerosis occurs from build up of plaque in the walls of arteries (including coronary arteries), where plaque can contain cholesterol, fatty substances, calcium and other substances
- Plaque accumulation can lead to narrowing and hardening of arteries over time
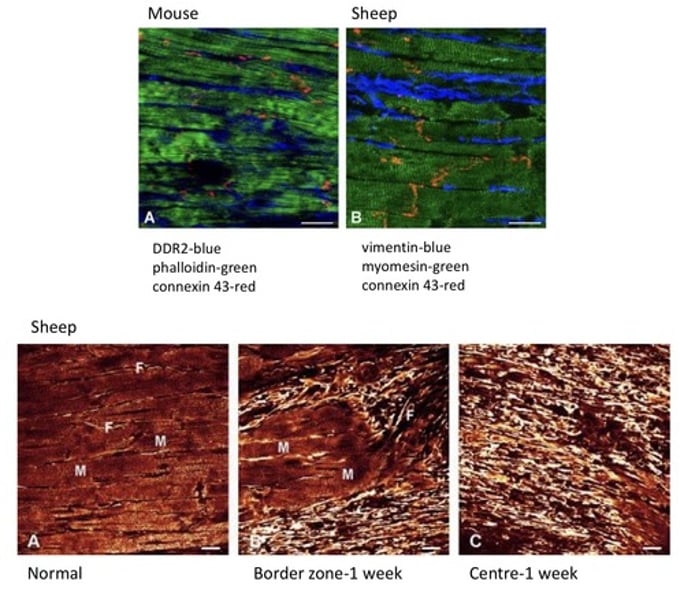
What is the interaction between Fibroblasts and Cardiomyocytes?
- Fibroblasts produce growth factors and keep myocytes healthy
- Apoptosis of cells can active fibroblasts to produce collagen and extracellular matrix for repair of the damaged region (eg. following myocardial infarction or other injuries)
- Reduced cardiac muscle mass and increased amount of collagen and extracellular matrix can lead to akinetic contraction
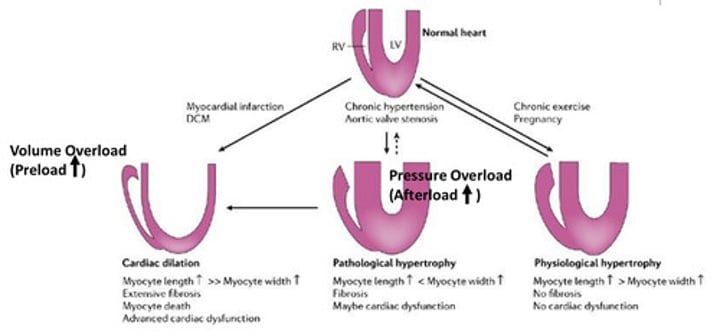
What is cardiac hypertrophy?
- Cardiac hypertrophy occurs when cardiac muscle enlarges and thickens, usually the left ventricle as it pumps at higher pressures into systemic circulation
- Cardiac hypertrophy can occur due to mitochondria (taking space), reduced ATP and less forceful contractions meaning more muscle mass is needed to produce higher pressures
- Causes of hypertrophic remodelling in Cardiac muscle can be a result of cardiac dilation (), pathological (maybe cardiac dysfunction - eg. aortic valve stenosis) or physiological (no cardiac dysfunction - eg. chronic exercise)
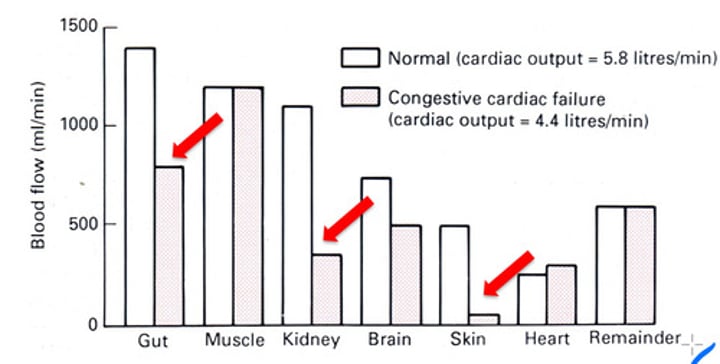
What is Heart Failure?
- Heart failure is the inability to pump out blood effectively to meet body's metabolic demands (inadequate cardiac output)
- HFpEF (preserved ejection fraction) is when ejection fraction is greater than 50% and a result of inability to relax and fill with blood during diastole
- HFrEF (reduced ejection fraction) is when ejection fraction is below 40% and a result of inability to contract and eject the blood during systole
- Symptoms depend on which side of the heart has failed and can include SOB, coughing, increased jugular vein pressure (neck), oedema of lower limbs and dilation of the ventricles
- Kidney failure may follow heart failure, due to kidney blood flow being one of the highest in the body, fluid overload, reduced renal perfusion pressure and activation of hormonal systems like RAAS (renin-angiotensin-aldosterone system)
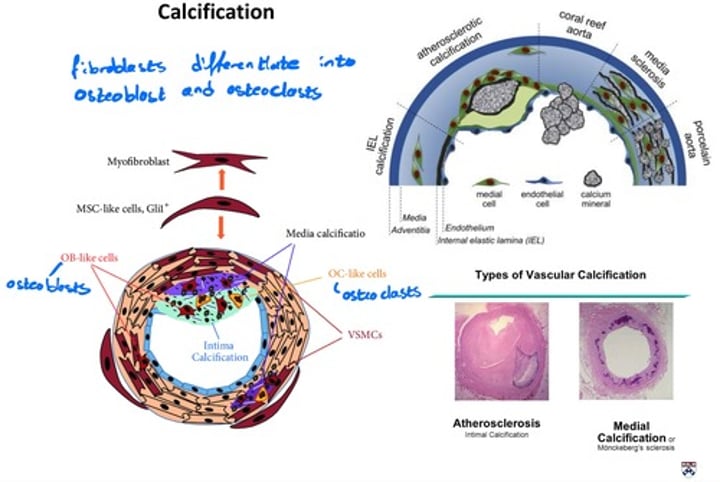
What is the calcification of blood vessels?
- Blood vessels can calcify and stiffen, so their ability to control pressure is reduced
- This is a normal process with age, where the ability to distend (elastic ability) is reduced from calcification
- This occurs by fibroblasts in the blood vessel differentiating into osteoblast-like cells and osteoclasts-like cells
- Calcification of blood vessels can be a result of atherosclerosis, due to high amount of calcium found in plaques