Exercise Physiology: Cellular Adaptation
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
Concept of Overload
Cellular adaptations only take place when the body is stressed beyond the norm
Concept of Specificity. What are some examples of factors that respond positively when they are specifically stressed
Cellular adaptations are similar to the type of stimulus induced on the body. Some of these factors include:
Muscle fiber type
Energy systems used
Contraction velocity
Contraction type (Concentric, eccentric, isometric)
Reversibility
Adaptations from exercise can be lost if the stimulus is no longer continued to the same degree.
Basic training princibles to improve Vo2 max
Use Large muscle group (greater demand for oxygen)
Dynamic exercise ( more reliant on aerobic energy systems)
20-60 mins of duration 3* a week minimum
Intensity = > 50% of vo2 max
Degree of vo2 max improvement
About 15-20% in untrained individuals
In individuals with low inital level of fitness, up to 50% is possible
High fitness individuals experience lower level of imporvement
Approximately how much does genetics effect inital Vo2 Max and adaptation to ET
In sedentary folk, about 50% of their vo2 max can be explained by their genetics
There are also high variations (47%, so about the same) to the degree of adaptation to exercise stimulus among individuals. Individuals who respond greatly to a given exercise stimulus are high responders while individuals who do not respond very much are considered low responders.
The degree of gene expression of important genes like PGC1-A for example, can determine both baseline fitness and the degree of adaptation.
Heart rate changes to Exercise. Mechanisms for change?
RHR: Decrease
Submax HR at any given intensity: Decrease
MHR: Stays the same (could decrease slightly)
Induced by an increased vagal tone
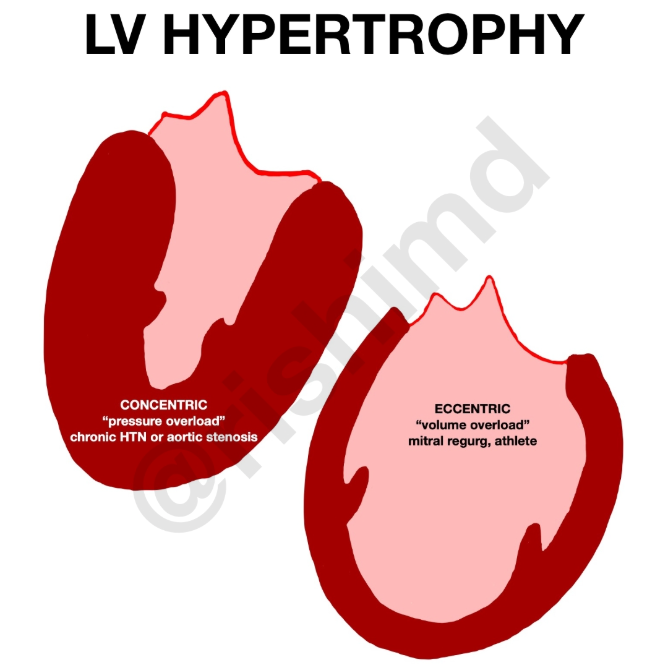
Adaptations to heart size; mechanisms for change
Left ventricle: Chamber increases so it can hold more volume due to VOLUME OVERLOAD during exercise
Myocardium: Hypertrophies
Why? Likely volume overload due to an increase in blood plasma. Also, a lower resting heart rate will also likely contribute. Remember, CO is the SAME regardless of how fit you are if your at rest. So if HR is lower at rest and CO must be the same, SV must be higher all the time as well as during sub max exercise, resulting in this adaptation.
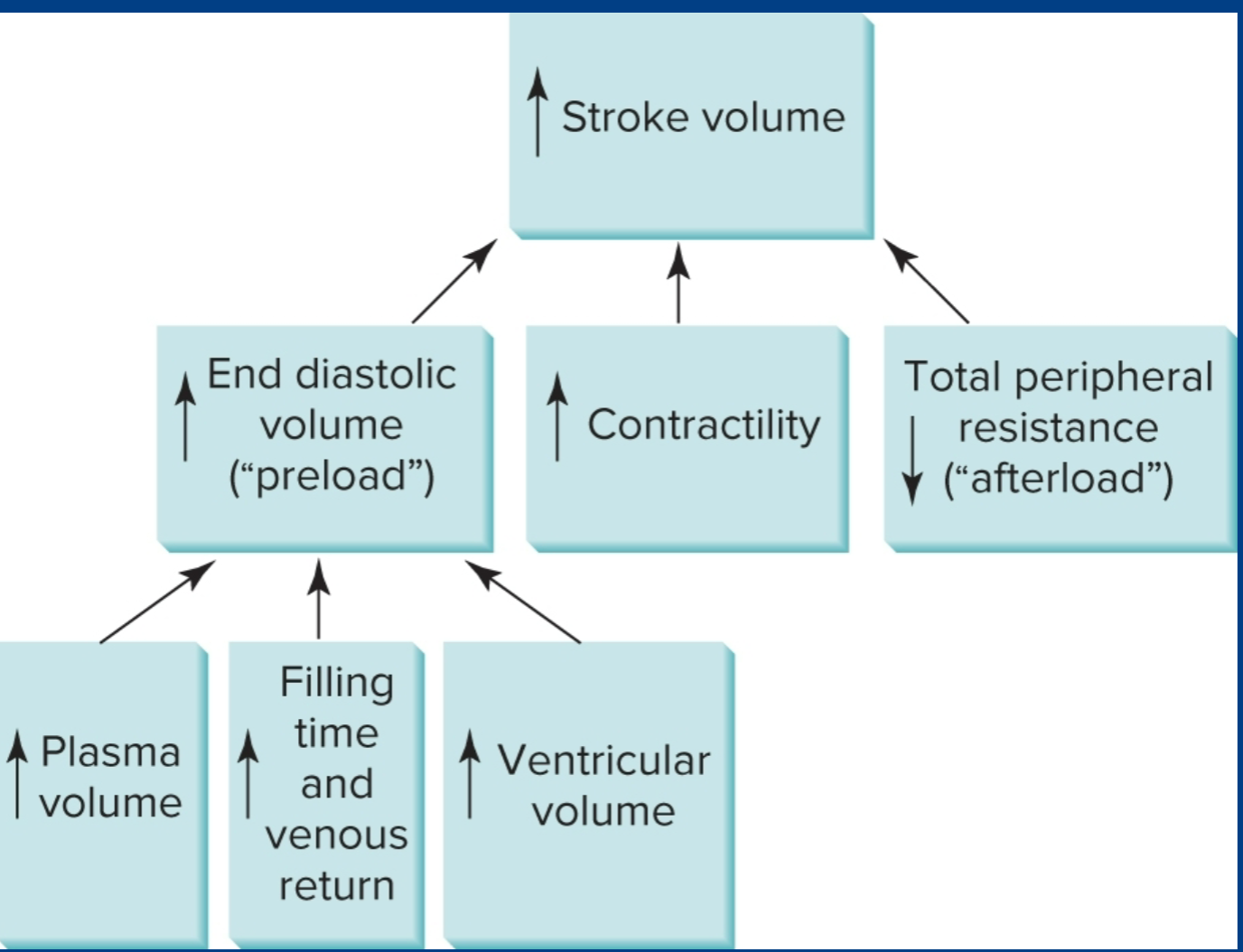
Stroke volume; changes and reason for changes
SV: Higher
The larger left ventricle holds more blood, resulting in a larger EDV and thus higher SV.
There is also an increase in preload (greater capacity for venous return, greater blood plasma,) which means frank sterling effect is exaggerated.
The afterload is also decreased as an adaptation due to less arterial resistance.
The chamber also has more time to fill because of the lower heart rate
Very helpful photo
;)
A-vo2 Difference; what happens to it and why?
It increases.
Blood flow is going to increase due to a decrease in SNS innervation. Remember, Greater SNS innervation means greater constriction of smooth muscle, including the veins.
There is also going to be more mitochondria, more oxidative enzymes, more capillaries, and more hemoglobin
So this means that the muscles are more efficient at using o2 and our circulatory system is better at sending oxygen to the muscles via the increased carrying capacity.
The greater o2 consumption capacity means o2 is consumed more rapidly, leading to a GREATER PO2 difference in the muscles and arteries. And because of this, diffusion has increased.
Increased HB concentration
Cardiac output; change and reason for change
Rest: stays the same
Submax: stays the same or decreases (id say mostly stays the same though)
Max: increases
CO = SV * HR
Explanation: Though heat rate is lower, CO remains the same because of an increase in efficent blood delivery (decrease in SNS innervation) and a greater A-vo2 difference. Hypothetically, CO could potentially DECREASE even as the muscles become more efficent at utilizing oxygen; creating a large difference in PO2.
Of course, CO improves at max intensities because of the increase in SV. for example;
Untrained: 190BPM * 20ml
Trained: 190 BPM * 30ml
Blood flow and Capillary Density; how does it change and why?
Blood flow; increases
Capillary Density: Increases
Mostly self explanitory: BF increases because of greater CO
Capillary density increases because there are more capillaries
Blood pressure; how does it change and why?
Blood pressure at rest: decrease
Blood pressure at submax: decrease
We have decreases because of a greater number of capillaries (the blood stays in contact with the walls of the vessels, reducing TPR) and a greater increase in the elasticity of the arteries
Pulmonary Diffusion: Changes and explanation
It increases
This is due to both more blood volume and greater capillary density
Minute venelation; changes and explanation (amount of breaths you take in a minute)
Rest: decrease
Submax: decrease
Max: Increase
Rest + Submax has an increase in TV, which is more effective than increasing RR (Respritory rate)
At max intensities both increase.
We have a higher RR in elites because we have a greater o2 demand.
Oxygen Consumption: same dealio
Rest: Stays same
Submax: Stay same:
Max: Increases (15-30% in 3 months and up to 50% in dose years)
We stay the same at rest and submax because the metabolic demand of exercise is the same. It increases at max because we have a new ceiling: or in other words we can generate more energy thus we need even more oxygen
Why do trained individuals have smaller o2 deficits than untrained?
They reach steady state o2 consumption faster
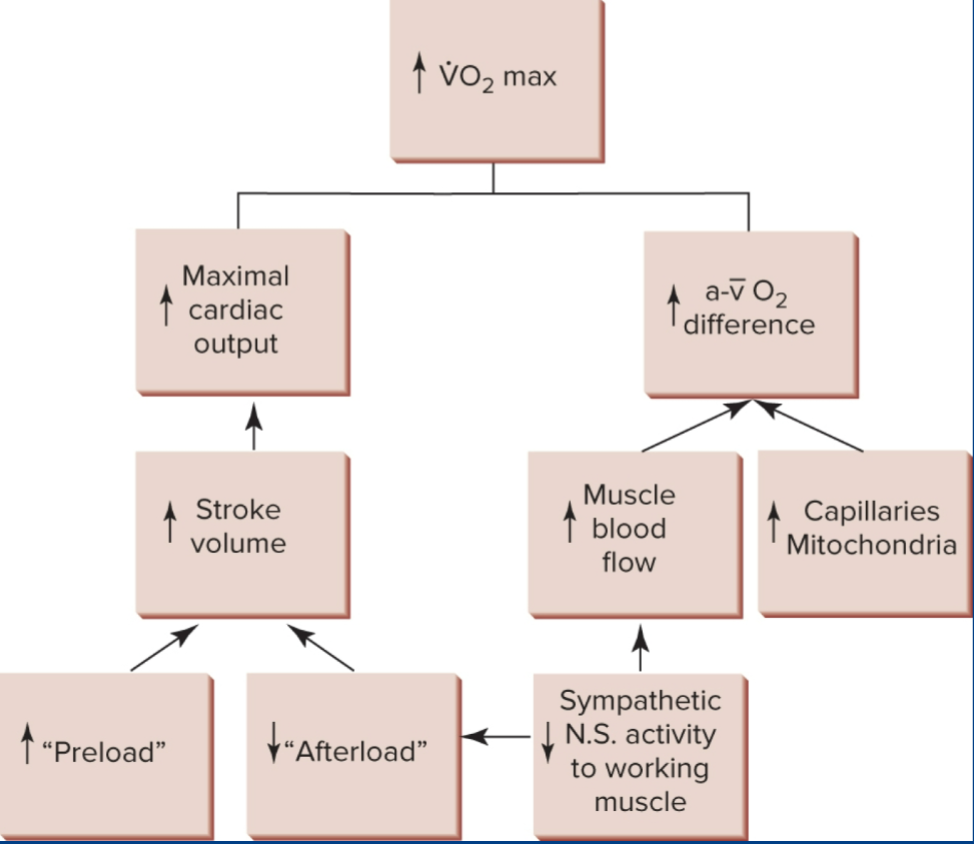
Main reasons for increased vo2
It is mostly the greater SV and CO
a-vo2, capillary density, blood volume, and VE are also contributers.
Very helpful photo
;)
Blood lactate; Same dealio
Rest: same
Submax: decrease
Max: Increase
Resting values are what they are. at submax we are more efficent at clearing lactate and thus have lower lactate levels. We can “tolerate” higher levels of lactate through training (remember HSPs?) and thus max goes up.
ATP-PC stores in trained individuals; what changes?
We can increase our ATPPC stores faster! fun fact; this is because ATP-PC stores are regenerated in the mitochondria!
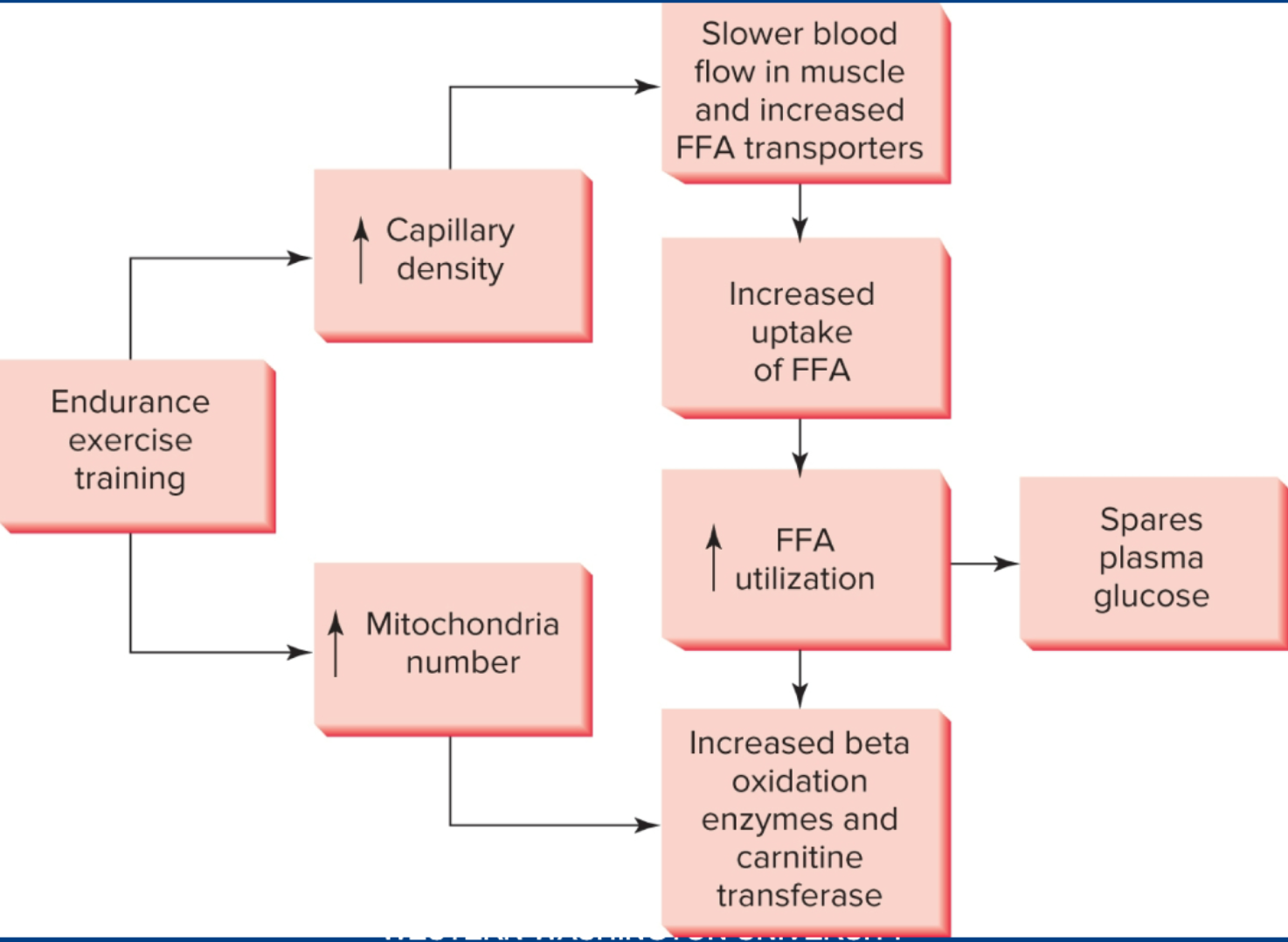
What changes about fuel utilization in general in aerobically trained athletes?
With a shift in muscle fiber type we have a change in fuel utilization from anaerobic systems (less ATP-PC). If a muscle fiber, for instance, develops mitochondria, it will rely more on aerobic pathways and less on anaerobic
What can highly trained individuals do with lactate more effectively?
oxidize it and turn more of it back into pyruvate.
What can more highly trained individuals do when it comes to free radicals?
balance them with higher antioxidant levels
Helpful picture
Primary signals for second messagers. What do they signal
AMP/ATP ratio (High ATP use) (ET). Signals AMPK
Cytosolic Calcium (muscle contraction) (ET) Signas adaptation to calcium handling
Muscle stretch (RT) (microtears need repair)
Free Radicals (ET) Signals adaptations fir improved antioxidant levels for balance
AMP/ATP ratios signals….
AMP Kinase. Activate PGC1-A through transcription factors. Also signals for glucose uptake.
Cytosolic Calcium signals…
Calmodulin Dependent Kinase. Signaling molecule that also activates PGC1-A
Free radicals signals…
NFkB. Protien complex that synthesizes antioxidant enzymes.
Muscle stretch signals…
mTOR. a extremely important kinase for protien synthesis and hypertrophy.
PGC1-A
Gene that is activated by CAMK, p38, AMPK among others. Major player in angiogenisis, Mitochondrial biogenesis, and synthesis of antioxidant enzymes.
Detraining rate of Vo2 max
8% within 12 days. 20% after 84 days.
Stroke volume response to detraining
decrease because of less plasma volume
Avo2 difference response to detraining
Decrease because of less blood flow and less mitochondria. also less oxidative enzymes. This is going to flip type 2as to 2x and even some 1s to 2as!
What goes down first, SV or A-V02?
SV, because blood plasma goes away quicker. mitochondria tend to hang for longer.
Rate of mitochondrial detraining
50% of gain within one week. Majority is lost within two.
Rate of mitochondrial retraining.
Muscle mitochjondria are pretty quick! 3-4 weeks.
Intensity and duration of zone of SIT. Energy systems?
>100% vO2 Max, 10-30 seconds. ATP-PC and glycolysis
Intensity and duration of HIIT
80-100% Vo2 max, 6s-240s. Largely ATP-PC and glycolysis with the remainder being aerobic
Adaptations from SIIT
Hypertrophy, Enhanced buffering, greater Anerobic energy system capacity. All these result in greater anaerobic performance
Muscular strength
maximal force generated during a 1RM
Muscular Power
amount of force one can generate over a period of time.
Muscular Endurance
Abillity to repeatedly contract against a load
Protocole for muscular Strength gains
6-10 reps to fatigue
protocole for muscular endurance gains
35-40 reps to failure
How do fiber types and motor neurons change with age
Muscle mass decline (sarcopenia)
Atrophy of type II fibers
Reduced number of type I and II fibers ( so this is the same as sarcopenia basically)
Motor neuron death
Reason behind neuromuscular decline in old muthafuckas?
resistance to signaling from androgens and GH.
Neural adaptations to RT.
Increased specific muscle fiber tension; increased muscle mass.
Explanation for Neural adaptations to RT. Time period?
First 2-8 weeks of training increases neural drive by virtue of increase motor unit activation, more synchrony among MUs, increased firing rate, improved neural transmission across NMJ (ACH and ACH receptors…)
We know this because there has been demonstrated strength gains in the first 2 weeks of training with no increase in fiber size.
Resistance training aids in strength in untrained limb
Muscle mass changes to RT? Factors? Explanation?
increases.
hypertrophy (size of fibers per CSA)
Hyperplasia (Questionable)
Drived by an increase in mRNA as a response to resistance training (mRNA directs cell to make a protien)
stimulation of mTOR is caused by RT, which increases degree and rate of protien synthesis.
mTOR can also be activated by BCAAs if accompsanied by RT.
mTOR is also linked to GF and IGF-1; both of which are hormones that signal growth.
Inflammatory response of weight training leads to a need for repair and renewal. Inflammatory response triggers satellite cells that increase myonuclei #s on the muscle fiber. With greater hypertrophy, more myonuclei (or a greater myonuclei domain) is neccesary for proper function of the cell.
helpful picta
:)
Anti-Inflammatory drugs effect on hoomans? animals? (in terms of hypertrophy
animals? yes apparently
Hoomans? no apparently
cool bro
Genetics effect on muscle mass and hypertrophy.
80% of difference in muscle mass is because of genetics
47 different genes relate to protien synthesis and a great deal of them go through mTOR and/or induced by RT
Genetic potential; again high versus low responders :)
The FUCK is muscle memory. What factor is responsible?
abillity to rapidly regain muscle mass after a damn break.
WHY??
Because MYOnuclei dont be leaving!!! and myonuclei is a manager of protien synthesis, so more myonuclei = greater protien synthesis = faster hypertrophy.
how does concurrent training fuck with everything and everyone
Possible interference of MU recruitment? so less development of type 1 MUs compared to just ET, and less type 2 MUs compared to just RT.
AMPK signaling blocks mTOR?? (resistance train BEFORE your cardio if you want hypertrophy)
Overtraining? if you are a bitch.