N - Motor Systems 2
1/24
Earn XP
Description and Tags
The Basal Ganglia + Cerebellum
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
25 Terms
Cerebellum + Basal Ganglia
Cerebellum:
closely involved with brainstem mechanisms
Basal Ganglia:
integration of sensory + motor info
neither project directly beyond the brain
The Cerebellum
sensorimotor coordination
control of muscle tone
motor learning
Cerebellum: 3 function + anatomical components
Spino-cerebellum (medial regions)
sensory input from the spinal cord
output to the reticular formation + red nucleus
cerebellum → motor cortex → spinal cord control over axial musculature + posture
Vestibular-cerebellum (caudal region)
input from + output to vestibular nucleus (ventromedial pathway)
control over posture/balance
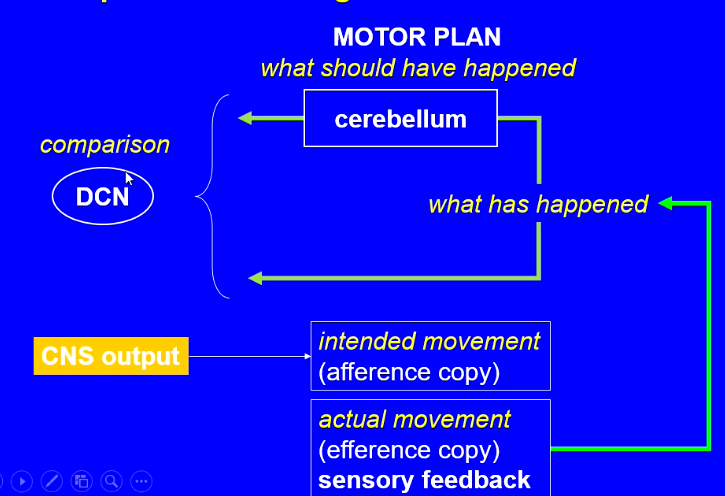
cerebrocerebellum (aka pontocerebellum)
an intracerebral loop
cortex → cerebellum → cortex (M1)
instructs the primary motor cortex (M1)
movement direction, timing, force
compares intended movements with actual movements sends compensatory instructions to M1
Layers of cerebellar cortex
molecular layer (top)
purkinje cell layer
granule cells layer
white matter (bottom)
Deep cerebellar nuclei (DCN)
DCN cells can compare input from mossy + climbing afferent input
before (via axons to P-cell) and after cerebellar processing (via inhibitory P cell output)
Cerebellum: comparing (image)
DCN sends an error signal to brain stem + thalamus if movement is not right
Intention tremor + dysmetria
damage to cerebellum
can’t draw square - go off track
go off track when bringing finger to nose
Function after damage to cerebellum
Symptom | Description | Functional Component |
|---|---|---|
Ataxia | Unsteady, staggering gait | Spino-cerebellum, Cerebro-(ponto-)cerebellum, Vestibulo-cerebellum |
Dysmetria | Inaccurate termination of movement | Spino-cerebellum, Cerebro-(ponto-)cerebellum |
Hypotonia | Reduced muscle tone | Spino-cerebellum |
Slow saccades / Nystagmus | Impaired eye movement | Vestibulo-cerebellum |
Dysarthria | Inarticulate speech due to poor oropharyngeal muscular control | Cerebro-(ponto-)cerebellum |
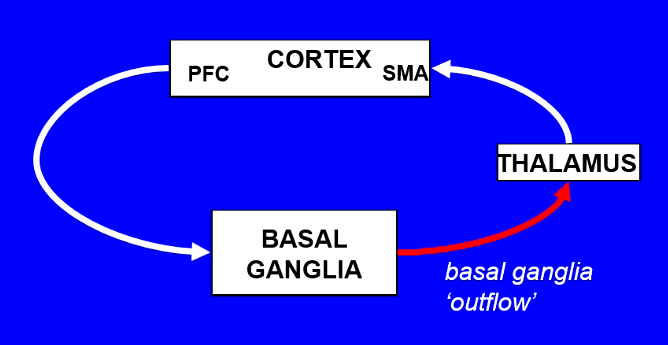
The Basal Ganglia: Cortico-basal ganglia-cortical loop
integrates motor + sensory info from the cortex
relays back to cortex via thalamus
motor circuit output to premotor/SMA cortex
selection and initiation of voluntary movement
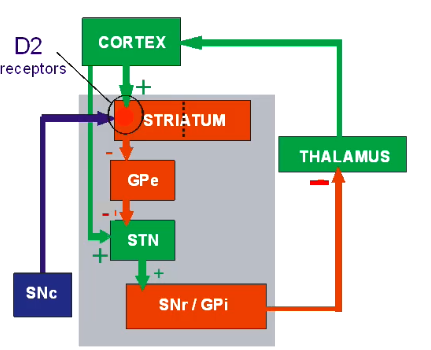
The Motor Loop (image)
The basal ganglia structures include:
striatum (STR):
the caudate nucleus
putamen
nucleus accumbens
subthalamic nucleus (STN)
globus pallidus (GP):
external (GPe)
internal (GPi)
substantia nigra:
reticulata (SNr)
pars compacta (SNc)
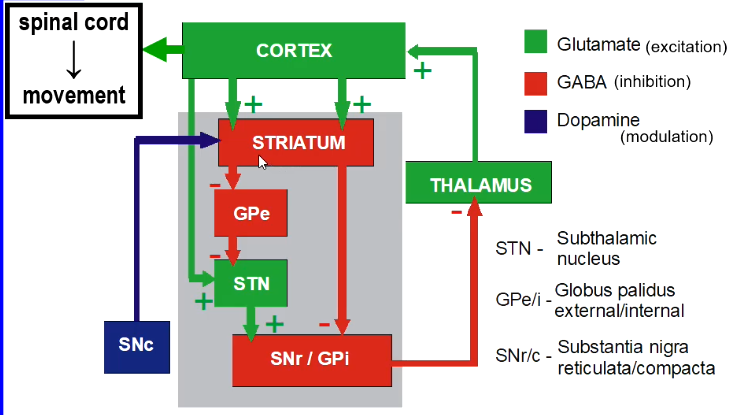
Direct + indirect pathways
from striatum - cortical input is relayed to 2 major basal ganglia areas = SNr + GPi
‘direct’ pathways - striato-nigral + stiato-pallidal (GPi)
‘indirect’ pathways projections via GPe + STN
opposing effects on thalamocortical output
balance between direct + indirect pathways
dopamine (from SNc) - plays key modulatory role
The basal ganglia - basic circuit
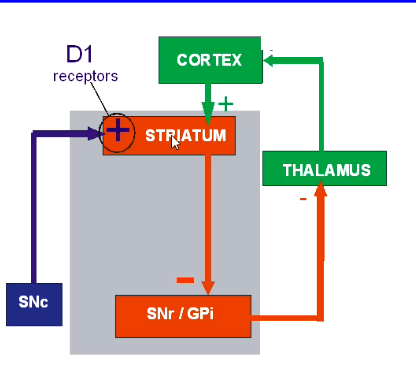
Direct pathway + dopamine
the direct pathway serves to promote movement
dopamine acts on excitatory D1 receptors on striato-GPi neurons
Indirect pathway + dopamine
the indirect pathway serves to suppress movement
dopamine acts on inhibitory D2 receptors on striato-GPe neurons
decreased STN activity
decreased BG output
= facilitates movement (bc basal ganglia movement usually inhibits cortical action)
The BG and Motor Dysfunction
imbalance between the direct + indirect pathways = motor dysfunction
hypokinetic disorders e.g. Parkinson’s disease
hyperkinetic disorders e.g. Huntington’s disease, Hemiballism, Tardive Dyskinesia
Parkinson’s Disease
tremor
bradykinesia (slowness of movement)
rigidity (resistance to passive movement)
primary pathology:
progressive degenerative loss of nigro-striatal dopaminergic pathway
Neurobiology of PD
dopamine loss in BG
leads to excessive inhibition of thalamo-cortical pathway
accompanied / driven by increase activity in STN (subthalamic nucleus)
Treatments for PD (1)
many drugs to boost dopamine in brain = replacement therapy:
L-DOPA
dopamine receptor agonists
drugs that reduce dopamine breakdown (MAO-B inhibitors)
deep brain stimulation
Treatments for PD (2)
Dopamine replacement therapy:
reduces rigidity + hypokinesia
L-DOPA:
metabolised to produce dopamine by DOP-decarboxylase
but L-DOPA will also elevate NAdr synthesis in sympathetic NS
non-brain penetrating carbidopa or benserazide co-administered to inhibit peripheral DOPA decarboxylase
Surgical treatment of Parkinson’s Disease
surgical lesion / inactivation of STN
Huntington’s disease
excessive ‘choreiform’ movement
uncontrollable, rapid motor patterns disrupts normal motor activity
later stages - psychiatric disturbance, dementia
neurobiology:
loss of striatal output neurons in indirect pathway - suppression of STN
= suppression of STN
= dominance of direct pathway
decreased GB output
= overactive thalamocortical pathway
Huntington’s disease: Drug Treatments
symptomatic relief only
Tetrabenazine - VMAT inhibitor, decreased DA storage + release
Chlorpromazine - DA receptor antagonist
Baclofen - GABA-B receptor agonist
Other hyperkinetic disorders: Hemiballismus
Cause:
damage to subthalamic nucleus (usually unilateral stroke)
Effect:
violent flailing movements of limbs (contralateral to damage)
Other hyperkinetic disorders: Tardive Dyskinesia
Cause:
long-term exposure to antipsychotic dopamine receptor antagonist drugs
Effect:
uncontrolled movement, especially of facial + trunk muscles