MUSCULOSKELETAL EXAMINATON HIP AND PELVIS (P1: PELVIS)
1/128
Earn XP
Description and Tags
gg
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
The sacroiliac joints are part synovial (i.e., diarthrosis) joint and part syndesmosis; thus they are sometimes called what type of joints?
Amphiarthrosis (slightly movable) joints
A type of fibrous joint in which the intervening fibrous connective tissue forms an interosseous membrane or ligament.
Syndesmosis
What is the shape of the synovial portion of the sacroiliac joint ?
C-Shape
the convex iliac surface of the C faces what direction?
Anteroinferiorly
True or False:
that the greater or more acute the angle of the C, the less stable the joint and the greater the likelihood of a lesion to the joint.
False:
that the greater or more acute the angle of the C, the more stable the joint and the less the likelihood of a lesion to the joint.
The iliac surface of the joint is concave/convex while the sacral surface is concave/convex?
Iliac - Convex
Sacral - Concave
True or False:
The sacroiliac joints act as shock absorbers to shear forces and provide a torsional load attenuation mechanism for forces between the lower legs and trunk.
True
The normal overall motion at the sacroiliac joints is about how many degrees
7°
Sacroiliac Joint
Resting position:
Capsular pattern:
Close pack:
Loose pack:
Sacroiliac Joint
Resting position: Neutral
Capsular pattern: Pain when joints are stressed
Close pack: Nutation
Loose pack: Counternutation
True or False:
The articular surfaces of the sacrum are smooth for children and irregular for adults.
In older persons, parts of the joint surfaces may be obliterated by adhesions.
True
Due to the irregular shape, adult sacroiliac joints are stronger and have a more restricted movement.
The articular surface of the ilium is covered with ____________
the articular surface of the sacrum is covered with ___________
Fibrocartilage
Hyaline Cartilage (3x thicker than ilium)
How does age affect the mobility of the sacroiliac joints compared to the spinal joints, and what condition may result from this change?
Older = Stiffer / Less mobile
Ankylosis
What ligaments that limit anterior pelvic rotation or sacral counternutation?
long posterior sacroiliac ligaments
The ligament that limits all pelvic and sacral movement:
Short posterior sacroiliac ligament
The ligaments limit nutation and posterior innominate rotation; they also provide vertical stability:
Sacrotuberous and Sacrospinous ligaments
What ligament stabilizes L5 on the ilium?
iliolumbar ligament
What ligament is the major connection between the sacrum and the ilium and is one of the strongest ligaments in the body?
interosseous sacroiliac ligament
These ligaments and the complex arrangement of dense connective tissue acting like a ______________ play a major role in stabilizing the sacroiliac joints.
Ligamentous Stocking
True or False:
The sacroiliac joints and symphysis pubis have no muscles that control their movements directly, although muscles do provide pelvic stability, so they are influenced by the action of the muscles moving the lumbar spine and hip because many of these muscles attach to the sacrum and pelvis.
True
Two mechanisms that stabilize the sacroiliac joint:
Form Closure and Force Closure
Closure due to specific anatomic features of the joint themselves which prevent shear (CPP of the joint).
Form Closure
intrinsic factors such as joint shape, coefficient of friction of the joint surfaces, and the integrity of the ligaments contribute to form closure.
Closure due to the compression generated by the muscles and, through them, the tensing of the ligaments when they act to accommodate specific load situations.
Force Closure
Responsible for the stability of the joint in Loose packed position
The muscles that support the pelvic girdle as well as the lumbar spine and hips can be divided into groups.
The outer group consists of _____groupings, which act primarily in crossing or oblique patterns of force couples to stabilize the pelvis.
Four
Deep posterior longitudinal system:
erector spinae
thoracolumbar fascia
hamstring muscles
sacrotuberous ligament
Superficial posterior oblique system:
latissimus dorsi
gluteus maximus
intervening thoracolumbar fascia
Anterior oblique system:
internal and external obliques
contralateral adductors
abdominal fascia in between
Lateral system
gluteus medius and minimus
contralateral adductors
Innermost muscle group:
plays a role in stabilizing the pelvis and indirectly the lumbar spine
multifidus
transverse abdominis
diaphragm
pelvic floor muscles
anterior-posterior superficial group:
controls the anteroposterior rotation of the pelvis on the fixed femur
hamstrings
gluteus maximus
erector spinae
rectus abdominis
internal and external obliques
psoas,
rectus femoris
sartorius
iliofemoral and sacrotuberous ligaments
A fibrocartilaginous joint held together by the pubic ligament
Symphysis Pubis
There is a disc of fibrocartilage between the two joint surfaces
interpubic disc
True or False:
The symphysis pubis does not allow limited movement
False:
This joint does allow limited movement.
This joint is usually a fused line (symphysis) united by a fibrocartilaginous disc. It is found between the apex of the sacrum and the base of the coccyx.
Sacrococcygeal Joint
True or False:
Occasionally the sacrococcygeal joint is freely movable and synovial. With advanced age, the joint may fuse and be obliterated.
True
Common Causes of injury to the Sacroiliac Joint:
sudden jar caused by inadvertently stepping off a curb
overzealous kick
a fall on the buttocks
lift and twist maneuver
Combined axial loading and rotation
Movements that increase the chance of sacroiliac joint sprains:
Recent Falls
Recent twists
Recent Strains
True or False:
Lesion in the sacroiliac joint causes deep, diffuse, dull, undefined pain that is difficult to localize. It tends to be bilateral and can be referred to the posterior thigh, buttock and iliac fossa of the same side.
False:
Lesion in the sacroiliac joint causes deep, diffuse, dull, undefined pain that is difficult to localize. It tends to be unilateral and can be referred to the posterior thigh, buttock and iliac fossa of the same side.
True or false:
Sacroiliac joint pain can spread to the abdominal area and sometimes to the groin, since groin pain is less commonly associated with hip problems.
False:
Sacroiliac joint pain can spread to the abdominal area and sometimes to the groin, although groin pain is more commonly associated with hip problems.
SI joint pain has been described as _______________ pain.
Sclerotomal
True or False:
SI joint pain never extends below the knee
False:
Sacroiliac pain does not commonly extend below the knee, although it can.
Both pain and numbness can originate from the sacroiliac joint and its ligaments, which ligament is primarily the source for this?
Posterior sacroiliac ligaments
Do symptoms from a SI joint problem follow a dermatomal distribution?
No
True or false:
Most patients with sacroiliac joint pathology indicate pain around the ASIS or inguinal region.
False:
Most patients with sacroiliac joint pathology indicate pain around the PSIS or buttock.
If the patient points slightly inferior and medial to the PSIS as the source of pain what sign does this indicate?
Point sign (Fortin finger test).
Pain arising from the posterior sacroiliac ligament is mainly on the which areas of the thigh?
lateral, posterolateral, and posteromedial thigh.
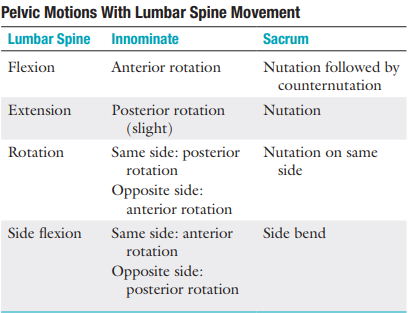
Pelvic motions with lumbar spine movement
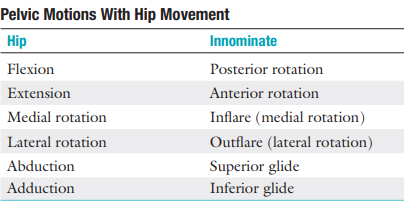
Pelvic motions with hip movement
True or False:
Pain that is caused by sacroiliac joint problems is usually felt when turning in bed, getting out of bed, or stepping up with the affected leg
True
True or False:
Often, SI joint pain is constant and relieved by position.
False:
Often, the pain is constant and unrelated to position.
Symphysis pubis pain tends to be localized and increases with any movement involving which muscles?
adductor or rectus abdominis muscles.
What particular movements bother the patient during SI joint involvement?
Transitional-type movements:
(e.g., sit to stand, single-leg squat)
Risk Factors of SI joint involvement:
obesity
leg length discrepancy
gait abnormalities
low-grade/persistent trauma
vigorous prolonged exercise
scoliosis
pregnancy
surgery
In the presence of sacroiliac joint pathology, endurance will increase or decrease?
In the presence of sacroiliac joint pathology, endurance will decrease
True or False
Apophyseal injuries and avulsion fractures of the pelvis can occur in young athletes.
True
Ankylosing spondylitis is found primarily in men between the ages of?
15 and 35 years.
Hypomobility is likely to be seen in:
men =
women =
Hypomobility is likely to be seen in:
men = 40-50 y/o
women = >50 y/o
True or False:
Neurological deficit in the limbs can be present if the sacroiliac joint is affected.
True
True or False:
It has been reported that sacroiliac joint dysfunction can lead to problems in parturition.
False:
It has been reported that sacroiliac joint dysfunction can lead to problems in micturition (urinary problems).
In females, sprain of the sacroiliac ligaments can be the result of increased laxity of the ligaments caused by hormonal changes.
It may take how many months longer for the ligaments to return to their normal state after a pregnancy?
3 to 4 months
Each of these conditions can involve the sacroiliac joints:
rheumatoid arthritis
Reiter syndrome
ankylosing spondylitis
This is the forward motion of the base of the sacrum into the pelvis; it could also be described as the backward rotation of the ilium on the sacrum.
Nutation (sacral locking)
The most stable position of the sacroiliac joint
Nutated
What type of closure is seen if the SI joint is fully nutated?
Form Closure
True or False
When moving from supine lying to standing, the sacrum normally moves unilaterally, just as it does in early movement of trunk flexion.
False:
When moving from supine lying to standing, the sacrum normally moves bilaterally, just as it does in early movement of trunk flexion.
Unilaterally, the sacrum normally moves with hip flexion of the lower limb
Pathologically, if nutation occurs only on one side (when it should occur bilaterally), the examiner will find that the anterior superior iliac spine (ASIS) is higher and the PSIS is lower on that side.
Follow-up questions next cards
Nutation is limited by which ligaments?
Which is more stable, nutation or counternutation?
In pathological nutation which is higher and lower? (ASIS/PSIS)
anterior sacroiliac ligaments, sacrospinous ligament, and sacrotuberous ligament
Nutation
ASIS is higher on one side and the PSIS is lower
True or False:
Nutation occurs when a person assumes a “pelvic tilt” position. During nutation, the sacrum will slide down its long part and then anteriorly along its short part.
False:
Nutation occurs when a person assumes a “pelvic tilt” position. During nutation, the sacrum will slide down its short part and then posteriorly along its long part.
This is the opposite movement to nutation. It indicates an anterior rotation of the ilium on the sacrum or backward motion of the base of the sacrum out of the pelvis.
Counternutation (sacral unlocking), or contranutation
Pathologically, if counternutation occurs only on one side as it does during extension of the extremity on that side, the lower limb on that side will probably be ______________
Medially rotated
Pathological or abnormal counternutation on one side occurs when the ASIS is ______ and the PSIS is _______ on one side.
Pathological or abnormal counternutation on one side occurs when the ASIS is lower and the PSIS is higher on one side.
Counternutation is limited by which ligaments
Posterior Sacroiliac Ligaments
Counternutation occurs when a person assumes a _______ or ________ position.
person assumes a “lordotic” or “anterior pelvic tilt” position.
True or False:
During counternutation, the sacrum will slide anteriorly along its long arm and then superiorly up its short arm
True
contraction of this muscle causes nutation of the sacrum
Multifidus
Therefore it supports the long posterior sacroiliac ligament in resisting counternutation
Anterior and posterior pelvic tilt has an effect on lumbar lordosis with an average change of how many degrees being possible
20° (9° posteriorly and 11° anteriorly)
_______ is the angle between a line joining the ASIS and PSIS and a horizontal line
Average value for this is?
Pelvic Tilt
11° ± 4°
True or False:
Ideal pelvic alignment would see the ASIS on the same vertical plane as the sacroiliac joint.
False:
Ideal pelvic alignment would see the ASIS on the same vertical plane as the symphysis pubis.
Three questions should be considered when one is looking for a neutral pelvis and whether the pelvis can be stabilized:
(read)
Can the patient get into the neutral pelvis position? If not, what is restricting the movement or what is weak so that the movement does not occur?
Can the patient hold (i.e., stabilize) the neutral pelvis statically while moving distal joints dynamically? If not, what muscles need to be strengthened?
Can the patient hold (i.e., stabilize) the neutral pelvis when moving it dynamically? If not, which muscles are weak and/or not functioning correctly (i.e., functioning isometrically, concentrically, eccentrically)?
If the sacroiliac joints are not free to move, the stride length is (increased/decreased?) and a ________ limp may be present.
If the sacroiliac joints are not free to move, the stride length is decreased and a vertical limp may be present.
A painful sacroiliac joint may also cause reflex inhibition of the (muscle?) leading to a (gait deviation?)
A painful sacroiliac joint may also cause reflex inhibition of the gluteus medius, leading to a Trendelenburg gait or lurch.
On which side does the ASIS often tends to be higher and slightly forward?
Affected Side
If the ASIS and PSIS on one side are higher than the ASIS and PSIS on the other, this indicates _________ of the ilium on the sacrum on the high side. a short leg on the ______ side, or muscle spasm caused by lumbar pathology.
an Upslip
Opposite side
If the ASIS is higher on one side and the PSIS is lower at the same time, what does this indicate?
anterior torsion of the sacrum (pathological nutation) on that side
This torsion may result in a spinal scoliosis, an altered functional leg length, or both.
This dysfunction is seen most frequently following a posterior horizontal thrust of the femur (dashboard injury), golf or baseball swing, or any forced anterior diagonal pattern.
Anterior rotational dysfunction
The sacrum is (higher/lower?) on the side of the pelvis that has rotated backward.
The sacrum is lower on the side of the pelvis that has rotated backward.
The most common rotation of the innominate bones is?
left posterior torsion or rotation (pathological counternutation)
The posterior rotational dysfunctions are usually the result of:
falling on an ischial tuberosity
lifting when the body is forward flexed with the knees straight
repeated standing on one leg
vertical thrusting onto an extended leg
sustaining hyperflexion and abduction of the hips
True or False:
If the patient stands favouring one leg, or have a lateral pelvic tilt these findings may indicate pathology in the sacroiliac joints, the leg, the spine, or a short leg
True
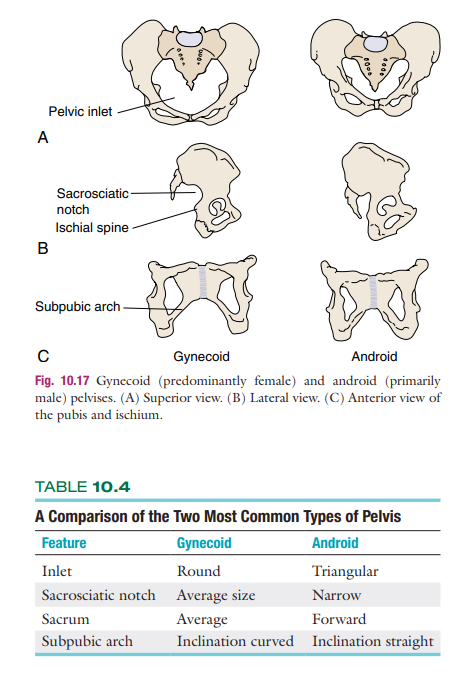
Types of Pelvis:
The _______ side is often flatter if there is loss of tone in the gluteus maximus muscle
The painful side is often flatter if there is loss of tone in the gluteus maximus muscle
If one _________ is higher, it may indicate an upslip of the ilium on the sacrum on that side
If one tuberosity is higher, it may indicate an upslip of the ilium on the sacrum on that side
Forward sacral torsion = increased or decreased lordosis?
Backward sacral torsion = increased or decreased lordosis?
Forward sacral torsion = decreased lordosis
Backward sacral torsion = increased lordosis
Forward sacral torsion = posterior pelvic tilt = decrease lordosis
Backward sacral torsion = anterior pelvic tilt = increase lordosis
If sacral sulci equal is deeper, it may indicate a _________.
Sacral torsion
Often, the affected limb is __________.
With spasm of the __________ muscle, the limb is _________rotated more on the affected side.
Often, the affected limb is medially rotated.
With spasm of the piriformis muscle, the limb is laterally rotated more on the affected side.
True or False:
the sacroiliac joints have muscles that directly control their movement.
False:
the sacroiliac joints do not have muscles that directly control their movement.
Active Movements That Stress the Sacroiliac Joints:
Forward flexion of the spine =
Extension of the spine =
Rotation of the spine, left and right =
Side flexion of the spine, left and right =
Flexion of the hip =
Abduction of the hip =
Adduction of the hip =
Extension of the hip =
Medial rotation of the hip =
Lateral rotation of the hip =
Active Movements That Stress the Sacroiliac Joints:
Forward flexion of the spine = (40° to 60°)
Extension of the spine =(20° to 35°)
Rotation of the spine, left and right =(3° to 18°)
Side flexion of the spine, left and right =(15° to 20°)
Flexion of the hip =(100° to 120°)
Abduction of the hip =(30° to 50°)
Adduction of the hip =(30°)
Extension of the hip =(0° to 15°)
Medial rotation of the hip =(30° to 40°)
Lateral rotation of the hip =(40° to 60°)
When the SI joint is injured, abduction can cause pain to this joint, which muscle pulls the ilium away from the sacrum during resisted isometrics?
Gluteus Medius
side flexion to the same side increases what stress to the sacroiliac joint on that side?
Shearing stress
Normally the PSISs __________ when the patient stands and __________ when the patient lies prone
Normally the PSISs approximate when the patient stands and separate when the patient lies prone
When a patient stands on one leg, which pubic bone moves forward as a result of rotation at the sacroiliac joint.
Same side / Supported side
True or False:
the earlier counternutation occurs during forward flexion, the more vulnerable the sacroiliac joint will be to instability problems.
True