10. Arteritic AION
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
What is anterior ischemic optic neuropathy (AION), and in whom is it most common?
AION is an acute ischemic optic neuropathy caused by impaired blood supply to the anterior optic nerve. It is the most common cause of acute optic neuropathy in elderly patients.
What are the two major types of AION, and what conditions are they associated with?
Non-arteritic AION: associated with vascular risk factors
Diabetes
Hypertension
Hypercholesterolemia
Sleep apnea
Arteritic AION: associated with giant cell arteritis, also called temporal arteritis
What is the pathogenesis of arteritic ischemic optic neuropathy?
Arteritic ION results from inflammatory vascular occlusion of the optic nerve blood supply, especially near the lamina cribrosa.
Key mechanisms include:
Occlusion or infarction of optic nerve blood supply
Immune-mediated inflammation
Luminal obstruction causing ischemia
Why does giant cell arteritis cause arteritic AION?
Giant cell arteritis is an inflammatory vasculitis that affects medium and large arteries.
It causes vessel wall inflammation, narrowing, and occlusion, which can reduce blood flow to the optic nerve and cause arteritic AION.
Why is arteritic AION considered an ocular and medical emergency?
Arteritic AION is an emergency because it is commonly caused by giant cell arteritis, which can rapidly cause severe, irreversible vision loss and may threaten the fellow eye if untreated.
What systemic disease is strongly associated with giant cell arteritis?
Polymyalgia rheumatica, or PMR. About 50% of patients with giant cell arteritis have symptoms of PMR.
Besides giant cell arteritis, what systemic diseases can be associated with arteritic ischemic optic neuropathy?
Arteritic ION can be associated with rheumatologic and inflammatory disorders, including:
Systemic lupus erythematosus
Polyarteritis nodosa
Rheumatoid arthritis
Behçet’s disease
What is the typical epidemiology of giant cell arteritis?
Giant cell arteritis is the most common vasculitis in the elderly.
Usually age >60 years
Incidence about 18 per 100,000 per year
More common in females than males, about 3:2 or 3:1
More common in Caucasians
Unusual in Black and Asian populations
What are the major demographic and genetic risk factors for giant cell arteritis?
Age >50, especially elderly
Female sex
Northern European ancestry
Family history
Genetic susceptibility, including HLA polymorphisms
What clinical and lifestyle factors increase risk for giant cell arteritis?
Risk factors include:
History of polymyalgia rheumatica
History of vascular disease
Smoking
Low body mass index
Estrogen deficiency
What is the basic pathophysiology of giant cell arteritis, and what size vessels does it affect?
Giant cell arteritis is believed to be an autoimmune inflammatory response against arterial elastic tissue.
It primarily affects medium and large arteries, causing vessel wall inflammation → luminal narrowing/occlusion → ischemia.
Which arteries are typically involved in giant cell arteritis?
GCA commonly affects branches supplying the head and eye, especially:
Temporal arteries
Posterior ciliary arteries
Ophthalmic artery
Central retinal artery
Besides cranial arteries, what major systemic arteries can be affected in giant cell arteritis?
GCA may also involve large systemic arteries, including:
Aorta
Coronary
Subclavian
Femoral
Radial
Cerebral
Hepatic
Renal
Mesenteric
Iliac arteries
What are the classic systemic symptoms of giant cell arteritis?
New-onset headache, often described as throbbing or pressure-like
Jaw claudication
Scalp tenderness
Neck or shoulder muscle ache/stiffness
Weight loss
Low-grade fever
Fatigue
What is jaw claudication in giant cell arteritis?
Jaw claudication is pain, fatigue, or discomfort while chewing, especially with chewing tougher foods or using the gums/jaw repeatedly.
When can systemic symptoms of giant cell arteritis occur relative to ocular symptoms?
Systemic symptoms can occur weeks to months before ocular symptoms.
Some patients may have occult GCA, where systemic symptoms are minimal or absent despite ocular involvement.
What inflammatory lab findings support a diagnosis of giant cell arteritis?
GCA commonly causes elevated inflammatory markers:
Elevated ESR: often >40 mm/hr
Elevated CRP: normal is <2.45 mg/dL
CRP is more sensitive than ESR
Anemia may also be present
How do you estimate the upper limit of a “normal” ESR by age and sex?
Males: normal ESR ≈ age / 2
Females: normal ESR ≈ (age + 10) / 2
Which inflammatory marker is more sensitive for giant cell arteritis: ESR or CRP?
CRP is more sensitive than ESR for GCA.
CRP sensitivity ≈ 100%
ESR sensitivity ≈ 92% when ESR is >47 mm/hr
What temporal artery findings are suggestive of giant cell arteritis?
The temporal artery may be:
Tortuous
Nodular
Swollen
Red
Tender
Lacking a palpable pulse
Why are systemic signs important in suspected GCA-related vision loss?
↑ ESR / ↑ CRP
Anemia
Tender or abnormal temporal artery
New headache, jaw claudication, scalp tenderness
What additional imaging tests can be used in suspected giant cell arteritis, and what are their limitations?
Imaging may help support GCA diagnosis, but temporal artery biopsy is more definitive.
MRI angiography
Can assess vascular involvement
Limitations: invasive/contrast dye risks, false negatives
PET scan
Not ideal for cranial GCA
Useful for detecting large-vessel vasculitis
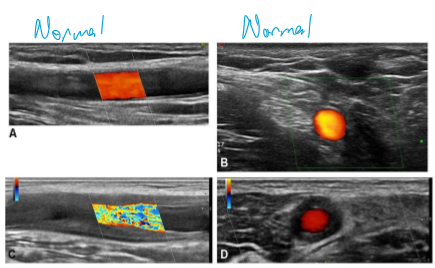
Ultrasonography
Can show the halo sign
About 80% sensitivity/specificity
What is the “halo sign” on ultrasound in giant cell arteritis?
The halo sign is a dark, hypoechoic ring around the temporal artery caused by arterial wall edema/inflammation.
What is the diagnostic importance of temporal artery biopsy in giant cell arteritis?
Temporal artery biopsy is highly useful because a positive biopsy supports GCA in about 90-95% of cases.
What histologic findings are seen on temporal artery biopsy in GCA?
Classic biopsy findings include:
Fragmentation/disruption of the internal elastic lamina
Swollen endothelium
Patchy degeneration of smooth muscle cells
Granulomatous inflammation with macrophages, lymphocytes, and/or giant cells
Fibrosis, hyaline thickening, and thrombosis
What are the major systemic complications of untreated giant cell arteritis?
Untreated GCA causes increased morbidity and mortality due to vascular occlusion.
Major complications include:
Blindness
Stroke
Aortic aneurysm
How does treatment affect mortality in giant cell arteritis?
If GCA is treated, there is no increased mortality.
If untreated, morbidity and mortality increase due to vascular occlusion complications such as blindness, stroke, and aortic aneurysm.
What is the typical disease course of giant cell arteritis?
GCA can be self-limiting within 1-2 years, but untreated disease can still cause serious vascular complications before resolution.
What ocular symptoms can occur in giant cell arteritis before permanent vision loss?
Early ocular symptoms may include:
Blurred vision
Transient visual disturbance
Amaurosis fugax
Diplopia
What is amaurosis fugax in GCA, and why is it clinically important?
Amaurosis fugax is transient monocular vision loss due to temporary ocular ischemia.
In GCA, it occurs in about 10% of patients and may appear days to months before AION.
How common is diplopia in giant cell arteritis, and what does it suggest?
Diplopia can be a presenting symptom in GCA.
Frequency:
Reported range: 2-43%
Average: about 12%
What are the major ocular signs of giant cell arteritis?
Major ocular signs include:
Arteritic AION
Ophthalmoparesis, especially 6th nerve palsy
Central retinal artery occlusion
Ptosis, unilateral or bilateral
How can giant cell arteritis cause diplopia or ocular motility problems?
GCA can cause ophthalmoparesis due to ischemia affecting ocular motor nerves or extraocular muscle blood supply.
Common findings include:
6th nerve palsy → impaired abduction → horizontal diplopia
Ptosis → can be unilateral or bilateral
What are unusual ocular signs that may occur in giant cell arteritis?
Unusual signs include:
Anterior segment ischemia
White eye
Hypotony
Corneal edema
Anterior chamber reaction
Marginal corneal ulceration
Scintillating scotoma
Visual hallucinations
Conjunctivitis
Bilateral uveitic glaucoma
How common is visual loss in giant cell arteritis, and what is the most common cause?
Visual loss occurs in about 12–50% of GCA cases.
Most common cause:
Infarct of the prelaminar optic nerve → arteritic AION, about 90%
Other causes:
Central retinal artery occlusion: 1–3%
Ischemic retinopathy: 7%
Why is untreated GCA considered a vision-threatening emergency?
Untreated GCA can rapidly involve the fellow eye.
About 65% of untreated patients with vision loss develop binocular vision loss.
Timing of second-eye involvement:
1/3 within 24 hours
1/3 within 1 week
1/3 within 4 weeks
When does the risk of additional vision loss decrease in GCA?
The risk of further vision loss becomes low after 6 months, especially with treatment.
What is the typical visual presentation of arteritic AION?
Arteritic AION typically presents with sudden, painless vision loss.
What are the key clinical signs of arteritic AION?
Arteritic AION typically shows:
Decreased visual acuity
Afferent pupillary defect (APD)
Pale, swollen optic nerve head
Possible sectoral peripapillary hemorrhages
May be associated with cilioretinal artery occlusion
How severe is visual acuity loss in arteritic AION?
Visual loss is often severe:
20/40 or better: 18%
20/40–20/200: 24%
20/200 or worse: 58%
How does visual acuity loss compare between arteritic and non-arteritic AION?
Arteritic AION causes more severe vision loss than non-arteritic AION.
Comparison pattern:
NA-AION: more likely to have better acuity, including >20/40
A-AION: more likely to have severe acuity loss, especially <20/200
What optic disc finding helps distinguish arteritic AION from non-arteritic AION?
Arteritic AION classically causes a pale, swollen optic nerve head due to severe ischemia.
What vascular retinal findings may accompany arteritic AION?
Arteritic AION may be associated with:
Sectoral peripapillary hemorrhages
Cilioretinal artery occlusion
How do arteritic AION and non-arteritic AION differ in patient risk factors and systemic associations?
Non-arteritic AION:
Males ≈ females
Associated with vascular risk factors: diabetes, HTN, hypercholesterolemia, sleep apnea
Typically no systemic symptoms
ESR/CRP usually normal
Arteritic AION:
Females > males
Associated with GCA/temporal arteritis and polymyalgia rheumatica
Systemic symptoms: headache, jaw claudication, weight loss, scalp tenderness, malaise
ESR/CRP typically elevated
What optic disc findings help distinguish non-arteritic AION from arteritic AION?
Non-arteritic AION:
Hyperemic disc edema
More flame-shaped hemorrhages
Small crowded disc at risk
Segmental optic nerve head edema
Arteritic AION:
Pale, chalky-white swollen disc
Retinal ischemia and cotton wool spots may be present
Normal-to-large cup
Diffuse optic nerve head edema
How do treatment and prognosis differ between arteritic and non-arteritic AION?
Non-arteritic AION:
No proven effective treatment
Up to 3-line improvement in ~43%
Fellow eye involvement <30%
Arteritic AION:
Requires high-dose steroids urgently
Poor prognosis for visual recovery
Fellow eye may be involved in up to 95% if untreated
What retinal and visual function signs can occur in arteritic ischemic optic neuropathy?
Arteritic ION may show:
Constricted retinal arterioles in ~50%
Decreased color vision / red desaturation
Nerve fiber bundle field defects
Common field defects:
Altitudinal defects, often inferior: 70–80%
Central scotoma: ~30%
What visual field defect is most characteristic of arteritic ION?
The most common visual field defect is an altitudinal defect, often inferior, occurring in about 70-80% of cases.
What is the risk to the fellow eye in untreated arteritic ION?
Untreated arteritic ION has a high risk of fellow-eye involvement.
About 65% may develop an attack in the other eye within hours to days.
Is vision loss from arteritic ION reversible?
Vision loss is generally irreversible, because it results from ischemic infarction of the optic nerve.
However, if pulse steroids are given within 36 hours of acute vision loss, vision may significantly improve in some cases.
What conditions should be considered in the differential diagnosis of arteritic AION?
Differential diagnoses include:
Non-arteritic AION
Central retinal vein occlusion
Compressive optic neuropathy
Papilledema
Buried optic disc drusen
Other optic neuritis causes, such as:
Sarcoidosis
Syphilis
How can central retinal vein occlusion mimic arteritic AION, and what fundus findings suggest CRVO instead?
CRVO can cause vision loss with optic disc edema, but it typically has prominent retinal vascular findings:
Diffuse retinal hemorrhages
Cotton wool spots
Macular edema
Optic disc edema
What immediate workup should be done when arteritic AION from GCA is suspected?
Initial management should include:
Ask about GCA symptoms
Headache
Jaw claudication
Scalp tenderness
Weight loss, malaise, fever
PMR symptoms
Order CBC, ESR, and CRP stat
Arrange temporal artery biopsy within 1 week
What is the main treatment for arteritic AION due to suspected GCA?
Treat immediately with high-dose systemic corticosteroids, typically around 40–60 mg/day prednisone.
Effects:
Relieves systemic symptoms
Usually gives little improvement in visual acuity
Decreases risk of vision loss in the other eye
Often required long-term
Why is urgent steroid treatment critical in arteritic AION?
Without treatment, there is a much higher risk of bilateral visual loss.
The slide notes a 3× greater chance of bilateral vision loss without treatment.
What medication may be used as low-dose therapy to reduce vascular complications in GCA?
Low-dose aspirin, commonly 75 mg, may be used to help reduce thrombotic/ischemic complications such as stroke.
What is the general long-term steroid taper strategy for arteritic AION/GCA?
After initial treatment for 2-4 weeks, taper gradually:
Decrease by 10 mg every 2 weeks until 20 mg
Then decrease by 2.5 mg every 2-4 weeks until 10 mg
Then decrease by 1 mg every 1-2 months
How long should symptoms and ESR remain controlled during treatment for GCA?
Symptoms and ESR should remain normalized for 6-12 months or longer.
What are important complications of long-term corticosteroid therapy?
Long-term steroids can cause Cushing-like complications, including:
Weight gain
Muscle wasting
Increased blood pressure
Increased infections
Delayed wound healing
Stomach irritation
Cataracts
Osteoporosis
What are steroid-sparing therapies used in long-term management of GCA?
Steroid-sparing therapies may include:
Methotrexate
Abatacept
What is the role of tocilizumab in giant cell arteritis treatment?
Tocilizumab (Actemra) is an FDA-approved steroid-sparing agent for GCA.
Mechanism/main effect:
IL-6 receptor antagonist → reduces inflammatory signaling
Clinical use:
Given as a subcutaneous injection
Used with steroids to help achieve remission and reduce steroid exposure
What is the role of upadacitinib in giant cell arteritis treatment?
Upadacitinib (RINVOQ) is a steroid-sparing agent used in GCA.
Mechanism/main effect:
Janus kinase (JAK) inhibitor → decreases inflammatory cytokine signaling
Clinical details:
Oral medication
Dose on slide: 15 mg PO daily
What is the treatment goal in a treat-to-target approach for GCA?
The treatment target is remission, defined as:
Absence of clinical symptoms
Absence of systemic inflammation
Main goals:
Maintain remission
Prevent tissue ischemia
Prevent vascular damage
How should treatment selection and monitoring be individualized in GCA?
Treatment choice should be based on:
Disease severity and activity
Comorbidities
Predictors of outcome
Response during follow-up
Monitoring:
Assess disease activity as frequently as every 1–4 weeks until remission
Once stable on therapy, monitor every 3–6 months
After remission, maintain with the minimal effective dose
Drug-free remission may be possible in some patients
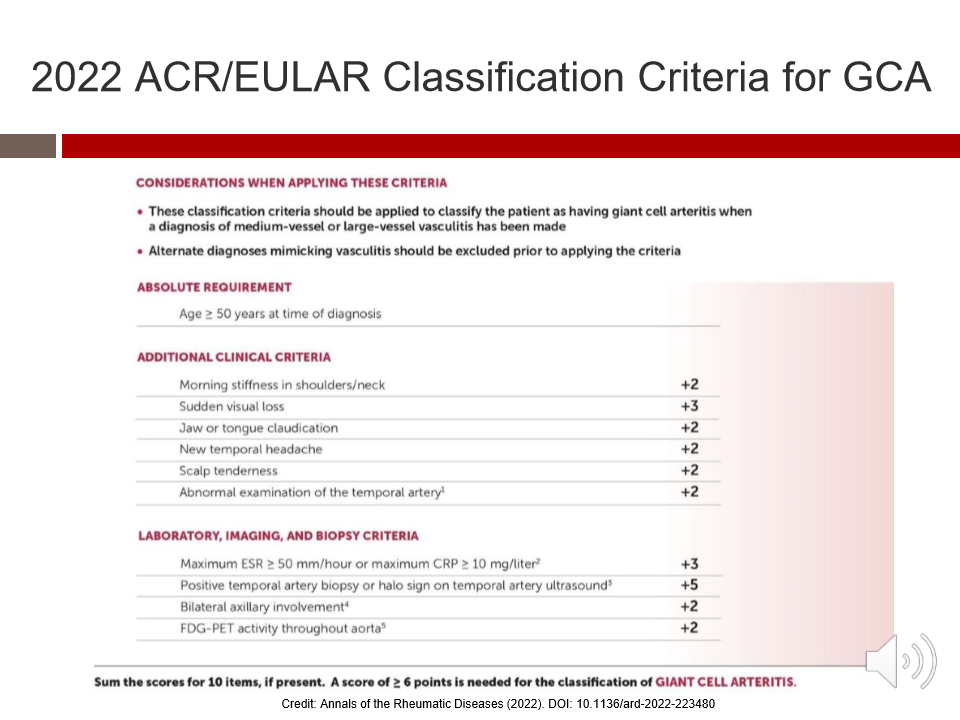
What is the absolute requirement before applying the 2022 ACR/EULAR classification criteria for giant cell arteritis?
The patient must be ≥50 years old at the time of diagnosis.
Also, these criteria should be applied only after:
A diagnosis of medium- or large-vessel vasculitis is being considered
Alternate diagnoses mimicking vasculitis have been excluded
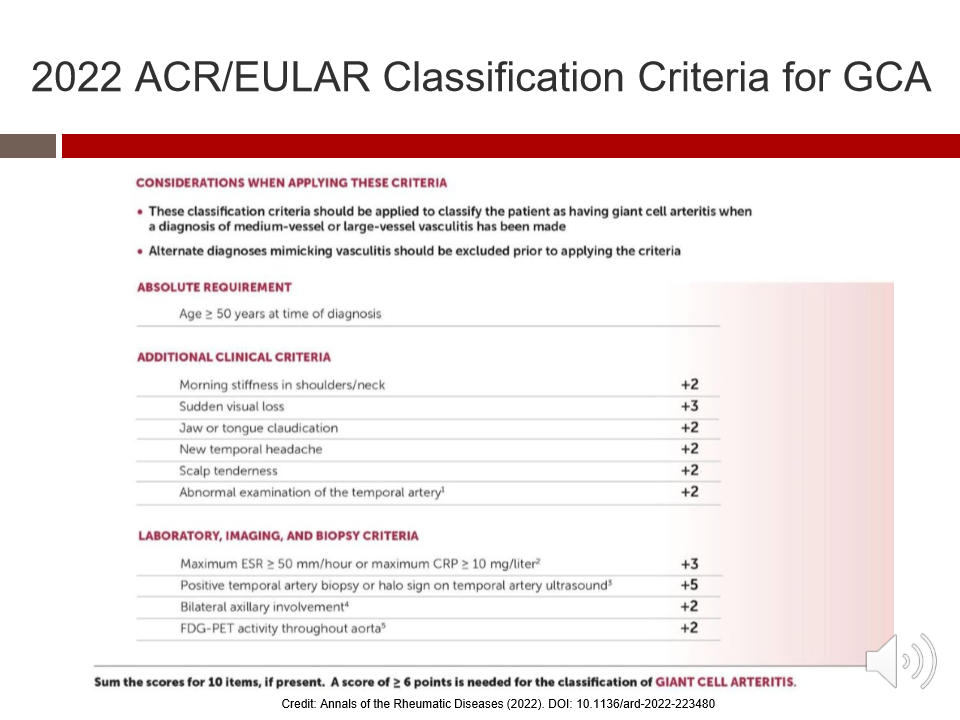
What score is needed to classify a patient as having giant cell arteritis using the 2022 ACR/EULAR criteria?
A total score of ≥6 points is needed to classify the patient as having GCA.
In an older patient with blurry vision, what findings in this case suggest optic neuropathy rather than refractive blur?
Clinical criteria include:
Morning stiffness in shoulders/neck: +2
Sudden visual loss: +3
Jaw or tongue claudication: +2
New temporal headache: +2
Scalp tenderness: +2
Abnormal temporal artery exam: +2
What systemic symptoms should raise suspicion for giant cell arteritis?
Classic systemic symptoms of GCA include:
New-onset headache: common, about 67–85%
Jaw claudication
Scalp tenderness
Neck or shoulder muscle ache/stiffness
Weight loss
Low-grade fever
Fatigue
When can systemic symptoms of GCA occur relative to ocular symptoms?
Systemic symptoms may occur weeks to months before ocular symptoms.
However, some patients may have occult GCA, meaning they have little or no systemic symptoms despite significant ocular disease.
Why is GCA considered both an ocular and medical emergency?
GCA is an emergency because it can cause severe ischemic complications, including:
Permanent vision loss
Fellow-eye involvement
Myocardial infarction
Aortic dissection
Stroke or large-vessel ischemia
What is the key rule for sudden vision loss in patients over age 50?
In any patient >50 years old with sudden vision loss, GCA must be ruled out urgently.
Workup/treatment should include:
Ask about systemic GCA symptoms
Order CBC, ESR, CRP stat
Refer urgently to neuro-ophthalmology or the ER
Start systemic steroids ASAP if suspected
Should steroid treatment wait until temporal artery biopsy confirms GCA?
No. If GCA is suspected, treat with systemic steroids immediately, even before temporal artery biopsy.
Why: Delaying treatment increases risk of irreversible vision loss and fellow-eye involvement.