Describe the anatomic component of the vestibular system • Recognize typical clinical signs of vestibular disease • Differentiate between central versus peripheral vestibular disease • Recognize paradoxical and bilateral vestibular disease • Discuss causes of peripheral vestibular disease in dogs and cats: – Describe clinical features of Canine Idiopathic Geriatric Vestibular disease • Discuss causes of central vestibular disease in dogs and cats • Recognize and describe clinical signs of diseases affecting the cranial nerves • Discuss causes of cranial nerves disease in dogs and cats – Describe clinical features of Idiopathic Trigeminal Neuritis and Idiopathic Facial Nerve Paralysis
Vestibular System • Responsible for
maintaining balance regulating the position of eyes, trunk and limbs in relation to changes in position of the head
Maintaining balance depends on
Vestibular receptors (main contributor)
Vision
Proprioceptive receptors in joints and tendons
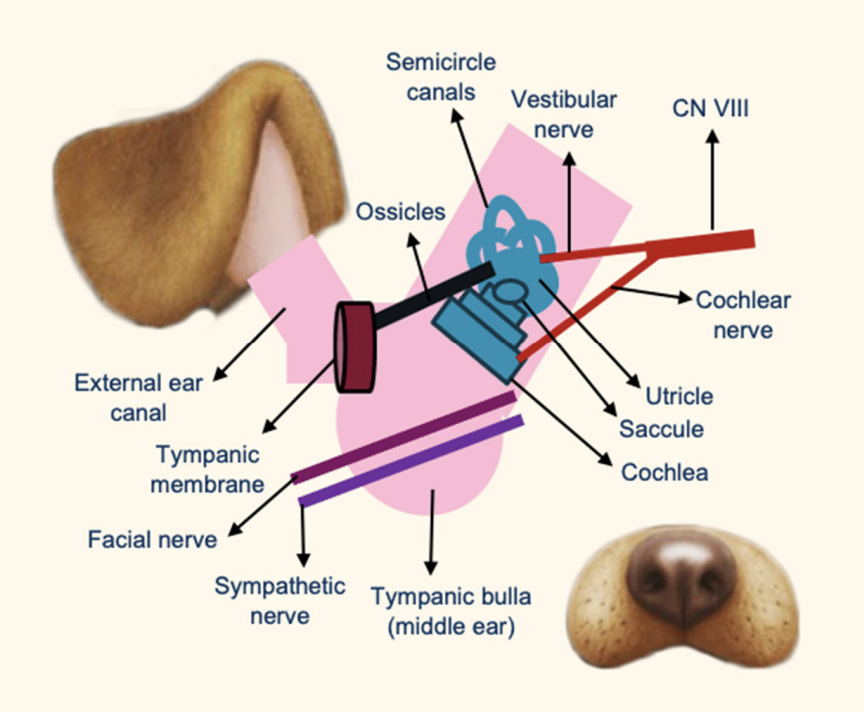
Anatomy of Vestibular System: Peripheral Vestibular System
receptor located at
nerve innervation
utricle and saccule, and semicircular canals
Vestibular nerve (CN VIII)
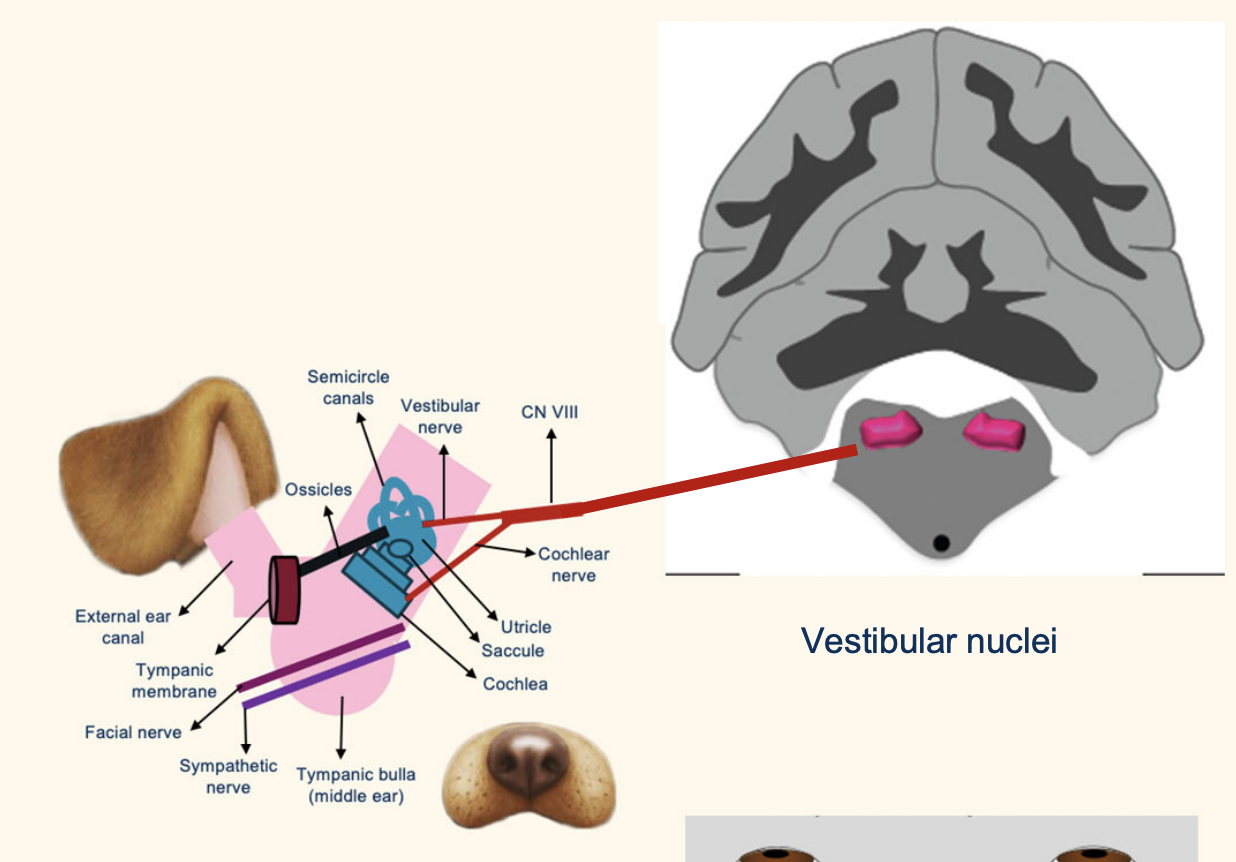
Anatomy of Vestibular System: Central Vestibular System
2 main part
name 1 for brainstem and 1 fro cerebellum
Vestibular nuclei – Brainstem
Cerebellum
Caudal cerebellar peduncle • Fastigial nucleus • Flocculonodular lobe
Clinical Signs of Vestibular Disease
add later exhaus list
Head tilt
Nystagmus
Vestibular ataxia (“off balance”
Vomiting and nausea
Ventral or ventrolateral positional (not static) strabismus
head tilt
Nystagmus:
define nustagus side depend on ____ phase.
fast face is ____ to leision
involuntary rhythmic oscillation of the eyes (jerk eye movement with slow and fast phase)
Physiologic nystagmus (vestibulo-ocular)
Pathological (spontaneous or positional):
Horizontal or Rotatory
Vertical indicated central disaese (RARE)
ast phase CONTRALATERAL to the lesion
Vestibular ataxia:
Falling – Rolling – Drifting – Tight circles toward the side of the lesion (cats)
Decreased extensor tone ipsilateral limbs, increased extensor tone contralateral limbs
Vomiting and nausea
Acute vestibular disease – Projections to the emetic center within medullary reticular formation
Ventral or ventrolateral strabismus
eye stays in position when lift head
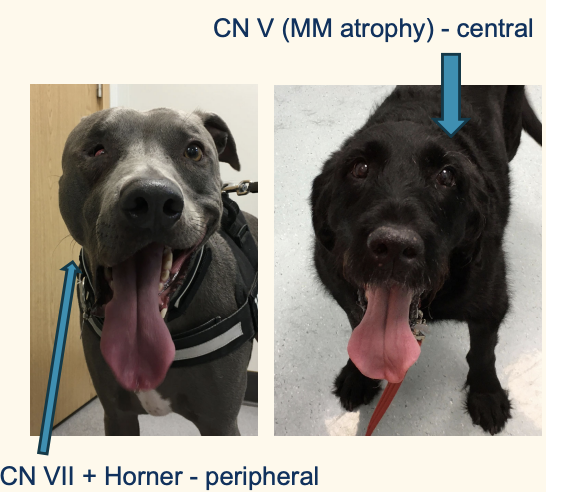
Differentiation of Peripheral versus Central Vestibular Diseas
the following indicate central diseae=se
Hemiparesis and postural reaction deficits IPSILATERAL to the lesion
Vertical nystagmus (rare)
Nystagmus changing direction with changes in head position
Cranial nerve deficits (other than CN VII and sympathetic innervation to the eye)
Cerebellar signs
Decreased level of consciousness
Paradoxical vestibular syndrome
Hemiparesis and conscious proprioceptive deficits in vestibular disease
• Ipsilateral to the lesion
central leision
Clinical Signs of Vestibular Disease: Cranial nerve deficits
Deficits of other cranial nerves besides CN VII and Horner = central lesion
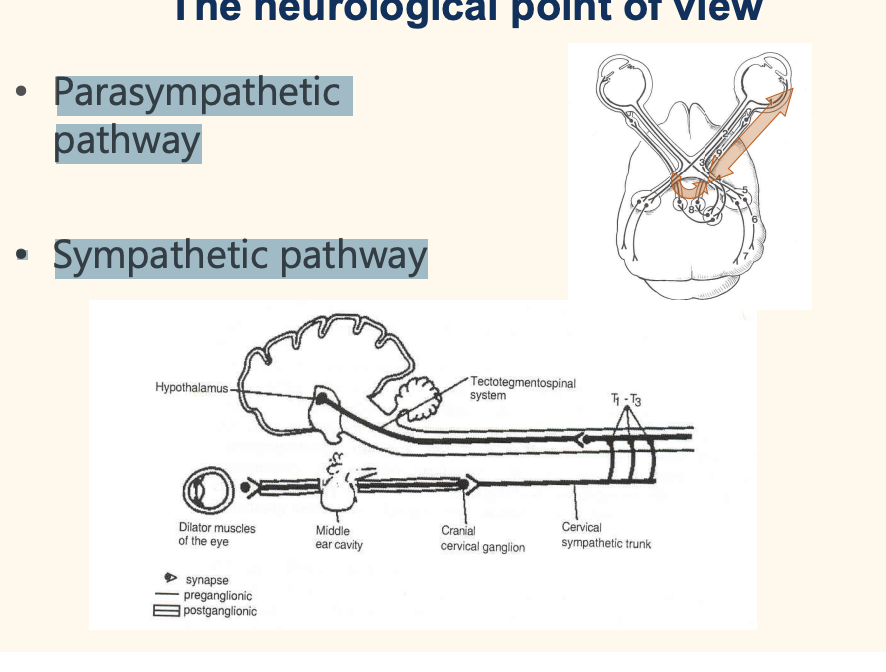
Horner syndrome— sym[athetic innervationof eye causes 4
Ptosis
Enophtalmus
Miosis
3rd eyelid protrusion
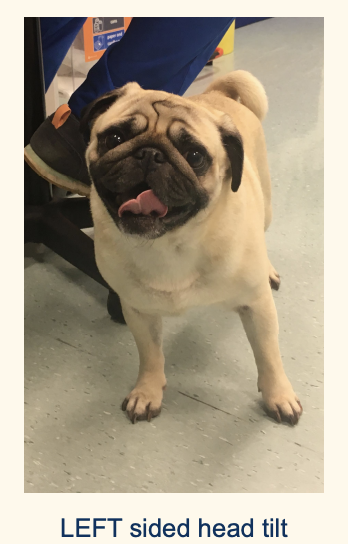
Paradoxical vestibular syndrome (rare)
contradictory vestibular sign contralateral to leision at cerebelum
Caused by loss of cerebellar inhibition of the vestibular output
pug L side head tilt actually have an infart leision at R cerebellum. right postural reaction deficit.
Bilateral Vestibular Disease
Absent physiologic and/or pathologic nystagmus
Absent head tilt
Side-to-side swaying of the head
Broad-base stance
Falling to either side
Diagnostic Procedures for Vestibular Disease
Physical, neurological, otoscopic examination (could may well be otitis externa/media!)
• Hematology and biochemistry
Skull radiographs
CT scan or MR
what wlse could u do?for Vestibular Disease dx procedure
Ear cytology • Ear culture and sensitivity • Myringotomy • CSF analysis • Infectious diseases titers on serum and/or CSF • Biopsy/histopathology
Differential diagnoses
Vascular • Infectious/Inflammatory • Traumatic • Toxic • Anomaly • Metabolic • Idiopathic • Iatrogenic • Neoplastic • Nutritional • Degenerative
wittamiinnd
Anomalous ddx
– Bilateral congenital vestibular disease: • Akitas • Beagles
Congenital peripheral vestibular disease: • German Shepherds • Doberman pinchers • English cocker spaniel • Siamese cat • Burmese cat
Metabolic: ddx Hypothyroidism (dog)
Associated with various neurological signs from seizures to mega esophagus, laryngeal and facial nerve paralysis – Mucinous deposits in and around facial and vestibular nerve may cause compression of the axons as they pass through the internal acoustic meatus of the temporal bone
Neoplastic ddx
Squamous cell carcinoma (cat) – Ceruminous gland adenoma (dog) and adenocarcinoma (cat) – Papillary adenoma (dog) – Others: lymphosarcoma, osteosarcoma, chondrosarcoma, fibrosarcoma.
Iatrogenic: ddx
chlorhexidine, aminoglycosides – Streptomycin and gentamycin vestibular receptors – Neomycin, kanamycin and amikacin auditory receptors
ototoxicity to ruptured eadrum; irreversible
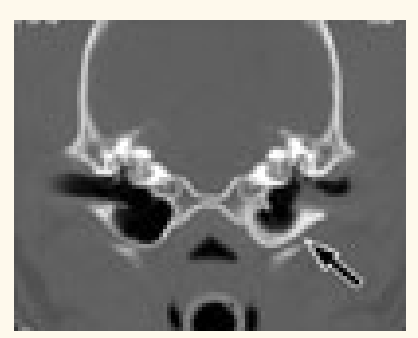
Infectious ddx • Otitis media-interna
Otoscopic examination is required for dogs or cats presented with peripheral vestibular disease
clinical history of previously diagnosed otitis externa
Medical treatment (ear flush and/or myringotomy) or surgical
another infetious in cat
• Inflammatory polyps (cats)
infectious ddx: Idiopathic vestibular disease:
both cat and dog
• Peracute onset and improving progression (in cats a deterioration can be seen) • Usually, older patients • Peripheral vestibular disease – Vomiting, nausea, and severe vestibular deficits • Spontaneous improvement in 2-3 days • Normal in 7-10 days - in some cases up to 2-3 weeks and sometimes there is a residual deficits (head tilt or mild ataxia) • Recurrence is possible • No specific treatment –anti-emetic (maropitant) and anti-nausea (ondansetron) medication
CENTRAL PREV IS PERI
Degenerative: centtral vestibular ddx
Lysosomal storage diseases
Anomalous ddx Central Vestibular Disease
Arachnoid cyst – Cerebellar cyst – Hydrocephalus
Nutritional: ddx central
Thiamine deficiency – Bilateral symmetrical central vestibular signs
esp cat w fish
dog wtih cooked meat? (dc)
neoplastic: central ddx
Thiamine deficiency – Bilateral symmetrical central vestibular signs
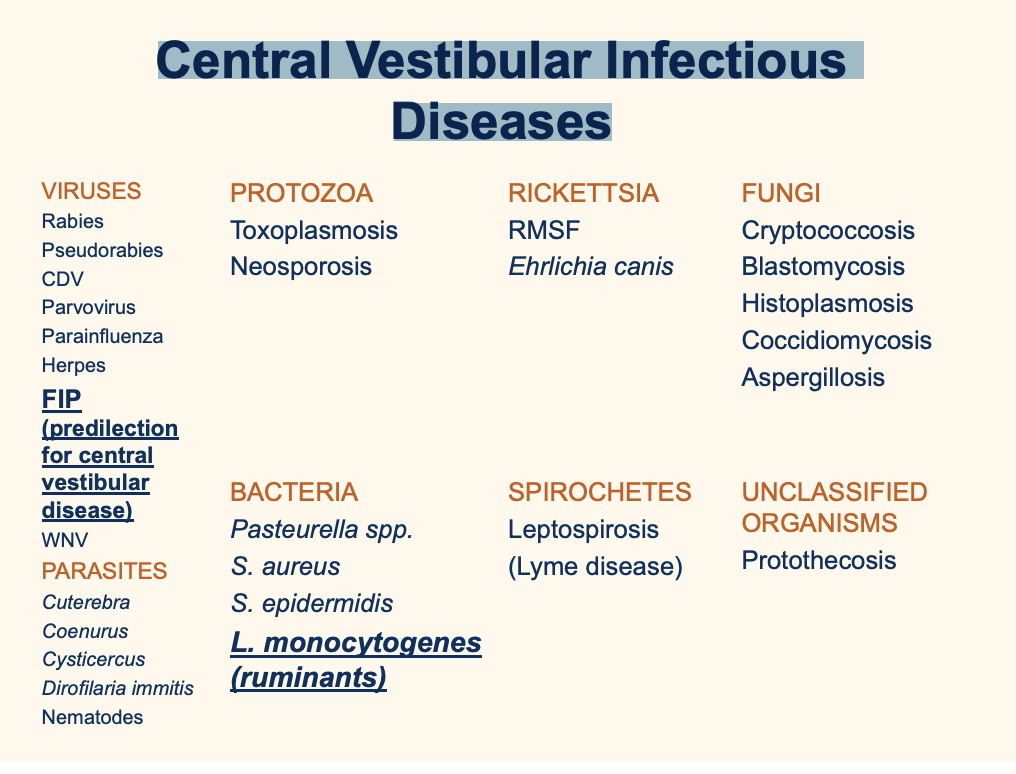
Central Vestibular Infectious Diseases
main cat: FIP, leisteria in ruminant
Central Vestibular Inflammatory Diseases most common
Granulomatous Meningoencephalomyelitis (GME)
Granulomatous Meningoencephalomyelitis (GME)
Subacute to chronic sterile inflammation, suspected immunemediated disorder • Middle age small breed dogs • Disseminated, focal and ocular (optic neuritis) form • Prognosis guarded to poor • Definitive diagnosis: histopathology • Traditional treatment: immunosuppressive doses of corticosteroids • Prolonged survival time with other immunosuppressive agents in addition to prednisolone such as cytarabine, cyclosporine, lomustine, procarbazine
toxic ddx: Central Vestibular Disease
– Metronidazole intoxication
Characterized by anorexia, vestibular ataxia and vertical nystagmus • Recovery may be enhanced by administration of diazepam at 0.4 mg/kg TID for 3 days. • Diazepam competitively displacing metronidazole from GABA receptors
Lead poisoning
Central Vestibular Disease what other ddx
Traumatic • Vascular
Diseases of the cranial nerves of dogs and cats: Cranial Nerve I - Olfactory
rare to be singular injury
Loss of appetite, anosmia – difficult to assess • Nasal discharge, nasal obstruction
DD: – Viral, bacterial or fungal rhinitis – Nasal adenocarcinoma, meningioma, neuroblastoma
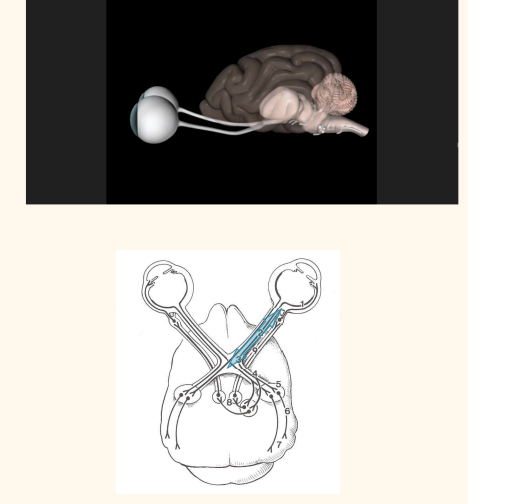
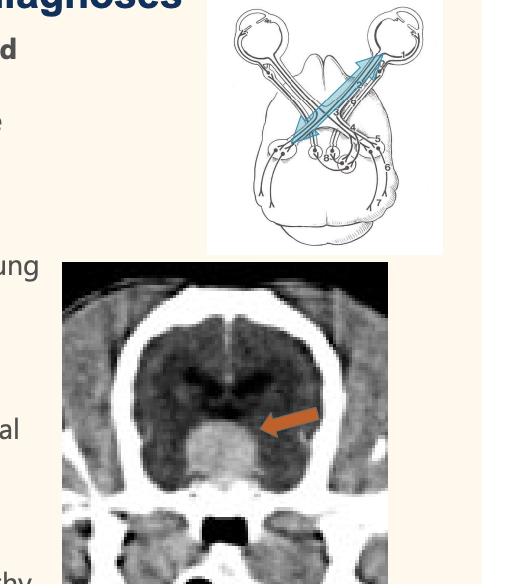
Diseases of the cranial nerves of dogs and cats Cranial nerve II - Optic
optic nerve is an extension of the CNS— any dx affecting CNS will effect ON
Neuroepithelial cells (rods & cones), bipolar and ganglion cells 2. Optic nerve 3. Optic chiasm 4. Optic tract
—>Lesion: blindness and pupillary light reflex (PLR) deficit
5 Lateral geniculate nucleus 6. Optic radiation 7. Occipital lobe
—>Lesion: central blindness
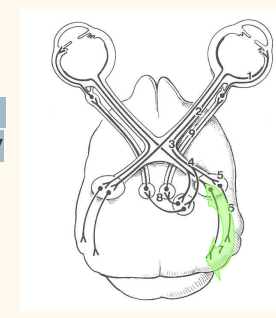
7a. Pretectal nuclei 8. Edinger-Westphal nucleus 9. CN III – Oculomotor nerve 10. Ciliary ganglion 11. Ciliary nerves 12. Sphincter pupillae muscle
Lesion: mydriasis, lack of response to light stimulus
Blindness and PLRs Step by step evaluation
Menace response CN II, complete visual pathway to occipital cortex, and CN VII 2. Blinking reflex CN V and VII 3. Obstacle course/cotton ball test CN II 4. PLR (direct and consensual) CN II, complete PLR pathway to CN III and sympathetic innervation 5. Ophthalmoscopic exam Retina and CN II
pre chiasmatic (ON, eye itself) (peripheral); post chiasmatic(
Blindness and PLRs Diagnostic procedures
Physical, neurological and ophthalmological examination • Hematology, biochemistry, blood pressure measurements • ERG – electroretinogram (tretinal activity) • Ultrasonography • MRI or CT head • CSF analysis • Infectious disease titers on serum and/or CSF
Blindness without PLRs Differential diagnoses
Degenerative: SARD (sudden aquired retinal degeneration
Anomalous: bilateral hypoplasia of the optic nerve in dog, cat, horse
Neoplastic: pituitary macroadenoma, meningioma, lymphoma
Nutritional: vitamin A deficiency in young growing cattle with stenosis of optic canals
Infectious/inflammatory: optic neuritis with GME, CDV, Toxoplasmosis, Cryptococcosis, Blastomycosis, bacterial infections, FIP
Traumatic: craniofacial trauma
Toxic: fluoroquinolone (cats)
Vascular: feline ischemic encephalopathy (optic tracts)
Blindness with intact PLRs Differential diagnoses (more central)
Degenerative: storage diseases • Anomalous: obstructive hydrocephalus, hydranencephaly in ruminants • Neoplastic: primary and metastatic tumors • Nutritional: polioencephalomalacia in cattle and sheep secondary to thiamine deficiency • Infectious/inflammatory: CDV, Neospora, Toxoplasma • Toxic: lead poisoning • Traumatic: head trauma • Vascular: cerebral ischemia following prolonged seizures, anesthetic accident
Anisocoria mechanism
add description
Lack of sympathetic or parasympathetic
Horner syndrome – Miosis – Ptosis – Enophthalmus – Protrusion third eyelid
parasymth: Mydriasis – ± Ptosis – ± Ventrolateral strabismus
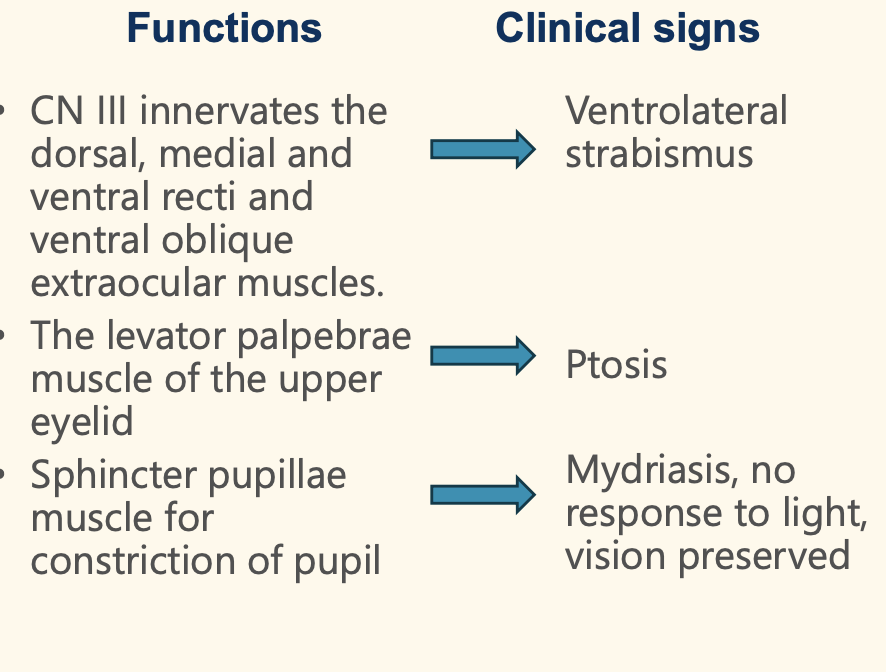
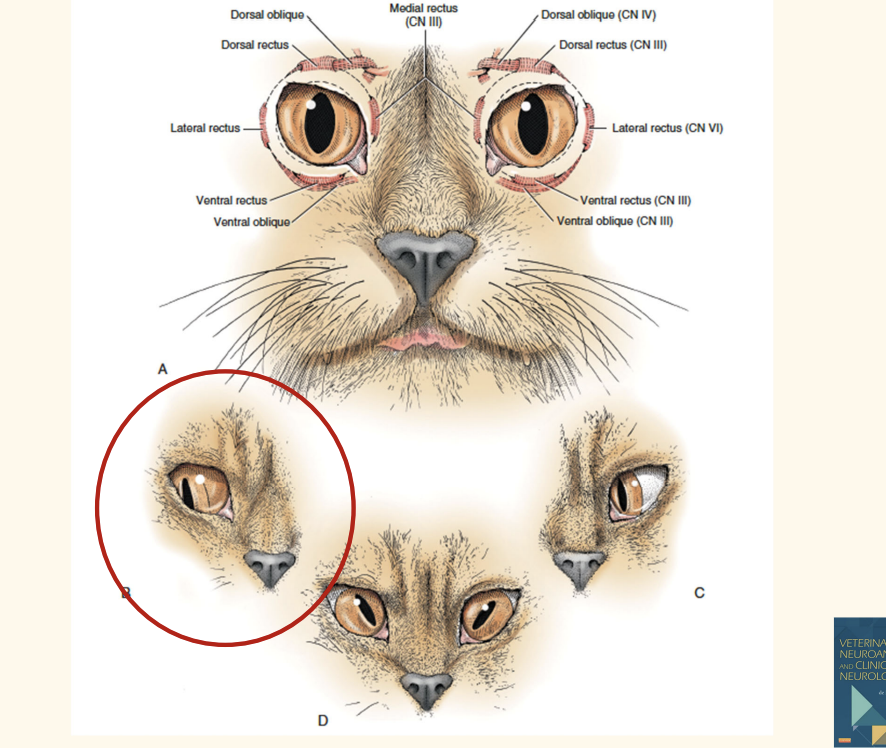
Diseases of the cranial nerves of dogs and cats: Cranial nerve III – Oculomotor
???????
Diseases of the cranial nerves of dogs and cats: Cranial nerve IV - Trochlear
Motor - Innervates the dorsal oblique extraocular muscle • CN IV deficit: lateral rotation of the eye • Ophthalmoscopic exam for animals with round pupil will reveal tilting of the dorsal retinal vein
Diseases of the cranial nerves of dogs and cats: Cranial nerve VI - Abducent
Motor - Innervates the lateral rectus extraocular muscle and the retractor bulbi muscle • CN VI deficit: – Medial strabismus – Inability to retract the globe • Corneal reflex – Ophthalmic branch CN V – CN VI and VII
Cranial nerves III, IV and VI
Diseases affecting motor components causes an absence of eye movements - external ophtalmoplegia • Diseases affecting the parasympathetic innervation of the pupil - internal ophtalmoplegia (mydriasis and ptosis) • Idiopathic oculomotor neuropathy – Good prognosis – improvement with no treatment
Diseases of the cranial nerves of dogs and cats
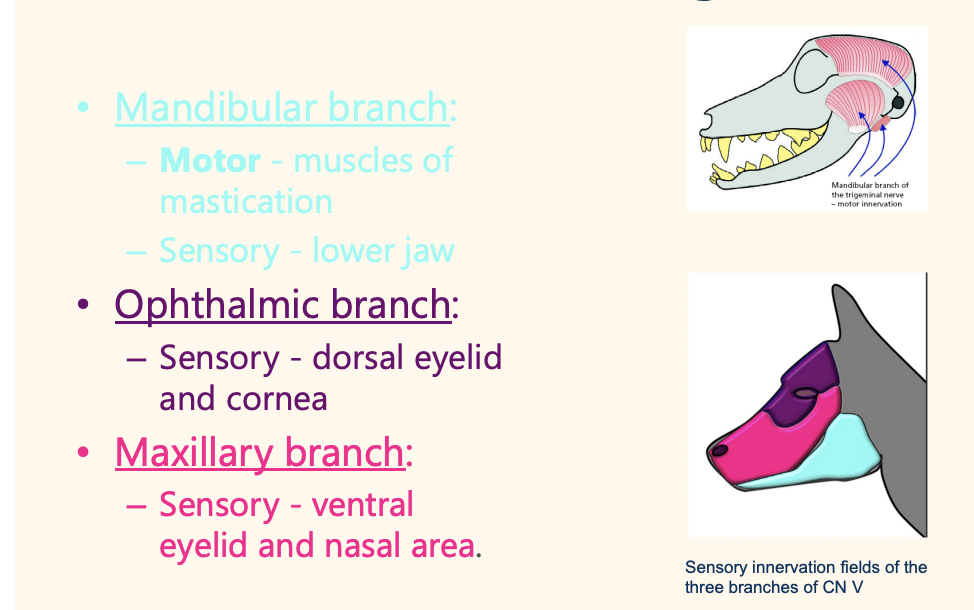
except mandibular branch has motor of mastication fucn
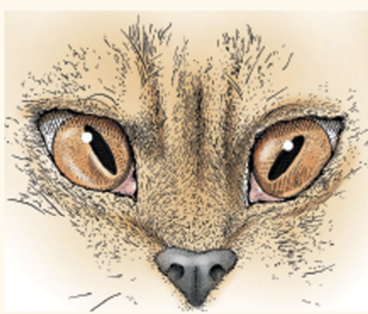
Mandibular branch: – Motor - muscles of mastication – Sensory - lower jaw • Ophthalmic branch: – Sensory - dorsal eyelid and cornea • Maxillary branch: – Sensory - ventral eyelid and nasal area.
Diseases of Cranial nerve V - Assessment
Palpebral reflex • Corneal reflex • Pinch upper lip and chin • Nasal stimulation • Open jaw • Observe/palpate skull to detect atrophy of masticatory muscles (MM)
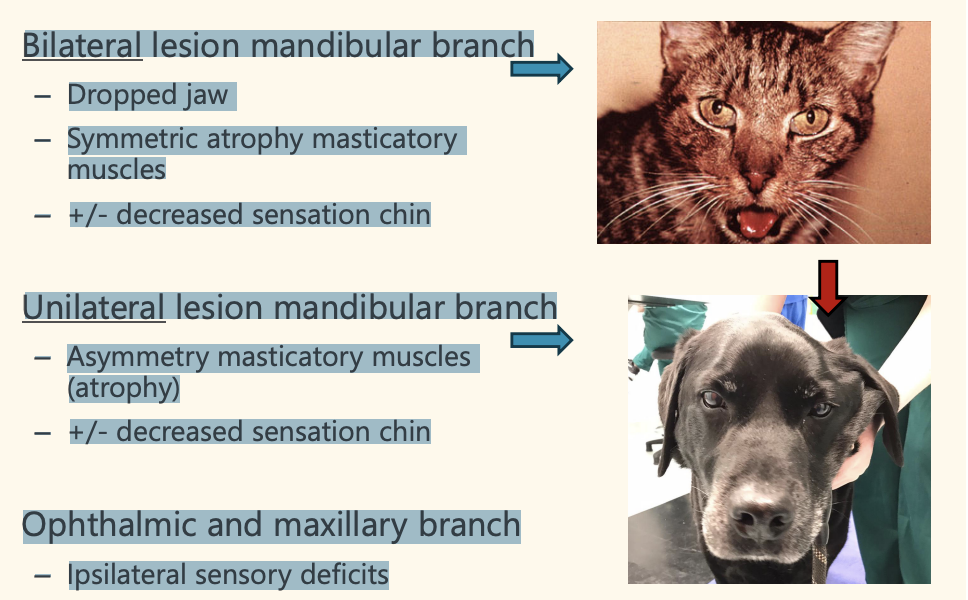
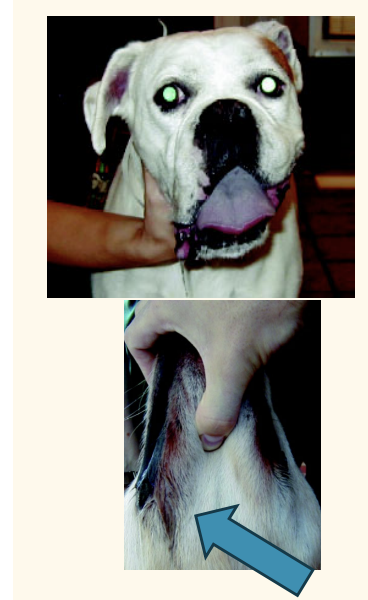
Diseases of Cranial nerve V - Trigeminal
Bilateral lesion mandibular branch – Dropped jaw – Symmetric atrophy masticatory muscles – +/- decreased sensation chin • Unilateral lesion mandibular branch – Asymmetry masticatory muscles (atrophy) – +/- decreased sensation chin • Ophthalmic and maxillary branch – Ipsilateral sensory deficits
Cranial nerve V – Trigeminal ddx: Inflammatory/infectious Bilateral lesion of mandibular branch:
– Lymphoma • More common in cats • Guarded prognosis
– Idiopathic trigeminal neuritis • Acute bilateral paralysis of the masticatory muscles • Dogs and cats • Dropped jaw, drooling saliva, difficulty prehending food and drinking • Horner syndrome sometimes • Treatment - supportive care • Prognosis: Good, resolution within in 2-3 weeks
Cranial nerve V – Trigeminal Tumours ddx
Unilateral lesion of mandibular branch: – Trigeminal nerve sheath tumor • With or without sensory deficits • Unilateral muscle atrophy • Poor prognosis
Cranial nerve VII - Facial function
Motor – muscles facial expression – Sensory – inner surface pinna – Taste sensation rostral two thirds tongue – Parasympathetic function to lacrimal gland, nasal glands, mandibular and sublingual salivary glands
disease of Cranial nerve VII - Facial clnical sign
Facial asymmetry – Absent movements ear, eyelids, upper lip nostrils – Drooling saliva – Neurogenic keratoconjutivitis sicca (KCS) (cannot blink +lacrimal system deficit)
disease of Cranial nerve VII - Facial ddx
Otitis media-interna • Idiopathic facial nerve paralysis • Hypothyroidism • Polyneuropathy • Neoplasms of CN VII or medulla
disae of CN7 ddx: Idiopathic
Idiopathic facial nerve paralysis
Commonly unilateral, but can affect both sides • Unknown pathogenesis (possibly like “Bell’s palsy” in humans) • Middle age to older dogs • Cocker Spaniels are predisposed • Diagnosed excluding other causes of facial neuropathy • Prognosis for recovery of function is guarded • Symptomatic treatment (i.e. artificial tears to protect cornea)
desease of Cranial Nerve VIII Vestibulocochlear clincial sign and diag tests
Deafness • Otoscopic examination • BAER test
desease of Cranial Nerve VIII Vestibulocochlear ddx
Degeneration auditory receptors/ossicles
Congenital deafness
Otitis media-interna
Ototoxic compounds
Trauma
Cranial Nerve IX Glossopharyngeal function
Motor - muscles of pharynx
Sensory - pharyngeal mucosa and caudal third of tongue
Parasympathetic function – zygomatic and parotid salivary glands.
Gag and swallowing reflex
—> Dysphagia + vestibular sign indicated CN 9 leision
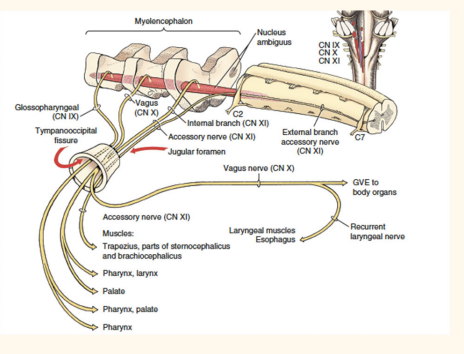
Cranial Nerve X - Vagus function
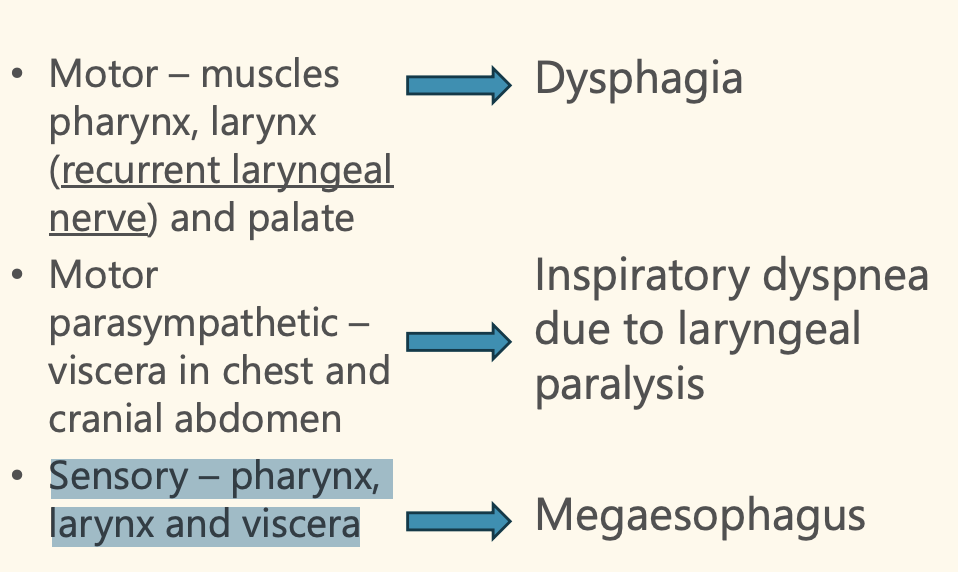
• Motor – muscles pharynx, larynx (recurrent laryngeal nerve) and palate
Motor parasympathetic – viscera in chest and cranial abdomen
Sensory – pharynx, larynx and viscera
diseae of Cranial Nerve X - Vagus clinical sign
Differential diagnoses for CN IX and X deficits
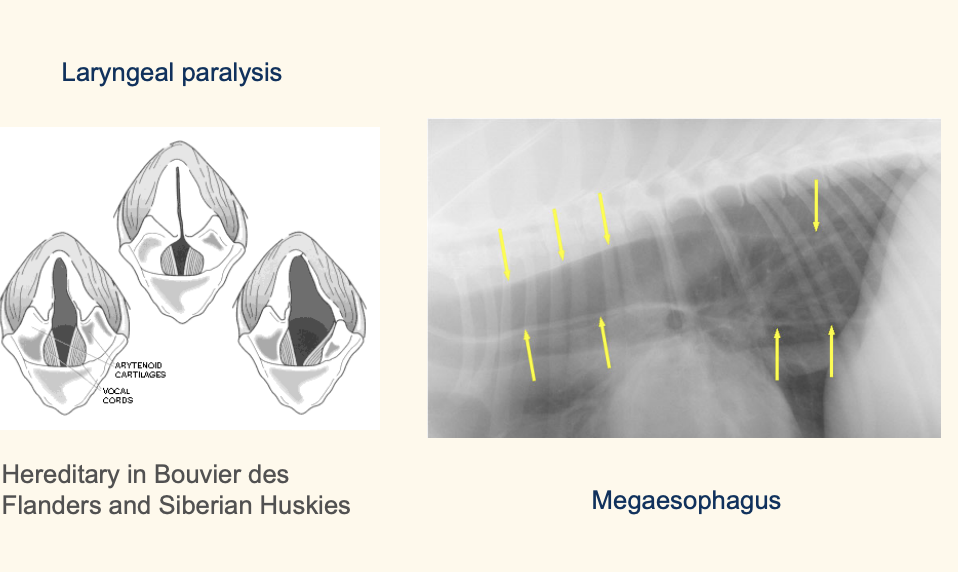
Degenerative: storage diseases. – Anomalous: congenital hereditary laryngeal paralysis in Bouvier des Flanders and Siberian Huskies. No treatment. – Metabolic: hypothyroidism (dog) – Neoplastic: brainstem tumors, paraneoplastic polyneuropathies. – Idiopathic: idiopathic laryngeal described in middleaged to older male large breed dogs = geriatric onset laryngeal paralysis polyneuropathy – Toxic: lead and organophosphate toxicity – Traumatic: post-surgical complication
add name
functionCranial nerve XI - Accessory
Motor – neck muscles (trapezius, sternocephalicus and brachiocephalicus) • Atrophy of neck muscles on palpation • Differential diagnoses - trauma
function of Cranial nerve XII – Hypoglossal
Motor – intrinsic and extrinsic muscles of the tongue
Deficits in tongue movements, atrophy, and deviation of the tongue (assymmetry)