Brainstem
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
Brainstem Stroke
• Knowing what we now know about spinal cord injuries, let’s imagine that our new patient has
actually had a rare brainstem stroke
• Because a lesion has occurred in a more caudal (or superior) location, we can imagine that damage
might be even greater compared to a spinal cord injury
• As we will learn though, the brainstem also houses structures necessary for important involuntary
functions
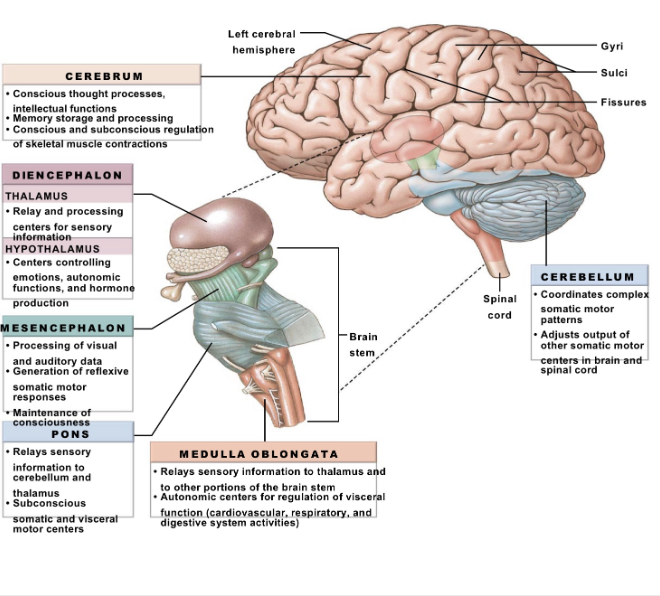
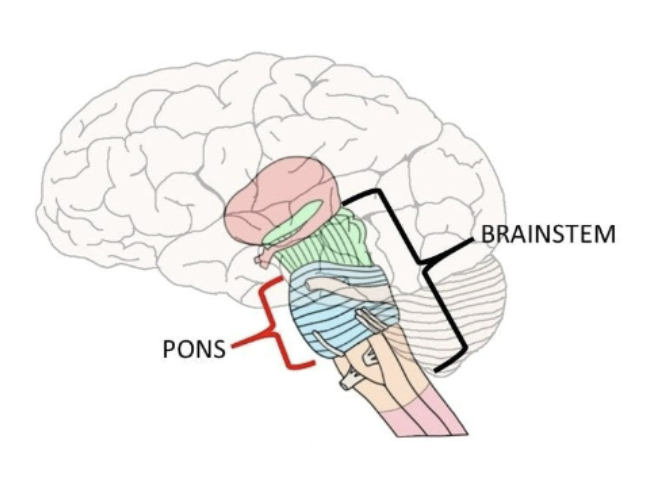
The Brainstem
• A required stop when transmitting signals
between the cerebrum and the spinal cord
• Located
• Inferior to the cerebrum
• Rostral to the spinal cord
• Anterior to the cerebellum
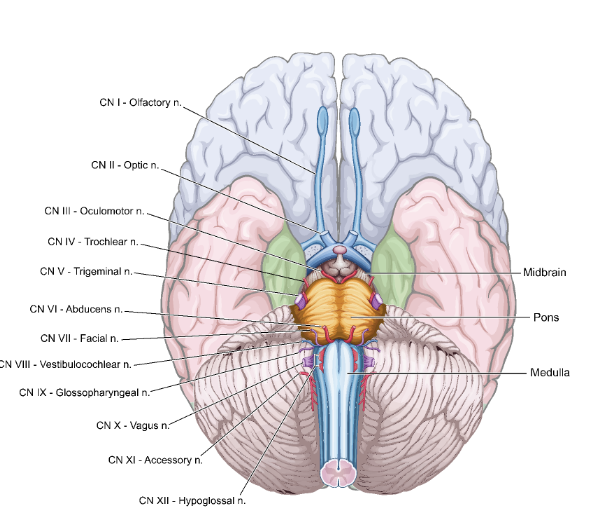
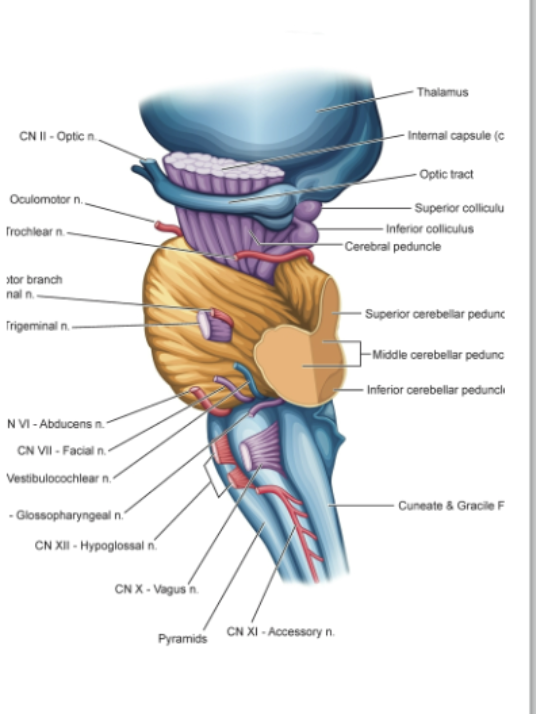
View of Ventral Brainstem and Cerebrum
• Although the structures of the brainstem look very
different, they transition into one another
• Can create difficulty in talking about structures independently
• Cranial nerves are also visible
Medulla
Importance:
• Critical center for cranial nerve
functions associated with:
• Sensory for hearing and balance (CN VIII)
• Swallowing and voice production (CN IX and CN X)
• Movement of the head (CN XI)
• Movement of the tongue (CN XII)
Nucleus is in the medulla
Reticular Formation
• A net-like formation of nuclei and neurons
• Stretches across various parts of the brainstem
• Includes ascending and descending tracts
• Involved in alertness, arousal, consciousness, and
sleep-wake cycles
• But speaking to the medullary reticular formation
• Autonomic control regulating blood flow and
heart rate
• One example of regulation is through the
baroreceptor reflex
Reticular
Formation
(cont.
• Medullary reticular
formation is also critical to
controlling respiration
• Part of the autonomic
regulatory system
• Based on feedback
regarding O2 and CO2
levels
• Integrates input from
the pons
Ascending
sensory
descending
motor
Damage to the
Reticular
Formation
• Among other concerns,
significant damage to the
reticular formation and the
ascending pathways from it
can lead to reduced
consciousness
• This may include hypersomnia,
coma, or death
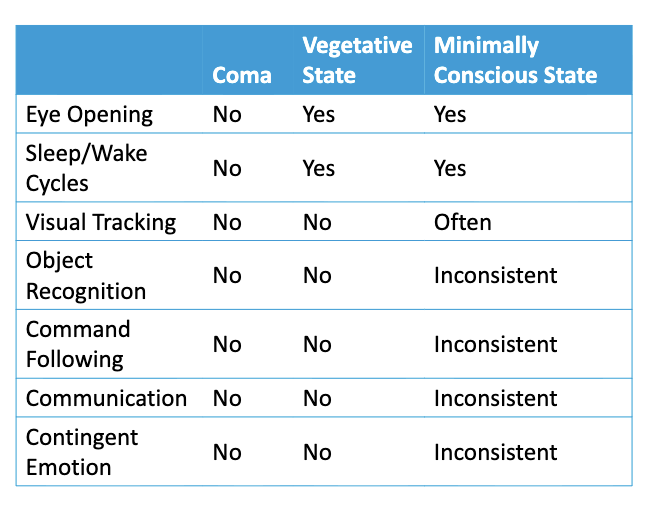
Potential
Outcomes
of a Coma
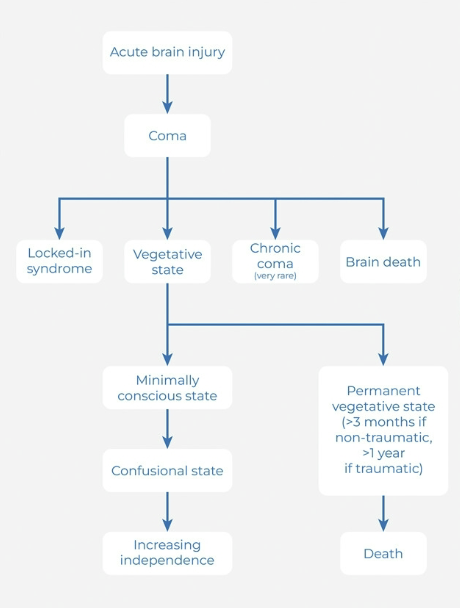
States of Recovery and Patterns
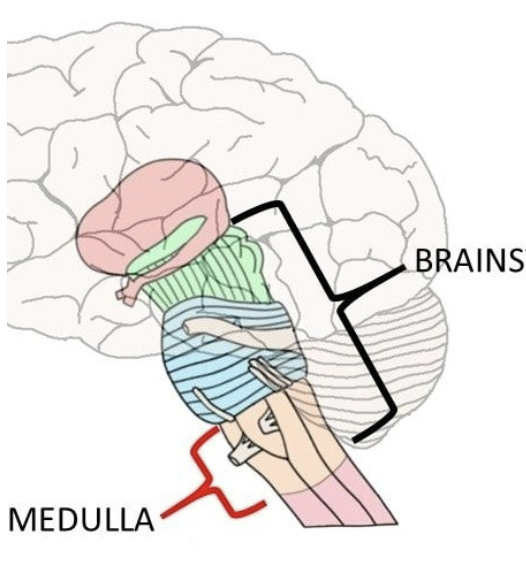
External Structures of the Medulla
• Highlighting the pyramids and
pyramidal decussation
• Pyramids contain axon fibers of the
Corticospinal and Corticobulbar Tracts
• Smooth-flat region two thirds of the
way down the medulla is the pyramidal
decussation of the corticospinal tract
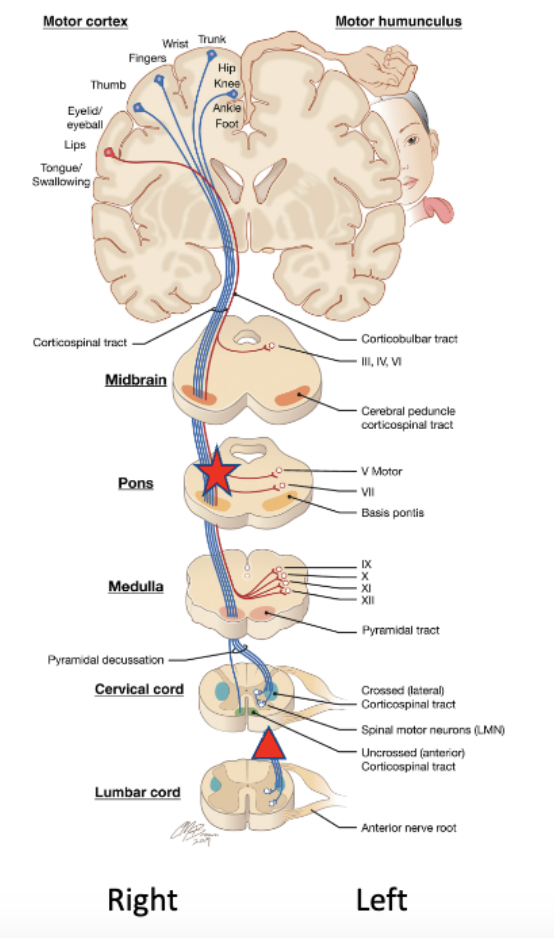
If there was damage approximately where
the star is, which side of the body (below the
neck) would be weak or paralyzed?
left side is damage before decuzation
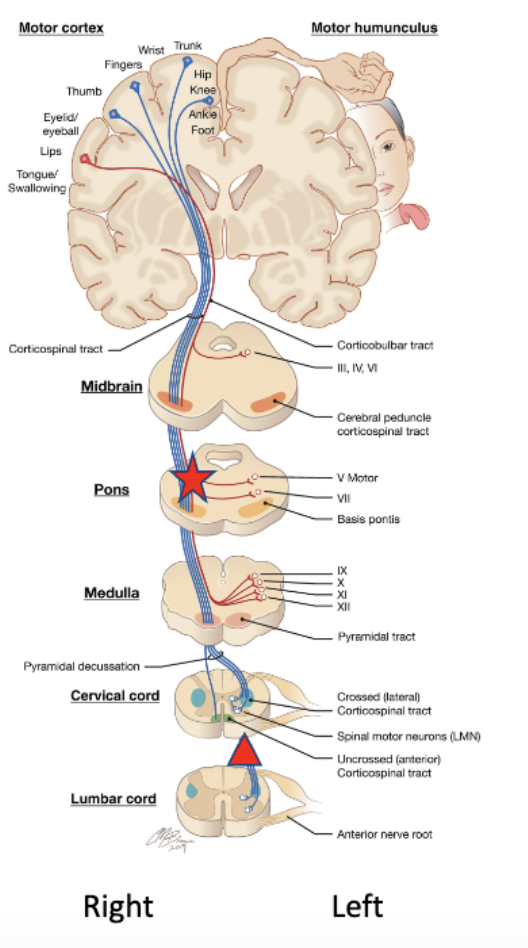
If there was damage approximately where
the triangle is, which side of the body (below
the neck) would be weak or paralyzed?
left post decuzation
Moving up to the
Pons
• Between the medulla and
mesencephalon
• Bounded posteriorly by the cerebellum
• Importance:
• Ascending and descending
pathways
• Major connector to the
cerebellum
• Critical center for cranial nerves
• Respiratory center functions
Pons: The Cerebellar Peduncles
• Axon pathways into and out of the cerebellum
• Divided into 3 zones:
• Inferior cerebellar peduncles (input)
• Middle cerebellar peduncles (input)
• Superior cerebellar peduncles (output)
• Necessary for motor control circuit
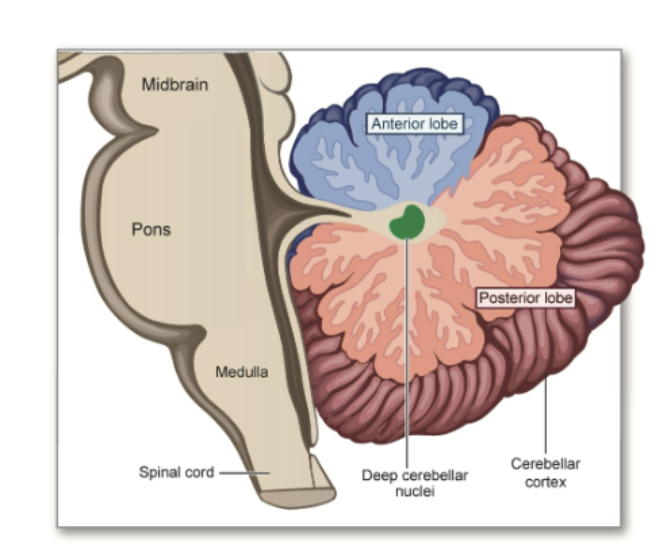
Quick Detour to the Cerebellum
• Regulates movement in an indirect way for motor learning and motor coordination
• Consists of two large lateral hemispheres
• Cerebellar hemispheres are divided into an anterior and posterior lobe
Friedrich’s Ataxia
genetic, don’t realize they have it
Pons
• Connection point for cranial nerves for:
• Control of facial muscles for speech (CN VII)
• Movement of the mandible (CN V)
• Sensory inputs to the skin, oral muscosa, and mandibular region (CN V)
• Pontine respiratory region
• Pneumotaxic center
• Apneustic center
Respiratory Inputs from the Pons
• Additional image for
respiratory centers (right)
• Able to momentarily stop
or modify respiration
• Needed for both:
• Voluntary behaviors
• Non-vital reflexive
behaviors
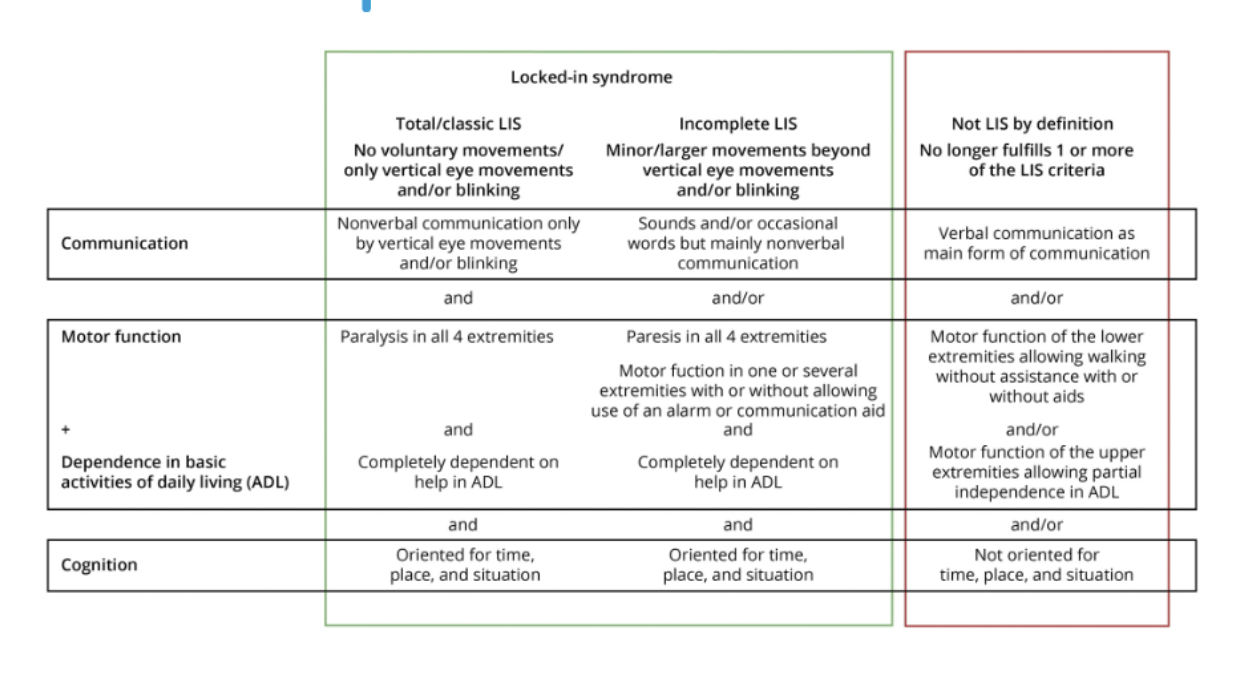
Damage to
Pons
• Potential impacts on facial sensation, facial movement,
eye movement and more via the cranial nerves
• In rare cases, can lead to locked-in syndrome
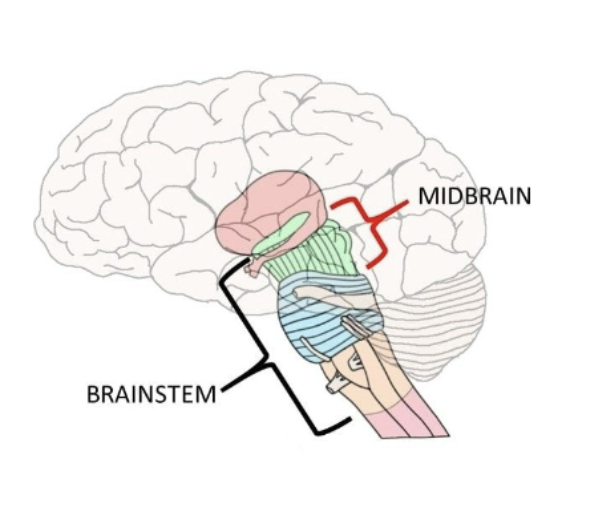
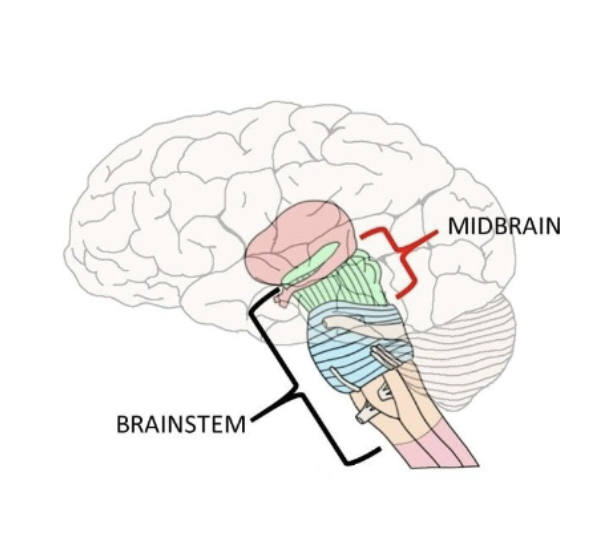
Mesencephalon
(Midbrain)
Uppermost segment of the
brainstem, with diencephalon
above (rostrally)
• Bounded posteriorly by the
cerebellum
Mesencephalon
• Importance:
• Ascending and descending
pathways
• Center for cranial nerves (albeit
ones less associated with
communication or swallowing)
• Gray matter structures
associated with the cerebellum
and basal ganglia
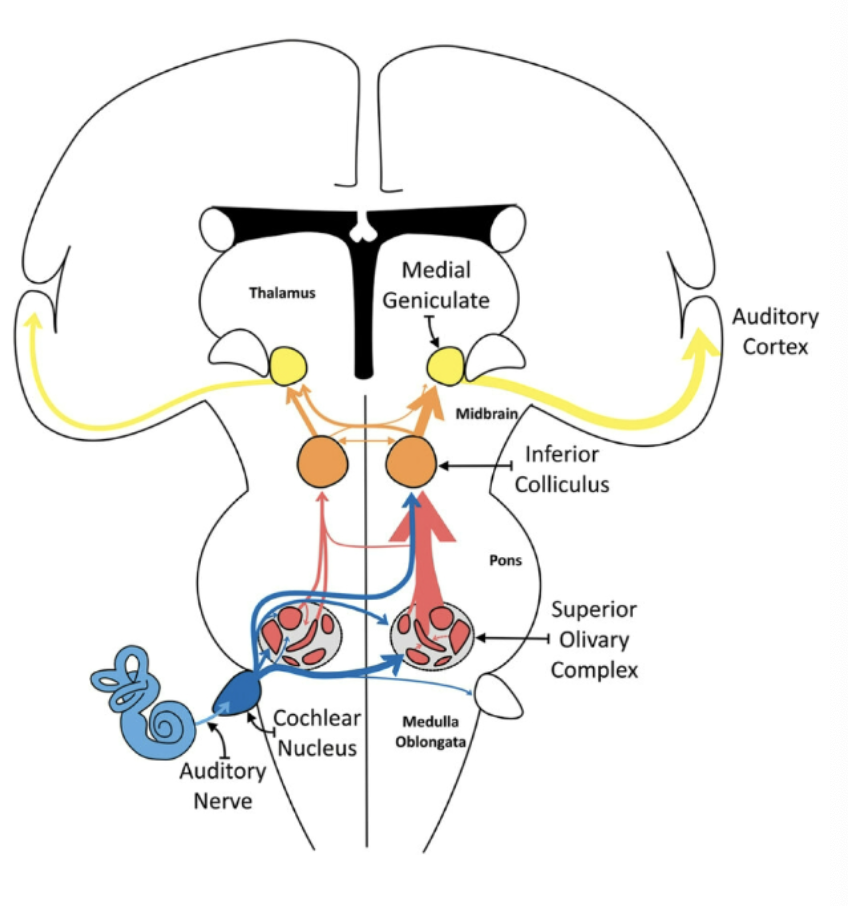
A Special Case
for Sensation
• Auditory pathways of
the brainstem and
beyond
• Damage to brainstem
areas can lead to
deafness or more
complex auditory
processing difficulties
Brainstem Stroke Symptoms

Pons - damage tissue to the pons part of the brainstem
Jane is a 29 year old female who was recently involved in a car accident. She is no longer able to use her facial muscles and therefore cannot express emotions. She needs to now use an AAC device as she is no longer able to verbally communicate. Her lower extremities have also been impacted therefore sign language is not able to be used. Where is the lesion?
Cranial Nerves
How many cranial nerves are there?
Twelve pairs of nerves
While considered part of the PNS, for 10 pairs of them, they’re really part of
the following system:
Nucleus within the brainstem (CNS) →Nerve (PNS) →Peripheral Target
(Motor)
Nucleus within the brainstem (CNS) →Nerve (PNS) →Peripheral Target
(Sensory)
Exceptions for Cranial Nerves I and II
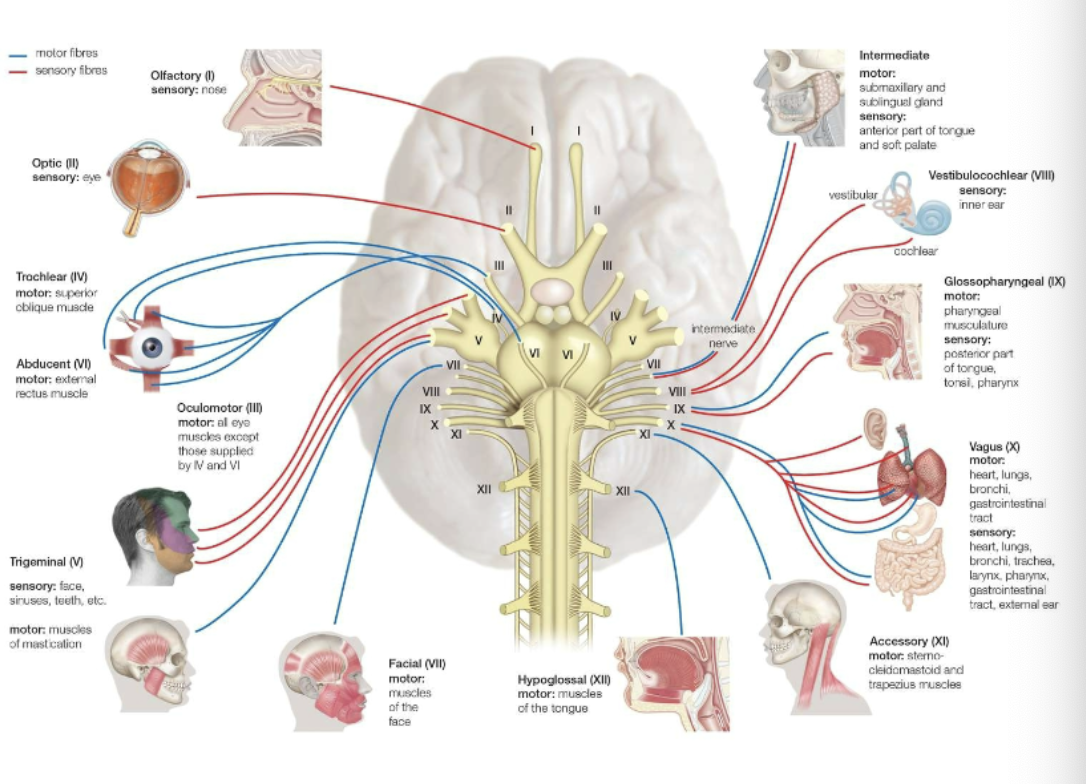
Cranial Nerves (Bolded specific for communication)
• Olfactory (CN I)
• Optic (CN II)
• Oculomotor (CN III)
• Trochlear (CN IV)
• Trigeminal (CN V)
• Abducens (CN VI)
• Facial (CN VII)
• Auditory-vestibular (CN VIII)
• Glossopharyngeal (CN IX)
• Vagus (CN X)
• Accessory (CN XI)
• Hypoglossal (CN XII)
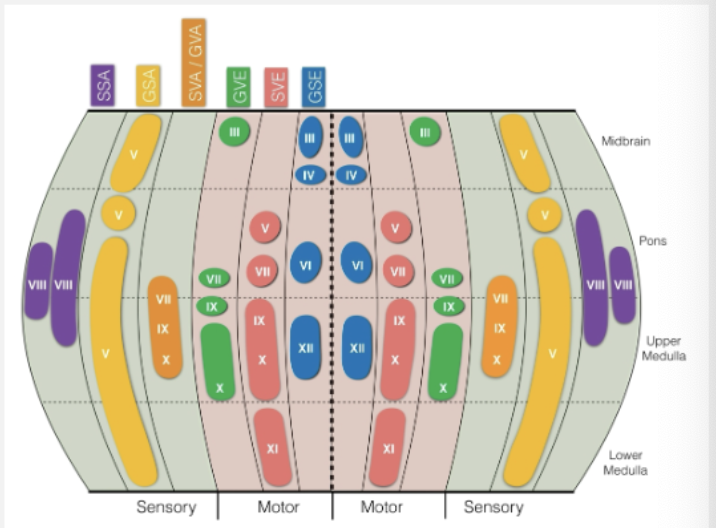
Flattened Perspective
of the Brainstem
Revealing CN Nuclei
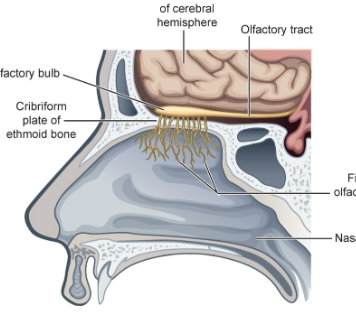
CN I – Olfactory
• Sensory: smell and discrimination of smell
• Links back to olfactory cortex and aspects of the temporal lobe
• Damage can lead to anosmia or hyposmia
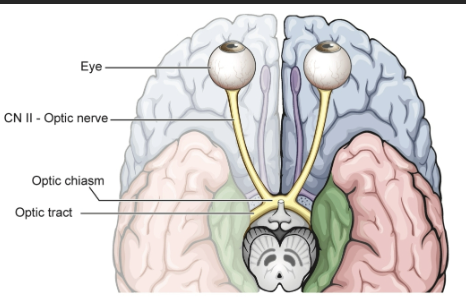
CN II – Optic
• Sensory: vision
• Links back to primary visual cortex in the occipital lobe
• Damage can lead to visual field losses corresponding to the site of injury
• Optic neuropathy
• Glaucoma
CN III – Oculomotor
• Motor: Inferior oblique; superior, inferior, and medial rectus; and pupillary reflex
• Only somewhat associated with eye closing
CN IV – Trochlear
• Motor: Superior oblique (allows for downward/inward movement)
CN VI – Abducens
Motor: Lateral rectus (allows for outward/lateral movement)
CN V – Trigeminal
• Mixed nerve
• 3 branches
• Ophthalmic (V1)
• Maxillary (V2)
• Mandibular (V3)
• Sensory: Somatosensation from facial skin and oral/nasal linings (including the tongue)
• Motor: Mandibular division for the masseter, temporalis, and pterygoid muscles
Damage to CN V – Trigeminal
• Trigeminal neuralgia
• Sharp, intense pain on one side of the face
• Weakness in muscles for chewing (shown on
right)
• Neuropathy: Reduced or atypical sensations of
the face
weakness means asymmetry
Assess sensation of face skin, bilaterally
• Using a wisp of cotton, lightly touch face within all skin territories of V1, V2, &
V3, bilaterally
• Cranial Nerve V: Sensory (Typical)
• Cranial Nerve V: Sensory (Atypical
Test Motor Component of V
• Palpate master and temporalis while lightly clenching teeth
• Also, checking for deviation
• Cranial Nerve V: Motor (Typical)
• Cranial Nerve V: Motor (Atypical