PATHO FINALS CUMULATIVE STUDY GUIDE
1/201
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
202 Terms
what is pathophysiology and what factors does it contain?
study of abnormal changes in body that are the cause of disease process
contains: etiology, pathogenesis, manifestations, treatment
what is etiology and what are the classifications and its meaning?
study of cause
idiopathic: cause unknown
iatrogenic: cause relating to unwanted treatment (i.e. chemo)
congenital
infectious
multifactorial
what is pathogenesis?
development/evolution of disease
sign and symptom, which is subjective and which is objective?
sign: objective (something that is observed)
symptom: subjective (feeling of abnormality)
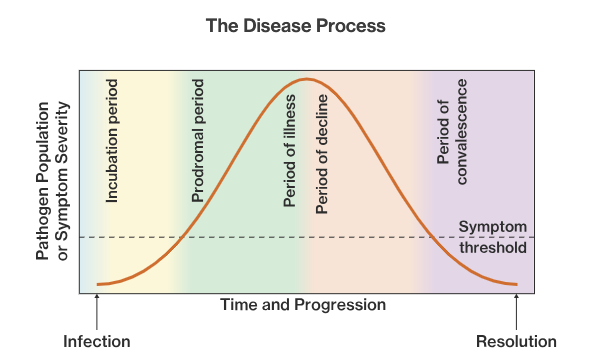
what are the stages of diseases?
exposure
latent period
prodromal period
illness
decline
convalescence
what is reliability when it comes to diagnostic assessments?
what is validity? what is predictive value?
reliability: test’s ability to give same result repeatedly
validity: test’s ability to reflect on true value intended
predictive value: test’s ability to differentiate between presence/absence of person’s condition (i.e. pregnancy test)
sensitivity: true + rate
specificity: true - rate
what is epidemiology and what are the types?
study of patterns of disease involving populations
type:
endemic (particular region - low spread)
epidemic (spread rapid thru large population)
pandemic (worldwide)
what are the levels of prevention?
primary (health & risk promotion) (i.e. vaccinations)
secondary (screening of risk of individual - early prevention)
tertiary (rehab, prevention of complication, improve quality of life)
describe the terms below:
homeostasis
allostasis
stress
stressors
distress
allostatic overload
state in which body system is in balance at ideal
ability to adapt to challenges (body undergoes adjustments to establish homeostasis)
tension of body/mind
agents that produce stress and endanger homeostasis
inability to cope w/ stressors
inadequate adaptation that lead to disease/death
what is general adaptation syndrome (GAS) and what are the stages?
stage that describes physiological changes body goes through when under stress
stages:
alarm reaction: fight or flight response due to stressful stimulus
resistance (adaptation): increase activity of nervous system and return to homeostasis
exhaustion: body can no longer return to homeostasis
what hormones do the body releases in respond to stress? what are there physiological effects of each hormone?
catecholamines:
norepinephrine: constrict blood vessel & raise BP
epinephrine: enhance muscle contractility
adrenocortical steroids:
cortisol: stress hormone (anti-inflammatory, energy burst)
aldosterone: promote absorption of sodium and water in kidney
endorphins:
oxytocin: produces during childbirth/sex/lactation (calming effect)
cytokines: secreted during stress response
what organs are affected during stress?
Stress generally affects all systems of the body including cardiovascular, respiratory, endocrine, gastrointestinal, nervous, muscular, and reproductive systems
what do these terms mean?
perfusion
ischemia
hypoxia
delivery of oxygen and nutrients
reduce blood flow (leads to hypoxia) (injures cells faster due to metabolic waste)
low levels of O2 in tissue (results from ischemia) (cause power failure in cell)
what is the cause(s) of cellular injury?
most common is ischemia
other causes:
hypoxia
nutrition
infections
chemical injuries
physical injuries
radiation injuries
what are some reversible cell injuries?
hydrophic swelling, intracellular cell injury, cellular adaptation
what are some irreversible cell injuries?
necrosis, apoptosis, cellular aging
what is hydropic swelling?
intracellular edema
what is intracellular cell injury and what are some example?
excess accumulation of substance in cell (fat, glucose, protein)
examples: fatty liver, gaucher disease, pigment
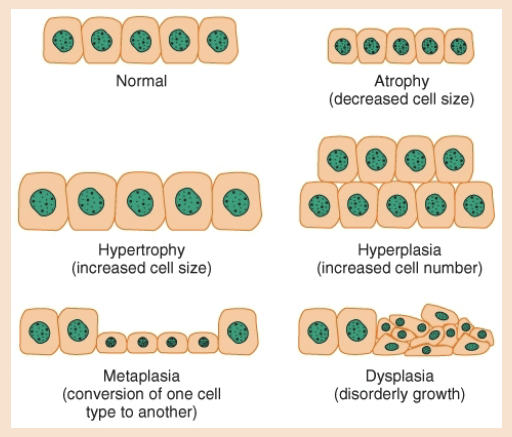
what is cellular adaptation and what are the different types?
definition: cells adapting to ongoing stressors
types:
atrophy: cells shrink and functionality reduces
hypertrophy: cell mass increase and augments functionality (takes up space)
hyperplasia: increase in functional capacity r/t increase cell number (i.e. callus)
metaplasia: conversion of one cell type to another
dysplasia: disorganized appearance of cell
what are the 4 types of necrosis?
what is gangrene? (describe what dry, wet, gas gangrene are)
what does gangrene result from?
4 types:
coagulative
liquefactive
fat necrosis
caseous necrosis
gangrene: necrosis in large area of tissue which results from ischemia
dry: formation of coagulative necrosis (dry, black, wrinkled)
wet: liquefactive necrosis (internal organs and can be fatal?
gas: from infection of necrosis by bacteria (bubble)
what is apoptosis and what can trigger it?
definition: type of cell death (normal for cell growth and no inflammation)
triggers:
withdrawal of survival that suppresses apoptotic pathway
extracellular signal that bind to cell and trigger death cascade
intrinsic pathway: sever cell damage leads to increase in protein which can cause own cell death
what is the cause of cellular aging?
what are theories about cellular aging?
cause: decline in proliferation and exposure to damaging environmental and metabolic factors
theories:
DNA damage accumulates overtime
stem cell decline
free radical theory (accumulated cell damage)
programmed senescence theory (finite # of cellular replication)
what is somatic death? general features of it? what enzyme is released during somatic death?
definition: death of entire organism
features: cessation of respiration and heartbeat, stiffened muscle due to calcium in body (riggor 0-6hrs, flaccid 24-48hr)
enzyme: lytic enzyme in body tissues
Which type of irreversible cell injury initiates an
inflammatory response?
A. Apoptosis
B. Necrosis
C. Hydropic swelling
D. Intracellular accumulations
B. Necrosis
what are the layers of the skin and the function of the skin?
layer: epidermis, dermis, hypodermis
function:
protective barrier for internal organs
regulate temperature
sense change in temp., pressure, pain
excrete fluid and electrolytes
store fat
synthesizes vitamin D
provide site of drug absorption
what are the age related changes when it comes to the integumentary (skin)?
epidermis thins
cell reproduce more slowly
dermis less elastic (decrease elastin)
decrease SQ fat
hair loss (thinning in males)
loss of melanocytes (hair is grey/white)
dull, brittle, hard, thick nails
increase longitudinal striations that cause splitting in nails
decrease sebum secretion and sebaceous glands
protective function, sensory nerves, blood vessels decline
skin easily injured and heals slowly
what are the types of skin lesions?
macule: flat discolored
patch: elevated pimple like bump
papule: elevated solid (1cm)
plaque: plateu-like, elevated, <1cm
vesicle: small fluid filled blister
bulla: big fluid filled blister
pustule: small pus filled
what do these terms mean?
excoriation
lichenification
scar
repetitive itching of skin leading to lesion
skin becomes thick and leathery
left over mark thats not completely healed
what are the distributions of skin lesions?
diffuse
localized
discrete (separate; not joined)
confluent (multiple small macules/papules that forms patches in net-like pattern)
linear
what are some infectious and bacterial skin conditions? (explain each one and treatments for it)
impetigo (staphylococci): starts as red itchy sore and heals as crusty honey colored scab
Tx: antibiotic (mupirocin)
syphilis: primary stage on tongue then moves to palms and rash on back
Tx: IM antibiotic (penicillin)
cutaneous abscess: break in skin
Tx: drainage & oral antibiotic
what are some infectious and viral skin conditions? (explain each one and treatments for it)
verrucae: warts caused by human papillomavirus
herpes simplex: virus causing contagious sores
Tx: antiviral for severity & recurrence
chicken pox: contagious itchy blister like rash on skin
Tx: childhood vaccine
herpes zoster: also known as shingles and those w chicken pox can develop this
Tx: vaccine and antiviral
what are some infectious and fungal skin conditions? (explain each one and treatments for it)
tinea corporis (neck, arms, legs)
tinea cruris (groin)
tinea pedis (foot)
tinea unguis (toenail, fingernail)
Tx: topical anti-fungal (clotrimazole)
what are some examples of skin preparation drugs?
isopropyl alcohol, iodine (betanide), chlorhexidine
what are some topical antipruritic drugs?
antihistamines
corticosteroids
what is pressure injury?
what are the risk, cause, and stages?
what are the treatments, prevention, and what tool used to assess risk?
definition: localized areas of necrosis resulting from ischemia r/t prolonged pressure
risk: poor nutrition, aging, immobility, sensory loss, incontinence
cause: pressure overtime, shear/friction, moisture, poor nutrition, poor circulation
stages:
stage 1: non-blanchable eythema
stage 2: partial thickness loss
stage 3: full thickness loss
stage 4: full thickness loss (able to see muscle, tendon, bone, cartilage)
unstageable: eschar (black) w/ slough (yellow) (undermining and tunneling present)
deep tissue injury: maroon/purple discoloration with either skin intact or not
Tx: skin dry & clean, fluid & protein, vitamin supplement, avoid infection
prevention: reposition, area clean, bed linen clean & no wrinkle, pillow
tool: braden scale (sensory perception, activity, mobility, moisture, nutrition, friction/shear)
what are some wound care medications and explain each one? what are the adverse effects of each?
vitamin C, zinc, topical such as:
dakin’s solution: bleach + baking soda that treat & prevent tissue infection
adverse effects: redness, irritation, pain, swelling of treated skin
cadexomer iodine: clean wound and promote healing; remove slough & debris
adverse effect: allergic reaction
collagenase: debriding agent; remove necrotic tissue (may increase risk of serious infection)
adverse effect: pain, burning, redness, irritation
medihoney: clean & promote healing; reduce inflammation; promote moist environment and protective barrier
adverse effect: none
silvadine: treat/prevent burn
adverse effect: pain, burning, itch
everything about the bone:
how many are there?
whats it’s function?
shapes and classification?
components?
what hormones influences bone growth?
what does absence of bone stress lead to?
how does modeling/remodeling happen? (sequence)
206
storage, protection, stability, stem cells
long, short, flat, irregular, sesamoid
mineral (Ca & phosphorus), water, fibrocytes, osteocytes
calcitonin, PTH, estrogen
demineralization
hematoma form → fibrocartilage form → callous form → ossification → remodel
what is wolff’s law?
bone in healthy person will adapt to the loads of work under which it’s placed (load bearing activity activates osteoblasts which increases bone density and lack of activity decrease is)
what are the three connective tissues and explain?
how does the joint respond to injury/stress?
cartilage (ends of bones - cushion)
tendons (muscle to one - flex)
ligaments (bone to bone - stabilize)
joints (point of contact between bones; responds to stress by cartilage becoming thin and surface irregular/rough and lead to swelling of joint cavity and lead to pain/stiffness)
what are the changes in older adults regarding the muscular system?
size and number of muscle mass decrease
muscle less responsive to neurotransmitters and hormones
decrease muscle strength and endurance
what are the changes in older adults regarding the skeletal system?
bone breakdown
synovial fluid thickens
bone mass decrease
kyphosis
narrowing of disk space (decrease height)
what are s/s and tx of muscle and connective tissue injuries?
explain for each (cartilage, ligament, muscle)
cartilage
s/s: pain, swelling, crepitus, stiff, locking
tx: NSAIDs, surgery, glucosamine
ligament
s/s: “snap,” pain, limited ROM, wt. bearing intolerance
tx: brace, RICE, NSAIDs, PT, surgery
muscle
s/s: pain, erythema, limited ROM, spasm, swell, weakness
tx: RICE, NSAIDs
what are the types of fractures?
nondisplaced (remain at alignment)
displaced (fracture separate and unaligned)
simple (skin not broken)
compound (skin broken)
transverse (straight line)
spiral (twisting motion)
longitudinal (along axis)
oblique (angle)
depressed (below level of bone surface)
comminuted (fracture line + fragment)
impacted (drives fragments to each other)
complete (clean break)
incomplete (break crack - “greenstick”)
pelvic fx (heal w/o complications; shortening ht., weak difficulty, pain sitting down)
what are some interventions, procedures, and assessment done w bone injuries?
interventions: ice & elevate, immobilize, meds., surgery
procedure: internal fixation, external fixation, bone graft (auto-: self, allo-: deceased, xeno-: non-human, synthetic)
circulation assessment: pain, pulse, pallor, paresthesia, paralysis
carpel tunnel
(definition, s/s, and tx)
narrow passageway of ligaments and bone surrounding median nerve at base of hand
s/s: weakness, pain, burn, numb, tingle (worst at AM & PM)
tx: rest, NSAIDS, steroids, surgery
compartment syndrome
(definition, s/s, and tx)
soft tissue injury and swelling due to compartment size decrease
tx: reduce pressure and swelling, surgery
DVT
(definition, s/s, and tx)
blood clot forming within large vessel r/t decrease circulation
s/s: erythema, edema
tx: anticoagulants (heparin & warfarin), thrombectomy, greenfield filter
pulmonary embolism
(definition, s/s, and tx)
foreign substance obstructing circulation in lung tissue
s/s: chest pain, hypoxemia, tachycardia
tx: ventilatory support, anticoag. (heparin), greenfield filter
fat emboli
(definition, s/s, and tx)
fat particles release into blood stream and lodge in lungs
s/s: shortness of breath, tachypnea, rash, altered mental status
tx: ventilatory support
osetomyelitis
(definition, s/s, and tx)
infection of bone
s/s: acute pain in bone, tender, heat, swell, erythema, fever, chills, drainage
tx: long term antibiotic, surgery
osetoporosis
(definition, s/s, and tx)
metabolic disease of skeleton where rate of resorption is greater than bone formation
s/s: short ht., muscle waste, back muscle spasm, difficulty bending over, humpback
tx: exercise, heat, calcium and vit. D supplement, bisphosphonate, PTH
paget’s disease
(definition, s/s, and tx)
idiopathic dysfunctional bone formation
s/s: pain, fracture, headaches, kyphosis, deafness, misshapen bone, increase ALP level
tx: bisphosphonate, calcitonin, monitor ALP
osteomalacia
(definition, s/s, and tx)
bone growth due to vitamin deficiency due to lack of building materials
s/s: bone pain, fracture, muscle weakness, low Ca
tx: vit. D, phosphate, calcium supplements
what is rheumatism?
disease marked by inflammation
osteoarthritis
(definition, s/s, tx)
joint disorder associated w aging wear and tear from repetitive stress
s/s: crepitus w/ movement, bony enlargement, spurs, coolness, DIP & PIP nodes
tx: PT, wt. reduction, NSAID, corticosteroids, assistive device
rheumatoid arthritis
(definition, labs, s/s, tx)
autoimmune inflammatory disease that lead to immune cells and production of antibody RF and infiltration of synovium
labs: RF present, ESR & WBC elevated
s/s: pain improves w/ activity, warm erythema, malaise, fatigue, sjogren syndrome
tx: NSAID, corticosteroids, DMARD, TNF, surgery
lupus (SLE)
(definition, labs, s/s, tx)
inflammatory autoimmune disorder of connective tissue (immune injury to basement membrane)
labs: elevated ANA & ESR, decrease C3, C4, WBC, PLT and anemia
s/s: butterfly rash, photophobia, renal insufficiency
tx: NSAIDs, immunosuppresents, antimalarials, methotrexate, glucorticoids
scleroderma
(definition, labs, s/s, tx)
inflammatory connective tissue disease which affects skin, blood vessel, synovium, organ
labs: ANA elevation
s/s: polyarthritis in small joints, edema of finger/hand/feet, limited ROM, CREST, atrophy
tx: vasodilator, anatcids, PPI, ACE inhibitor, prostaglandins
ankylosing spondylitis
(definition, s/s, tx)
fusion of inflamed vertebrae
s/s: low back pain relieved w/ activity, severe s/s upon waking, limited ROM in lower back
tx: stretching, ROM exercise, NSAIDS, corticosteroids, methotrexate, joint replacement
psoriatic arthritis
(definition, s/s, tx, five types)
inflammatory autoimmune disease
s/s: patches of thick red skin covered by white/silver scales, stiffness
tx: corticosteroids, NSAID, immunosuppressants, TNF
five types:
symmetric (all joints)
asymmetric (not all joints)
distal (ends of fingers/toes)
spondylitis (spine and neck)
mutilans (severe deformities of small joints in fingers and toes)
gout
(definition, cause, phases, s/s, tx)
limited excretion of uric acid by kidneys (urate acids buildup in blood stream and deposit in joints)
cause: genetic, renal insufficiency, diet high in purine
phases:
asymptomatic
gouty arthritis
complicated arthritis
tophaceous arthritis
s/s: warm, erythema, tender
tx: may resolve within 10-14 days, elevate, immobilize, cold pack, colchicine
fibromyalgia
(definition, s/s, tx)
chronic widespread muscle stiffness, fatigue, and tender point pain that lasts 3months (idiopathic & no diagnostic)
s/s: pain, tenderness, muscle fatigue, stiffness
tx: exercise, duloxetine, milnacipren, pregabalin, gabapentin
lyme disease
(definition, s/s, tx)
caused by borrelia burgorferri bacteria carried by deer tick
s/s: flulike symptom, erythema migrans (rash at site), stiff neck, arthritis, nerve pain, facial palsy
tx: oral or IV antibiotic
rheumatic fever
(definition, s/s, tx)
group A streptococcal infection
s/s: fever, polyarthritis, muscle spasm, eythema, carditis
tx: antibiotic, NSAID, corticosteroids
what are the mechanism of action of NSAIDs
inhibit leukotriene and prostaglandin and blocks chemical activity of enzyme COX that cause inflammatory response
hemostasis:
what is it?
what does it involve? (organs)
what essentials elements are involved?
whats the process?
what are the stages?
arrest of bleeding/prevention of blood loss after blood vessel injury (body allows blood flow while repairing the wall)
vessel wall, circulating PLTs, plasma protein, liver, bone marrow, kidney
calcium and vitamin K
injury → vascular spasm → PLT formation → coagulation
primary, secondary, and final stage
explain the stages of hemostasis (primary, secondary, final stage)
primary: exposure to collagen → vasoconstrictions to minimize blood loss → release of TF → PLT activate → forms PLT plug
secondary: clotting factor activates → forms insoluble fibrin strands
final: clot retraction → tissue buildups → plasmin activates to dissolve clot (increase of thrombin levels → ingests fibrin → dissolve)
what are the two components of blood?
PLT and insoluble fibrin strands
whats the role of TF and vWF?
TF: activates due to exposed blood/disruption in vessel wall
vWF: released due to injury to blood vessel and joins PLTs together and promote production of clotting factors
Platelets:
where is it produced?
function/role?
how much in % in circulation?
whats the normal levels?
resting vs activated (explain the difference of state of PLT during rest and activation)
bone marrow
self adhere in presence of vWF and form mechanical plug
75% in circulation and 25% stored in spleen and liver
150,000 - 400,000
resting: spends more time free floating in resting state
activated: process: adhesion (PLT - vessel wall) → aggregation (PLT - PLT) → degranulation
what organ produces coagulation factors?
liver and majority are in inactive form
what drives the coagulation cascade? what are the two pathways?
clotting factors secreted by liver, PLT, endothelium
pathways:
intrinsic: initiated by exposed collagen
extrinsic: initiated by release of TF
bleeding:
what are the sources of active bleeding
what are some nursing considerations?
arteries: spurting & bright red
veins: steady flow & dark red
capillaries: slow even flow
education (any activities that causes bleeding), fall prevention, avoid IM injections, avoid prolonged constrictive item, and manual BP
what are the lab findings and their normal range?
CBC: identify anemia (RBC, WBC, HCT, HGB)
PLT: # of PLTs (15-40)
PT/INR: extrinsic pathway (10-14)
PTT: intrinsic pathway (33-45)
Fibrinogen: common pathway (200-400)
FDP: (<3)
D-Dimer: fibrinolysis (<200)
thromboctopenia
(define, lab values, tx)
lack of PLT caused by inadequate PLT production, hyperactive PLT destruction, dilution (low PLT to circulating volume), excessive splenic pooling
lab values: low PLT, normal PTT, PT/INR
Tx: antimicrobials, splenectomy, PLT transfusion
hemophilia
(define, lab values, tx)
blood does not clot properly due to decrease ability to form fibrin strands
lab values: elevated PTT, normal PLT, PT/INR
Tx: factor VIII/IX replacement, frozen plasma (FFP), cryo 1
vonwillebrand disease
(define, lab values, tx)
lack of vWF (PLT won’t be sticky w/o vWF) and impacts primary hemostasis
lab values: elevated PTT, normal PT/INR, PLT
Tx: DDAVP & cryo
vitamin K deficiency
(define, lab values, tx)
needed for liver to synthesize coagulation factors
lab values: elevated PT/INR, normal PLT, PTT
Tx: vit. K replacement, FFP
Disseminated intravascular coagulation (DIC)
(define, lab values, tx)
abnormal clotting and bleeding
lab values: elevated PT/INR, PTT, FDP/FSP & low PLT
Tx: transfuse FFP, cryo, PLT and anticoagulants
liver disease
(define, lab values, tx)
large number of clotting factor produced in liver
lab values: elevated PTT, PT/INR and low PLT
Tx: Vit k supplement and transfuse FFP, PLT, cryo
thrombosis
definition
what can it lead to?
what is the cause?
blood clot reduces blood flow through affected vessel
ischemia, necrosis, MI, PE, ATN
Virchow’s triad:
abnormal blood flow
hyper coagulability
injury to vessel wall (needle that exposes collagen which activates PLT and clot formation happens)
catheter thrombosis
(definition, s/s, tx)
thrombosis due to catheter
s/s: sluggish flow of catheter, edema, erythema, tender, increase WBC
tx: remove line, tPA
atherosclerosis
(definition, tx, risk)
artery stiffens and narrows due to buildup of plaque
tx: diet, exercise, control HTN & cholesterol, ASA, Plavix
risk: stroke and heart attack
acute coronary syndrome
(definition, s/s, tx)
blockage and narrowing coronary vessel that reduce blood flow
s/s: angina, jaw pain, diaphoresis, anxiety, ECG changes, sudden cardiac death
tx: vasodilator, ASA, plavix, anticoag., tPA, bypass graft, cardiac cath
ischemic stroke
(definition, tx, sign)
impairment of cerebral circulation in one or more blood vessel supporting the brain
tx: tPA, TNK, embolectomy
signs: B.E.F.A.S.T. (balance, eyes, face, arms, speech, time)
what is the difference between ischemic and hemorrhagic?
ischemic: blood clot blocks blood flow
hemorrhagic: artery rupture and causes bleeding around brain
atrial fibrillation
(definition, what can it lead to, tx)
absence of coordinated and rhythmic atrial contractions
leads to: stasis of blood and clot formation
tx: ablation, MAZE, peacemaker, anticoags., antirrhythmics
what is hematopoiesis?
what are the two stages?
formation of blood cellular components
stages: proliferation and maturation (RBC, PLT, WBC)
RBC
function
lifespan
manufactured where?
made up of what?
deliver O2 to tissues via hemoglobin chain
120 days
bone marrow by stem cells
hemoglobin
erythropoiesis
define
how is it stimulated?
what does it require?
stages
process of production of RBC
decrease in O2 which is detected by kidneys which release erythropoietin
Vit. B12, iron, folic acid
stage:
kidney secrete erythropoietin
pro erythroblast into erythroblast (huge nucleus)
turns into normoblast (nucleus shrinks)
reticulocyte (nucleus ejected & matures)
RBC demise, what is it?
spleen removes old/ages/dead RBC and broken down into iron and bilirubin which then recycled to make new RBC (stored in liver) or secreted as waste
anemia
define
insufficient production of what?
what does it lead to?
s/s?
lack of mature healthy RBC (insufficient delivery of O2)
iron, folic acid, B12
increase O2 demand
fatigue, tachycardia, hypotension, pallor, lightheadedness, enlarged spleen
iron deficiency anemia
(define, s/s, tx)
lack of iron and leads to small RBCs that are unable to carry O2
s/s: s/s of anemia, PICA, koilonchychias, blue sclera
tx: diet (citrus but no tea since it can impair iron absorption)
folic acid anemia
(define, s/s, tx)
lack of folic acid crucial to proper brain function and fetal development
s/s: depression, forgetfulness, ulceration of cheek and tongue, fissure on mouth
tx: folate supplement
vitamin B12 anemia
(define, s/s, tx)
lack of B12 where RBC can’t synthesize and lead to large RBC with poor O2 carrying capacity
s/s: brain fog, mood swing, muscle weakness, depression, dementia
tx: B12 supplement
aplastic anemia
(define, s/s, tx)
lack of healthy material in bone marrow caused by toxic/radiant injury
s/s: low PLT and WBC
tx: blood transfusion, bone marrow transplant
chronic renal failure
(define, s/s, tx)
impaired renal endocrine function resulting in decreased erythropoietin production
s/s: low EPO, general s/s of anemia
tx: epogen or aranesp
hemorrhagic anemia
(define, acute vs chronic, s/s, tx)
lack of total circulating blood volume
acute: large volume in short amount of time
chronic: short volume in long amount of time
s/s: low RBC, HGB/HCT
tx: transfusion
hemolyctic anemia
(define, s/s, tx)
RBC are being destroyed faster than they are replaced
s/s: low RBX, HGB/HCT, jaundice, splenomegaly, dark/red blood urine
tx: transfusion
sickle cell anemia
(define, s/s, tx)
misshaped RBC leading to RBC destruction
s/s: jaundice, splenomegaly, stunted growth
tx: voxelotor, hyrocyurea, folic acid supplement, bone marrow transplant, gene therapy