J CM ER
1/135
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
136 Terms
#1 cause of burns
hot drinks

1st degree burn (superficial thickness) sx*
epidermis only
red burns that BLANCH, NO blisters
erythema, minor pain

tx of 1st degree burn*
aloe
benzocaine
pain = ibuprofen/acetaminophen

2nd degree burn (superficial partial thickness) burn findings*
superficial (papillary) dermis
blisters b/w epidermis and dermis that BLANCH with pressure, looks WET
clear fluid, pain, moist + weep

2nd degree burn (superficial partial thickness) tx*
drain large, floppy blisters
bacitracin/silvadene
sterile vaseline gauze
± topical anesthetic, ibuprofen, acetaminaphen

2nd degree burn (deep partial thickness) findings*
deep (reticular) dermis
easily unroofed blisters that do NOT blanch w pressure, WAXY appearance, DEC pain, hemorrhagic blisters
be concerned with hypothermia, water/electrolyte loss, infx

2nd degree burn (deep partial thickness) tx*
opioids
ibuprofen = anti-inflamm
tetanus prophylaxis

3rd degree burn (full thickness) findings*
dermis/muscle/bone (destroys dermis entirely)
waxy white/leathery gray, insensate**, hard eschar, charring

3rd degree burn (full thickness) tx*
cover w sterile vaseline gauze
skin grafting
biobrane/pig skin
narcotics/ketamine/sedatives/ibuprofen
tetanus prophylaxis
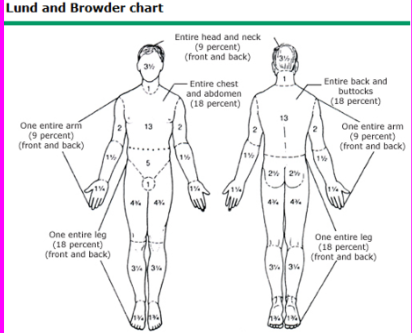
rule of 9’s (adult Lund and Browder chart)*
Head + neck = 9%
Chest + abdomen = 18%
Back + butt = 18%
1 entire arm = 9%
1 entire leg = 18%
special concerns for a burn victim*
any burn to face/hands/feet/genitalia/circum burn
3rd degree or full thickness burns that covers large area
any burn that interferes w respiration
any burn to infant/elderly
any chemical/electrical burn (alkali** more caustic > acid)
why is circumferential burn a concern?
the healing process → compartment syndrome/compress on that body part (tourniquet)
sx that a burn is evidence of abuse*
pattern burns that suggest contact w/ object
cigarette burns
stocking/glove/circum burn
burns to genitalia/perineum
major factors involved in severity of electrical burn*
AMOUNT of shocking current through body
DURATION
PATH
immediate death with burns is the result of?*
coexisting trauma
airway compromise
NOT THE BURN ITSELF
remember to remove the person from the source of burn!
signs of inhalation injury*
carbonaceous sputum
singed facial / nasal hairs
facial burns
oropharyngeal edema
changes in voice
altered mental status
initial management of burns
ABC
stop burn process (remove clothing, cool tissures)
irrigate chemical burns for 15 mins
circumferential full thickness burns require escharotomy
AMPLE = allergies, meds, PMH, last meal, events leading to injury
IV access, labs, foley, abx, wound care, pain control
3 RF for death (with burns)*
>60 yo
more than 40% BSA burned
inhalation injury
ARDS
edema from leaky capillaries from traumatized lung
(inhalation injury)
what burn pts hospitalized vs. goes home?
admission:
full thickness (3rd degree) >5% BSA
partial thickness (2nd degree) >10% BSA
any full thickness/partial thickness around critical areas (face, hands, feet, genitals, perineum, skin) → significant risk for fx problems
circumferential burns (thorax/extremities)
significant chemical injury, electrical burns, lightning injury, coexisting major trauma, significant comorbidities
presence of inhalation injury
goes home
first degree
_ venom is associated with neuromuscular paralysis
elapids
produces complex/mixed toxidromes (muscle/tissue destruction)
neurotoxic snake venoms cause _ paralysis
descending
diplopia, ptosis, dysphagia, dysarthria, muscle weakness,
characteristics of elapid bites
snake hangs on → multiple tiny bite wounds
^ higher risk of envenomation vs. crotalid bites
minimal pain, redness, swelling
systemic effects of elapid envenomation + tx
sx delayed several hours!
euphoria, local paresthesia, N/V, drowsiness, dysphagia
antivenom can PREVENT paralysis but can NOT REVERSE it
→ NO fasciotomy, MUST treat if no snake ID, tourniquets
viperidae is the subfamily of?
crotalidae (pit vipers) = venous members of this family
moveable anterior fangs
viperids venom + systemic effects
cytotoxic and myotoxic effects
possible sig dysregulation of coag
= soft tissue necrosis, rhabdo, DIC
hypotension, fasiculations, diaphoresis, N/V, coag
mixed toxidrome (“broken neck” syndrome)
sx of viperidae envenomation
metallic taste
perioral tingling
fang marks
vesicles, necrosis
local swelling/pain/ecchymosis/erythema
Which snake is responsible for the most fatalities in North America?
Rattlesnake
grading for viperidae (crotalidae) bites
None
Minimal
Moderate
Severe
Moderate + severe might require fasciotomy
non-venomous vs venomous snake bites*
non-venomous: horseshoe
venomous:
crotalid = fang marks
elapidae = multiple tiny puncture wounds
why not to apply cold packs to snake bites?*
if you concentrate the venom where the bite is
→ DEC neurotoxic (don’t want to spread) BUT INC cytotoxic (you want cytotoxic venom to spread)
→ more risk of damage to area
what family of deadly snakes do not kill by envenomation?*
boidae (boas, pythons, anacondas)
kills by crushing
prehospital care of snake bite
ID snake
carry victim
remove jewelry
tourniquet (only in elapids)
do NOT “cut and suck”
NO cold packs
what does antivenom have
IgG antibodies
big SE: allergic rxn (Type 1 or 4 d/t the Fc portion/bottom part of “Y”)
mechanisms of type 1 hypersensitivity reactions*
must have previous sensitization to antigen against IgE (which is made by antibody-producing B lymphocytes)
release of chemical mediators from mast cells, basophils, eosinophils
histamine release → inc capillary permeability and vasodilation
what 2 WBC are bound to IgE → anaphylaxis?
eosinophils → degranulate
basophils → degranulate
neutrophils (eventually)
mast cell definition
basophils hat have migrated to a tissue
monocyte that has gone into tissues
macrophage
causes of anaphylaxis
proteins (food, venom, insulin)
haptens (PCN, abx, some anesthetics)
prostaglandin inhibitors (ASA, NSAID)
physical factors (exercise, stress, cold)
anaphylactoid (mast cell degranulation NOT from IgE ie vit K, morphine)
premonitory symptoms of anaphylaxis*
#1: pruritis of palms/soles
tingling in mouth/tongue
tightness in chest
dizziness/syncope
palpitations
clinical presentation of anaphylaxis*
urticaria (edema upper dermis, generalized flushing, wheals)
angioedema (PAINLESS edema of deep dermis d/t to vasodilation and 3rd spacing, “puffy” near mucous membranes)
laryngeal edema (“lump in throat”/hoarseness)
angioedema in uvula (pt chokes when speaking)
steeple sign
→ hypotension, CV collapse, respiratory arrest, GI
part of skin with most capillaries
deep dermis layer
treatment of anaphylaxis*
airway compromise → epi 0.3cc SQ
IV, O2, monitor, hydrate
hypotension/airway obstruction → epi 1.0cc IV
prepare intubate → cricothyrotomy tray
mild bronchospasm → inhaled beta-agonists (albuterol)
antihistamines
solumedrol or hydrocortisone IVP (q4hr)
terbutaline
if on BB, give glucagon
frostnip definition (mild)
superficial reversible ice crystal formation
frostnip information*
mild + least serious form of hypothermia
warm skin, sensate, normal texture
PE exam of frostnip*
painful sensations
darker areas of skin
red hyperemic skin
definition of chilblains (pernio) - moderate
painful inflammation of SMALL blood vessels in skin
occurs in response to sudden warming from cold temperatures
clears up within 1-3 weeks
chilblains (pernio) PE
red patches
blisters and swelling on extremities
frostbite (severe) definition
destruction of tissues d/t freezing
superficial damage can be reversed w tx
if severe (injury to reticular dermis + subdermal plexus → bone, muscle, tendon) → mummification
factors determining tissue loss from frostbite
magnitude of temperature depression
length of exposure
wetness/immersion
wind
associated factors of frostbite
poor nutrition
smoking/etoh
vascular disease
immunocompromised
PE findings of different severities of frostbite*
superficial: numb, white/yellow/molted, aching, throbbing/firm
moderate: vesicles/bullae w clear fluid
severe: gangrene, bullae w purple bloody fluid, waxy hard skin (deep injury)
prehospital management of frostbite*
do NOT rub/aggressively manipulative frozen parts
do NOT warm pre-hospital
remove cold clothing
trim clothing frozen to skin
treat systemic hypothermia
consider corneal/internal/bony injury
hospital management of frostbite*
tetanus shot
rapid thawing (40-42 C) ASAP!!
dress fingers and toes individually
leave hemorrhagic blisters intact
analgesia
elevate, split, avoid pressure
how is immersion foot similar/diff from frostbite?*
devs slowly and has no actual freezing
no ice crystals
neurovasc dmg/hypersensitivity/paresthesia/gangrene
immediate appearance = red
later = pale, edema, numb, pain
better prognosis than frostbite
systemic hypothermia is when the core temp is less than _*
35 C (95F)
organ dysfx occurs once temp goes below 35c
systemic hypothermia mild, mod, severe*
mild (32-35C): elevated HR and resp rate, alt mental status, shivering
mod (28-32C): shivering stops, worse vitals, stupor, polyuria, wheezing, a fib, osborn waves
severe (<28C): v fib occurs <28C, mydriasis (dilated pupil), coma, weak pulse, slow respiration, no reflex, bradycardia, heart block, v fib, asystole
RF/predisposing factors to systemic hypothermia
dec heat prod (CNS depression, immobility, endocrine failure, hypoglycemia)
inc heat loss (exposure, drugs, sepsis, neuro)
hypothalmic dysfx (acidosis, anoxia, stroke)
iatrogenic cooling (or, surgery)
how to warm a hypothermic patient?*
cardiac bypass (9-18C/hr)
chest tubes (3-6C/hr) - thoracic lavage
peritoneal lavage (3)
bladder irrigation w foley catheter (2)
shivering (1.5C)
warming blanket (2)
warm O2 w ET tube (1.5)
wram O2 w mask (1)
warm IV fluids (NO lactate) - least effective
bretylium - most effective
open cardiac massage
1st line tx for hypothermia*
bretylium
when can you declare death of hypothermic pt?*
the pt isn’t dead until he’s warm and dead
30-32C+ to be pronounced dead
if K+>10 = pt is not coming back even if cold and dead
what to be aware of when actively rewarming someone after hypothermia?*
afterdrop
second drop in temp d/t reperfusion of cold extremities
how are toxins classified?
meds
illicit substances
heavy metals
marine foodborne illness
plant/mushroom toxins
what are the pertinent historical considerations when a person is poisoned?
exposure
when and why
what form is toxin
route of exposure
how much/long was exposure
body systems in person who is poisoned*
blood pressure
heart rate
respiratory rate
body temp
pupillary diameter
nyastagmus
poisoned drugs that cause hypertension
amphetamines,
cocaine,
ergot,
head trauma,
MAOI,
PCP
poisoned drugs causing hypotension
BB,
amantia mushrooms,
CCB,
opioids,
TCA< phenothiazines,
sedatives
poisoned drugs causing tachycardia
amphetamines,
antichol,
ethanol,
nicotine,
organophosphates,
PCP
poisoned drugs causing bradycardia
BB,
cholinergic,
CCB,
clonidine,
digoxin,
opioids,
sedatives
poisoned drugs causing hyperventilation
ASA,
sympathomimetics,
hydrocarbons,
alc,
withdraw
poisoned drugs causing hypoventilation
botulin toxin,
ethanol,
organophosphates,
sedative,opioids
poisoned drugs causing hyperthermia
amphetamines,
anticholinergics,
cocaine,
phencyclidine,
ASA,
phenothiazines,
EtOH/Sedative withdrawal,
thyroid storm
poisoned dugs causing hypothermia
ethanol,
opioids,
phenothiazines,
sedative-hypnotics
, hypoglycemia
poisoned drugs causing miosis
cholinergics,
opioids,
PCP,
sedative-hypnotics,
phenothiazines
poisoned drugs causing mydriasis
anoxia,
anticholinergics,
sympathomimetics
poisoned drugs causing nystagmus
ethanol
pcp
phenytoin
sedatives
Amphetamines toxidromes
Hyperthermia
Tachycardia
Hypertension
anticholinergics toxidromes
Hyperthermia
Tachycardia
Mydriasis
Cocaine toxidromes
Hyperthermia
Hypertension
Phencyclidine (PCP) toxidromes
Hyperthermia
Tachycardia
Hypertension
Miosis
Nystagmus
MAOI toxidrome
hypertension
ASA toxidromes
Hyperthermia
Tachycardia
Hyperventilation
phenothaizines toxidrome
Hyperthermia
Tachycardia
Hypotension
Miosis
opioids toxidrome
Hypothermia
Bradycardia
Hypotension
Hypoventilation
Miosis
et/oh sedative withdrawal toxidrome
Hyperthermia
Hyperventilation
thyroid storm toxidrome
hyperthermia
nicotine toxidrome
tachycardia
organophosphates toxidromes
tachycardia
hypoventilation
treatment for poisoned pt*
labs (CUTE DIMPLES, glucose, BMP, HCG, utox, etoh, acetaminophen/ASA, EKG)
charcoal
gastric lavage
acute stabilization + antidote
cholinergic toxidrome (SLUDGE syndrome)*
salivation
lacrimation
urination
diaphoresis
GI upset
emesis
antidote for opioid (heroin, morphine, oxycodone)
narcan
antidote for acidosis, cocaine, cyanide, salicylate, TCA, barbiturate, cardiac arrest
bicarb
antidote for digoxin
digibind
antidote for cholinergic, organophosphates, cholinesterase, neuromuscular blockade
atropine
antidote for organophosphate + cholinesterase
pralidoxime
antidote for toxic alcohol poisoning (methanol/ethylene glycol)
ethanol
antidote for beta blocker, insulin, CCB, hypoglycemia, anaphylaxis
glucagon
antidote for acetaminophen
N-AC ((N-acetyl cysteine)
antidote for benzo, reversal for sedation + respiratory depression
flumazenil
most feared complication of methanol poisoning
blindness