Neuro Exam 3
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
Sympathetic vs Parasympathetic
Sympathetic- flight or fight, mobilize glucose stored (release stored energy), decrease digestion, increased bp and heart rate, divergence, anxiety disorder
Parasympathetic- rest and digest, increase digestion, stop sweating, pupils constrict, distributed processing
Cortisol
stress hormone - released from adrenal cortex because of communication from secretory hypothalamus
aids in metabolism and use of stored energy - can cause oxidative stress (stress that causes a protein to misfold - ex: plagues in brain)
long term exposure can cause exocytosis (cell death)
PTSD
long term sympathetic state- brain starts to shrink in mass because of increased cortisol levels over long periods of time
Oxytocin
increase bonds within groups and ethnocentric behavior
released from posterior pituitary gland
Vasopressin (ADH)
sodium gets high in blood and body needs to retain water - ADH tells kidney to not excrete and to retain as much fluid as it can, inhibit urine production
blood hypertonic- retain, get thirsty
blood hypotonic- low sodium, excrete as much water and increase the Na in blood
Hypothalamus
homeostasis - keep body in regulated steady state
secreting hypothalamus releases neurohormones through blood stream
hypothalamus → pituitary gland → neurohormones
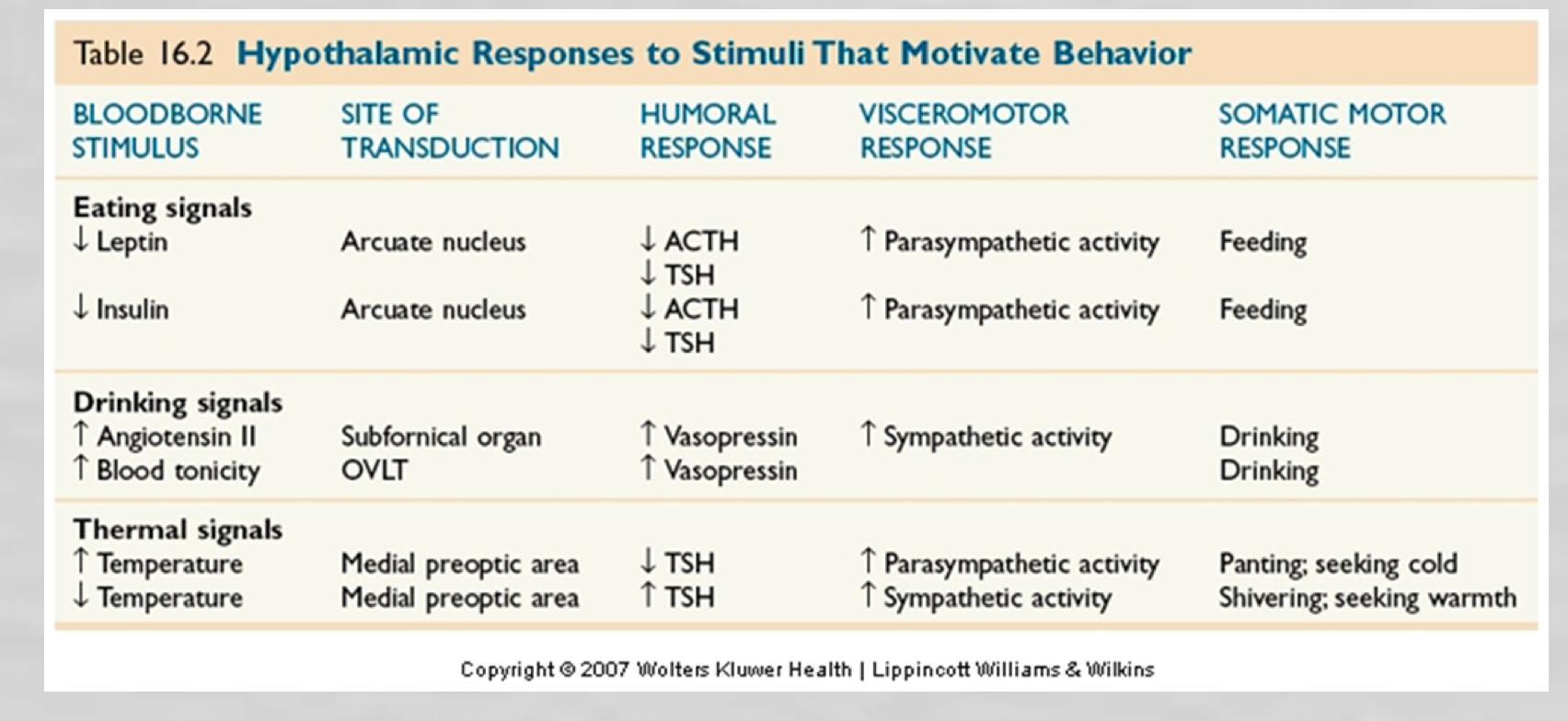
3 components of neuronal response
Humoral- how much salt in blood
Visceromotor- muscular - blood goes to organs - shivering, hair stands up when cold, sweating, panting when hot
Somatic- voluntary motor- cold=stand up and move, hot=jump in pool
Lateral hypothalamus
initiates motivation to actively seek or generate warmth - homeostasis
Prandial state
Anabolism - intestines full, nutrients broken down in gut into glucose and glycogen and ketone and fatty acids - triglycerides go into blood and become adipose tissue
energy stored as glycogen and triglycerides
Postabsorptive state
catabolism - breaking down complex macromolecules
intestines empty and glycogen gets released from liver - triglycerides broken into: ketones, fatty acids, and glucose = now can use energy
Lipostatic hypothesis
keeps body at certain set point
period of starvation- body weight drops, eat normal food, retain more glycogen, body returns to normal weight - leptin drops and starvation response
forced feeding- gain weight,retain back to normal eating, weight declines back to set point
Leptin
spikes= decreases appetite, increase energy expenditure
Anorexia
lesion lateral hypothalamus - related to leptin signaling
Obesity
lesion ventromedial hypothalamic - related to leptin signaling
Elevated leptin levels
activates arcuate neurons that release aMSH and CART (anorectic peptides- diminish appetite and increase energy expenditure)
arcuate nucleus, connects areas of hypothalamus - cause humoral, spinal cord affected (jitters), lateral hypothalamus (starved)
fire off paraventricular nucleus → activates sympathetic nervous system → stimulates release of ACTH and thyrotropin → turns off eating behavior
Decreased leptin levels
arcuate neurons release NPY and AgRP (counteract the CART and aMSH) from arcuate nucleus→ and stimulate lateral hypothalamus (eat more) → NPY and AgRP inhibits secretion of TSH and ACTH
oxygentic peptides-make you want to eat more, located in arcuate nucleus
neurons stimulating feeding behavior
lateral hypothalamic peptides - make us feel good
melanin-concentrating hormone (MCH) and orexin
Cephalic
smell good food, food is in head - ghrelin is released, hungry !
Gastric
stomach fills up - signals brain by vagus nerve
works with CCK released by intestines in response to certain foods and tells brain when full
Substrate
food is in intestines and broken down to distribute energy throughout the body, storing
insulin released by B cells of pancreas - insulin is highest in this phase
Ghrelin
released when stomach is empty
activates NPY and AgRP in arcuate nucleus
Dopamine reward circuit
high calorie = more reward neurons fire off
dopaminergic axons in the ventral tegmental area projecting to the forebrain
parkinson’s disease typically have a damages ventral tegmental area and do not get the same thrill from eating
dopamine depleted animals
lack motivation to seek food but enjoy it when available
Serotonin
low: postabsorptive period
rise: anticipation of food
spike: during meals
high calories elevates mood and rise blood tryptophan and brain serotonin
Volumetric drinking
hypovolemia: decrease in blood tone
receptors detect drop in bp → sends message vagus nerve → nucleus of solitary tract → hypothalamus → stimulates subtomical organ which releases angiotensin and decrease blood flow to kidneys (stop peeing)
Osmotic/tonic thirst
Hypertonicity- increased concentration Na in blood
neurons of OVLT stimulate → lateral hypothalamic area activate → magnocellular neurosecretory cells → releases vasopressin (ADH)
Diabetes insipidus- loss of vasopressin, lots of pale watery urine
Temperature regulation
anterior hypothalamus - cause humoral and visceromotor responses
fall in temp- TSH is released by anterior pituitary, stimulates thyroid gland
cheat sheet
genotype differences
X chromosome (1500) is much larger than Y (50)
genetic disorder- have to have bad transcript on both chromosomes - females less likely to have it, but can be carrier
X linked disease- much more common in males
SRY gene
on Y chromosome, sex determining region - encodes TDF (testis determining factor) causes genetic areas to develop testicles
TDF= not released=female. the default pathway is female
gender is determined at union
hormones and sex
sex hormones- steroids
endocrine glands- release sex hormones
pituitary gland- regulated endocrine glands
male hormone= testosterone (androgens), female hormone=estradiol (estrogens)
Aromatase
only difference of testosterone and estrogen hormone
Protein vs steroid hormones
protein- do not pass through cell membrane, bind surface receptors
steroid- pass through cell membrane which allows to change genetics of cell (alter DNA) and bind cytoplasmic receptors - alter membrane excitability, sensitivity to neurotransmitters, neurotransmitters released
hormone difference in cycles
Men- levels fluctuate daily, twice a day; rise when first wake up and rise in the middle of the afternoon
Woman- levels fluctuate, 28 day cycle
Gonadotropins
signaled by hypothalamus and released by anterior pituitary
males- LH produces testosterone, FSH aids in sperm maturation
female- LH and FSH cause estrogen secretion (follicular phase and luteal phase)
Sexual response cycle
Arousal, plateau, orgasm, resolution
cerebral cortex- tells us what is attractive/what we want in mate
spinal cord- mediates sexual response of genitals
spinal cord injury and sexual response
ganglions come out of the sympathetic chain in the sympathetic ganglion - ganglion near parasympathetic - operates independently of spinal cord- therefore still sexual response even though they cannot feel it
parasympathetic vs sympathetic in arrousal
parasympathetic- engorgement (blood goes to genitals),
sympathetic- orgasm
Neurotransmitters within sex
relax smooth muscle
acetylcholine, vasoactive intestinal polypeptide (VIP), nitric oxide (NO)
nitric oxide- relaxes smooth muscle to help for engorgement in males
mammals mating strategy
polygyny- male mates with many females
polyandry- female mates with many males
monogamy- one mate per person
prairie vs meadow voles
prairie- solid family values, monogamous, more oxytocin (female) and vasopressin (male)
meadow- asocial and only want sex, fewer receptors
Male and female brains differences
only 2-3 nuclei are different
Males- onuf’s nucleus help with urinating or defecating- extra sphincter and coded to ejaculate, sexually dimorphic nucleus (SDN) in rats or INAH in humans is two times larger
Females- smaller brain because smaller body, denser corpus callosum and more communication between the sides of the brain
homosexual males- INAH size of female
cognition differences male vs female
relation between cognition and hormones
males better with spatial reasoning, woman are better with language reasoning
woman get low estrogen levels (menopause) spatial reasoning improves
Prostaglandins
involved in tissue damage, pain, and fever
synthesized from arachidonic acid via COX enzyme
inhibit COX enzyme- males no longer want to mount females and allow to be mounted by other males
females to COX enzyme- start to look like males
Mismatches between genes and hormones
androgen insensitive genetic males- defective androgen gene and an X chromosome, genetically XY, phenotype XX (look female, female behavior etc) : no ovaries but undescended testicals
congenital adrenal hyperplasia genetic females- abnormally large adrenal glands, genotype: XX, more male phenotype (look more male)and produce more testosterone
activational effects of sex hormones
cause temporary modifications in brain organization, structural changes in neurites
men- rise in testosterone (want sex), fall in testosterone (no sex)
females- rise in estrogen (ovulation) increases sexual interest
estradiol surges = more receptors in hippocampus and reach more surface area = rat has peak fertility = increase in density
estradiol may have some neuro protective effects
James-Lange theory
emotion = response to physiological change in body
see snake = emotional expression first then experience fear (sweating, heart rate, before brain relates to something fearful) - do not have to have experience have physiological reaction
Cannon Bard Theory
emotions independent of emotional expression
see snake= need to be afraid - attach to things we know and are fearful of - then physiological change - need experience to know if you should be afraid
unconscious emotions
stimulus can have emotional impact without any conscious awareness - (stick tongue out and get smacked in head, stop sticking out tongue)
amygdala becomes active and changes the way we process information
Brocas limbic lobe
involved in emotion and emotional expression - cortex forming a ring around corpus callosum
cingulate gyrus, medial temporal lobe (limbic system), hippocampus
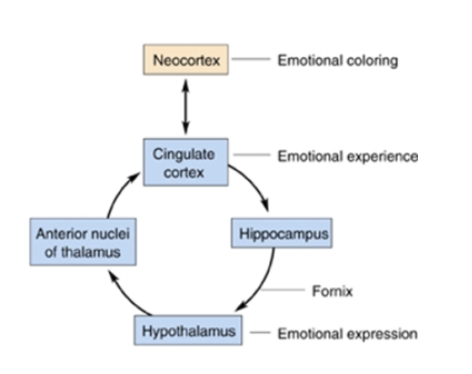
Papez circuit
limbic structures - links cortex with hypothalamus
starts at neocortex when seeing/processing something - gives us reasoning and controls response → cingulate cortex- emotional experience - connects with emotional memory → hippocampus connects the experience and expression→ hypothalamus- emotional expression- look of fear, happiness and releases neurohormones → anterior nuclei of thalamus- sensory related
Abnormal emotional expressions
Rabies infection - hyper emotional expression - infection targets the hippocampus and gets extra stimulated
Lesion anterior thalamus - leads to spontaneous laughter or crying not associated with an emotion
Single emotion concepts
we have diverse emotions - can be happy but also feel anxiety, mixed emotions
things that are relatively minor from a stimulus standpoint that cause a great response or the opposite
Temporal lobe and emotion
Kluver Bucy syndrome - take temporal lobe out and decreased fear and aggression, decreased vocalizations and facial expressions
hypersexuality, placidity, hyperorality (put inappropriate things in mouth), disordered eating
temporal lobe becomes damaged from stroke, trauma, encephalitis
Amygdala and fear
bilateral amygdalectomy reduces fear and aggression - anger, sadness, and disgust may be affected - inability to recognize fear in facial expressions, unable to concentrate and low energy
normal people- amygdala kicks off for fearful faces compared to happy/neutral faces and kicks off from learned fear
Predatory vs affective aggression
Predatory- attack towards head or neck, no sympathetic activity, attack to kill, quiet, no eye contact - elicited by stimulating lateral hypothalamus - medial forebrain bundle → ventral tegmental area
Affective- attract attention, bigger and stronger but tries to avoid violence, high levels of sympathetic - elicited by medial hypothalamus - dorsal longitudinal fasciculus → periaqueductal grey
hypothalamus and aggression
removal of cerebral hemispheres but not hypothalamus - sham rage = aggressive behavior without stimulus - can be reversed with lesions in hypothalamus
can happen from strokes
Serotonin and aggression
block serotonin = increase aggression
too much serotonin = cause aggression
physiological sweet spot - SSRI good drug to block reuptake and make your own source to keep it in range
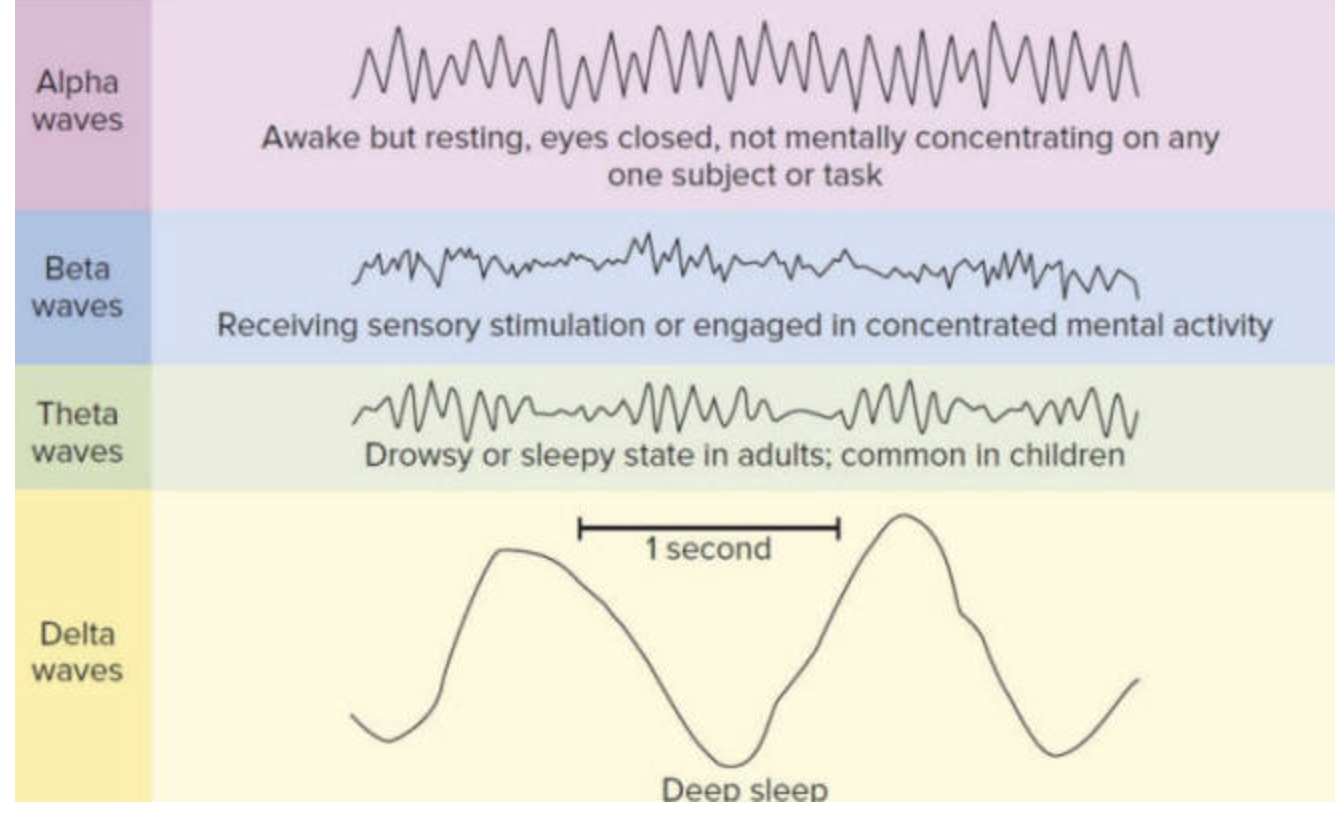
Electroencephalogram (EEG)
device on head that records brain rhythms and measures generalized cortical activity
recognizes burst activity of neurons (afferent axons) in pyramidal cells in dendrites of the cortex
diagnose: epilepsy, sleep disorders, ICU patients, neurosurgery
recording brain waves
voltage fluctuations measured by finding the difference between positive and negative charges = wave, wave gives current
tiny fluctuations of AP firing on afferent axons in the pyramidal cells of the cortex = make into wave and wave gives current
Irregular vs synchronized
Irregular- dense, low amplitude wave
synchronized- slower wave but higher amplitude, low frequency - everything is firing together in an organized burst
Magnetoencephalography (MEG)
recording magnetic signals generated by neural activity - shows sources of activity better than EEG - but can’t give detailed images of fMRI
fMRi and PET show blood flow differences and the changes in brain matabolism of glucose
Beta
dense, lowest amplitude, irregular - awake and moving around - uses lots of areas of the brain
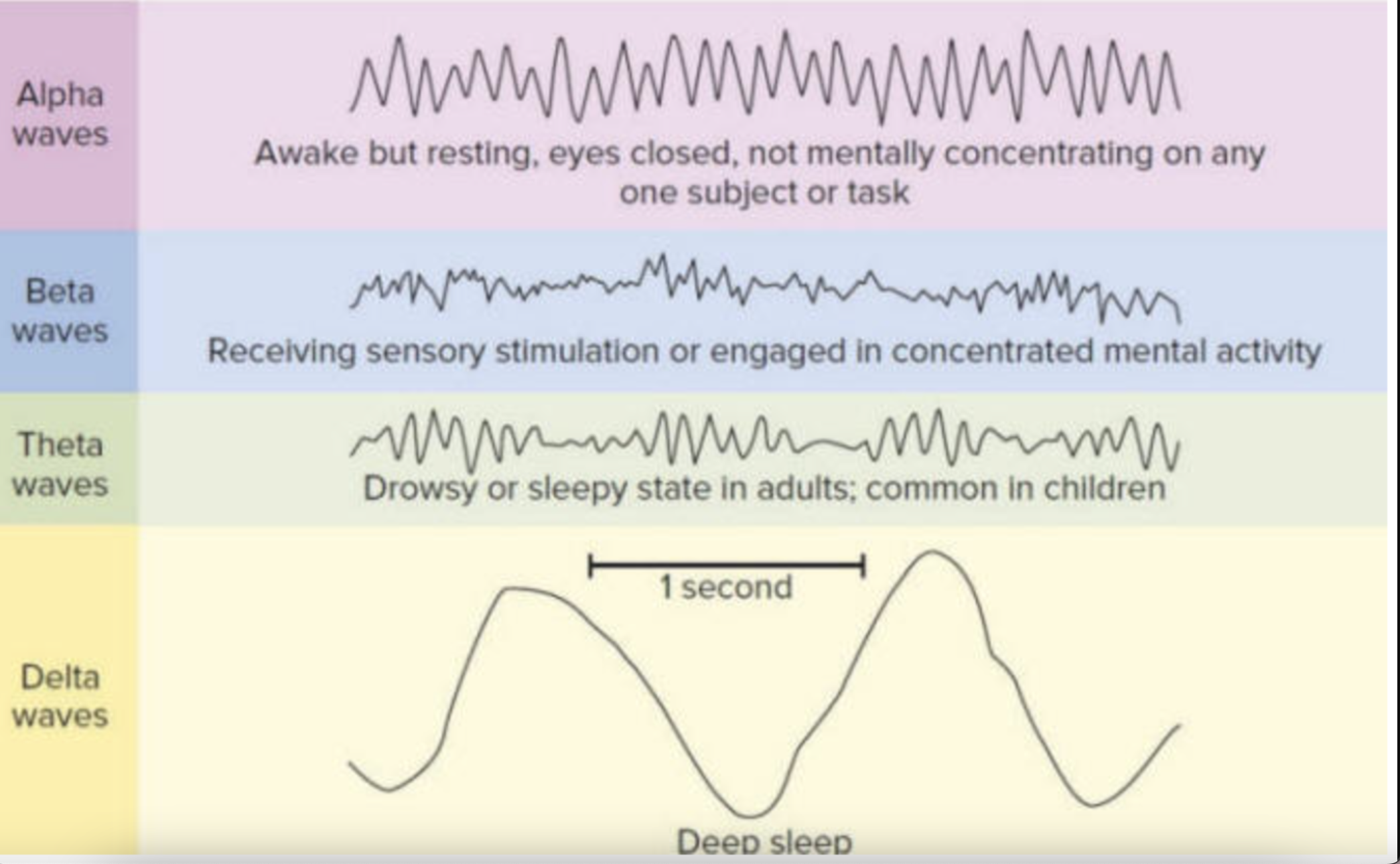
Alpha
quiet, waking state - sitting in a chair, dozing off
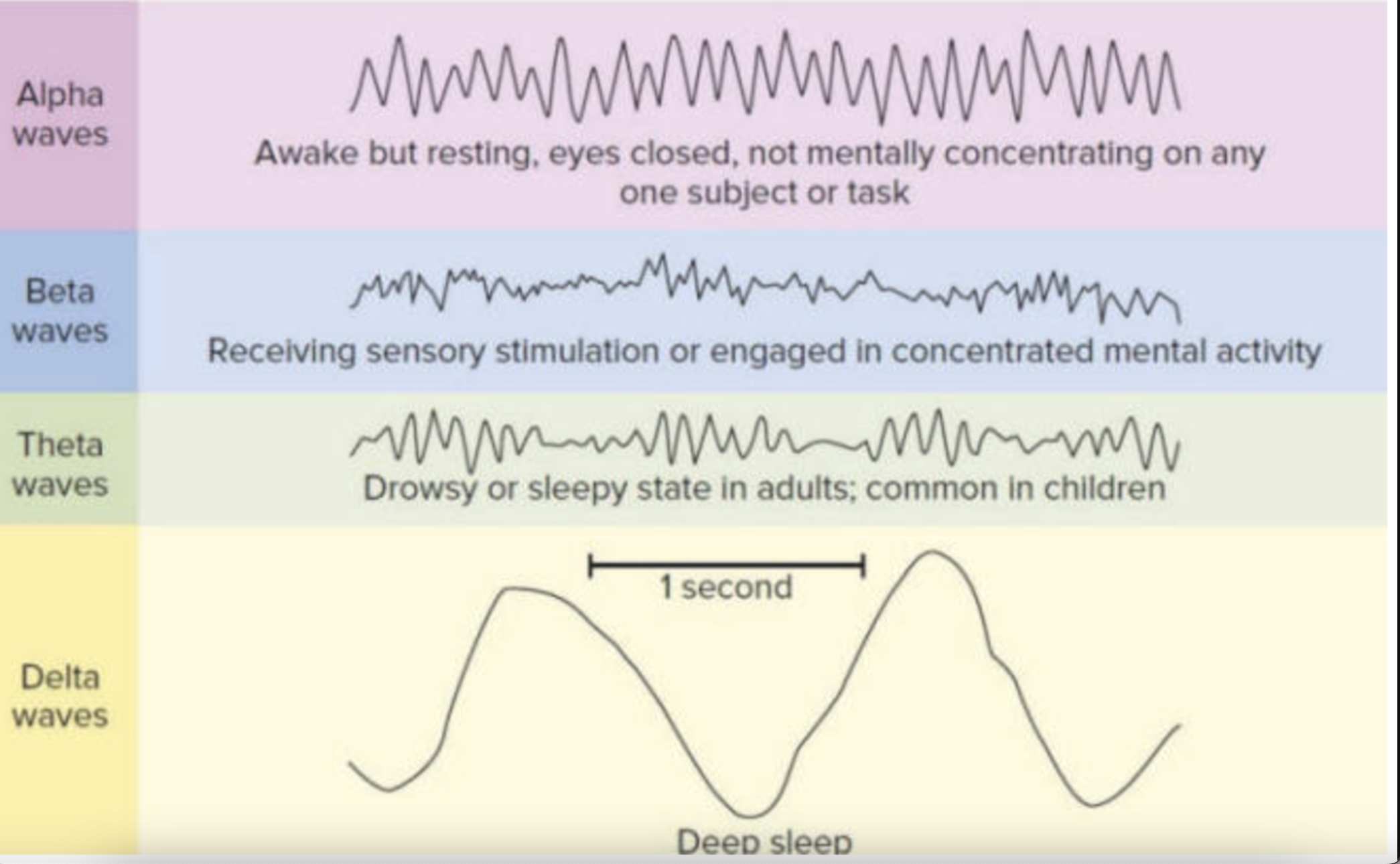
Theta
more regular and spaced out, really drowsy - light sleep, tossing and turning - K complexes and spindles
stage 1+2
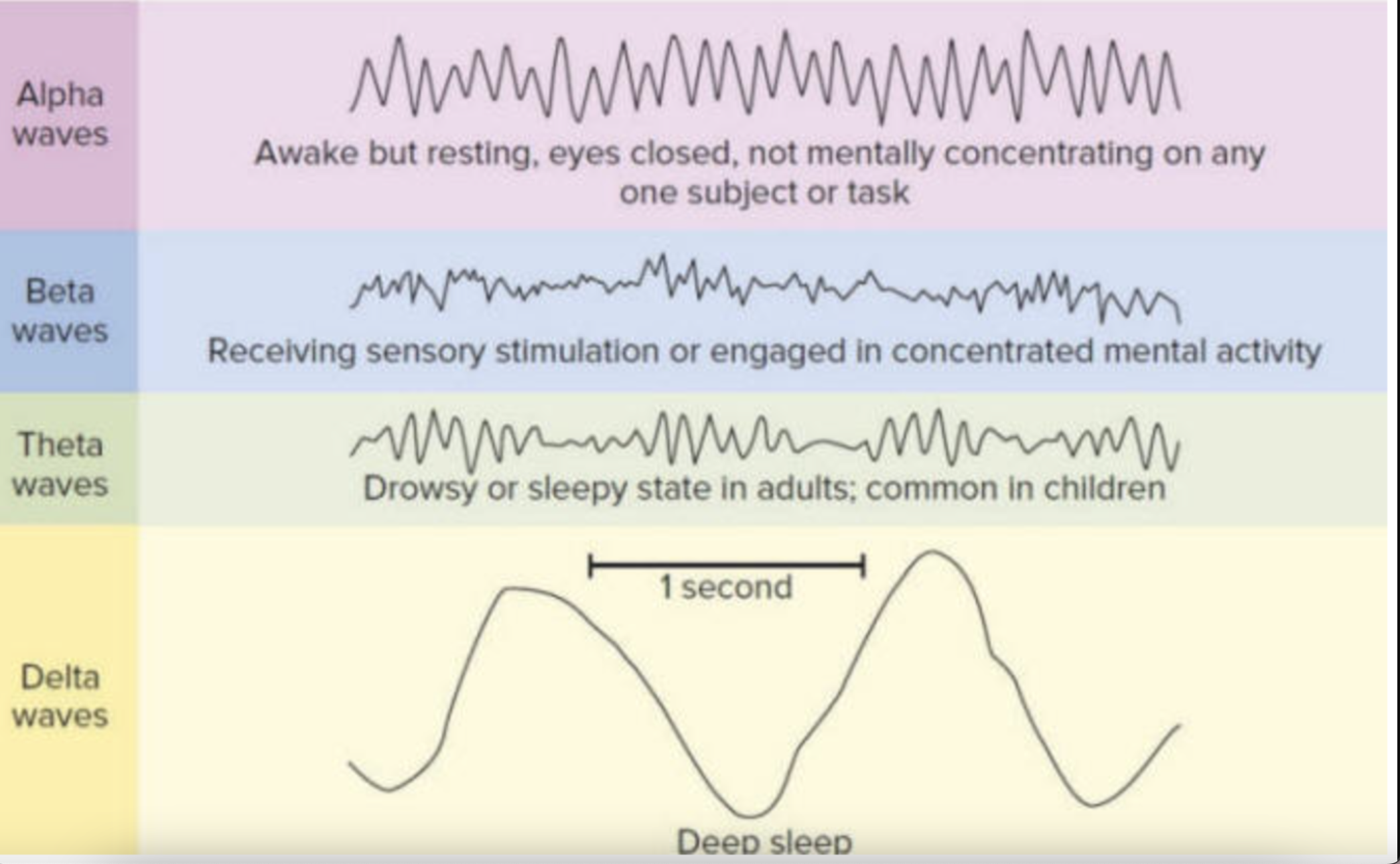
Delta
very regular, high amplitude and slow waves - deep sleep - disconnected from outside sensory world
stage 3+4, 4 is the longest stage of sleep
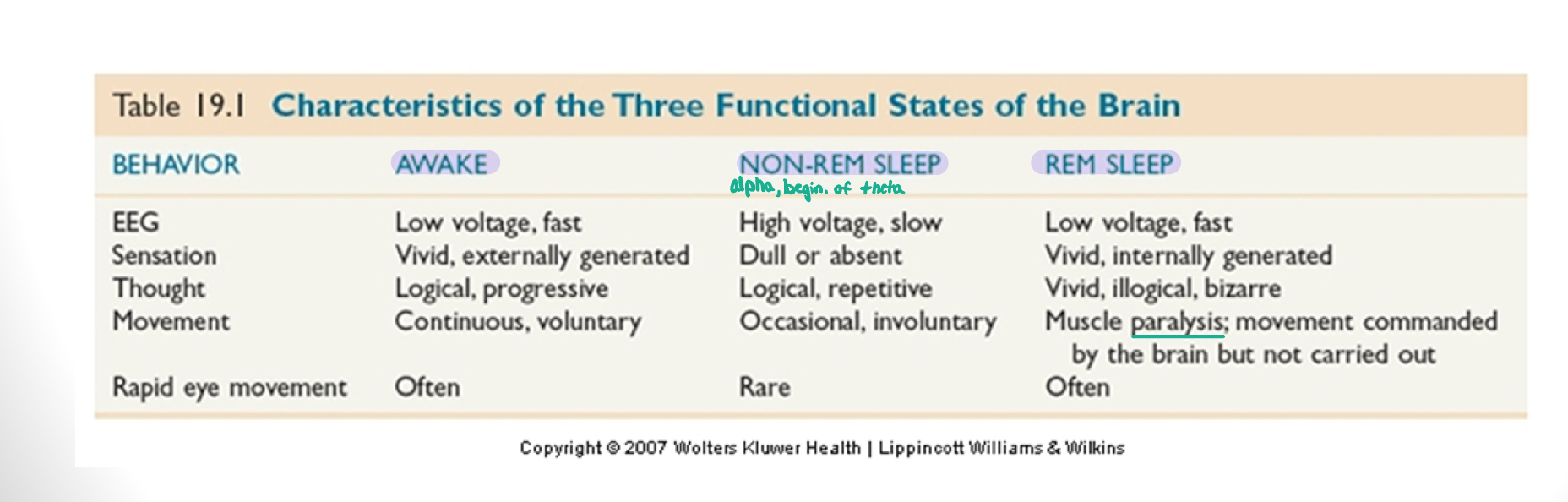
REM sleep
looks like beta - brain is very active
stage 5 - heart rate increases, piloerection
sleep releases hormones that
shut off the thalamus - paralysis so you don’t act out dreams
thalamus is active during REM
low hormone = sleep walking
Walter freeman
neuro rhythms coordinate with burst activity and bind together the pyramidal cells to burst together at identical times = waves of sleep
more synchorounous the waves = less conscious control
Seizures
usually respond well with meds
Generalized- entire cerebral cortex - electrodes exploding with activity - high amplitude, high frequency - lose consciousness
Partial- circumscribed cortex area (ex: arm or visual)
Absence- less than 30 sec of generalized - not disruptive to motor but yes cognition - misdiagnosed as ADD
old passive sleep theories
toxin- body produces toxins that accumulate, toxins build up and gets drowsy, so sleep to process toxins
ischemia- standing all day and blood pools to legs and lower body = makes us tired and want to sleep
synaptic fatigue (Pablo)- produce neurotransmitters and once the body has spend it all you need to sleep to reproduce neurotransmitters
Cleighton- natural state is sleep and only wake for needs (hunger, bathroom)
Bremer- brain is resting while asleep which isolates body from sensory experience - thought the thalamus was not active
three functional brain states
people talkin about sleep
Sigmund Freud- dream functions, wish fulfillment, conquer anxieties - doesn’t do much
Allan Hobson and Robert McCarley- activation synthesis hypothesis - need to synthesis proteins - true
Avi Karni- certain memories require strengthening period for REM sleep - true
diffuse modulatory neurotransmitter systems
norepinephrine and serotonin- very important in waking cycle and REM cycle
when falling asleep= decrease the firing/inhibited
Cholinergic neurons
enhance REM events - active during waking - turn off in most of sleep cycle
control rhythmic behaviors of the thalamus and sends burst activity to inhibitory neurons (GABA)
thalamus burst in activity controls the cortical EEG which blocks the sensory input which keeps us from acting out
Reticular Activating System
in midline of brain, if stimulated people get burst activity and start to sleep, more stimulation= wake up and be alert
gives signals for us to sleep but has to be active for us to be awake
Sleep promoting factors
Muramyl dipeptide- from CSF and goes away in REM sleep
Interleukin-stimulates the immune system - sleep deprived = get sick
Adenosine- amino acid that gets released when inhibitory system activates and body paralysis
Melatonin- hormone produced by pineal gland, helps with circadian rhythm
Gene expression in sleep
half a percent of genes are either awake or sleep states - certain genes are triggered by sleeping - neuro plasticity related gene
no sleep= no memories, no new proteins, no healing
Circadian Rhythms
daily cycles of light and dark
need to be active= physiological and biochemical highest
can drift from lack of zeitgebers
Zeitgebers
environmental time cues - light and dark cycle
no environmental cues of light and dark = drift out of 12 hour phase and into 24 hours
Suprachiasmatic Nucleus
regulates the circadian rhythm -each SCN has a rhythmic message that has a firing rate that varies with the circadian rhythm - genes cause this to happen not tetrodotoxin
photoreceptor synapses directly on SCN neurons - photoreceptor is a ganglion cell in the retina that contains melanopsin (slowly excited by light)
SCN sends out efferent to the hypothalamus, midbrain, diencephalons - uses GABA
each cell has a clock gene that changes mRNA which causes us to sleep and wake
Creativity
understanding the fundamental rules for meaningful utterances
Form
language is formed for an arrangement of difference sounds from a limited range in a predictable sequence
Content
language requites a combination of phonemes and the connection of words
Use
language is used as a mean of social communication
language in brain
Parietal-occipital-temporal association cortex- links several sensory modalities
Pre-frontal cortex- planning responses
Parietal lobe (left)- locate lots of language function
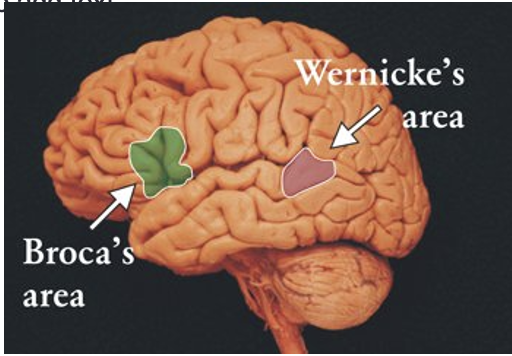
Brocas vs Wenickes’s area
Brocas- motor area of the frontal cortex that allows our mouth/tongue to move speech
Wernicke’s- understanding of speech
Wada procedure
used to determine hemisphere dominant for speech (typically left- rarely right side)
gives an anesthetic that shuts down speech so they can see where the speech centers are so they don’t damage them in brain surgery
Stages of language in lil kids
6 months - babbling
1 year- one word sentences - (mom, dad, yes, no)
1.5 years- 30-50 words, adjectives, nouns, verbs
2 years- 2 word speech - 50-several hundred words
2.5 years- 3 or more word sentences, multiple combinations, grammatical errors, good comprehension
3 years- full sentences, few error around 1000 word vocabulary
4 years- close to adult speech
Brocas aphasia
Lesions: Left posterior inferior frontal
Verbal output: Non-fluent - use filler words (bro, like, um)
Repetition: Impaired- cant repeat a word you tell them to
Comprehension: Normal - gets frustrated because they know what they want to say but can’t
Naming: Marginally impaired- cannot name object even if they know what its used for
Associated Signs: Right hemiparesis, Right homonymous hemianopia, apraxia of left face and limbs
Wernicke’s aphasia
Lesions: Left posterior superior temporal
Verbal output: Fluent- words messed up but they do not realize
Repetition: Impaired
Comprehension: Impaired- do not realize what they are saying is wrong
Naming: Impaired
Associated Signs: Difficulty with occupational engagement
Conduction Aphasia
Lesions: left parietal - arcuate fasciculus is damaged
Verbal output: fluent
Repetition: impaired
Comprehension: normal
Naming: impaired (paraphasic)
Associated Signs: Right hemisensory deficit, apraxia of all limbs and face
Global Aphasia
everything verbal is impaired and outcome is not good
Lesions: left frontal temporal perietal
Verbal output: nonfluent
Repetition: impaired
Comprehension: impaired
Naming: impaired
Associated Signs: Right hemiparesis, right hemisensory, right homonymous hemianopsia
Anomic Aphasia
Lesions:left posterior inferior temporal or temporal-occipital region
Verbal output: fluent
Repetition: normal (anomic)
Comprehension: normal
Naming: impaired - can tell everything about the object but cannot get the correct word
Associated Signs: none
Transcortical motor
similar to brocas but bigger and effects the motor production and right hemiparesis - hard to tell the difference
Lesions: Left medial frontal or anterior border zone
Verbal output: nonfluent
Repetition: normal
Comprehension: normal
Naming: impaired
Associated Signs: right hemiperesis
Sensory
similar to Weirnkes but can repeat normally
Lesions: left medial parietal or posterior border zone
Verbal output: fluent
Repetition: normal
Comprehension: impaired
Naming: impaired
Associated Signs: Right homonymous hemianopia
mixed aphasia
Lesions: left medial frontal parietal or complete border zone
Verbal output: nonfluent
Repetition: normal
Comprehension: impaired
Naming: impaired
Associated Signs: Right hemiparesis, right hemisensory defect
Wernicke Geschwind Model
it over simplifies and takes speech into a sutomotor response- makes the assumption that speech is just like writing and you’ll have the same problems with speech and writing but thats not true
Split brain procedures
opposite side acts as if it wasn’t there; conflicting behaviors and brief stimuli only went to one hemisphere
left hemisphere language dominance- right visual field repeated easily - left visual field has difficulty verbalizing - unable to describe anything to left of visual fixation point
Right vs left hemisphere
right- can perceive the left side of body, drawing, puzzles, holistic
left- can perceive both sides of the body, language, logical, objective - left planum temporal is larger than right