531 Lec 28
5.0(2)
Studied by 11 peopleCard Sorting
1/31
There's no tags or description
Looks like no tags are added yet.
Last updated 6:22 PM on 4/16/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
1
New cards
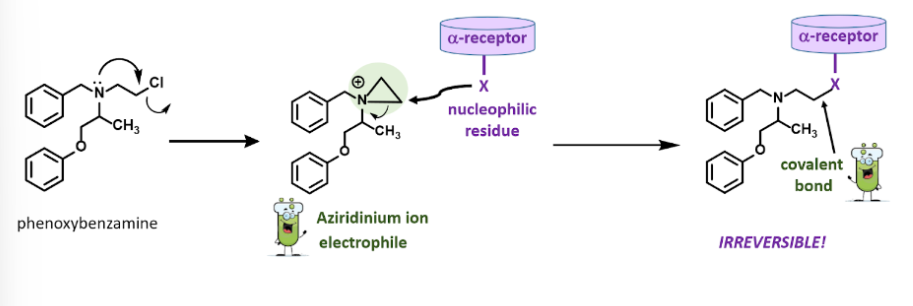
Phenoxybenzamine
Nonselective alpha adrenergic antagonists
2
New cards
the mechanism by which phenoxybenzamine inhibits the receptor, what intermediate it forms and what bonds are relevant to its action.
• The chlorine leaves and an epoxide forms, this intermediate is called an Aziridinium ion electrophile and it is positively charged
•A nucleophilic residue on the alpha receptor will attack the epoxide causing it to open and forming a covalent bond
•A nucleophilic residue on the alpha receptor will attack the epoxide causing it to open and forming a covalent bond
3
New cards
why is phenoxybenzamine toxic
Phenoxybenzamine is toxic because it is non selective
4
New cards
what phenoxybenzamine is used for clinically.
Clinically, phenoxybenzamine is used to treat adrenal medulla tumors (pheochromocytoma) → counteracts release of large amounts of NE epinephrine that lead to hypertension
5
New cards
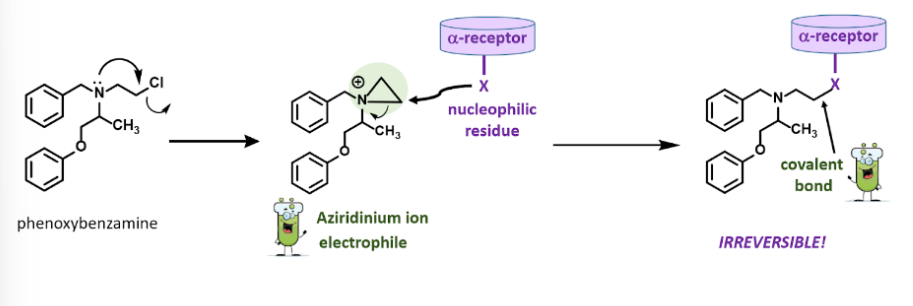
Quinazolines
Antihypertensive agents
• Prazosin (Minipres)
• Terazosin (Hytrin)
• Doxazosi (Cardura)
• Prazosin (Minipres)
• Terazosin (Hytrin)
• Doxazosi (Cardura)
6
New cards
rank the quinazoline class of selective alpha-1 adrenergic antagonists based on half life
Prazosi (Minipres), Terazosin (Hytrin), Doxazosi (Cardura)
7
New cards
What structural changes were made to quinazoline class of selective alpha-1 adrenergic antagonists to alter half life?
8
New cards
Why is half life relevant to the patient treatment plan?
Half life of the drug affects how frequently the patients will have to take the drug. Having a short half life means patients will have to take the drug more frequently which can make medication adherence difficult.
9
New cards
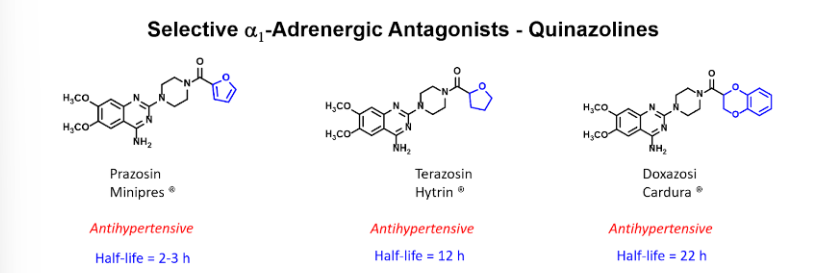
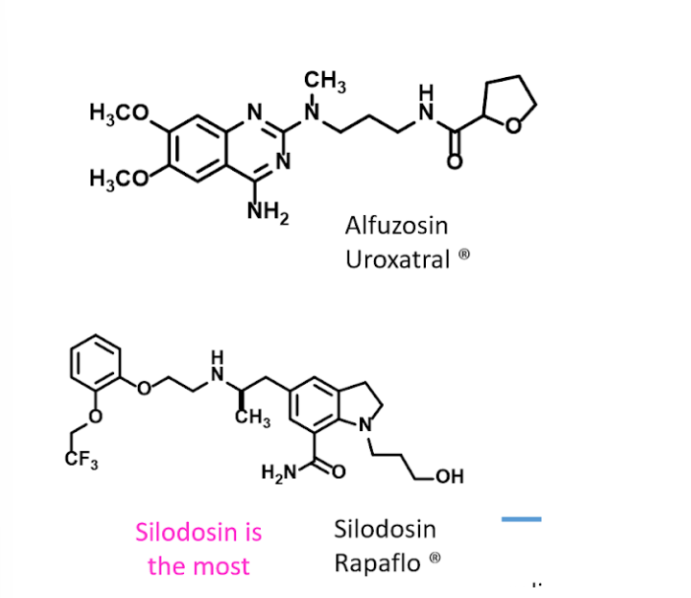
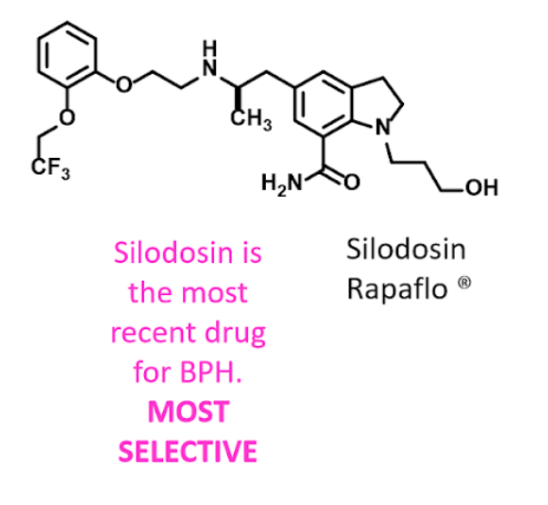
first line treatments for BPH and know why they are not used for hypertension.
• BPH: Benign prostatic hyperplasia (Enlarged prostate)
→Alfuzosin (Uroxatral)
→Silodosin (Rapaflo) - more selective
\
•Treats BPH due to blocking the alpha A1 receptors in the prostate gland
\
•Since they are more selective for a subtype of alpha adrenergic receptors (A1) they are useless for treating hypertension
→Alfuzosin (Uroxatral)
→Silodosin (Rapaflo) - more selective
\
•Treats BPH due to blocking the alpha A1 receptors in the prostate gland
\
•Since they are more selective for a subtype of alpha adrenergic receptors (A1) they are useless for treating hypertension
10
New cards
What is the most selective drug for treating BPH that we discussed?
Silodosin (Rapaflo)
11
New cards
Alpha Blockers
Prevents NE from tightening the muscles in the walls of smaller arteries and veins→ Causes vasodilation which improves blood flow to the heart and lowers blood pressure
12
New cards
Beta Blockers
Works by blocking effects of epinephrine on heart
\
Blocking epinephrine causes slower and softer heart beat which reduces blood pressure
\
Blocking epinephrine causes slower and softer heart beat which reduces blood pressure
13
New cards
Understand why beta blockers may be contraindicated in patients with COPD or uncontrolled Asthma
• B1 receptors are found in the heart and kidneys
• B2 receptors are found in the lungs, GI, liver, uterus, vascular and skeletal muscle (antagonists can cause bronchoconstriction)
• B2 receptors are found in the lungs, GI, liver, uterus, vascular and skeletal muscle (antagonists can cause bronchoconstriction)
14
New cards
Where are beta 1 receptors predominately found? Where are beta 2 receptors predominately Found?
•Heart and Kidneys
•Lungs, GI, liver, uterus, vascular and skeletal muscle
•Lungs, GI, liver, uterus, vascular and skeletal muscle
15
New cards
Why is hypoglycemia a concern with certain beta blockers (which ones?) In what patient
population would you be most concerned with this side effect and why?
population would you be most concerned with this side effect and why?
•Hypoglycemia: low blood sugar
\
•Stimulating B2 receptors normally stimulate hepatic glycogen breakdown (glycogenolysis) and pancreatic release glucagon which work together to increase plasma glucose
\
Blocking B2 lowers plasma glucose
\
•Stimulating B2 receptors normally stimulate hepatic glycogen breakdown (glycogenolysis) and pancreatic release glucagon which work together to increase plasma glucose
\
Blocking B2 lowers plasma glucose
16
New cards
Understand the role beta blockers have on renin release and the eventual outcome on hypertension.
beta blockers decrease renin which reduces angiotensin production which means decrease in blood pressure
17
New cards
What are the main differences/differentiating characteristics among the three generations of beta blockers?
1st Generation: nonselective (reactive at B1 and B2 receptors)
→Propanolol, Sotalol
\
2nd Generation: B1 selective or cardioselective- low dose
→ Atenolol, metoprolol, bisoprolol
\n
3rd Generation: additional vasodilating effects and neutral on plasma glucose/lipids
→ Nebivolol, carvedilol
→Propanolol, Sotalol
\
2nd Generation: B1 selective or cardioselective- low dose
→ Atenolol, metoprolol, bisoprolol
\n
3rd Generation: additional vasodilating effects and neutral on plasma glucose/lipids
→ Nebivolol, carvedilol
18
New cards
what is meant by “cardioselective” beta blockers and under what circumstances they are not cardioselective?
Cardioselective agents have a greater affinity for β1-adrenergic receptors located in the heart. However, at high doses cardioselectivity is lost.
19
New cards
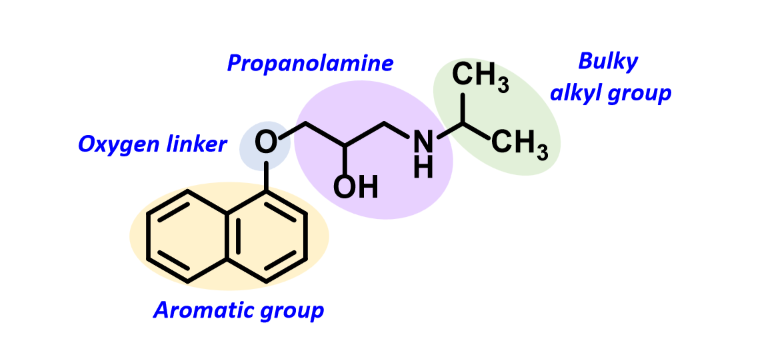
What is the general pharmacophoric model of the beta blocker drug class?
Aromatic group
Oxygen linker
Propanolamine
Bulky alkyl group
Oxygen linker
Propanolamine
Bulky alkyl group
20
New cards
Compared to all other beta blockers, propranolol has a characteristic than permits it to cross the blood-brain barrier. What is this physiochemical parameter and how does this feature extend the number of indications for which propranolol can be used?
Highly lipophilic → Anti anxiety
21
New cards
first generation beta blocker
Bunolol
Carteolol
Metipranolol
Nadalol
Pindolol
Penbutolol
\
\
Used for hypertension, angina, cardiac arrythmias, migraine, stage fright, glaucoma, congestive heart failure
Carteolol
Metipranolol
Nadalol
Pindolol
Penbutolol
\
\
Used for hypertension, angina, cardiac arrythmias, migraine, stage fright, glaucoma, congestive heart failure
22
New cards
second generation beta blocker
Acebutolol
Atenolol
Betaxolol
Esmolol
Metoprolol
Bisopropol
Atenolol
Betaxolol
Esmolol
Metoprolol
Bisopropol
23
New cards
Name two mechanisms by which first generation beta blockers work as antihypertensive agents
Decrease cardiac output and heart rate
Reduce renin release from kidneys
Reduce renin release from kidneys
24
New cards
what general structural modification imakes B1 selectivity?
4 substitution
25
New cards
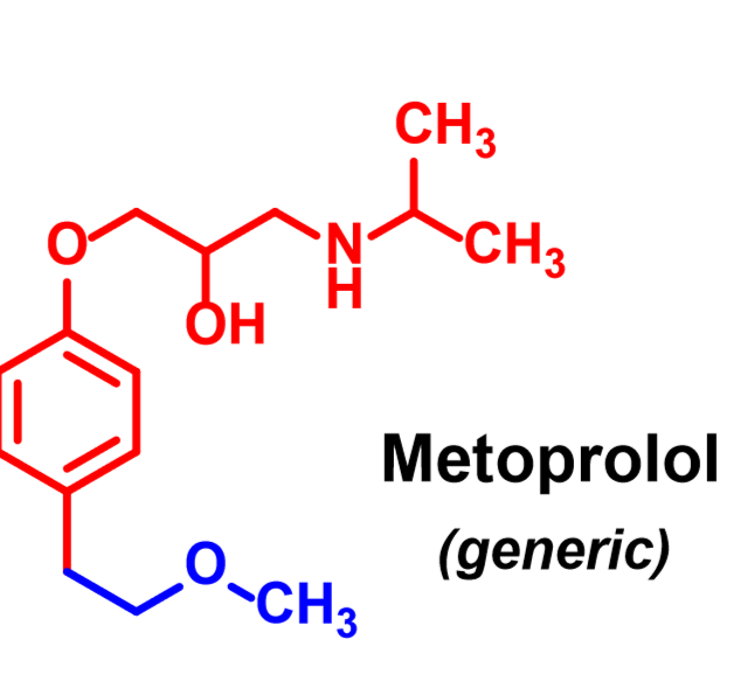
Metoprolol
Exception to 2nd gen- not B1 selective
Use: hypertension, angina, aniarrythmic, congestive heart failure
Signif first pass effect
Use: hypertension, angina, aniarrythmic, congestive heart failure
Signif first pass effect
26
New cards
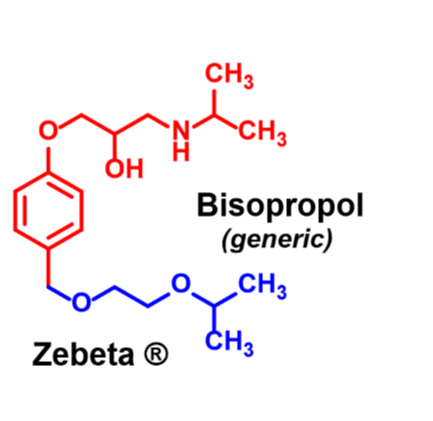
Bisoprolol
Use: hypertension, angina, aniarrythmic, congestive heart failure
Signif first pass effect
Longer side chain
Signif first pass effect
Longer side chain
27
New cards
what functional group is present in Esmolol that imparts a very short half-life and how this is different in Atenolol.
Ester- rapid hydrolysis by esterases in red blood cells
Half life: 9 min
Half life: 9 min
28
New cards
What are key characteristics of third generation beta blockers that distinguishes them from other generations?
Additional vasodilating effects and are most effective in decrease of blood pressure
29
New cards
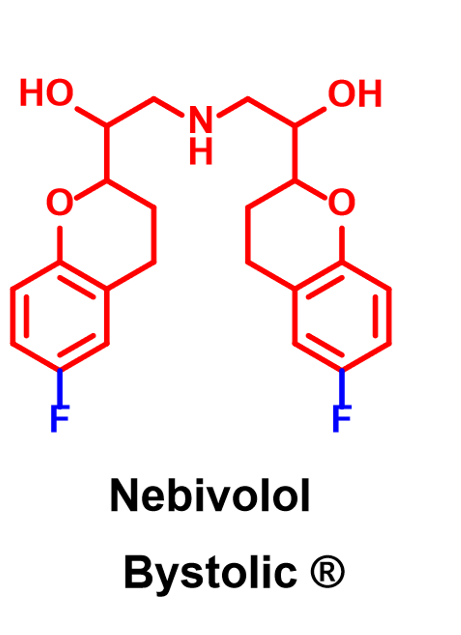
Nebivolol
→Nitric Oxide potentiating vasodilatory effects: induces endothelium dependent arterial realxation in a dose dependent manner, by stimulation of the release of endothelial nitroc oxide
→ Cardioselective
→Half life: 10 hours
→ Increases Stroke volume without compromising cardiac output
→Less bronchoconstriction
→Reduced side effects such as fatigue, depression, impotence, bradycardia
\-3rd gen beta blocker
→Neutral on plasma glucose or lipids- may be favored in diabetic patients
→ Cardioselective
→Half life: 10 hours
→ Increases Stroke volume without compromising cardiac output
→Less bronchoconstriction
→Reduced side effects such as fatigue, depression, impotence, bradycardia
\-3rd gen beta blocker
→Neutral on plasma glucose or lipids- may be favored in diabetic patients
30
New cards
Carvediol
→ 3rd gen beta blocker
→Nonselective beta blocker and alpha 1 blocker
\
Used:
Mild to severe congestive heart failure
Left ventricular dysfunction following heart attack
High blood pressure
→Nonselective beta blocker and alpha 1 blocker
\
Used:
Mild to severe congestive heart failure
Left ventricular dysfunction following heart attack
High blood pressure
31
New cards
adverse effects of beta blockade
1)Bronchoconstriction (contraindicated in asthma patients)
2)Arrhythmia if stopped suddenly
3)Cold extremities
4)Disturbed metabolism (care should be taken in diabetic patients)
5)Drug interactions/metabolism can reduce beta blocker effect or increase its concentration
6)Decrease nocturnal melatonin release→may account for sleep disturbances in some cases
2)Arrhythmia if stopped suddenly
3)Cold extremities
4)Disturbed metabolism (care should be taken in diabetic patients)
5)Drug interactions/metabolism can reduce beta blocker effect or increase its concentration
6)Decrease nocturnal melatonin release→may account for sleep disturbances in some cases
32
New cards
other drugs available to modify blood pressure that do not involve blockade of beta receptors
1)Drugs interfering with NE/EPi biosynthesis
2)Drugs affecting NE release, reuptake, and metabolism
2)Drugs affecting NE release, reuptake, and metabolism